 Rima Moghnieh1*Nour Estaitieh1Anas Mugharbil2Tamima Jisr3Dania I. Abdallah4Fouad Ziade5Loubna Sinno6Ahmad Ibrahim2
Rima Moghnieh1*Nour Estaitieh1Anas Mugharbil2Tamima Jisr3Dania I. Abdallah4Fouad Ziade5Loubna Sinno6Ahmad Ibrahim2- 1Department of Internal Medicine, Makassed General Hospital, Beirut, Lebanon
- 2Division of Hematology-Oncology, Department of Internal Medicine, Makassed General Hospital, Beirut, Lebanon
- 3Department of Laboratory Medicine, Makassed General Hospital, Beirut, Lebanon
- 4Pharmacy Department, Makassed General Hospital, Beirut, Lebanon
- 5Faculty of Public Health, Lebanese University, Beirut, Lebanon
- 6Research Coordinator, Makassed General Hospital, Beirut, Lebanon
Introduction: Bacteremia remains a major cause of life-threatening complications in patients receiving anticancer chemotherapy. The spectrum and susceptibility profiles of causative microorganisms differ with time and place. Data from Lebanon are scarce. We aim at evaluating the epidemiology of bacteremia in cancer patients in a university hospital in Lebanon, emphasizing antibiotic resistance and risk factors of multi-drug resistant organism (MDRO)-associated bacteremia.
Materials and Methods: This is a retrospective study of 75 episodes of bacteremia occurring in febrile neutropenic patients admitted to the hematology-oncology unit at Makassed General Hospital, Lebanon, from October 2009-January 2012. It corresponds to epidemiological data on bacteremia episodes in febrile neutropenic cancer patients including antimicrobial resistance and identification of risk factors associated with third generation cephalosporin resistance (3GCR) and MDRO-associated bacteremia.
Results: Out of 75 bacteremias, 42.7% were gram-positive (GP), and 57.3% were gram-negative (GN). GP bacteremias were mostly due to methicillin-resistant coagulase negative staphylococci (28% of total bacteremias and 66% of GP bacteremias). Among the GN bacteremias, Escherichia coli (22.7% of total, 39.5% of GN organisms) and Klebsiella pneumoniae(13.3% of total, 23.3% of GN organisms) were the most important causative agents. GN bacteremia due to 3GC sensitive (3GCS) bacteria represented 28% of total bacteremias, while 29% were due to 3GCR bacteria and 9% were due to carbapenem-resistant organisms. There was a significant correlation between bacteremia with MDRO and subsequent intubation, sepsis and mortality. Among potential risk factors, only broad spectrum antibiotic intake >4 days before bacteremia was found to be statistically significant for acquisition of 3GCR bacteria. Using carbapenems or piperacillin/tazobactam>4 days before bacteremia was significantly associated with the emergence of MDRO (p < 0.05).
Conclusion: Our findings have major implications for the management of febrile neutropenia, especially in breakthrough bacteremia and fever when patients are already on broadspectrum antibiotics. Emergence of resistance to 3GCs and, to a lesser extent, to carbapenems in GN isolates has to be considered seriously in our local guidelines for empiric treatment of febrile neutropenia, especially given that their occurrence was proven to be associated with poorer outcomes.
Introduction
The progress of anticancer therapy with aggressive supportive care for patients with malignancies and patients undergoing hematopoietic stem cell transplantation (HSCT) have recently improved patient prognosis (Trecarichi and Tumbarello, 2014). However, these advances, resulting in a prolonged and profound level of immunosuppression, neutropenia in particular, along with the extensive use of implantable medical devices, have also increased the risk of severe infections (Trecarichi and Tumbarello, 2014). Different types of infections may occur in cancer patients, but bloodstream infections (BSIs) are the most common severe infectious complications; the reported prevalence of BSIs ranges from 11 to 38%, and the crude mortality rate reaches up to 40% (Wisplinghoff et al., 2003a,b; Tumbarello et al., 2012; Montassier et al., 2013).
The type of microorganisms isolated on blood culture from febrile neutropenic patients varies with time and place (Jones, 1999; Dettenkofer et al., 2003; Wisplinghoff et al., 2003b; Irfan et al., 2008; Freifeld et al., 2011). Data from the Middle East and North Africa (MENA) region is scarce.
At the beginning of the use of cytotoxic chemotherapy in the 1960s and 1970s in cancer patients, gram-negative bacteria (GNB) were the most common organisms causing bacteremia in febrile neutropenic patients (Jones, 1999; Irfan et al., 2008); however, at the turn of the century, the most common bacterial pathogens isolated from blood cultures were coagulase-negative staphylococci (Dettenkofer et al., 2003; Wisplinghoff et al., 2003b; Freifeld et al., 2011).
However, in recent years several studies have demonstrated a clear trend in the epidemiology of BSIs, showing a shift of prevalence from gram-positive to gram-negative bacteria (Wisplinghoff et al., 2003b; Pagano et al., 2012; Montassier et al., 2013). There is an emergence of drug-resistant GNB such as multidrug resistant (MDR) Pseudomonas aeruginosa, Acinetobacter baumannii, Stenotrophomonas maltophilia, extended-spectrum beta-lactamase (ESBL)-producing GNB, and carbapenemase-producing GNB (Zinner, 1999; Wisplinghoff et al., 2003b; Ramphal, 2004; Freifeld et al., 2011; Pagano et al., 2012; Wu et al., 2012; Montassier et al., 2013). The issue of antimicrobial resistance has become a significant problem worldwide, where treatment of infections due to MDR bacteria represents a clinical challenge because the therapeutic options are often very limited. Risk factors of bacteremia due to MDR GNB in febrile neutropenic cancer patients vary depending on the type of organism, duration of hospitalization, and antibiotic therapy (Gudiol and Carratala, 2014).
So, the fact that the epidemiology of pathogens is dynamic makes contemporary local data extremely important, and identification of pathogens locally recovered from blood cultures of febrile neutropenic patients and the patterns of their antibiotic susceptibilities are essential in making therapeutic decisions (Sigurdardottir et al., 2005).
The purpose of this study is to evaluate the epidemiology of bacteremia occurring during neutropenia in adult cancer chemotherapy patients in a university hospital in Lebanon, with a special emphasis on the prevalence, susceptibility profile and risk factors associated with bacteremia caused by third generation cephalosporin-resistant (3GCR) and carbapenem-resistant bacteria.
Materials and Methods
Setting, Patients and Study Design
This is retrospective study performed at Makassed General Hospital, a 200-bed university hospital in Beirut, Lebanon. The hospital's Institutional Review Board approved the study, and an informed consent was waived since it was observation. Medical records of patients admitted between October 2009 and January 2012 were reviewed. Seventy-five episodes of bacteremia occurring in 70 hospitalized neutropenic adult patients were recorded.
Adult cancer patients with fever and neutropenia, including those undergoing Hematopoietic Stem Cell Transplantation (HSCT), with positive blood cultures were selected. All positive results of blood cultures with the corresponding antibiogram were checked and recorded from the Microbiology Laboratory log books and computerized laboratory records. Information regarding these episodes were collected and recorded in a specific database from patients' medical records.
Patient characteristics were identified, including age, gender, type of cancer, risk level, recurrence of admissions, duration of neutropenia prior to bacteremia, hospital stay prior to bacteremia, presence of a focus of infection, presence of a central line or an implantable venous access, outcome, sepsis, intubation, HSCT, antibiotic and antifungal intake in the hospital setting. Univariate analysis of these characteristics was used to identify risk factors for3GCR and multi-drug resistant (MDR) organism-associated bacteremia.
Definitions and Inclusion Criteria
Patients were included if they met all three of the following inclusion criteria:
(1) Fever, defined as a single oral temperature of 38.3°C or an oral temperature of 38°C lasting 1 h or more.
(2) Neutropenia, defined as a neutrophil count of <500 cells/mm3, or a count of <1000 cells/mm3 with a documented decrease to <500 cells/mm3 within the following 48–72 h.
(3) Receipt of chemotherapy prior to the episode of febrileneutropenia.
Patients who had fever and neutropenia as a result of their underlying disease without having received chemotherapy were excluded.
In Lebanon, anaerobic cultures are performed only in reference laboratories. Hospital-based laboratories perform only aerobic cultures. According to hospital policy, one set of blood cultures consists of two bottles of aerobic cultures taken from two different draws at the same time, with no bottles for anaerobic culture. Bacteremia is defined as isolation of the same bacterial or pathogen from at least one set of blood cultures (2 bottles taken at the same time). Bacteremia is considered polymicrobial if at least two organisms from the same blood culture on two occasions are isolated or more than one organism each in at least two separate blood cultureswithin 48 h (Reuben et al., 1989). Bacteremia occurring more than 14 days after a previous episode and separated by repeatedly negative blood cultures was considered a separate episode. Each separate hospital admission for febrile neutropenia was defined as one episode. Subsequent hospital admissions for febrile neutropenia in the same patient were included as separate cases.
Bacteremia caused by a potential skin contaminant (such as coagulase-negative staphylococci, Bacillus, or Corynebacterium species) was considered significant only if it met the following criteria:
(1) Growth of the same bacterial strainin two blood cultures taken from two different sites at the same time.
(2) Growth of the same bacterial strain in one blood culture and in one other sterile site (urine, cerebrospinal fluid, ascetic fluid, pleural fluid, joint fluid).
(3) Growth of the same bacterial strain in one peripheral blood culture and one blood culture taken from an intravenous catheter where both cultures were taken at the same time.
Interpretive criteria (breakpoints) for susceptible, intermediate, and resistant bacterial isolates were those included in the Clinical and Laboratory Standards Institute guidelines (Clinical and Laboratory Standards Institute, 2010).
The 3GCR Enterobacteriaceae phenotypes included all isolates not susceptible to one or more of five agents including aztreonam, cefotaxime, ceftizoxime, ceftazidime, and ceftriaxone (Clinical and Laboratory Standards Institute, 2010). These isolates were, however, susceptible to imipenem.
Many different definitions for multidrug resistance are used in the medical literature to characterize different patterns of resistance in healthcare-associated, antimicrobial-resistant bacteria (Magiorakos et al., 2012).However, generally speaking, MDR-Gram negative bacteria are resistant to key antimicrobial agents (Siegel et al., 2007; Hidron et al., 2008). Third and fourth generation cephalosporins, along with fluoroquinolones, aminoglycosides, and carbapenems, constitute the major therapeutic options in treatment guidelines of febrile neutropenia in adult cancer patients (Freifeld et al., 2011; Averbuch et al., 2013). In this study, gram-negative bacteria were considered MDR when resistant to third and fourth generation cephalosporins, fluoroquinolones, aminoglycosides and carbapenems, including S. maltophilia, carbapenem-resistant P. aeruginosa and Acinetobacter baumannii, or carbapenem-resistant 3GCR Enterobacteriaceae.
Statistical Analysis
Data were reported as the mean standard deviation (SD) or number of patients (percentage). T-tests (two-tailed), Fisher's exact tests and Chi-square tests were used to assess any significant differencesamong the groups. P < 0.05 were considered statistically significant.
Results
During the study period, 75 episodes of bacteremia occurring in 70 hospitalized neutropenic adult patients with hematological malignancies, including those undergoing HSCT, were recorded. Epidemiological and clinical characteristics of the patients, antibiotic treatment, and patient outcomes are shown in Table 1.
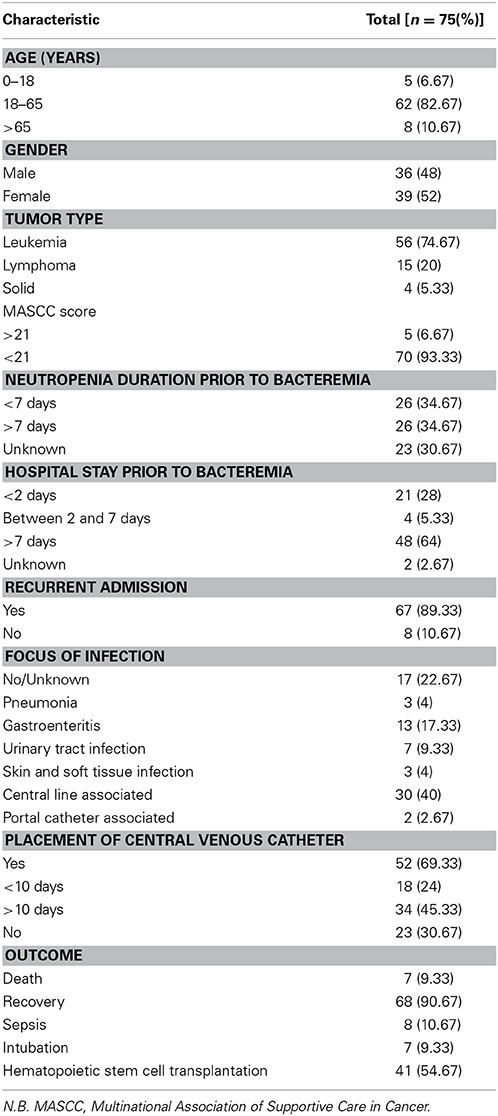
Table 1. Epidemiological and clinical characteristics of all episodes of bacteremia.
Of the 75 bacteremias, 42.7% were due to gram-positive organisms, and the remaining 57.3% were gram-negative. Gram-positive bacteremias were mostly due to methicillin-resistant coagulase negative staphylococci, which represented 66% of gram-positive bacteremias and 28% of total bacteremias. No methicillin-resistant Staphylococcus aureus-related bacteremia was detected and only one episode of methicillin-sensitive Staphylococcus aureus-related bacteremia was observed. (Refer to Tables 2, 3).
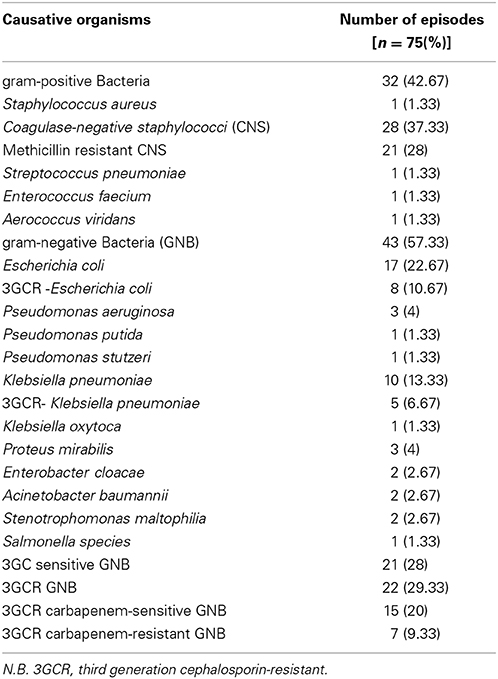
Table 2. Causative organisms of all episodes of bacteremia.
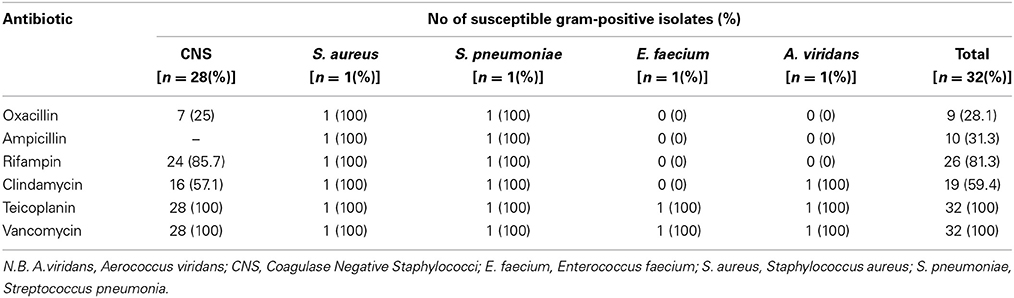
Table 3. Antibiotic susceptibility profile of isolated gram-positive bacteria.
Among the gram-negative bacteremias, Escherichia coli (22.7% of total, 39.5% of gram-negative) and Klebsiella pneumonia (13.3% of total, 23.3% of gram-negative) were the most important causative agents. Out of the 17 bacteremias caused by E. coli, eight were due to 3GCR resistant strains (10.7% of total bacteremias and 47% of E. coli strains). From those caused by K. pneumoniae (10 bacteremias), five cases were due to 3GCR strains (6.7% of total bacteremia and 50% of K. pneumoniae). In general, 28% of the total bacteremias were due to 3GC sensitive gram-negative bacteria and 29.3% of the total bacteremias were caused by 3GC resistant gram-negative bacteria. Concerning carbapenem susceptibility in the 3GC resistant category, seven cases were carbapenem-resistant, representing 9.3% of total bacteremias. (Refer to Tables 2, 4).
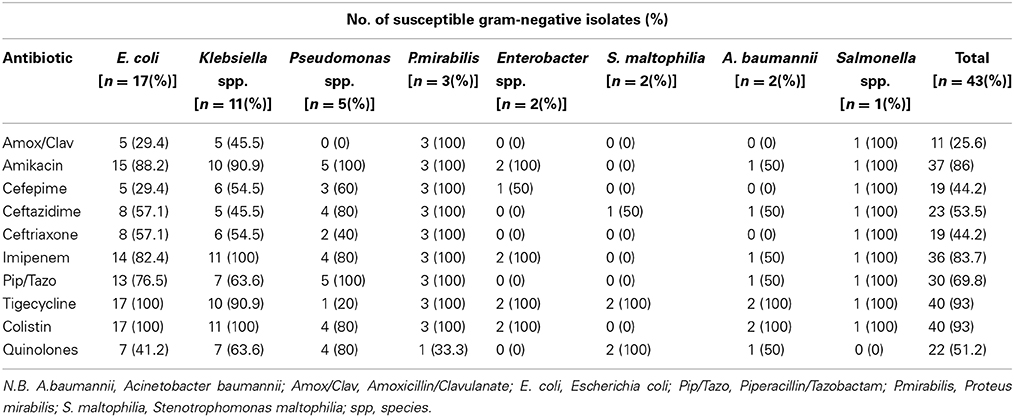
Table 4. Antibiotic susceptibility profile of isolated gram-negative bacteria.
Results of the univariate analysis of factors potentially associated with 3GCR bacteremia, including baseline and demographic characteristics, major disease and risk, hospitalization prior to bacteremia, recurrent admissions, neutropenia prior to bacteremia, presence of CVC, and focus of infection, did not show any statistical significance, suggesting that the former factors were not risk factors. However, history and duration of antibiotic intake before the episode of bacteremia was majorly implicated in the occurrence of 3GCR bacteremia. The type of broad spectrum antibiotic use did not affect the results; butduration of intake did affect results. The use of carbapenems, piperacillin/tazobactam, or 3rd or 4th GC ± aminoglycosides for more than 4 days prior to the bacteremic episode was significantly associated with 3GCR bacteremia compared with all other types of bacteremias. (P < 0.01) A worse outcome, defined by need for intubation and the occurrence of sepsis in bacteremic patients, was also statistically significant in the 3GCR group compared with the other groups. (P < 0.03) (Refer to Tables 5, 6).
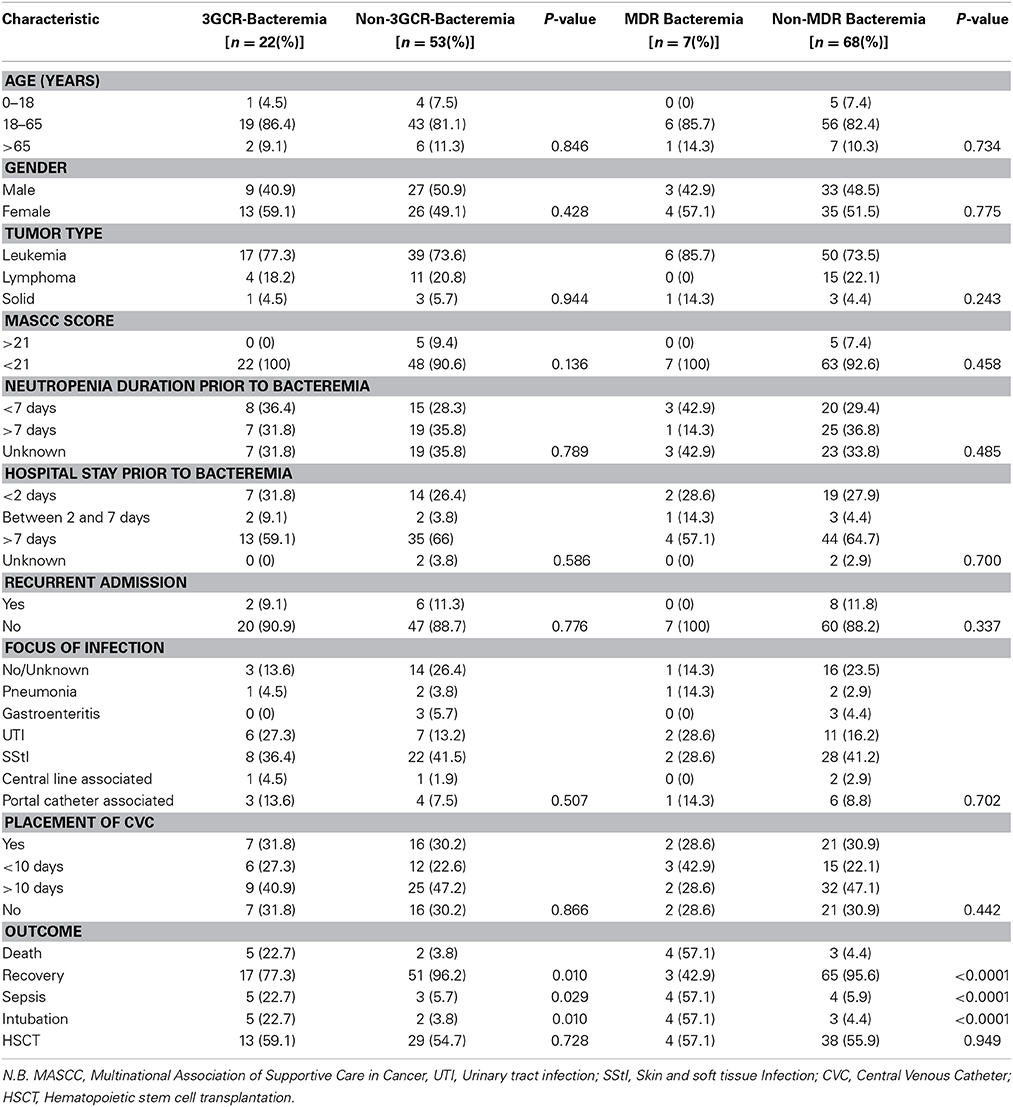
Table 5. Baseline and demographic characteristics, clinical features, and outcome of patients with 3GCR-bacteremia compared with non-3GCR-bacteremia and MDR-bacteremia compared with non-MDR-bacteremia.
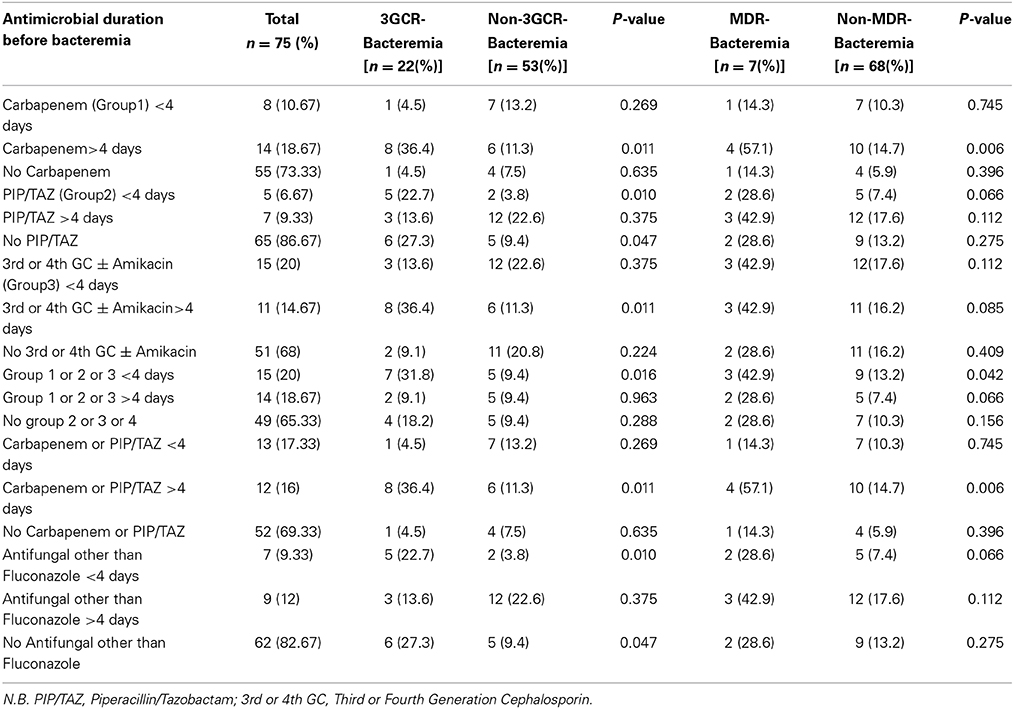
Table 6. Antimicrobial history and duration prior to bacteremia in all cases, in patients with 3GCR- bacteremia compared with non-3GCR-bacteremia and in MDR-bacteremiacompared with non-MDR-bacteremia.
Similarly, infection with an MDR strain was associated with significantly higher rates of subsequent intubation, sepsis, and mortality. (P < 0.03) The history and duration of antibiotic intake before the episode of bacteremia was significantly associated with the occurrence of MDR bacteremia as well. The use of cephalosporins ± aminoglycosides was not significantly associated with MDR bacteremia, while the use of carbapenems or piperacillin/tazobactam for more than 4 days prior to MDR-bacteremia was significantly associated with its occurrence. (P < 0.04) (Refer to Tables 5, 6).
Discussion
Data from Lebanon in neutropenic patients is scarce, and the available literature reveals the dynamic nature of the etiology of bacteremias with time. Previous studies from Lebanon have shown gram-negative organisms to be the predominant agents in febrile neutropenic patients (Hamzeh et al., 2000; Kanafani et al., 2007). In addition to the subdivision between gram-positive and gram-negative organisms, we investigated antibiotic susceptibility patterns and the risk factors associated with bacteremia caused by antibiotic-resistant gram-negative organisms.
In this study, the distribution of the 75 cases was almost equal between gram-positive and gram-negative organisms (42.7 vs. 57.3%). Yet, a study by Kanafani et al. (2007) in 2007 from Lebanon showed gram-negative predominance in febrile neutropenia bacteremic episodes. Gram-negative organisms were responsible for 78.8% of bloodstream infections compared with 33.3% gram-positive organisms (Kanafani et al., 2007).
In fact, the shift from a preponderance of gram-negative bacteria causing bloodstream infections in febrile neutropenic patients to gram-positive bacteria has been observed worldwide. The widespread use of indwelling catheters, early-generation fluoroquinolone prophylaxis, and broad spectrum empirical anti-gram-negative antibacterial therapy led to an increase in the incidence of gram-positive pathogens in the 1980s and 1990s (Zinner, 1999; Ramphal, 2004; Freifeld et al., 2011). Thereafter, the most common bacterial etiologic agent isolated from blood cultures in most centers was reported to be coagulase-negative staphylococci (Dettenkofer et al., 2003; Wisplinghoff et al., 2003b; Freifeld et al., 2011). In our study, coagulase-negative staphylococci were the most common among gram-positive organisms (37.3% of total cases, 87.5% of gram-positive cases), where methicillin-resistant coagulase-negative staphylococciisolatesrepresented 28% of the total cases and 65.6% of gram-positive cases.
Our results showed that E. coli and K. pneumoniae were the most prevalent gram-negative organisms, representing 22.7 and 13.3%, respectively, of total cases. A systematic literature review conducted by Trecarichi and Tumbarello (2014) from January 2007 to August 2013 examined the recent trends in epidemiology and antimicrobial resistance in gram-negative bacteria recovered from cancer patients, with a particular emphasis on the impact of antimicrobial resistance on the clinical outcome of severe infections caused by such microorganisms. The gram-negative bacterial species most frequently isolated were E. coli, whose frequency ranged from 10.1 to 53.6% (mean 32.1%), and K. pneumoniae, which was isolated with a frequency ranging from 4.1 to 44.6% (mean 19.5%) (Trecarichi and Tumbarello, 2014).
In our study, 3GCR strains of E. coli and K. pneumoniae caused 10.7 and 6.7% of total bacteremias, respectively. 3GCR-Enterobacteriaceae colonization or infection of patients with febrile neutropenia has been reported with increased frequency during the last decade. Bloodstream infections due to 3GCR E. coli isolates have been reported with a frequency ranging from 12 to 75% (mean 35%) in cancer patients. 3GCR K. pneumoniae isolates causing BSIs in neutropenic patients have been reported with a frequency ranging from 3 to 66.6% (mean 37.8%) (Trecarichi and Tumbarello, 2014).
We found that 9.3% of episodes of bacteremia in cancer patients were caused by MDR gram-negative bacteria. This finding is in line with recent studies, which report an increase in antibiotic resistance among gram-negative bacteria in immunocompromised hosts. One study performed in Italy by Gudiol et al. (2011) reported an incidence of 13.7% of MDR gram-negative associated bacteremia, andin another study performed in Pakistan by Irfan et al. (2008), the emergence of carbapenem resistance was reported in Pseudomonas species (20.7% of the isolates) and in Acinetobacter species (65.4% of the isolates). In another study by Trecarichi et al. (2011) from Italy, among 38 patients diagnosed with P. aeruginosa bacteremia, 27 were MDR species (71.1%). The percentages of in vitro resistance to major antimicrobial classes were the following: carbapenems (imipenem and meropenem) 60%, antipseudomonal cephalosporins (ceftazidime and cefepime) 42%, and piperacillin 24% (Trecarichi et al., 2011).
The emergence of 3GCR Enterobacteriaceae and MDR gram-negative organisms causing bacteremia in cancer patients is very critical in terms of empiric therapy for febrile neutropenia. Third and fourth generation cephalosporins remain the first line option for primary therapy in febrile neutropenia (Freifeld et al., 2011; Averbuch et al., 2013). In this group of patients, appropriate initial empirical antibiotic therapy is essential, (Gudiol and Carratala, 2014) and empiric antibiotic therapy in febrile neutropenic patients has reduced mortality rates from approximately 21% (Viscoli et al., 2005) to 2–10%, (Vidal et al., 2004; Toussaint et al., 2006) depending upon the underlying diagnosis, degree of cancer control, duration of severe neutropenia and type of infection. Inappropriate empiric therapy is defined, in context, as not including at least one antibiotic active in vitro against the infecting microorganism(s) (Freifeld et al., 2011; Averbuch et al., 2013), and the emergence of 3GCR and MDR organisms in febrile neutropenia renders 3rd or 4th GCs inappropriate choices in certain situations.
Our results showed that the use of broad spectrum antibiotics, including carbapenems, piperacillin/tazobactam, and 3rd or 4th GC ± aminoglycosides, for more than 4 days prior to bacteremia was significantly associated with 3GCR bacteremia. (P < 0.01) However, in the case of carbapenem-resistant 3GCR bacteremia (MDR), the use of carbapenems or piperacillin/tazobactam, but not cephalosporins, for more than 4 days prior to MDR-bacteremia was significantly associated with its occurrence. (P < 0.04) (Refer to Table 6) Previous antibiotic therapy has been recognized as a major risk factor for the development of bacterial resistance. In prospective study involving13 Brazilian HSCT centers (Oliveira et al., 2007), 22% of 91 episodes of bacteremia were MDR-gram-negative in origin. Previous exposure to third generation cephalosporins either as prophylaxis or empirical therapy and belonging to one of the HSCT centers were associated with an increased risk for ESBL-producing Enterobacteriaceae (Oliveira et al., 2007). Another retrospective case-control study involving HSCT recipients (Garnica et al., 2009) showed by univariate analysis that previous use of a third or fourth-generation cephalosporin (P = 0.005 and 0.02, respectively) and duration of antibiotic use (P < 0.001) were among the factors associated with bacteremia due to MDR-gram-negative isolates including K. pneumonia and P. aeruginosa. In another study performed in the United States by Rangaraj et al. (2010), the use of multiple broad spectrum antibiotics compared with no antimicrobial agents was significantly associated with isolation of MDR P. aeruginosa (8.2 vs. 0.7%, p < 0.005). This finding is consistent with a more recent study in 2013 by Satlin et al. (2013), where exposure to any broadspectrum antibacterial agent may be sufficient to increase the risk of carbapenem-resistant Enterobacteriaceae acquisition and cause bloodstream infections in patients with hematologic malignancies.
Our results showed that patient outcome was influenced significantly by antimicrobial resistance, and the risk ofsubsequent intubation, sepsis and mortality were high in the 3GC-resistant bacteremia group and in the MDR-bacteremia group compared with patients having other bacteremias(P < 0.03). (Refer to Table 5) Other studies indicated that a dramatic increase in the detection rate of MDR gram-negative bacteremia compared with previous periods was associated with increased morbidity, mortality, and cost, especially in patients with hematological diseases (Lodise et al., 2007). Moreover, mortality was independently associated with inadequate initial antimicrobial treatment in the case of antibiotic-resistant bacteremia (Giske et al., 2008). Thus, local monitoring of bacterial isolates is recommended to adapt initial empiric antibiotic therapy based on the local prevalence of MDR strains (Caselli et al., 2010).
Our study has at least two major limitations. The first is that the samples were collected from a single medical center; therefore, results could not be generalized to other medical centers in Lebanon because the microbial ecology differs from one center to another. The second limitation is that the small sample size did not allow us to perform a multivariate analysis and limited our statistical analysis to a univariate model.
Conclusion
In conclusion, our data showed equal occurrence of gram-negative and gram-positive organisms causing bacteremia in febrile neutropenic cancer patients in our center. We found that bacteremia caused by gram-negative antimicrobial resistant strains is common among cancer patients, especially in those exposed to antibiotic pressure. Emergence of resistance to third and fourth generation cephalosporins and, to a lesser extent, to carbapenems, in gram-negative isolates has to be considered seriously in our local guidelines for empiric treatment of febrile neutropenia, especially given that their occurrence was associated with poorer clinical outcomes.
The empiric use of broad spectrum antibiotics in febrile neutropenia is very critical. On the one hand, it is crucial to decrease mortality during the febrile episode; on the other hand, it is a risk factor for emergence bacteremia with resistant organisms. In our therapeutic guidelines for the management of febrile neutropenia, we should include coverage for MDR bacteria in patients who have persistent or relapsing fever after 4 days of initial empiric therapy.
Author Contributions
All authors have contributed equally to the analysis and interpretation of the study data as well as to the drafting of the article, but Rima Moghnieh made the primary contribution to the conception and design of the study and revising the draft critically for important intellectual contentand Nour Estaitieh to the acquisition and collection of data. All authors gave the final approval of the article to be sent for publication and agreed to be accountable for all aspects of the paper in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Averbuch, D., Orasch, C., Cordonnier, C., Livermore, D. M., Mikulska, M., Viscoli, C., et al. (2013). ECIL4, a joint venture of EBMT, EORTC, ICHS, ESGICH/ESCMID and ELN. European guidelines for empirical antibacterial therapy for febrile neutropenic patients in the era of growing resistance: summary of the 2011 4th European Conference on Infections in Leukemia. Haematologica 98, 1826–1835. doi: 10.3324/haematol.2013.091025
Caselli, D., Cesaro, S., Ziino, O., Zanazzo, G., Manicone, R., Livadiotti, S., et al. (2010). Multidrug resistant Pseudomonas aeruginosa infection in children undergoing chemotherapy and hematopoietic stem cell transplantation. Haematologica 95, 1612–1615. doi: 10.3324/haematol.2009.020867
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Clinical and Laboratory Standards Institute (CLSI) (2010). Performance Standards for Antimicrobial Susceptibility Testing: 20th Informational Supplement. Wayne, PA: CLSI.
Dettenkofer, M., Ebner, W., Bertz, H., Babikir, R., Finke, J., Frank, U., et al. (2003). Surveillance of nosocomial infections in adult recipients of allogeneic and autologous bone marrow and peripheral blood stem-cell transplantation. Bone Marrow Transplant. 31, 795–801. doi: 10.1038/sj.bmt.1703920
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Freifeld, A. G., Bow, E. J., Sepkowitz, K. A., Boeckh, M. J., Ito, J. I., Mullen, C. A., et al. (2011). Infectious diseases society of america clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america. Clin. Infect. Dis. 52, 427–431. doi: 10.1093/cid/ciq147
Garnica, M., Maiolino, A., and Nucci, M. (2009). Factors associated with bacteremia due to multidrug-resistant Gram-negative bacilli in hematopoietic stem cell transplant recipients. Braz. J. Med. Biol. Res. 42, 89–93. doi: 10.1590/S0100-879X2009000300010
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Giske, C. G., Monnet, D. L., Cars, O., and Carmeli, Y. (2008). ReAct-action on antibiotic resistance clinical and economic impact of common multidrug-resistant gram-negative bacilli. Antimicrob. Agents Chemother. 52, 813–821. doi: 10.1128/AAC.01169-07
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Gudiol, C., and Carratala, J. (2014). Antibiotic resistance in cancer patients. Expert Rev. Anti. Infect. Ther. 12, 1003–1016. doi: 10.1586/14787210.2014.920253
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Gudiol, C., Tubau, F., Calatayud, L., Garcia-Vidal, C., Cisnal, M., Sánchez-Ortega, I., et al. (2011). Bacteraemia due to multidrug-resistant Gram-negative bacilli in cancer patients: risk factors, antibiotic therapy and outcomes. J. Antimicrob. Chemother. 66, 657–663. doi: 10.1093/jac/dkq494
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Hamzeh, F., Kanj, S. S., and Uwaydah, M. (2000). Febrile neutropenia in cancer patients in a tertiary care medical center in Lebanon: microbial spectrum and outcome. J. Med. Liban. 48, 136–142
Hidron, A. I., Edwards, J. R., Patel, J., Horan, T. C., Sievert, D. M., Pollock, D. A., et al. (2008). NHSN annual update: antimicrobial-resistant pathogens associated with healthcare-associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007. Infect. Control Hosp. Epidemiol. 29, 996–1011. doi: 10.1086/591861
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Irfan, S., Idrees, F., Mehraj, V., Habib, F., Adil, S., and Hasan, R. (2008). Emergence of carbapenem resistant gram negative and vancomycin resistant gram positive organisms in bacteremic isolates of febrile neutropenic patients: a descriptive study. BMC Infect. Dis. 8:80. doi: 10.1186/1471-2334-8-80
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Jones, R. N. (1999). Contemporary antimicrobial susceptibility pattern of bacterial pathogens commonly associated with febrile patients with neutropenia. Clin. Infect. Dis. 29, 495–502. doi: 10.1086/598621
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Kanafani, Z. A., Dakdouki, G. K., El-Chammas, K. I., Eid, S., Araj, G. F., and Kanj, S. S. (2007). Bloodstreaminfections in febrile neutropenicpatients at a tertiary care center in Lebanon: a view of the past decade. Int. J. Infect. Dis. 11, 450–453. doi: 10.1016/j.ijid.2006.12.008
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Lodise, T. P. Jr., Patel, N., Kwa, A., Graves, J., Furuno, J. P., Graffunder, E., et al. (2007). Predictors of 30-day mortality among patients with Pseudomonasaeruginosa bloodstream infections: impact of delayed appropriate antibiotic selection. Antimicrob. Agents Chemother. 51, 3510–3515. doi: 10.1128/AAC.00338-07
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Magiorakos, A. P., Srinivasan, A., Carey, R. B., Carmeli, Y., Falagas, M. E., Giske, C. G., et al. (2012). Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 18, 268–281. doi: 10.1111/j.1469-0691.2011.03570.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Montassier, E., Batard, E., Gastinne, T., Potel, G., and de La Cochetière, M. F. (2013). Recent changes in bacteremia in patients with cancer: a systematic review of epidemiology and antibiotic resistance. Eur. J. Clin. Microbiol. Infect. Dis. 32, 841–850. doi: 10.1007/s10096-013-1819-7
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Oliveira, A. L., Souza, M., Carvalho-Dias, V. M., Ruiz, M. A., Silla, L., Tanaka, P. Y., et al. (2007). Epidemiology ofbacteremia and factors associated with multi-drug-resistantGram-negative bacteremia in hematopoietic stem cell transplant recipients. Bone Marrow Transplant. 39, 775–781. doi: 10.1038/sj.bmt.1705677
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Pagano, L., Caira, M., Rossi, G., Tumbarello, M., Fanci, R., Garzia, M. G., et al. (2012). Hema e-Chart Group, Italy. A prospective survey of febrile events in hematological malignancies. Ann. Hematol. 91, 767–774. doi: 10.1007/s00277-011-1373-2
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Ramphal, R. (2004). Changes in the etiology of bacteremia in febrile neutropenic patients and the susceptibilities of the currently isolated pathogens. Clin. Infect. Dis. 39, S25–S31. doi: 10.1086/383048
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Rangaraj, G., Granwehr, B. P., Jiang, Y., Hachem, R., and Raad, I. (2010). Perils of quinolone exposure in cancer patients: breakthrough bacteremia with multidrug-resistant organisms. Cancer 116, 967–973. doi: 10.1002/cncr.24812
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Reuben, A. G., Musher, D. M., Hamill, R. J., and Broucke, I. (1989). Polymicrobial bacteremia: clinical and microbiologic patterns. Rev. Infect. Dis. 11, 161–183.
Satlin, M. J., Calfee, D. P., Chen, L., Fauntleroy, K. A., Wilson, S. J., Jenkins, S. G., et al. (2013). Emergence of carbapenem-resistant Enterobacteriaceae as causes of bloodstream infections in patients with hematologic malignancies. Leuk. Lymphoma 54, 799–806. doi: 10.3109/10428194.2012.723210
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Siegel, J. D., Rhinehart, E., Jackson, M., and Chiarello, L. (2007). Management of multidrug- resistant organisms in health care settings, 2006. Am. J. Infect. Control 35(Suppl 2): 165–193. doi: 10.1016/j.ajic.2007.10.006
Sigurdardottir, K., Digranes, A., Harthug, S., Nesthus, I., Tangen, J., Dybdahl, B., et al. (2005). A multi-centre prospective study of febrile neutropenia in Norway: microbiological findings and antimicrobial susceptibility. Scand. J. Infect. Dis. 37, 455–464. doi: 10.1080/00365540510038497
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Toussaint, E., Bahel-Ball, E., Vekemans, M., Georgala, A., Al-Hakak, L., Paesmans, M., et al. (2006). Causes of fever in cancer patients (prospective study over 477 episodes). Support Care Cancer 14, 763–769. doi: 10.1007/s00520-005-0898-0
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Trecarichi, E. M., and Tumbarello, M. (2014). Antimicrobial-resistant Gram-negative bacteria in febrile neutropenic patients with cancer: current epidemiology and clinical impact. Curr. Opin. Infect. Dis. 27, 200–210. doi: 10.1097/QCO.0000000000000038
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Trecarichi, E. M., Tumbarello, M., Caira, M., Candoni, A., Cattaneo, C., Pastore, D., et al. (2011). Multidrug resistant Pseudomonas aeruginosa bloodstream infection in adult patients with hematologic malignancies. Haematologica 96, e1–e3 doi: 10.3324/haematol.2010.036640
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Tumbarello, M., Trecarichi, E. M., Caira, M., Candoni, A., Pastore, D., Cattaneo, C., et al. (2012). He.M.A.B.I.S. (Hematological Malignancies Associated Bacterial Infections Surveillance) Italy. Derivation and validation of a scoring system to identify patients with bacteremia and hematological malignancies at higher risk for mortality. PLoS ONE 7:e51612. doi: 10.1371/journal.pone.0051612
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Vidal, L., Paul, M., Ben-Dor, I., Pokroy, E., Soares-Weiser, K., and Leibovici, L. (2004). Oral versus intravenous antibiotic treatment for febrile neutropenia in cancer patients: a systematic review and meta-analysis of randomized trials. J. Antimicrob. Chemother. 54, 29–37. doi: 10.1093/jac/dkh303
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Viscoli, C., Varnier, O., and Machetti, M. (2005). Infections in patients with febrile neutropenia: epidemiology, microbiology, and risk stratification. Clin. Infect. Dis. 40(Suppl. 4), S240–S245. doi: 10.1086/427329
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Wisplinghoff, H., Cornely, O. A., Moser, S., Bethe, U., Stützer, H., Salzberger, B., et al. (2003a). Outcomes of nosocomial bloodstream infections in adult neutropenic patients: a prospective cohort and matched case—control study. Infect. Control Hosp. Epidemiol. 24, 905–911. doi: 10.1086/502158
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Wisplinghoff, H., Seifert, H., Wenzel, R. P., and Edmond, M. B. (2003b). Current trends in the epidemiology of nosocomial bloodstream infections in patients with hematological malignancies and solid neoplasms in hospitals in the United States. Clin. Infect. Dis. 36, 1103–1110. doi: 10.1086/374339
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Wu, H. S., Kuo, S. C., Lee, Y. T., Yang, Y. S., Cheng, S. S., Chen, T. L., et al. (2012). Clinical characteristics and prognostic factors of Acinetobacternosocomialbacteraemia in patients with solid tumors. Clin. Microbiol. Infect. 18, E373–E376. doi: 10.1111/j.1469-0691.2012.03927.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Zinner, S. H. (1999). Changing epidemiology of infections in patients with neutropenia and cancer: emphasis on gram-positive and resistant bacteria. Clin. Infect. Dis. 29, 490–494. doi: 10.1086/598620
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Keywords: febrile neutropenia, bacteremia, 3GCR gram-negative bacteria, MDR gram-negative bacteria, Lebanon
Citation: Moghnieh R, Estaitieh N, Mugharbil A, Jisr T, Abdallah DI, Ziade F, Sinno L and Ibrahim A (2015) Third generation cephalosporin resistant Enterobacteriaceae and multidrug resistant gram-negative bacteria causing bacteremia in febrile neutropenia adult cancer patients in Lebanon, broad spectrum antibiotics use as a major risk factor, and correlation with poor prognosis. Front. Cell. Infect. Microbiol. 5:11. doi: 10.3389/fcimb.2015.00011
Received: 13 November 2014; Accepted: 17 January 2015;
Published online: 12 February 2015.
Edited by:
Ghassan M. Matar, American University of Beirut, LebanonReviewed by:
Charles Martin Dozois, Institut National de la Recherche Scientifique, CanadaMax Maurin, Université Aix-Marseille II, France
Copyright © 2015 Moghnieh, Estaitieh, Mugharbil, Jisr, Abdallah, Ziade, Sinno and Ibrahim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rima Moghnieh, Department of Internal Medicine, Makassed General Hospital, PO Box 11-6301 Riad El-Solh, Beirut 1107 2210, Lebanon e-mail:amlakkis@yahoo.com