 João Soares Felício*
João Soares Felício* Antônio Maria Silva ConceiçãoFlávia Marques SantosMichelle Masuyo Minami SatoFabíola de Arruda BastosAna Carolina Contente Braga de SouzaCamila Cavalcante KouryJoão Felício Abrahão NetoFranciane Trindade Cunha de MeloCarolina Tavares CarvalhoThaís Pontes ArbageAntonio Bentes de Figueiredo JuniorHana Andrade de Rider BritoMarcelo Oliveira Mourão JúniorFabricio de Souza ResendeAmanda Soares PeixotoKarem Miléo Felício
Antônio Maria Silva ConceiçãoFlávia Marques SantosMichelle Masuyo Minami SatoFabíola de Arruda BastosAna Carolina Contente Braga de SouzaCamila Cavalcante KouryJoão Felício Abrahão NetoFranciane Trindade Cunha de MeloCarolina Tavares CarvalhoThaís Pontes ArbageAntonio Bentes de Figueiredo JuniorHana Andrade de Rider BritoMarcelo Oliveira Mourão JúniorFabricio de Souza ResendeAmanda Soares PeixotoKarem Miléo Felício
- Endocrinology Division, University Hospital João de Barros Barreto, Federal University of Pará, Belém, Brazil
Context: Ultrasound (US)-guided percutaneous ethanol injection (PEI) has been proposed for treatment of benign thyroid nodules (TNs). However, there is no consensus for the optimal amount of ethanol injection, number of applications, and time to re-evaluation in order to achieve maximum volume reduction with minimum adverse effects.
Objective: The purpose of the present study was to analyze the effectiveness of an US-guided PEI protocol to treat solid and mixed TNs based on a new target outcome.
Patients and methods: We performed a prospective study evaluating the results of PEI in 52 patients with benign solid and mixed TNs. The ethanol dose was fixed in 30% of the nodular volume per session. Patients returned 1 month after each session for US re-evaluation. Therapeutic success was defined as volume reduction of at least 30% associated with disappearance of clinical symptoms and a complete esthetic satisfaction reported by the patient.
Results: We performed a mean of 2.8 ± 1.9 PEI sessions, with an average total volume of ethanol injected of 9.1 ± 10.3 ml, and a follow-up time of 10.0 ± 8.7 months. There was a reduction of at least 50% of the initial nodular volume in 33 patients (63.5%). In 11 patients (21.2%), the reduction did not reach 50% (mean reduction of 31 ± 11%), but 6 of them reported esthetically satisfactory results and treatment was stopped. Our therapeutic success rate considering the patients with esthetic improvement was 75%. There were no severe complications.
Conclusion: Our protocol is effective and safe to treat solid and mixed benign TNs based on our established outcome.
Introduction
Thyroid nodules (TNs) are common entities, often detected in clinical practice, with a largely variable prevalence, depending on the diagnostic method (1, 2). Epidemiological studies have shown that 4–7% of women and 1% of men living in iodine-sufficient regions present palpable TNs (3, 4), whereas ultrasound (US) detects nodules in up to 76% of the adult population, with a greater incidence in women and elderly people (5–9).
Most TNs are benign (94–96%) (10, 11) small and remain asymptomatic, being usually managed only by observation and follow-up. A proportion of them, however, may lead to local compressive symptoms or esthetic complaints, due to significant enlargement, requiring specific intervention (1, 12). The best treatment for benign nodules remains uncertain (13). Alternatively to thyroidectomy, the use of non-surgical, image-guided, minimally invasive methods has been proposed (12–14), such as US-guided percutaneous ethanol injection (PEI) (15, 16).
This method has been suggested to be an effective, safe, and inexpensive outpatient procedure for the treatment of benign TNs, leading to reduction of nodular volume, with a low rate of early and late clinical complications (3, 17–29). It has been recommended as the first-line therapy of symptomatic and recurrent thyroid cysts with benign cytology (30), and may also be used in solid nodules, particularly in case of contraindication to or refusal of surgery and radioiodine therapy (2, 31–34). However, a standard US-guided PEI protocol is yet to be established, since there is no consensus definition for the optimal amount of ethanol to be injected, the number of applications, and the intervals between sessions in order to achieve maximum volume reduction with minimum adverse effects.
Most articles in literature have considered a nodule volume reduction of at least 50% as a partial success and more than 90% as a complete outcome (34). It is well known that an established benign thyroid nodule rarely becomes too malignant during the lifelong (35). Therefore, it makes more sense to evaluate the treatment success of this pathology based on disappearance of clinical symptoms and a complete esthetic satisfaction to stop PEI applications, independently of volume percent reduction. Our protocol was based mainly on this idea.
Therefore, the purpose of the present study was to analyze the effectiveness of an US-guided PEI protocol to treat solid and mixed TNs based on that concept of treatment outcome.
Materials and Methods
Study Design and Patients
We performed a prospective study evaluating the results of an original US-guided PEI protocol in patients with solid and mixed TNs at Endocrinology Department of Federal University of Pará, from January 2011 to January 2016. We included 52 patients diagnosed with TNs and normal thyroid function, confirmed to be benign by fine-needle aspiration biopsy (FNAB). Mixed TNs were only included when the solid component was >50% of the nodular volume. All patients presented compressive local symptoms and/or esthetic complaints. Exclusion criteria were the presence of malignancy or suspected malignancy detected by FNAB. Cystics and autonomous TNs were not included. The study was approved by the local ethics committee-University Hospital João de Barros Barreto, Federal University of Pará.
Ultrasound-Guided Percutaneous Ethanol Injection
Patients were placed in a supine position with mild neck extension. After skin sterilization, a 22 gage needle (Becton Dickinson 30 × 7) was inserted through the epidermis to the thyroid pericapsular space under US guidance, reaching the center of the target lesion. Then, 99% ethanol was slowly instilled into the nodule, respecting the patient’s tolerance. Ethanol diffusion through the lesion was monitored as intense echogenicity in real-time observation by US. The procedure was stopped if ethanol leaked out of the nodule or if the patient complained of severe pain. None of 52 patients were dropped out through this procedure, and no cases of severe pain were reported. The procedure was carried out without local anesthesia at the puncture site.
The amount of ethanol injected was equivalent to approximately 30% of the nodule volume, estimated by ultrasonography before each application. The nodular volume (milliliter) was obtained by multiplying the product of the longitudinal, lateral, and anteroposterior axes (centimeter) by the constant 0.52.
In mixed nodules, we removed the liquid portion guided for the US, and the nodular volume was calculated. In cases of septated nodules, the greatest possible liquid part was removed. If patients had a multinodular goiter, treatment was only performed in the dominant nodule. In all alcoholization sessions, the amount of injected ethanol did not exceed 5 ml.
Nodular volume reduction was calculated according to the following formula: [Pretreatment volume (milliliter) − Post-treatment volume (milliliter)] × 100%/Pretreatment volume (milliliter). The PEI sessions were followed by monthly assessments of nodular volume by US, and clinical evaluation.
Therapeutic success was defined as volume reduction of at least 30% associated with disappearance of clinical symptoms and a complete esthetic satisfaction reported by the patient. The procedure was considered ineffective when the nodule did not show significant volume reduction (30%) and the patient did not refer esthetic improvement after at least three sessions of PEI and a follow-up period of at least 6 months.
The new information of our study is a protocol that used ethanol fixed doses, but with shorter periods of re-evaluation by US and consequently more frequent applications based not just in nodule volume. We have also taking in consideration the disappearance of clinical symptoms and a complete esthetic satisfaction to stop PEI applications.
Statistical Analysis
Categorical variables were presented as frequency (percentage). All normally distributed values were given as mean ± SD and all other values were given as median (range). The Wilcoxon test was applied to compare thyroid nodules initial and final volumes. A two-sided p < 0.05 was considered statistically significant. Data were analyzed using Sigma Stat version 3.5 (Jandel Scientific Corporation, Chicago, IL, USA) and Statistical Package for the Social Sciences version 21.0 (IBM, Chicago, IL, USA).
Results
Our study group consisted of 51 women (98%) and 1 man, with a mean age of 45.2 ± 16.6 years. Among TNs, 19 (36, 5%) were mixed and 33 (63, 5%) solid.
We performed a mean of 2.8 ± 1.9 PEI sessions, with an average total volume of ethanol injected of 9.1 ± 10.3 ml, and a follow-up time of 10.0 ± 8.7 months. Data regarding the US evaluation of the TNs before and after treatment are described in Table 1. There was a reduction of at least 50% of the initial nodular volume in 33 patients (63, 5%). In 11 patients (21, 2%), the reduction did not reach 50% (mean reduction of 31 ± 11%). In eight patients (15, 3%), the nodular volume either increased or remained unchanged.
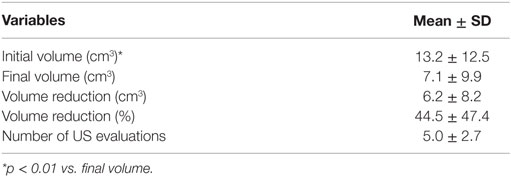
Table 1. US evaluation of the thyroid nodules before and after treatment (n = 52).
Additionally, 6 of the 11 patients who did not achieve 50% of nodular volume reduction reported esthetically satisfactory results with a reduction of 30–50%, continuing in the protocol with only clinical follow-up. Considering all patients with nodular volume reduction ≥50% (n = 33) and those who reported esthetic improvement with reduction of 30–50% (n = 6), the therapeutic success rate of our PEI protocol increases to 75% (39/52). We compared our results with other series using PEI for treating TNs (Table 2).
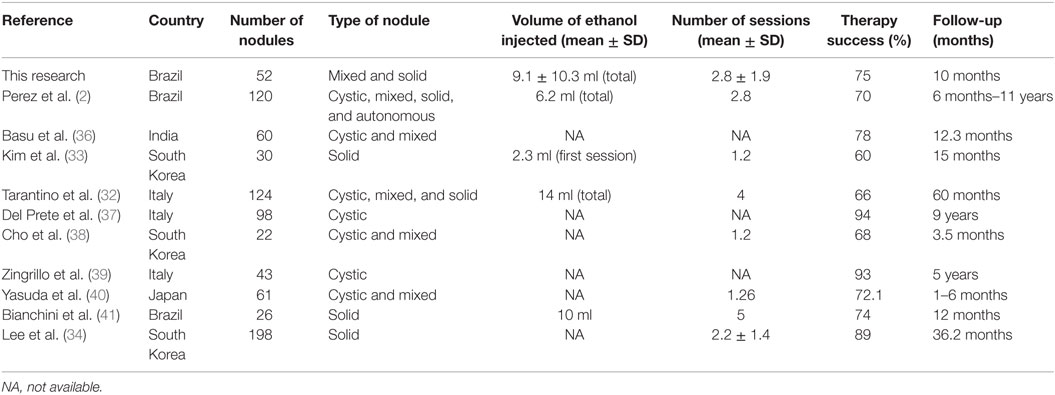
Table 2. Outcomes of US-guided PEI for treatment thyroid nodules.
Complications associated with PEI were reported in two patients, and included one hematoma with full recovery during the follow-up period. Some patients complained of local pain at the injection site. However, pain was mild and transient, and there were no severe complications, such as massive hemorrhage, vocal cord paralysis, or transient thyrotoxicosis.
Discussion
In the present study, we realized an US-guided PEI protocol for the treatment of benign mixed and solid TNs, with a 75% success rate in a short follow-up period. The procedure was safety in comparison to other methodologies previously described.
The use of USG-guided PEI as an alternative to surgery in the management of benign thyroid nodules was first proposed in 1990, by Livraghi et al. (42). Ethanol acts as a primary sclerosing agent (43) promoting cellular dehydration, coagulation necrosis and small vessel thrombosis, which is followed by progressive fibrosis and nodular volume reduction (18, 44, 45).
This procedure is well established as the first-line option for treatment of benign thyroid cysts that recur after evacuation (30), and has also been used in solid nodules, particularly in patients who are not candidates for surgery or radioiodine therapy (2, 32–34, 43).
Perez et al. (2), using PEI, have found a greater mean volume reduction in cystic (66.7%) compared to mixed (63%) and solid TNs (52.9%). The solid nodules (n = 37) were less likely to completely respond compared to the others nodules. They have found a global satisfactory response in 70% of cases. Nevertheless, it was not reported the success rate specifically in solid TNs. Furthermore, Lee et al. (34), in a large study with 198 patients, demonstrated a relevant reduction in solid TNs in 89% of cases. Even though they needed a long follow-up period of 3 years and some patients were submitted to six applications, it suggests that ethanol ablation still could be a good option to treat solid TNs since we achieve a standard protocol. Finally, Bianchini et al., in 2003, treated 26 solid TNs with ethanol injection amount according to TNs volume (41). In our protocol, we also used ethanol fixed doses, but with shorter periods of re-evaluation and consequently more frequent applications. These differences contributed to satisfactory success rates, with a larger number of patients in a shorter follow-up period.
When compared to other methods of treatment, PEI has shown more effective results and fewer complications. Four controlled studies demonstrated a 75–85% success rate after an average of two PEI sessions, compared with a 7–38% success rate in controls treated by simple cyst evacuation or saline injection (46–49). Additionally, a 12-month randomized study evidenced that the use of levothyroxine for thyroid stimulating hormone (TSH) suppression had no significant effect on nodule reduction, while a single PEI session occasionally induces a nearly 50% volume reduction (50). Furthermore, Zingrillo et al. (51) demonstrated a greater nodule volume reduction percentage in patients treated with PEI in comparison to radioiodine therapy, which, in addition, is accompanied by a 10–40% risk of hypothyroidism (51–53). Other therapies have been reported as a good alternative to treat solid TNs. Particularly, percutaneous laser ablation and radiofrequency have showed good results (54–56). Although several studies have demonstrated significant volume reduction of thyroid nodules treated with PEI, the protocols proposed are a lot heterogeneous in concern to nodules size and type, doses of ethanol used, number of injections, intervals between sessions, and follow-up length (50, 57, 58).
The highly variable success rate reported in different series might be related to the heterogeneous nature of thyroid nodules evaluated, ranging from purely cystic to purely solid nodules (36). The best results have been obtained in the treatment of large or symptomatic cystic nodules. In a prospective study with a mean follow-up of 5 years, volume reductions of at least 50% were achieved in 40/43 (93%) of patients with cystic nodules treated by PEI (39). Del Prete et al. (37) found similar results, with volume reduction >50% induced by PEI in 92/98 (94%) patients with symptomatic thyroid cysts. Outcomes have been reported to be worst in solid TNs, which is likely to be due to poor diffusion of ethanol in the solid tissue along with early wash out of ethanol due to the increased vascularity of a solid nodule as compared to a thyroid cyst (59). Our series included patients mixed and solid TNs, which might explain the lower success rate of PEI treatment when compared to other authors that assessed only simple or complex cysts. Additionally, the amount of ethanol to be injected has not been well established, with great variability between each protocol (30–100% of the initial nodular volume), which might also be related to the different outcomes observed with PEI treatment (2, 33, 38, 46, 47, 60–62). In the present study, the ethanol dose calculated was 30% of the nodular volume measured before the beginning of each session. Some authors have demonstrated a positive correlation between the volume of ethanol instilled and the volume reduction rate of cysts, without an increase of side effects with more ethanol injected (38, 59). However, most authors do not recommend administering a single dose of more than 10 ml of ethanol (63). In our study, we basically adopted a short time between evaluations. Therefore, the patients were submitted to a higher frequency of applications according to evaluation results. It may have contributed to our success rate in a short follow-up period compared to other studies.
Percutaneous ethanol injection is a safe procedure without serious complications (2). The most common reported adverse effects, caused by ethanol leakage into the surrounding tissues (63), are local pain, dysphonia, flushing, and dizziness (46, 47, 49). Although rare, other complications have been reported, such as recurrent nerve palsy, Graves’ disease, Graves’ orbitopathy, Horner’s syndrome, facial dysesthesia with increased tear flow, necrosis of the larynx and skin, and impairment of post-PEI surgery due to local fibrosis (57, 64). Accordingly, in our study there were no severe or long-standing complications.
In conclusion, our US-guided PEI protocol is safe and effective for mixed and solid thyroid nodules when compared with other methodologies described, with a 75% success rate, in a short follow-up period and no major complications based on that new target idea. In addition, we need to increase the number of patients to confirm the effectiveness of this approach.
Author Contributions
JF wrote, reviewed and edited the final version, and was responsible for submitting the manuscript. AS and KM are university professors and helped writing the paper. CK, JN, CC, TA, AJ, HB, MJ, FR, FS, MS, FB, FM, AP and AC who have contributed by creating the database and contacting patients. All authors read and approved the final manuscript, and agreed to its submission.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Popoveniuc G, Jonklaas J. Thyroid nodules. Med Clin North (2012) 96(2):329–49. doi: 10.1016/j.mcna.2012.02.002
2. Perez CLS, Fighera TM, Misaki F, Junior COM, Filho GJP, Graf H, et al. Evalution of percutaneous ethanol injection in benign thyroid nodules. Arq Bras Endocrinol Metab. (2014) 58(9):912–7. doi:10.1590/0004-2730000003444
3. Vander JB, Gaston EA, Dawber TR. The significance of nontoxic thyroid nodules. Final report of a 15-year study of the incidence of thyroid malignancy. Ann Intern Med (1968) 69:537–40. doi:10.7326/0003-4819-69-3-537
4. Tunbridge WM, Evered DC, Hall R, Appleton D, Brewis M, Clark F, et al. The spectrum of thyroid disease in a community: the Wickham survey. Clin Endocrinol (Oxf) (1977) 7:481–93. doi:10.1111/j.1365-2265.1977.tb01340.x
5. Mazzaferri EL. Management of a solitary thyroid nodule. N Engl J Med (1993) 328(8):553–9. doi:10.1056/NEJM199302253280807
6. Ezzat S, Sarti DA, Cain DR, Braunstein GD. Thyroid incidentalomas. Prevalence by palpation and ultrasonography. Arch Intern Med (1994) 154(16):1838–40. doi:10.1001/archinte.1994.00420160075010
7. Rojeski MT, Gharib H. Nodular thyroid disease. Evaluation and management. N Engl J Med (1985) 313:428–36. doi:10.1056/NEJM198508153130707
8. Rosário PW, Ward LS, Carvalho GA, Graf H, Maciel RMB, Maciel LMZ, et al. Nódulo tireoidiano e câncer diferenciado de tireoide: atualização do consenso brasileiro. Arq Bras Endocrinol Metab (2013) 57:240–64.
9. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid (2006) 16(2):109–42. doi:10.1089/thy.2006.16.109
10. Hegedus L. Clinical practice. The thyroid nodule. N Engl J Med (2004) 351(17):1764–71. doi:10.1056/NEJMcp031436
11. Lin JD, Chao TC, Huang BY, Chen ST, Chang HY, Hsueh C. Thyroid cancer in the thyroid nodules evaluated by ultrasonography and fine-needle aspiration cytology. Thyroid (2005) 15(7):708–17. doi:10.1089/thy.2005.15.708
12. Gharib H, Hegedus L, Pacella CM, Baek PJ, Papini E. Nonsurgical, image-guided, minimally invasive therapy for thyroid nodules. J Clin Endocrinol Metab (2013) 98(10):3949–57. doi:10.1210/jc.2013-1806
13. Hegedüs L. Clinical practice. The thyroid nodule. N Engl J Med (2004) 351:1764–71. doi:10.1056/NEJMcp031436
14. Papini E, Pacella CM, Hegedus L. Thyroid ultrasound and ultrasound-assisted procedures. From the shadows into an array of applications. Eur J Endocrinol (2014) 170:R133–R146. doi:10.1530/EJE-13-091
15. Pacella CM, Papini E. Image-guided percutaneous ablation therapies for local recurrences of thyroid tumors. J Endocrinol Invest (2013) 36:61–70. doi:10.1007/BF03346744
16. Shin JE, Baek JH, Lee JH. Radiofrequency and ethanol ablation for the treatment of recurrent thyroid cancers: current status and challenges. Curr Opin Oncol (2013) 25:14–9. doi:10.1097/CCO.0b013e32835a583d
17. Lima MA, Fagundes TA, Raffaelli CM, Ferreira BP, Rezende EM, Fonseca ECR, et al. Alcoolização de nódulo tireoidiano em região endêmica de bócio coloide. Arq Bras Endocrinol Metab (2007) 51:1007–12. doi:10.1590/S0004-27302007000600017
18. Crescenzi A, Papini E, Pacella CM, Rinaldi R, Panunzi C, Petrucci L, et al. Morphological changes in a hyperfunctioning thyroid adenoma after percutaneous ethanol injection: histological, enzymatic and sub-microscopical alterations. J Endocrinol Invest (1996) 19:371–6. doi:10.1007/BF03344972
19. Monzani F, Goletti O, Caraccio N, Del Guerra P, Ferdeghini M, Pucci E, et al. Percutaneous ethanol injection treatment of autonomous thyroid adenoma: hormonal and clinical evaluation. Clin Endocrinol (1992) 36:491–7. doi:10.1111/j.1365-2265.1992.tb02251.x
20. Papini E, Panunzi C, Pacella CM, Bizzarri G, Fabbrini R, Petrucci L, et al. Percutaneous ultrasound-guided ethanol injection: a new treatment of toxic autonomously functioning thyroid nodules? J Clin Endocrinol Metab (1993) 76:411–6. doi:10.1210/jcem.76.2.8432784
21. Livraghi T, Paracchi A, Ferrari C, Reschini E, Macchi RM, Bonifacino A. Treatment of autonomous thyroid nodules by percutaneous ethanol injection: four-year experience. Radiology (1994) 190:529. doi:10.1148/radiology.190.2.8284411
22. Goletti O, Monzani F, Caraccio N, Del Guerra P, Lippolis PV, Pucciarelli M, et al. Percutaneous ethanol injection treatment of autonomously functioning single thyroid nodules: optimization of treatment and short term outcome. World J Surg (1992) 16:784–9. doi:10.1007/BF02067387
23. Paracchi A, Ferrari C, Livraghi T, Reschini E, Macchi RM, Bergonzi M, et al. Percutaneous intranodular ethanol injection: a new treatment for autonomous thyroid adenoma. J Endocrinol Invest (1992) 15:353–62. doi:10.1007/BF03348753
24. Martino E, Murtas ML, Loviselli A, Piga M, Petrini L, Miccoli P, et al. Percutaneous intranodular ethanol injection for treatment of autonomously functioning thyroid nodules. Surgery (1992) 112:1161–4.
25. Mazzeo S, Toni MG, De Gaudio C, Caramella D, Pinto F, Lencioni R, et al. Percutaneous injection of ethanol to treat autonomous thyroid nodules. AJR Am J Roentgenol (1993) 161:871–6. doi:10.2214/ajr.161.4.8372778
26. Ozdemir H, Ilgit ET, Yücel C, Atilla S, Isik S, Cakir N, et al. Treatment of autonomous thyroid nodules: safety and efficacy of sonographically guided percutaneous injection of ethanol. AJR Am J Roentgenol (1994) 163:929–32. doi:10.2214/ajr.163.4.8092038
27. Di Lelio A, Rivolta M, Casati M, Capra M. Treatment of autonomous thyroid nodules: value of percutaneous ethanol injection. AJR Am J Roentgenol (1995) 164:207–13. doi:10.2214/ajr.164.1.7998541
28. Pacella CM, Papini E, Bizzarri G, Fabbrini R, Anelli V, Rinaldi R, et al. Assessment of the effect of percutaneous ethanol injection in autonomously functioning thyroid nodules by colourcoded duplex sonography. Eur J Radiol (1995) 5:395–400.
29. Monzani F, Caraccio N, Goletti O, Lippolis PV, Casolaro A, Del Guerra P, et al. Five-year followup of percutaneous ethanol injection for the treatment of hyperfunctioning thyroid nodules: a study of 117 patients. Clin Endocrinol (1997) 46:9–15. doi:10.1046/j.1365-2265.1997.d01-1752.x
30. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Revised American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid (2009) 19(11):1–48. doi:10.1089/thy.2009.0110
31. Rosário PW, Ward LS, Carvalho GA, Graf H, Maciel RM, Maciel LM, et al. Thyroid nodules and differentiated thyroid cancer: update on the Brazilian consensus. Arq Endocrinol Metab (2013) 57(4):240–64. doi:10.1590/S0004-27302013000400002
32. Tarantino L, Francica G, Sordelli I, Sperlongano P, Parmeggiani D, Ripa C, et al. Percutaneous ethanol injection of hyperfunctioning thyroid nodules: long-term follow-up in 125 patients. AJR Am J Roentgenol (2008) 190:800–8. doi:10.2214/AJR.07.2668
33. Kim DW, Rho H, Park J, Kwag J. Ultrasonography-guided ethanol ablation of predominantly solid thyroid nodules: a preliminary study for factors that predict the outcome. Br J Radiol (2012) 85:930–6. doi:10.1259/bjr/81849588
34. Lee SJ, Ahn IM. Effectiveness of percutaneous ethanol injection therapy in benign nodular and cyatic thyroid diseases: long-term follow-up experience. Endocr J (2005) 52(4):455–62. doi:10.1507/endocrj.52.455
35. Yoon DY, Chang SK, Choi CS, Yun EJ, Seo YL, Nam ES, et al. The prevalence and significance of incidental thyroid nodules identified on computed tomography. J Comput Assist Tomogr (2008) 32:810–5. doi:10.1097/RCT.0b013e318157fd38
36. Basu N, Dutta D, Maisnam I, Basu S, Ghosh S, Chowdhury S, et al. Percutaneous ethanol ablation in managing predominantly cystic thyroid nodules: an eastern India perspective. Indian J Endocrinol Metab (2014) 18(5):662–8. doi:10.4103/2230-8210.139229
37. Del Prete S, Caraglia M, Russo D, Vitale G, Giuberti G, Marra M, et al. Percutaneous ethanol injection efficacy in the treatment of large symptomatic thyroid cystic nodules: ten-year follow-up of a large series. Thyroid (2002) 12:815–21. doi:10.1089/105072502760339398
38. Cho YS, Lee HK, Ahn IM, Lim SM, Kim DH, Choi CG, et al. Sonographically guided ethanol sclerotherapy for benign thyroid cysts:results in 22 patients. AJR Am J Roentgenol (2000) 174:213–6. doi:10.2214/ajr.174.1.1740213
39. Zingrillo M, Torlontano M, Chiarella R, Ghiggi MR, Nirchio V, Bisceglia M, et al. Percutaneous ethanol injection may be a definitive treatment for symptomatic thyroid cystic nodules not treatable by surgery: five-year follow-up study. Thyroid (1999) 9:763–7. doi:10.1089/thy.1999.9.763
40. Yasuda K, Ozaki O, Sugino K, Yamashita T, Toshima K, Ito K, et al. Treatment of cystic lesions of the thyroid by ethanol instilation. World J Surg (1992) 16:958–61. doi:10.1007/BF02067001
41. Bianchini EX, Ikejiri ES, Mamone MC, Paiva ER, Maciel RMB, Furlanetto RP, et al. Injeção percutânea de etanol no tratamento de nódulos tiroidianos sólidos, císticos e autônomos. Arq Bras Endocrinol Metab (2003) 47(5):543–51. doi:10.1590/S0004-27302003000500007
42. Livraghi T, Paracchi A, Ferrari C, Bergonzi M, Garavaglia G, Raineri P, et al. Treatment of autonomous thyroid nodules with percutaneous ethanol injection. Radiology (1990) 175:827–9. doi:10.1148/radiology.175.3.2188302
43. Camargo RYA, Tomimori EK. Injeção percutânea de etanol dirigida pelo ultra-som no tratamento dos nódulos tireóideos. Arq Bras Endocrinol Metab (1998) 42:292–5. doi:10.1590/S0004-27301998000400009
44. Sugiura N, Takara K, Ohto M, Okuda K, Hirooka N. Percutaneous intratumoral injection of ethanol under ultrasound imaging for treatment od small heptocellular carcinoma. Acta Hepatol Jpn (1983) 24:1920.
45. Livraghi T, Ravetto C, Solbiati L, Suter F. Percutaneous interstitial chemotherapy of a small hepatocellular carcinoma under ultrasound guidance. Tumori (1986) 72:525–7.
46. Bennedbaek FN, Hegedüs L. Treatment of recurrent thyroid cysts with ethanol: a randomized double-blind controlled trial. J Clin Endocrinol Metab (2003) 88:5773–7. doi:10.1210/jc.2003-031000
47. Valcavi R, Frasoldati A. Ultrasound-guided percutaneous ethanol injection therapy in thyroid cystic nodules. Endocr Pract (2004) 10:269–75. doi:10.4158/EP.10.3.269
48. Antonelli A, Campatelli A, Di Vito A, Alberti B, Baldi V, Salvioni G, et al. Comparison between ethanol sclerotherapy and emptying with injection of saline in treatment of thyroid cysts. Clin Investig (1994) 72:971–4. doi:10.1007/BF00577738
49. Verde G, Papini E, Pacella CM, Gallotti C, Delpiano S, Strada S, et al. Ultrasound guided percutaneous ethanol injection in the treatment of cystic thyroid nodules. Clin Endocrinol (Oxf) (1994) 41:719–24. doi:10.1111/j.1365-2265.1994.tb02785.x
50. Bennedbaek FN, Nielsen LK, Hegedus L. Effect of percutaneous ethanol injection therapy versus suppressive doses of L-thyroxine on benign solitary solid cold thyroid nodules: a randomized trial. J Clin Endocrinol Metab (1998) 83:830–5. doi:10.1210/jc.83.3.830
51. Zingrillo M, Torlontano M, Ghiggi MR, Frusciante V, Varraso A, Liuzzi A, et al. Radioiodine and percutaneous ethanol injection in the treatment of large toxic thyroid nodule: a long-term study. Thyroid (2000) 10(11):985–9. doi:10.1089/thy.2000.10.985
52. David E, Rosen IB, Bain J, James J, Kirsh JC. Management of the hot thyroid nodule. Am J Surg (1995) 170:481–3. doi:10.1016/S0002-9610(99)80334-1
53. Giuffrida D, Gharib H. Controversies in the management of cold, hot, and occult thyroid nodules. Am J Med (1995) 99:642–50. doi:10.1016/S0002-9343(99)80252-6
54. Dossing H, Bennebaek FN, Karstrup S, Hegedüs L. Benign solitary solid cold thyroid nodules: US-guided interstitial laser photocoagulation-initial experience. Radiology (2002) 225(1):53–7. doi:10.1148/radiol.2251011042
55. Papini E, Guglielmi R, Bizarri G, Pacella CM. Ultrasound-guided laser termal ablation for treatment of benign thyroid nodules. Endocr Pract (2004) 10(3):276–83. doi:10.4158/EP.10.3.276
56. Baek JB, Lee JH, Valcavi R, Pacella CM, Rhim H, Gyu D. Thermal ablation for benign thyroid nodules: radiofrequency and laser. Korean J Radiol (2011) 12(5):525–40. doi:10.3348/kjr.2011.12.5.525
57. Bennedbaek FN, Karstrup S, Hegedus L. Percutaneous ethanol injection therapy in the treatment of thyroid and parathyroid diseases. Eur J Endocrinol (1997) 136:240–50. doi:10.1530/eje.0.1360240
58. Bennedbaek FN, Hegedus L. Percutaneous ethanol injection therapy in benign solitary solid cold thyroid nodules: a randomized trial comparing one injection with three injections. Thyroid (1999) 9:225–33. doi:10.1089/thy.1999.9.225
59. Kim JH, Lee HK, Lee JH, Ahn IM, Choi CG. Efficacy of sonographically guided percutaneous ethanol injection for treatment of thyroid cysts versus solid thyroid nodules. AJR Am J Roentgenol (2003) 180:1723–6. doi:10.2214/ajr.180.6.1801723
60. Sung JY, Baek JH, Kim YS, Jeong HJ, Kwak MS, Lee D, et al. One-step ethanol ablation of viscous cystic thyroid nodules. AJR Am J Roentgenol (2008) 191(6):1730–3. doi:10.2214/AJR.08.1113
61. Jayesh SR, Mehta P, Cherian MP, Ilayaraja V, Gupta P, Venkatesh K. Efficacy and safety of USG-guided ethanol sclerotherapy in cystic thyroid nodules. Indian J Radiol Imaging (2009) 19(3):199–202. doi:10.4103/0971-3026.54879
62. Kim YJ, Baek JH, Ha EJ, Lim HK, Lee JH, Sung JY, et al. Cystic versus predominantly cystic thyroid nodules: efficacy of ethanol ablation and analysis of related factors. Eur Radiol (2012) 22(7):1573–8. doi:10.1007/s00330-012-2406-5
63. Halenka M, Karasek D, Frysak Z. Ultrasound-guided percutaneous ethanol injection of small and medium-sized thyroid cysts with relatively small amounts of ethanol. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub (2015) 159(3):417–21. doi:10.5507/bp.2014.009
Keywords: thyroid nodules, percutaneous ethanol injection, alcoholization, US-guided, nodule volume reduction
Citation: Felício JS, Conceição AMS, Santos FM, Sato MMM, Bastos FdA, Braga de Souza ACC, Koury CC, Neto JFA, Cunha de Melo FT, Carvalho CT, Arbage TP, Junior ABdF, de Rider Brito HA, Júnior MOM, Resende FdS, Peixoto AS and Felício KM (2016) Ultrasound-Guided Percutaneous Ethanol Injection Protocol to Treat Solid and Mixed Thyroid Nodules. Front. Endocrinol. 7:52. doi: 10.3389/fendo.2016.00052
Received: 02 April 2016; Accepted: 17 May 2016;
Published: 06 June 2016
Edited by:
Noriyuki Koibuchi, Gunma University Graduate School of Medicine, JapanReviewed by:
Eijun Nishihara, Kuma Hospital, JapanKyung Tae, Hanyang University Hospital, South Korea
Copyright: © 2016 Felício, Conceição, Santos, Sato, Bastos, Braga de Souza, Koury, Neto, Cunha de Melo, Carvalho, Arbage, Junior, de Rider Brito, Júnior, Resende, Peixoto and Felício. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: João Soares Felício, felicio.bel@terra.com.br