Myocardial ischemia assessment in chronic kidney disease: challenges and pitfalls
 Susie F. C. Parnham
Susie F. C. Parnham Jonathan M. Gleadle
Jonathan M. Gleadle Carmine G. De Pasquale1,2
Carmine G. De Pasquale1,2  Joseph B. Selvanayagam
Joseph B. Selvanayagam- 1Department of Cardiovascular Medicine, Flinders Medical Centre, Bedford Park, SA, Australia
- 2School of Medicine, Flinders University, Bedford Park, SA, Australia
- 3Department of Renal Medicine, School of Medicine, Flinders University, Bedford Park, SA, Australia
Coronary artery disease is the leading cause of mortality and morbidity in the chronic kidney disease (CKD) population and often presents with atypical symptoms. Current diagnostic investigations of myocardial ischemia in CKD lack sensitivity and specificity or may have adverse effects. We present a case vignette and explore the challenges of diagnostic myocardial stress investigation in patients with CKD.
Case Vignette
A 60-year-old woman with stage 5 chronic kidney disease (CKD) from glomerulonephritis presented with atypical chest discomfort at rest. She is worried about coronary artery disease (CAD). She has hypertension treated with an angiotensin converting enzyme inhibitor and a beta blocker. Her total cholesterol is 5 mmol/L with low-density lipoprotein of 3.2 mmol/L. She has no diabetes mellitus, no family history of premature CAD, and does not smoke. How should she be evaluated?
Clinical Problem
Cardiovascular disease (CVD) is the leading cause of mortality and a major cause of morbidity in the CKD population. Myocardial ischemia is a major cause of death in CKD patients. Myocardial ischemia can be caused by both epicardial and microvascular CAD.
Coronary artery disease is highly prevalent in the CKD population (1) being evident even in early renal disease (2, 3) and in young CKD patients (4). CKD patients have both traditional and non-traditional cardiac risk factors (Table 1).
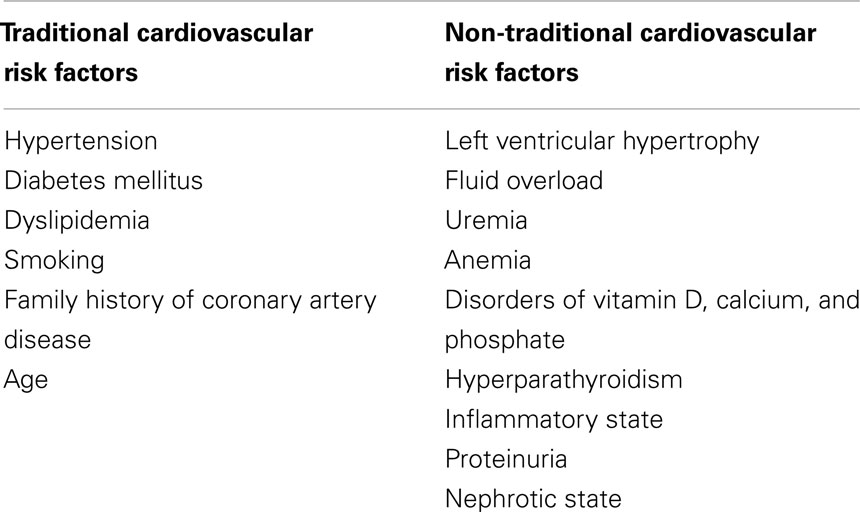
Table 1. Cardiovascular risk factors in the chronic kidney disease population.
In the CKD population, CAD is often multi-vessel and causes silent or asymptomatic myocardial ischemia (5, 6). Asymptomatic epicardial CAD has been detected even in people with early stage CKD (7) and is associated with a higher major adverse cardiac event rate compared to those without CAD (6). While the coronary plaque characteristics in patients with CKD showed no difference in the prevalence of high-risk plaque compared to the group without CKD (8), Kawai et al. showed that patients with mild CKD had higher prevalence of severe epicardial CAD compared to those without CKD (8), thus, suggesting that the problem relates to coronary stenosis rather than plaque stability.
Microvascular CAD is also present in the CKD population. Charytan et al. assessed mild to moderate CKD subjects without diabetes or uncontrolled hypertension using positron emission tomography imaging and found that the CKD cohort had decreased coronary flow reserve (CFR) compared to controls (9). Chade et al. suggested that microvascular dysfunction occurred in early CKD (10). They performed coronary flow wire to the left anterior descending artery using adenosine on early CKD subjects with no angiographically significant CAD and found the CKD subjects had lower CFR compared to normal controls (10). Microvascular CAD has been shown to be associated with reduced survival, although, similar to patients without CKD, the rate of survival is better than for epicardial CAD (11).
Strategies and Evidence
Diagnostic Evaluation
Diagnostic evaluation starts with a thorough clinical history and examination and a baseline 12-lead ECG. Cardiovascular examination, especially to exclude uncontrolled hypertension or significant aortic stenosis is important prior to cardiac stress investigation. Cardiac stress investigations in CKD patients and their limitations are outlined in Table 2.
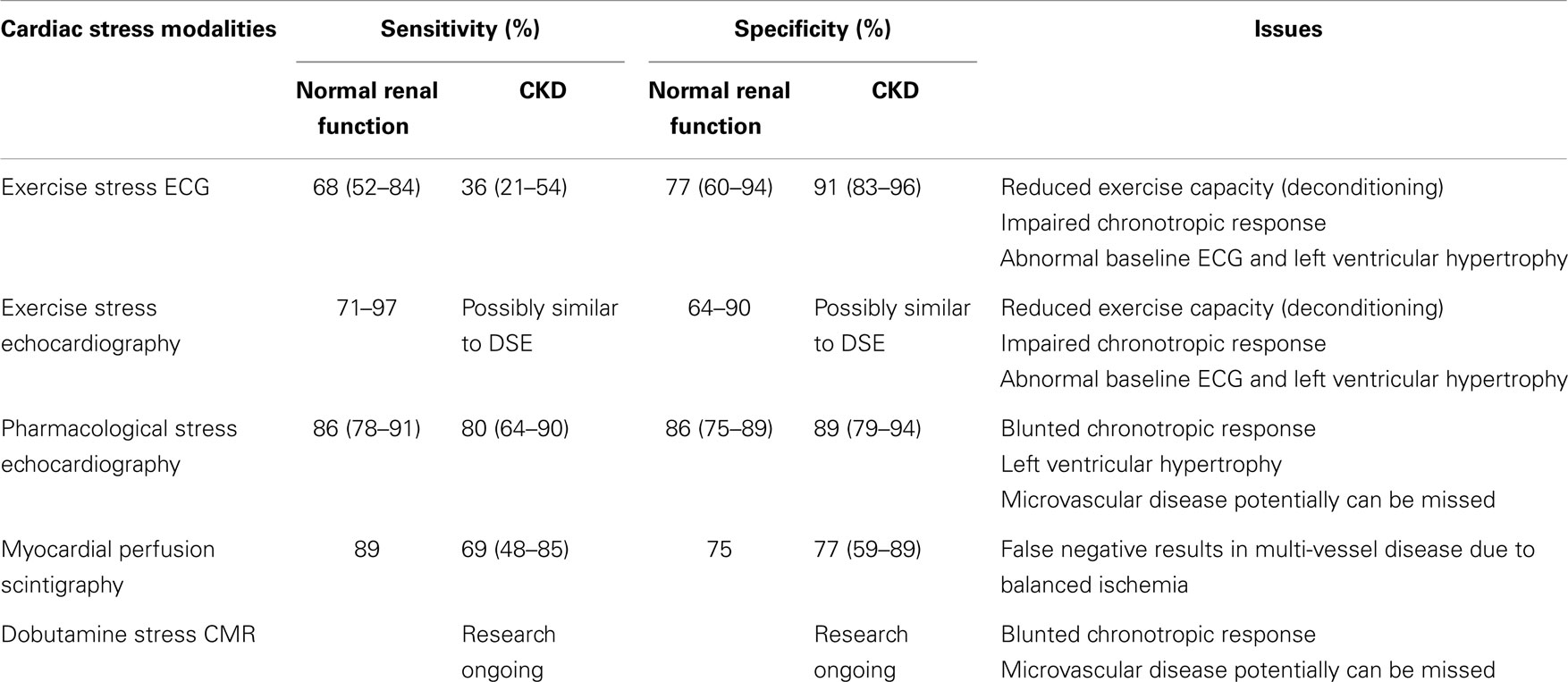
Table 2. Cardiac stress investigations in the normal renal function versus advanced chronic kidney disease (CKD) patients.
Exercise Stress ECG
In patients with normal renal function, exercise stress test (EST) with ECG has a low to moderate sensitivity and specificity, 68 ± 16% and 77 ± 17%, respectively, even when adequate exercise capacity and 85% heart rate is achieved (12). EST is further limited in the advanced CKD population, with poor sensitivity of 36% (13) (especially those undergoing dialysis), as deconditioning leads to reduced exercise capacity (14). Deconditioning can be due to vascular, neurological or musculoskeletal comorbidities, and the catabolic/cachexic metabolic state associated with CKD. CKD patients have also been shown to have impaired heart rate response to exercise (15), and the frequently abnormal baseline ECG in CKD patients (often secondary to hypertension) hampers the interpretation of standard stress testing. In advanced CKD patients, the ST segment changes at stress were shown to be not significantly different between non-severe CAD and severe CAD group, despite a longer treadmill exercise time in the non-severe group (13).
Exercise Stress Echocardiography and Dobutamine Stress Echocardiography
Exercise stress echocardiography (ESE) is better than the standard stress ECG in ruling in CAD (Positive likelihood ratio ESE 7.94 versus EST 3.57) and ruling out CAD (Negative likelihood ratio ESE 0.19 versus EST 0.38) (16). Its sensitivity has been reported ranging from 71 to 97% with specificity ranging from 64 to 90% (17). However, the utility of ESE in CKD population remains limited due to the same physical reasons as EST limitations above.
The addition of echocardiography allows assessment of ventricular size and function, aortic and mitral valvular calcification, left ventricular hypertrophy (LVH), and potentially CFR. CFR measurement by Doppler echocardiography in the left anterior descending artery has been shown to be a determinant of cardiac events in CKD patients in the absence of obstructive epicardial CAD (18), although this is not performed routinely by many echocardiography laboratories due to technical difficulties.
Dobutamine and dipyridamole stress echocardiography (DSE) technique detects inducible myocardial ischemia based on detection of wall motion abnormalities, thus, would detect significant epicardial CAD, not microvascular disease.
A meta analysis in 2008 showed that dipyridamole and dobutamine stress echocardiography had a sensitivity of 85% (confidence interval 80–89) and 86% (confidence interval 78–91), respectively, and a specificity of 89% (confidence interval 82–94) and 86% (confidence interval 75–89), respectively, in detecting myocardial ischemia in the non-renal population (19). It is often recommended as a screening test in advanced CKD patients.
A systematic review in 2011 identified 11 DSE studies with 690 potential renal transplant recipients (19). Overall, DSE had moderate sensitivity of 80% (confidence interval 64–90) in detecting inducible myocardial ischemia in renal transplant candidates (20). Several mechanisms may explain the reduced accuracy of DSE in the advanced CKD population. The majority of advanced CKD patients had a blunted chronotropic response, thus, did not achieve 85% maximal predicted heart rate despite the use of atropine, significantly reducing the sensitivity of DSE in detecting myocardial ischemia (21). The thick myocardium due to LVH with small intracavitary volume, commonly found in CKD patients, obscures the detection of wall motion abnormalities at stress, thus, significantly reducing the sensitivity of stress echocardiography in detecting inducible myocardial ischemia in CKD population. Microvascular CAD is difficult to appreciate given the focus on regional wall motion abnormality and likely to be missed.
Abnormal DSE results in CKD patients have been associated with poorer prognosis for cardiac events and overall mortality (13, 22–24). Bergeron et al. showed that among 485 patients with CKD, the percentage of ischemic segments during DSE was an independent predictor of mortality (22). Negative stress echocardiography results, on the other hand, have been shown to be associated with low incidence of major adverse cardiac events (21).
Blunted chronotropic response with exercise in CKD population may relate to poorer overall cardiac prognosis. A 2012 meta analysis of 11,542 patients showed that submaximal age-predicted heart rate (<85% maximum heart rate) in the setting of normal ESE and DSE had higher cardiovascular risk than those who achieved >85% maximal predicted heart rate (25).
Myocardial Perfusion Scintigraphy
Exercise and pharmacological myocardial perfusion scintigraphy (MPS) have sensitivity of 87 and 89%, and specificity of 73 and 75%, respectively, in detecting >50% coronary artery stenosis in patients without advanced CKD (26). Exercise MPS in the advanced CKD population has the same limitation as EST and ESE, i.e., related to the inadequate exercise performance and chronotropic incompetence (27).
A systematic review in 2011 showed that MPS has sensitivity of 69% (confidence interval 48–85) and specificity of 77% (confidence interval 59–89) in diagnosing inducible myocardial ischemia in the pre-renal transplant population (20). MPS has high false negative result in detecting ischemia in people with significant triple vessel CAD, as in the CKD population, because of homogeneous tracer uptake due to “balanced ischemia” (28, 29).
Normal myocardial perfusion measured by SPECT may not be associated with excellent prognosis in CKD population unlike the normal population (30, 31), perhaps due to the high-false negative result from balanced ischemia. Hakeem et al. showed patients with CKD with normal MPS still had a three times higher cardiac death rate than those with normal MPS and no CKD (31). In addition, concurrent reduced CFR and LVH may play a role. Fukushima et al. reported CKD patients with normal clinical myocardial perfusion by PET scan had reduced global myocardial flow reserve, which implied an underlying microvascular dysfunction in this population (32) that could explain the poorer prognosis. Increased baseline myocardial blood flow and peripheral endothelial dysfunction in CKD patients have been suggested by Koivuviita et al. (33).
Nonetheless, abnormal MPS results in CKD patients have been shown to be associated with a higher incidence of cardiac events and mortality (34–40). A meta analysis of 12 studies of pre-renal transplant patients showed that the presence of reversible defects of inducible myocardial ischemia was associated with sixfold increased risk of myocardial infarction and almost fourfold risk of cardiac death (41). The presence of fixed defects was associated with a nearly fivefold increased risk of cardiac death (41). Joki et al. suggested that myocardial perfusion abnormalities significantly predicted cardiac events in CKD patients independently of eGFR and left ventricular ejection fraction (34). Among 2967 patients with CKD, the incidence of major adverse cardiac events at 1 year was 1.0, 3.9, 5.9, and 7.3% for normal, mild, moderate, and severe summed stress score, respectively (36). Al-Mallah et al. demonstrated that an interaction between renal function and the magnitude of perfusion deficit assessed by stress MPS in patients with moderate and severe CKD in the presence of abnormal MPS (38).
Blunted heart rate response in CKD patients during stress myocardial perfusion imaging has been reported to be associated with increased mortality (42–44).
Cardiovascular Magnetic Resonance
Cardiovascular magnetic resonance (CMR) with gadolinium contrast has not been widely utilized clinically in the CKD population due to the concern of nephrogenic systemic fibrosis (NSF) (45–47). The use of Gadolinium chelates is prohibitive in CKD patients due to the rare but serious side effect of NSF. NSF manifests as a hardening of the skin and internal organs resembling scleroderma, which is irreversible and potentially fatal.
Cardiovascular magnetic resonance spectroscopy has been studied to assess early cardiac dysfunction in pediatric population with advanced CKD (48). Dobutamine stress CMR was shown to be safe in the pre-renal transplant population (49).
Recommendation
Exercise tolerance has utmost importance both for prognosis and symptoms capacity and has implication in the case of peri-operative risk assessment (50), in this case, renal transplantation. Therefore, we recommend ESE to the case vignette described, to exclude inducible myocardial ischemia, inducible arrhythmia, and to assess exercise capacity and symptoms objectively. Resting echocardiography is useful to exclude significant aortic stenosis prior to exercise stress and to visually assess the degree of LVH.
Future Developments
Further research is needed for better diagnostic testing for myocardial ischemia in CKD. A new non-contrast blood oxygen level dependent (BOLD) CMR technique has been utilized in several human studies to assess myocardial oxygenation as a measure of ischemia with promising benefits (51–57), namely, in syndrome X, hypertensive patients, patients with CAD, hypertrophic cardiomyopathy, and aortic stenosis. It detects both epicardial and microvascular CAD without the use of potentially toxic Gadolinium chelate contrast agents. The combination of non-contrast BOLD CMR and non-contrast whole-heart magnetic resonance coronary angiography, which can characterize significant proximal epicardial CAD, has potential for assessing myocardial ischemia in the advanced CKD population. This needs to be tested in prospective studies.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Stack AG, Bloembergen WE. Prevalence and clinical correlates of coronary artery disease among new dialysis patients in the United States: a cross-sectional study. J Am Soc Nephrol (2001) 12(7):1516–23.
2. Joosen IA, Schiphof F, Versteylen MO, Laufer EM, Winkens MH, Nelemans PJ, et al. Relation between mild to moderate chronic kidney disease and coronary artery disease determined with coronary CT angiography. PLoS One (2012) 7(10):e47267. doi: 10.1371/journal.pone.0047267
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
3. Henry RM, Kostense PJ, Bos G, Dekker JM, Nijpels G, Heine RJ, et al. Mild renal insufficiency is associated with increased cardiovascular mortality: the Hoorn Study. Kidney Int (2002) 62(4):1402–7. doi:10.1111/j.1523-1755.2002.kid571.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
4. Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, et al. Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med (2000) 342(20):1478–83. doi:10.1056/NEJM200005183422003
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
5. Ohtake T, Kobayashi S, Moriya H, Negishi K, Okamoto K, Maesato K, et al. High prevalence of occult coronary artery stenosis in patients with chronic kidney disease at the initiation of renal replacement therapy: an angiographic examination. J Am Soc Nephrol (2005) 16(4):1141–8. doi:10.1681/ASN.2004090765
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
6. Hase H, Tsunoda T, Tanaka Y, Takahashi Y, Imamura Y, Ishikawa H, et al. Risk factors for de novo acute cardiac events in patients initiating hemodialysis with no previous cardiac symptom. Kidney Int (2006) 70(6):1142–8. doi:10.1038/sj.ki.5001726
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
7. Cho I, Min HS, Chun EJ, Park SK, Choi Y, Blumenthal RS, et al. Coronary atherosclerosis detected by coronary CT angiography in asymptomatic subjects with early chronic kidney disease. Atherosclerosis (2010) 208(2):406–11. doi:10.1016/j.atherosclerosis.2009.08.040
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
8. Kawai H, Sarai M, Motoyama S, Harigaya H, Ito H, Sanda Y, et al. Coronary plaque characteristics in patients with mild chronic kidney disease. Analysis by 320-row area detector computed tomography. Circ J (2012) 76(6):1436–41. doi:10.1253/circj.CJ-11-1384
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
9. Charytan DM, Shelbert HR, Di Carli MF. Coronary microvascular function in early chronic kidney disease. Circ Cardiovasc Imaging (2010) 3(6):663–71. doi:10.1161/CIRCIMAGING.110.957761
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
10. Chade AR, Brosh D, Higano ST, Lennon RJ, Lerman LO, Lerman A. Mild renal insufficiency is associated with reduced coronary flow in patients with non-obstructive coronary artery disease. Kidney Int (2006) 69(2):266–71. doi:10.1038/sj.ki.5000031
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
11. Lin T, Rechenmacher S, Rasool S, Varadarajan P, Pai RG. Reduced survival in patients with “coronary microvascular disease”. Int J Angiol (2012) 21(2):89–94. doi:10.1055/s-0032-1315799
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
12. Gianrossi R, Detrano R, Mulvihill D, Lehmann K, Dubach P, Colombo A, et al. Exercise-induced ST depression in the diagnosis of coronary artery disease. A meta-analysis. Circulation (1989) 80(1):87–98. doi:10.1161/01.CIR.80.1.87
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
13. Sharma R, Pellerin D, Gaze DC, Gregson H, Streather CP, Collinson PO, et al. Dobutamine stress echocardiography and the resting but not exercise electrocardiograph predict severe coronary artery disease in renal transplant candidates. Nephrol Dial Transplant (2005) 20(10):2207–14. doi:10.1093/ndt/gfi005
14. Schmidt A, Stefenelli T, Schuster E, Mayer G. Informational contribution of noninvasive screening tests for coronary artery disease in patients on chronic renal replacement therapy. Am J Kidney Dis (2001) 37(1):56–63. doi:10.1053/ajkd.2001.20584
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
15. Howden EJ, Weston K, Leano R, Sharman JE, Marwick TH, Isbel NM, et al. Cardiorespiratory fitness and cardiovascular burden in chronic kidney disease. J Sci Med Sport (2014). doi:10.1016/j.jsams.2014.07.005
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
16. Banerjee A, Newman DR, Van den Bruel A, Heneghan C. Diagnostic accuracy of exercise stress testing for coronary artery disease: a systematic review and meta-analysis of prospective studies. Int J Clin Pract (2012) 66(5):477–92. doi:10.1111/j.1742-1241.2012.02900.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
17. Armstrong WF, Zoghbi WA. Stress echocardiography: current methodology and clinical applications. J Am Coll Cardiol (2005) 45(11):1739–47. doi:10.1016/j.jacc.2004.12.078
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
18. Nakanishi K, Fukuda S, Shimada K, Miyazaki C, Otsuka K, Kawarabayashi T, et al. Prognostic value of coronary flow reserve on long-term cardiovascular outcomes in patients with chronic kidney disease. Am J Cardiol (2013) 112(7):928–32. doi:10.1016/j.amjcard.2013.05.025
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
19. Picano E, Molinaro S, Pasanisi E. The diagnostic accuracy of pharmacological stress echocardiography for the assessment of coronary artery disease: a meta-analysis. Cardiovasc Ultrasound (2008) 6:30. doi:10.1186/1476-7120-6-30
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
20. Wang LW, Fahim MA, Hayen A, Mitchell RL, Lord SW, Baines LA, et al. Cardiac testing for coronary artery disease in potential kidney transplant recipients: a systematic review of test accuracy studies. Am J Kidney Dis (2011) 57(3):476–87. doi:10.1053/j.ajkd.2010.11.018
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
21. Tita C, Karthikeyan V, Stroe A, Jacobsen G, Ananthasubramaniam K. Stress echocardiography for risk stratification in patients with end-stage renal disease undergoing renal transplantation. J Am Soc Echocardiogr (2008) 21(4):321–6. doi:10.1016/j.echo.2007.06.004
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
22. Bergeron S, Hillis GS, Haugen EN, Oh JK, Bailey KR, Pellikka PA. Prognostic value of dobutamine stress echocardiography in patients with chronic kidney disease. Am Heart J (2007) 153(3):385–91. doi:10.1016/j.ahj.2006.11.012
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
23. Herzog CA, Marwick TH, Pheley AM, White CW, Rao VK, Dick CD. Dobutamine stress echocardiography for the detection of significant coronary artery disease in renal transplant candidates. Am J Kidney Dis (1999) 33(6):1080–90. doi:10.1016/S0272-6386(99)70145-9
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
24. Marwick TH, Lauer MS, Lobo A, Nally J, Braun W. Use of dobutamine echocardiography for cardiac risk stratification of patients with chronic renal failure. J Intern Med (1998) 244(2):155–61. doi:10.1046/j.1365-2796.1998.00354.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
25. Makani H, Bangalore S, Halpern D, Makwana HG, Chaudhry FA. Cardiac outcomes with submaximal normal stress echocardiography: a meta-analysis. J Am Coll Cardiol (2012) 60(15):1393–401. doi:10.1016/j.jacc.2012.05.041
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
26. Salerno M, Beller GA. Noninvasive assessment of myocardial perfusion. Circ Cardiovasc Imaging (2009) 2(5):412–24. doi:10.1161/CIRCIMAGING.109.854893
27. De Vriese AS, Vandecasteele SJ, Van den Bergh B, De Geeter FW. Should we screen for coronary artery disease in asymptomatic chronic dialysis patients? Kidney Int (2012) 81(2):143–51. doi:10.1038/ki.2011.340
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
28. Bourque JM, Beller GA. Stress myocardial perfusion imaging for assessing prognosis: an update. JACC Cardiovasc Imaging (2011) 4(12):1305–19. doi:10.1016/j.jcmg.2011.10.003
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
29. Lima RS, Watson DD, Goode AR, Siadaty MS, Ragosta M, Beller GA, et al. Incremental value of combined perfusion and function over perfusion alone by gated SPECT myocardial perfusion imaging for detection of severe three-vessel coronary artery disease. J Am Coll Cardiol (2003) 42(1):64–70. doi:10.1016/S0735-1097(03)00562-X
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
30. Furuhashi T, Moroi M, Joki N, Hase H, Minakawa M, Masai H, et al. Prediction of cardiovascular events in pre-dialysis chronic kidney disease patients with normal SPECT myocardial perfusion imaging. J Cardiol (2014) 63(2):154–8. doi:10.1016/j.jjcc.2013.07.011
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
31. Hakeem A, Bhatti S, Dillie KS, Cook JR, Samad Z, Roth-Cline MD, et al. Predictive value of myocardial perfusion single-photon emission computed tomography and the impact of renal function on cardiac death. Circulation (2008) 118(24):2540–9. doi:10.1161/CIRCULATIONAHA.108.788109
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
32. Fukushima K, Javadi MS, Higuchi T, Bravo PE, Chien D, Lautamaki R, et al. Impaired global myocardial flow dynamics despite normal left ventricular function and regional perfusion in chronic kidney disease: a quantitative analysis of clinical 82Rb PET/CT studies. J Nucl Med (2012) 53(6):887–93. doi:10.2967/jnumed.111.099325
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
33. Koivuviita N, Tertti R, Jarvisalo M, Pietila M, Hannukainen J, Sundell J, et al. Increased basal myocardial perfusion in patients with chronic kidney disease without symptomatic coronary artery disease. Nephrol Dial Transplant (2009) 24(9):2773–9. doi:10.1093/ndt/gfp175
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
34. Joki N, Hase H, Kawano Y, Nakamura S, Nakajima K, Hatta T, et al. Myocardial perfusion imaging for predicting cardiac events in Japanese patients with advanced chronic kidney disease: 1-year interim report of the J-ACCESS 3 investigation. Eur J Nucl Med Mol Imaging (2014) 41(9):1701–9. doi:10.1007/s00259-014-2781-z
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
35. Bhatti S, Hakeem A, Dhanalakota S, Palani G, Husain Z, Jacobsen G, et al. Prognostic value of regadenoson myocardial single-photon emission computed tomography in patients with different degrees of renal dysfunction. Eur Heart J Cardiovasc Imaging (2014) 15(8):933–40. doi:10.1093/ehjci/jeu036
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
36. Yoda S, Nakanishi K, Tano A, Kasamaki Y, Kunimoto S, Matsumoto N, et al. Risk stratification of cardiovascular events in patients at all stages of chronic kidney disease using myocardial perfusion SPECT. J Cardiol (2012) 60(5):377–82. doi:10.1016/j.jjcc.2012.06.011
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
37. Okuyama C, Nakajima K, Hatta T, Nishimura S, Kusuoka H, Yamashina A, et al. Incremental prognostic value of myocardial perfusion single photon emission computed tomography for patients with diabetes and chronic kidney disease. Nucl Med Commun (2011) 32(10):913–9. doi:10.1097/MNM.0b013e3283495787
38. Al-Mallah MH, Hachamovitch R, Dorbala S, Di Carli MF. Incremental prognostic value of myocardial perfusion imaging in patients referred to stress single-photon emission computed tomography with renal dysfunction. Circ Cardiovasc Imaging (2009) 2(6):429–36. doi:10.1161/CIRCIMAGING.108.831164
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
39. Hatta T, Nishimura S, Nishimura T. Prognostic risk stratification of myocardial ischaemia evaluated by gated myocardial perfusion SPECT in patients with chronic kidney disease. Eur J Nucl Med Mol Imaging (2009) 36(11):1835–41. doi:10.1007/s00259-009-1165-2
40. Momose M, Babazono T, Kondo C, Kobayashi H, Nakajima T, Kusakabe K. Prognostic significance of stress myocardial ECG-gated perfusion imaging in asymptomatic patients with diabetic chronic kidney disease on initiation of haemodialysis. Eur J Nucl Med Mol Imaging (2009) 36(8):1315–21. doi:10.1007/s00259-009-1110-4
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
41. Rabbat CG, Treleaven DJ, Russell JD, Ludwin D, Cook DJ. Prognostic value of myocardial perfusion studies in patients with end-stage renal disease assessed for kidney or kidney-pancreas transplantation: a meta-analysis. J Am Soc Nephrol (2003) 14(2):431–9. doi:10.1097/01.ASN.0000047560.51444.3A
42. Hage FG, Dean P, Bhatia V, Iqbal F, Heo J, Iskandrian AE. The prognostic value of the heart rate response to adenosine in relation to diabetes mellitus and chronic kidney disease. Am Heart J (2011) 162(2):356–62. doi:10.1016/j.ahj.2011.05.014
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
43. Hage FG, Dean P, Iqbal F, Heo J, Iskandrian AE. A blunted heart rate response to regadenoson is an independent prognostic indicator in patients undergoing myocardial perfusion imaging. J Nucl Cardiol (2011) 18(6):1086–94. doi:10.1007/s12350-011-9429-1
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
44. Venkataraman R, Hage FG, Dorfman TA, Heo J, Aqel RA, de Mattos AM, et al. Relation between heart rate response to adenosine and mortality in patients with end-stage renal disease. Am J Cardiol (2009) 103(8):1159–64. doi:10.1016/j.amjcard.2009.01.007
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
45. Saxena SK, Sharma M, Patel M, Oreopoulos D. Nephrogenic systemic fibrosis: an emerging entity. Int Urol Nephrol (2008) 40(3):715–24. doi:10.1007/s11255-008-9361-8
46. Rydahl C, Thomsen HS, Marckmann P. High prevalence of nephrogenic systemic fibrosis in chronic renal failure patients exposed to gadodiamide, a gadolinium-containing magnetic resonance contrast agent. Invest Radiol (2008) 43(2):141–4. doi:10.1097/RLI.0b013e31815a3407
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
47. Othersen JB, Maize JC, Woolson RF, Budisavljevic MN. Nephrogenic systemic fibrosis after exposure to gadolinium in patients with renal failure. Nephrol Dial Transplant (2007) 22(11):3179–85. doi:10.1093/ndt/gfm584
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
48. Malatesta-Muncher R, Wansapura J, Taylor M, Lindquist D, Hor K, Mitsnefes M. Early cardiac dysfunction in pediatric patients on maintenance dialysis and post kidney transplant. Pediatr Nephrol (2012) 27(7):1157–64. doi:10.1007/s00467-012-2124-x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
49. Ripley DP, Kannoly S, Gosling OE, Hossain E, Chawner RR, Moore J, et al. Safety and feasibility of dobutamine stress cardiac magnetic resonance for cardiovascular assessment prior to renal transplantation. J Cardiovasc Med (Hagerstown) (2014) 15(4):288–94.
50. Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof EL, Fleischmann KE, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol (2007) 50(17):1707–32.
51. Karamitsos TD, Arnold JR, Pegg TJ, Francis JM, Birks J, Jerosch-Herold M, et al. Patients with syndrome X have normal transmural myocardial perfusion and oxygenation: a 3-T cardiovascular magnetic resonance imaging study. Circ Cardiovasc Imaging (2012) 5(2):194–200. doi:10.1161/CIRCIMAGING.111.969667
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
52. Karamitsos TD, Leccisotti L, Arnold JR, Recio-Mayoral A, Bhamra-Ariza P, Howells RK, et al. Relationship between regional myocardial oxygenation and perfusion in patients with coronary artery disease: insights from cardiovascular magnetic resonance and positron emission tomography. Circ Cardiovasc Imaging (2010) 3(1):32–40. doi:10.1161/CIRCIMAGING.109.860148
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
53. Wacker CM, Hartlep AW, Pfleger S, Schad LR, Ertl G, Bauer WR. Susceptibility-sensitive magnetic resonance imaging detects human myocardium supplied by a stenotic coronary artery without a contrast agent. J Am Coll Cardiol (2003) 41(5):834–40. doi:10.1016/S0735-1097(02)02931-5
54. Friedrich MG, Niendorf T, Schulz-Menger J, Gross CM, Dietz R. Blood oxygen level-dependent magnetic resonance imaging in patients with stress-induced angina. Circulation (2003) 108(18):2219–23. doi:10.1161/01.CIR.0000095271.08248.EA
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
55. Beache GM, Herzka DA, Boxerman JL, Post WS, Gupta SN, Faranesh AZ, et al. Attenuated myocardial vasodilator response in patients with hypertensive hypertrophy revealed by oxygenation-dependent magnetic resonance imaging. Circulation (2001) 104(11):1214–7. doi:10.1161/hc3601.096307
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
56. Karamitsos TD, Dass S, Suttie J, Sever E, Birks J, Holloway CJ, et al. Blunted myocardial oxygenation response during vasodilator stress in patients with hypertrophic cardiomyopathy. J Am Coll Cardiol (2013) 61(11):1169–76. doi:10.1016/j.jacc.2012.12.024
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
57. Mahmod M, Francis JM, Pal N, Lewis A, Dass S, De Silva R, et al. Myocardial perfusion and oxygenation are impaired during stress in severe aortic stenosis and correlate with impaired energetics and subclinical left ventricular dysfunction. J Cardiovasc Magn Reson (2014) 16:29. doi:10.1186/1532-429X-16-29
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Keywords: chronic kidney disease, myocardial ischemia, coronary disease, echocardiography, myocardial perfusion imaging
Citation: Parnham SFC, Gleadle JM, De Pasquale CG and Selvanayagam JB (2014) Myocardial ischemia assessment in chronic kidney disease: challenges and pitfalls. Front. Cardiovasc. Med. 1:13. doi: 10.3389/fcvm.2014.00013
Received: 02 November 2014; Paper pending published: 18 November 2014;
Accepted: 07 December 2014; Published online: 19 December 2014.
Edited by:
Nicola Mumoli, ASL 6 Livorno, ItalyReviewed by:
Probal Roy, Concord Hospital, AustraliaRajesh Puranik, Royal Prince Alfred Hospital, Australia
Copyright: © 2014 Parnham, Gleadle, De Pasquale and Selvanayagam. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joseph B. Selvanayagam, Department of Cardiovascular Medicine, Flinders Medical Centre, Bedford Park, SA 5042, Australia e-mail: joseph.selva@health.sa.gov.au