 Francisca Sá1,2* Paula Pinto3 Catarina Cunha2,3 Raquel Lemos3 Liliana Letra2,4 Mário Simões3 Isabel Santana2,4
Francisca Sá1,2* Paula Pinto3 Catarina Cunha2,3 Raquel Lemos3 Liliana Letra2,4 Mário Simões3 Isabel Santana2,4
- 1 Neurology Service of the Hospital de Faro E.P.E, Faro, Portugal
- 2 Neurology Department of the Centro Hospitalar Universitário de Coimbra, Coimbra, Portugal
- 3 Faculty of Psychology and Educational Sciences, University of Coimbra, Coimbra, Portugal
- 4 Faculty of Medicine, University of Coimbra, Coimbra, Portugal
Although patients with Alzheimer disease (AD) share clinical and histological features regardless of age of onset, the hypothesis that early onset AD constitutes a distinct subgroup prevails. Some authors suggest that early attention or language impairment constitute patterns of differentiation in terms of neuropsychological profile, between these groups. However, investigations are not consensual in terms of cognitive domains affected in each group. Aim: To investigate whether there is early neuropsychological difference between two types of AD using the conventional dividing line of 65 years. Methods: We evaluated the results obtained in the Mini-Mental State Examination (MMSE) and in a comprehensive neuropsychological battery – Battery of Lisbon for the Assessment of Dementia (BLAD), at a Dementia clinic in the University Hospital of Coimbra and a Memory Clinic. The study was developed in consecutive patients with a clinical probable diagnosis of mild to moderate AD, using standard criteria (DSMIV and NINCDS-ADRDA). Statistical analysis was performed using Qui-square and U-Mann–Whitney, for categorical and non-categorical variables. The degree of relation between variables, was measured using the coefficient of correlation rs de Spearman. Results: The total sample included 280 patients: 109 with early onset AD and 171 with a late-onset form. Groups were comparable in terms of gender, education or severity of disease, and MMSE. In BLAD, for univariate analysis the early onset group had lower scores in Naming (p = 0.025), Right–Left Orientation (p = 0.029) and Praxis (p = 0.001), and better performances in Orientation (p = 0.001) and Visual Memory (p = 0.022). After application of Bonferroni correction for multiple comparisons only Praxis and Orientation could differentiate the two groups. No significant differences were found in other tests or functions. Discussion: The results are suggestive of dissociated profiles between early and late-onset AD. Younger patients have a major impairment in Praxis and a tendency for a great impairment in neocortical temporal functions. AD patients with late-onset forms had a tendency for worse performances in Visual Memory and Orientation, suggesting a more localized disease to the limbic structures.
Introduction
Alzheimer’s disease (AD) is the most common form of dementia and although its prevalence is much higher in the older population, it is still the most frequent form of dementia under the age of 65 years (Harvey et al., 2003). Early onset dementia conventionally includes patients with onset before 65 years of age (Rossor et al., 2010). This cut-off is an arbitrary division based in sociological aspects and has no biological significance but is considered in diagnostic criteria and is randomly used in clinical practice. Despite neuropathological hallmarks being the same (Khachaturian, 1985), many research groups continue to report phenotypic differences between early and late-onset Alzheimer’s disease (EOAD and LOAD), considering age of onset an important determinant of the heterogeneity observed in the disease (Kensinger, 1996). Differences have been reported in rate of progression of the disease (Rogaeva, 2002), perfusion and metabolic deficits in the temporal and parietal lobes (Lantos et al., 1992; Mann et al., 1992; Kim et al., 2005, 2010), grade and distribution of gray matter atrophy (Ishii et al., 2005; Frisoni et al., 2007), and prevalence of the allele ApoE ε4 (van der Flier et al., 2011). Studies have also shown different clinical profiles with higher prevalence of language impairment and other non-memory symptoms as the initial presentation in the EOAD subgroup (Koedam et al., 2010). However, investigations are not consensual in terms of cognitive domains affected in each group (Licht et al., 2007).
The relative low prevalence of AD under 65 years old (McMurtray et al., 2006; Shinagawa et al., 2007), question about the differential diagnosis with other forms of dementia more frequent in this age level as fronto-temporal dementia, which seems to be responsible for up to 20% of pre-senile dementia cases (Snowden et al., 2002; Weder et al., 2007), and the higher frequency of mutations with more atypical phenotypes (Lucatelli et al., 2009), contribute to divergences in clinical profiles described in literature. Furthermore, although it was generally accepted that Primary Progressive Aphasia (PPA) was a non-Alzheimer type of dementia, some studies have demonstrated that atypical distribution of AD is responsible for 20–30% of cases with various forms of PPA (Alladi et al., 2007). Namely, AD could be the most frequent cause of Logopenic Progressive Aphasia, a subtype of PPA, clinically characterized by slow speech, sentence repetition, and comprehension deficits, with relative sparing of motor speech, grammar, and single-word comprehension (Gorno-Tempini et al., 2008).
The increasing interest in the early forms of the disease because of genetic implications, and the recent biomarker developments will certainly allow a more precise classification in clinical practice.
The aim of this study is to better characterize the neuropsychological profile and cognitive deficits of these subgroups or forms of AD, as this may be relevant to an earlier and accurate diagnosis, as well as to the design of clinical trials.
Materials and Methods
Participants and Procedures
Patients were collected consecutively from January 1990 until June 2009, at the Dementia Clinic of the University Hospital of Coimbra and in a private Memory Clinic in the same city and as purposed; we assigned each patient to one of the two ages of onset groups, using the conventional division line of the 65 years.
Each patient had a structured clinical interview, laboratory routine exams, physical and neurological examination, and structural (CT or MRI) and functional (SPECT or PET) imaging. Laboratory exams included complete blood count, chemistry profile, thyroid function, B12, and folic acid. Age at onset was estimated from caregiver’s information using a standard questionnaire and disease duration was established in years, from the estimated age at onset until the date of the first neuropsychological assessment (Sano et al., 1995). Information related to family history was also taken from patient’s relatives. Education was calculated considering schooling years of the patients.
Inclusion criteria included (i) clinical probable diagnosis of AD using the of DSM-IV-TR criteria (American Psychiatric Association, 2000) and NINCDS-ADRDA (McKhann et al., 1984); (ii) classification in mild to moderate severity using the Mini-Mental State Examination (MMSE; Folstein et al., 1975) and Clinical Dementia Rating (CDR) Scale considering as a cut-off for mild AD ≥17 points and CDR of 1, and moderate severity when scores were from 16 to 10; (iii) cognitive evaluation with a comprehensive neuropsychological battery which includes all the items intended to be assessed – Battery of Lisbon for the Assessment of Dementia (BLAD).
Patients with MMSE score under 10, with relevant psychiatric manifestations and/or sensory or motor deficits that could interfere with the neuropsychological assessment were excluded. All subjects were right-handed.
The present research complied with the ethical guidelines for human experimentation stated in the Declaration of Helsinki and was approved by the Ethics Board of Coimbra University Hospital. An informed consent was obtained from all the participants after the aims and procedures of the investigation were fully explained by a member of the study group. For AD patients who were incapable of providing consent on his/her own behalf, a legal representative provided the informed consent.
Material and Neuropsychological Testing
The instruments for neuropsychological evaluation were applied at the time of the diagnosis by two trained neuropsychologists. A standardized assessment was performed in which a sociodemographic questionnaire and an inventory of current clinical health status were firstly applied, followed by the administration of the MMSE and finally by the comprehensive neuropsychological assessment. MMSE (Folstein et al., 1975) is a widely recognized and used brief screening instrument for detecting cognitive deficits and therefore is not described in detail here. It is in paper-and-pencil format and is scored out of a possible 30 points, with higher scores indicating better cognitive performance. In this project we used the Portuguese adaptation of the MMSE (Guerreiro et al., 1994). The BLAD (Garcia, 1984) is a comprehensive battery adapted and normalized for the Portuguese population that integrates tests with sensitivity and specificity for the explored cognitive domains and critical to outline the clinical profiles of these patients. This battery assesses the following cognitive domains: attention (Cancelation Task); verbal, motor, and graphomotor initiatives (Verbal Semantic Fluency, Motor and Graphomotor Initiative – Luria sequences); verbal comprehension (modified version of the Token Test); sentences repetition; verbal and non-verbal abstraction (Interpretation of Proverbs and the Raven Progressive Matrices); visuo-constructional abilities (Cube Copy); calculation (Basic Written Calculation); immediate memory (Digit Span forward); working memory (Digit Span backward); learning and verbal memory (subtests from de Wechsler Memory Scale-R) (Wechsler, 1987); right–left orientation and praxis.
Statistical Analysis
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) version 16.0 for Windows.
Non-parametric analyses were performed as there was no equivalence in number, normal distribution, or homogeneity of variances (Qui-square and U-Mann–Whitney, for categorical and non-categorical variables, respectively, with Bonferroni correction).
To measure degree of relation between variables, the coefficient of correlation rs de Spearman was applied.
Results
The study sample consisted of 280 patients: 109 with EOAD and 171 with LOAD. The characterization of the study sample and details of both subgroups is provided in Table 1. For this description the following variables were considered: sample size, age, gender, education level, age at onset, disease duration, MMSE mean scores and classification in terms of severity of the disease.
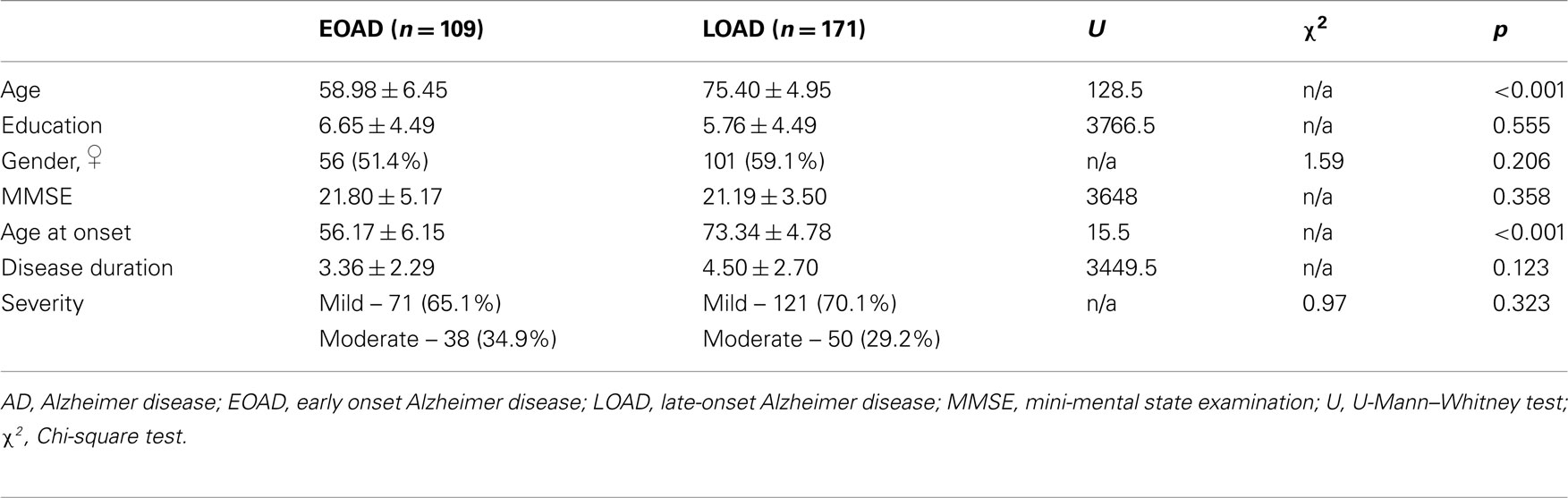
Table 1. Comparisons of demographic and clinical variables in both groups: EOAD and LOAD.
Groups were matched for education, gender, MMSE, disease duration, and severity. As expected, significant differences were found for age and age at onset (Table 1).
The comparisons of scores obtained in the neuropsychological assessment (BLAD) are presented in Table 2. Results suggest that patients with EOAD performed significantly poorly than the LOAD group in Naming (p = 0.025), Praxis (p = 0.001), and Right–Left Orientation (p = 0.029), and had better performances in Orientation (p = 0.001) and Visual Memory (p = 0.022). After correction for multivariate comparisons only Praxis and Orientation could differentiate the two groups.
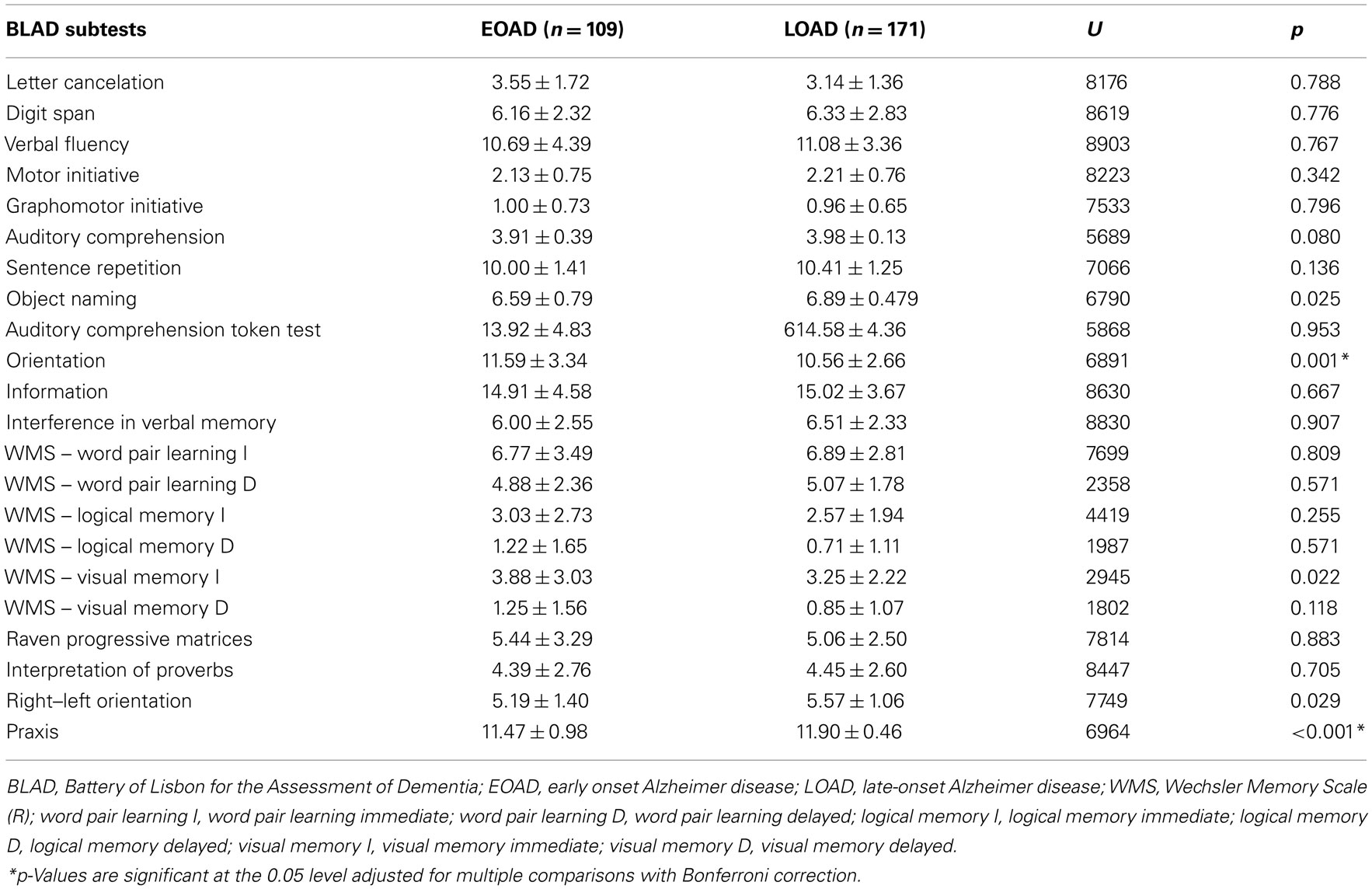
Table 2. Comparison of neuropsychological performances on BLAD of EOAD and LOAD groups.
In order to investigate in which degree the performances in neuropsychological tests were related to clinical variables, it was conducted a Spearman’s correlation. The clinical variables included in the analysis were the mean scores on MMSE, age at onset and disease duration. The neuropsychological variables included the performances in the subtests of BLAD in which were found significant differences in the univariate analysis (Tables 3 and 4).
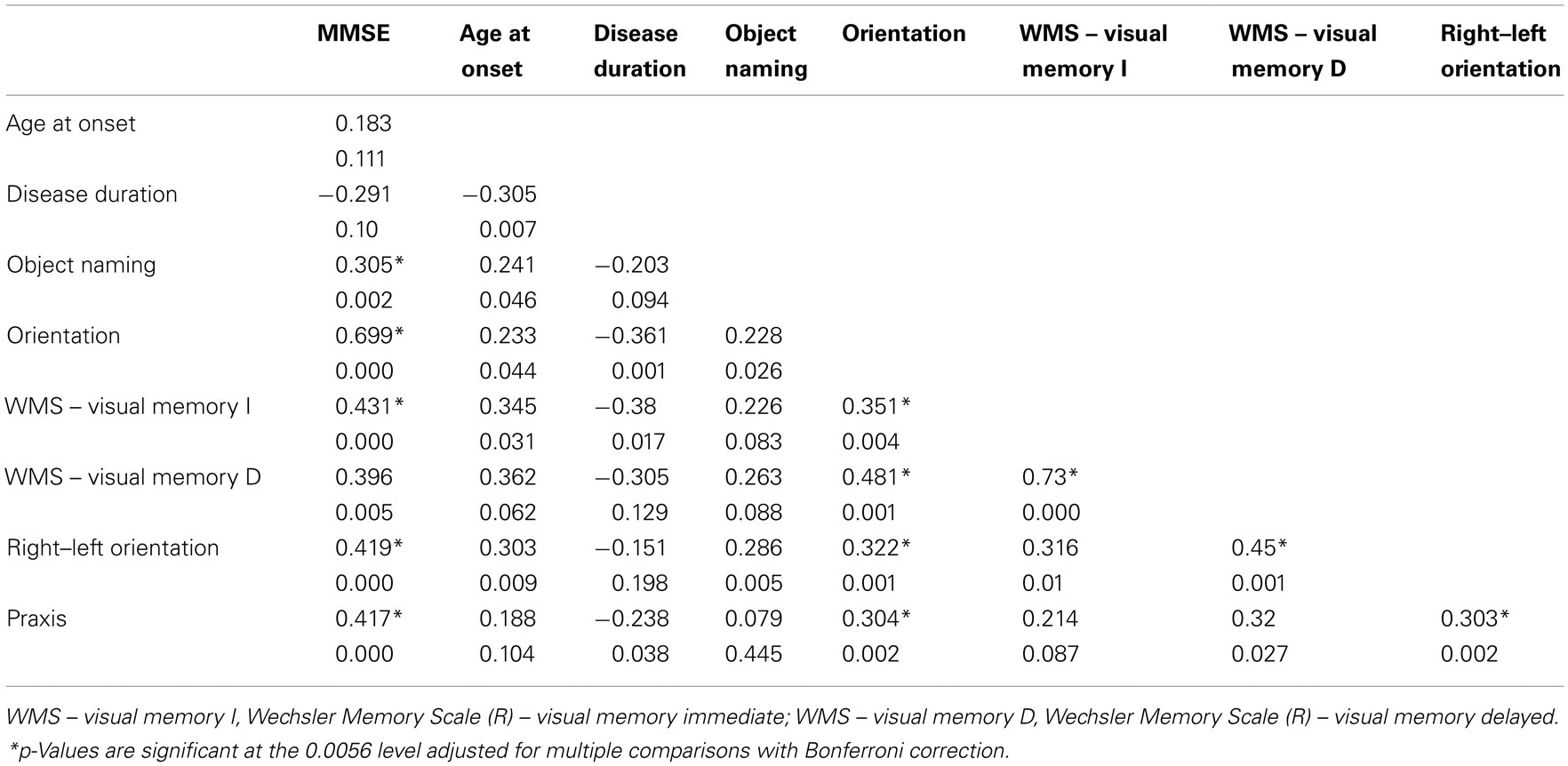
Table 3. Spearman’s correlations between BLAD subtests and clinical variables – MMSE, age at onset and disease duration in EOAD group.
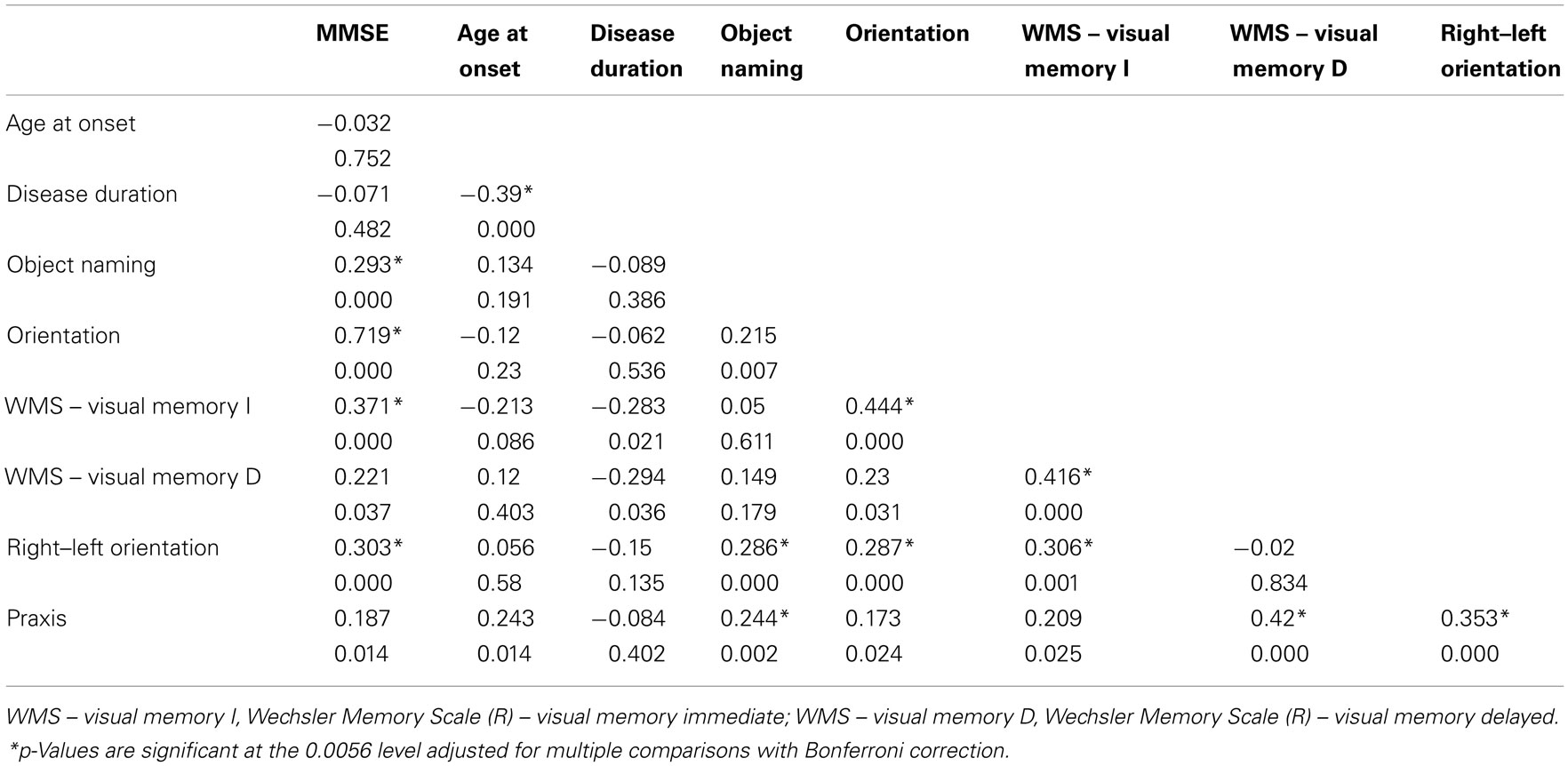
Table 4. Spearman’s correlations between BLAD subtests and clinical variables – MMSE, age at onset and disease duration in LOAD group.
Considering the EOAD group, it was found a significant positive correlation between the Immediate visual memory and Orientation subtests. A positive correlation was also found between Right–left orientation and Visual memory, both immediate and delayed subtests. Although not reaching statistical significance, a higher negative correlation between the Disease duration and the subtests Orientation and Immediate visual memory was noticed.
In the LOAD group it was observed a significant positive correlation between the Praxis subtest, and Object naming, Right–left orientation and Visual memory. In this group, significant correlation was also found for Orientation and Immediate visual memory.
The results are presented in the Table 3 for the EOAD group and in the Table 4 for the LOAD.
Discussion
Our results are indicative of dissociated profiles between early and late-onset AD. In language domain, initially we found differences in naming, while comprehension and repetition scores were similar in both groups. When multivariate analysis was applied using all the variables considered, this difference was no longer significant. Reviewing the literature, language has shown to be the cognitive domain more useful and consensual to differentiate early from late-onset subgroups (Seltzer and Sherwin, 1983; Filley et al., 1986; Imamura et al., 2005; Suribhatla et al., 2004) In fact, Seltzer and Sherwin (1983) which were the first authors to investigate this hypotheses, found that the major differences between the groups were in a naming task from the Boston Diagnostic Aphasia Examination battery, with worst performances in the EOAD group. However, Jacobs et al. (1994) could not find this same difference in naming ability using a modified version of MMSE, and in Koss and Suribhatla studies the EOAD group had even better scores in the Boston Naming Test (BNT; Koss et al., 1996; Suribhatla et al., 2004). A justification for these contradictory findings was the possible influence of aging-associated sensorial declines when population samples from different studies were non-equivalent in terms of demographic variables. For instance, a deficit in visual perception or object identification could contribute to worst scores in the naming tasks (Imamura et al., 2005). This interpretation of a dominant deficit in perception and object identification, applied to our results that indicate a tendency for a worse performance in EOAD, can lead us to infer that in this form there is a broader area of cerebral alterations, probably involving posterior regions interfering with normal occipital lobe compensatory strategies (Lawlor et al., 1994). Severity could also be influencing this task performances as naming alterations have been reported in more severe stages of AD (Imamura et al., 2005). This is not an explanation for some asymmetry of our results, because samples in this study were matched for severity.
Even though some authors have observed differences in comprehension and repetition tasks, we have not found significant differences between groups, in comprehension of simple orders, complex orders (Token Test) and repetition. We should admit that this controversy results are mainly a reflex of the despair in level of difficulty in the tasks used in each study, nonetheless Frisoni et al. (2007) reported similar results in the Token Test as we did with the same test, reinforcing the similarity of performances in receptive language task for both age of onset groups.
The difference found in the left–right orientation scores, did not reach statistical significance when correction factors were applied, but is consistent with other studies, reveling that younger subjects with AD have more difficulties in eye–hand coordination tasks that require special-motor abilities (Fujimori et al., 1998; Imamura et al., 2005). And in fact, in our data, the praxis task evaluating ideomotor apraxia was the only one, to reach statistical significance after multivariate analysis, with worse performance in the early onset group. This difference was also described by Reid et al. (1996) and supports the hypothesis of left posterior hemisphere susceptibility in EOAD.
Memory is a complex function aggregating many different modalities. The neuropsychological comprehensive battery used in the study, allowed us to investigate the most representative ones, including primary or working memory, and secondary memories, namely remote and episodic memory. Attention/working memory was tested by a cancelation task (letter “A”) and the Digit span (Forward and Backward). Many authors have reported attention and working memory deficits to be more pronounced in EOAD (Jacobs et al., 1994; Koss et al., 1996; Suribhatla et al., 2004; Kalpouzos et al., 2005), but our results do not corroborate this because performances of EOAD and LOAD groups were equivalent. To evaluate recollection of very well learned non-autobiographical material we used a BLAD’s Information test which is a 20 item multi-thematic cultural task (retrograde memory) and a verbal fluency experiment consisting of food items (semantic memory). Once again the comparison between groups did not reach significance in our patients, corroborating other findings (Suribhatla et al., 2004; Kalpouzos et al., 2005; Frisoni et al., 2007). But this is not a consensual result because Jacobs et al. (1994) have pointed worst performances for the LOAD group in the enunciation of four United States of America presidents in the modified MMSE and Koss et al. (1996) found to be more difficult for EOAD to enunciate animal names, a well-known verbal semantic memory task similar to the one we used in our battery. The evaluation of episodic memory is fundamental in the diagnosis of dementia and especially in AD. The neuropsychological battery used in our study includes the well-known tests of the Wechsler Memory Scale-Revised (WMS-R) version, with immediate and delayed recall of verbal and visual material. For the evaluation of verbal episodic memory we compared the performance of EOAD and LOAD groups in the Associated learning of paired words and Logical memory tasks, evaluation, and differences did not reach statistical significance in immediate or delayed evocation. Our findings are similar to others (Lawlor et al., 1994; Kalpouzos et al., 2005), but some studies have reached different results, with LOAD group presenting lower scores, suggesting more vulnerability of limbic regions (Chui et al., 1985; Jacobs et al., 1994; Koss et al., 1996; Suribhatla et al., 2004). This lack of consensus may be due to intra or inter-study group-differences in duration and severity of disease. Although these variables were well controlled in our study, we could not also get significance for the higher performances in Logic and Visual memory in the EOAD, with multivariate comparisons analysis. In previous studies no differences were found in reproduction of Rey complex geometric figure (Kalpouzos et al., 2005) or LOAD had better performances in visual memory (Suribhatla et al., 2004). Both studies made use of different materials for task execution presenting a single visual stimulus, while in BLAD four drawings are presented.
In our study LOAD individuals had worst performances in Orientation (p = 0.001), and the plausible justification is a more pronounced decline in memory, as the observed errors were mainly in questions related to temporal orientation (date and day of the week). Besides, in correlation analysis between Orientation and Visual memory there was a moderate positive association in LOAD group (0.444; p < 0.0056), which means that better performance in orientation correlated with higher scores in visual memory. These results and explanatory observations have already been reported in previous studies (Jacobs et al., 1994; Imamura et al., 2005).
So, the lower performance in Orientation task correlated to worst visual memory observed in LOAD can be integrated in the same cognitive deficit, and is consistent with a tendency in literature to point episodic memory as a dissociate factor in AD (Jacobs et al., 1994; Koss et al., 1996; Suribhatla et al., 2004; Kalpouzos et al., 2005; Frisoni et al., 2007).
In the present study visual-constructional abilities were not analyzed properly, because related-tasks in BLAD (clock and cube drawing) were only qualitatively evaluated and no quantitative scoring or analysis was available. This cognitive function has been associated in literature with worst performances in EOAD groups (Koss et al., 1996; Imamura et al., 2005; Mendez, 2006; Frisoni et al., 2007). Other limitation of this study is the lack of a formal assessment of behavioral and psychological symptoms of dementia.
So, in conclusion in this study the younger patients presented a major impairment in Praxis. Despite the strong size sample we failed to confirm a significant difference in language tasks, although there was a tendency for worse performance in naming in the younger set. LOAD patients had inferior performances in Temporal Orientation which is related to a tendency for great impairment in visual memory, suggesting a more localized disease to the limbic structures. This data may contribute to a better recognition of AD in younger patients and suggests atypical clinical presentations to be considered in the differential diagnosis of early onset dementia.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This work was supported by the Portuguese Foundation for Science and Technology (FCT) through PIC/IC/83206/2007; we would like to thank Bárbara Oliveiros for the help with the statistical analysis.
References
Alladi, S., Xuereb, J., Bak, T., Nestor, P., Knibb, J., Patterson, K., and Hodges, J. R. (2007). Focal cortical presentations of Alzheimer’s disease. Brain 130(Pt 10), 2636–2645.
American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders (DSM IV-TR), 4th Edn. Washington, DC: American Psychiatric Association. [Portuguese translation, Lisbon, Climepsi, 2002].
Chui, H., Teng, E., Henderson, V., and Moy, A. (1985). Clinical subtypes of dementia of the Alzheimer type. Neurology 35, 1544–1550.
Filley, C. M., Kelly, J., and Heaton, R. K. (1986). Neuropsychologic features of early and late onset Alzheimer’s disease. Arch. Neurol. 43, 574–576.
Folstein, M., Folstein, S., and McHugh, P. (1975). Mini mental state: a practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12, 189–198.
Frisoni, G., Pievani, M., Testa, C., Sabattoli, F., Bresciani, L., Bonetti, M., Beltramello, A., Hayashi, K. M., Toga, A. W., and Thompson, P. M. (2007). The topography of grey matter involvement in early and late onset Alzheimer’s disease. Brain 130, 720–730.
Fujimori, M., Imamura, T., Yamadori, A., Hirono, N., Ikejiri, Y., Shimomura, T., and Mori, E. (1998). Age at onset and visuocognitive disturbances in Alzheimer’s disease. Alzheimer Dis. Assoc. Disord. 12, 163–166.
Garcia, C. A. (1984). Doença de Alzheimer. Problemas do diagnóstico clínico (Tese de doutoramento). Lisboa: Faculdade de Medicina de Lisboa - colecҫões.
Gorno-Tempini, M. L., Brambati, S. M., Ginex, V., Ogar, J., Dronkers, N. F., Marcone, A., Perani, D., Garibotto, V., Cappa, S. F., and Miller, B. L. (2008). The logopenic/phonological variant of primary progressive aphasia. Neurology 71, 1227–1234.
Guerreiro, M., Silva, A. P., Botelho, M. A., Leitão, O., and Garcia, C. (1994). Adaptação à população portuguesa da tradução do “Mini Mental State Examination” (MMSE). Rev. Port. Pneumol. 1, 9.
Harvey, R. J., Skelton-Robinson, M., and Rossor, M. N. (2003). The prevalence and causes of dementia in people under the age of 65 years. J. Neurol. Neurosurg. Psychiatr. 74, 1206–1209.
Imamura, T., Fujimori, M., Hirono, N., Hashimoto, M., Kazui, H., and Mori, E. (2005). Age at onset and the disturbance of orientation in Alzheimer’s disease. Niigata J. Health Welf. 5, 60–64.
Ishii, K., Kawachi, T., Sasaki, H., Kono, A., Fukuda, T., Kojima, Y., and Mori, E. (2005). Voxel-based morphometric comparison between early and late onset mild Alzheimer’s disease an assessment of diagnostic performance of Z score images. AJNR Am. J. Neuroradiol. 26, 333–340.
Jacobs, D., Sano, M., Marder, K., Bell, K., Bylsma, F., Lafleche, G., Albert, M., Brandt, J., and Stern, Y. (1994). Age at onset of Alzheimer’s disease: relation to pattern of cognitive dysfunction and rate of decline. Neurology 44, 1215–1220.
Kalpouzos, G., Eustache, F., de la Sayette, V., Viader, F., Chételat, G., and Desgranger, B. (2005). Working memory and FDG-PET dissociate early and late onset Alzheimer disease patients. J. Neurol. 252, 548–558.
Kensinger, E. (1996). Early and late onset as subdivisions of Alzheimer’s disease. Harv. Brain 26–36. Available at: http://www.wjh.harvard.edu/∼ekensing/Kensinger_1996.pdf
Kim, E. J., Cho, S. S., Jeong, Y., Park, K. C., Kang, S. J., Kang, E., Kim, S. E., Lee, K. H., and Na, D. L. (2005). Glucose metabolism in early onset versus late onset Alzheimer’s disease: an SPM analysis of 120 patients. Brain 128, 1790–1801.
Kim, S. H., Seo, S. W., Yoon, D. S., Chin, J., Lee, B. H., Cheong, H. K., Han, S. H., and Na, D. L. (2010). Comparison of neuropsychological and FDG-PET findings between early- versus late-onset mild cognitive impairment: a five-year longitudinal study. Dement. Geriatr. Cogn. Disord. 29, 213–223.
Koedam, E. L., Lauffer, V., van der Vlies, A. E., van der Flier, W. M., Scheltens, P., and Pijnenburg, Y. A. (2010). Early-versus late-onset Alzheimer’s disease: more than age alone. J. Alzheimers Dis. 19, 1401–1408.
Koss, E., Edland, S., Fillenbaum, G., Mohs, R., Clark, C., Galasko, D., and Morris, J. (1996). Clinical and neuropsychological differences between patients with earlier and later onset of Alzheimer’s disease: a CERAD analysis, part XII. Neurology 46, 136–141.
Lantos, P. L., Luthert, P. J., Hanger, D., Anderton, B. H., Mullan, M., and Rossor, M. N. (1992). Familial Alzheimer’s disease with the amyloid precursor protein position 717 mutation and sporadic Alzheimer’s disease have the same cytoskeletal pathology. Neurosci. Lett. 137, 221–224.
Lawlor, B., Ryan, T., Schmeider, J., Mohs, R., and Davis, K. (1994). Clinical symptoms associated with age at onset in Alzheimer’s disease. Am. J. Psychiatry 151, 1646–1649.
Licht, E. A., McMurtray, A. M., Saul, R. E., and Mendez, M. F. (2007). Cognitive differences between early- and late-onset Alzheimer’s disease. Am. J. Alzheimers Dis. Other Demen. 22, 218–222.
Lucatelli, J., Barros, A., Maluf, S., and Andrade, F. (2009). Influência genética sobre a doença de Alzheimer de início precoce. Revista Psiquiatria Clínica. 36, 25–30.
Mann, U., Mohr, E., Gearing, M., and Chase, T. (1992). Heterogeneity in Alzheimer’s disease: progression rate segregated by distinct neuropsychological and cerebral metabolic profiles. J. Neurol. Neurosurg. Psychiatr. 55, 956–959.
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., and Stadlan, E. M. (1984). Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of the Department of Health and Human Services Task Force on Alzheimer’s disease. Neurology 34, 939–944.
McMurtray, A., Clark, D., Christine, D., and Mendez, M. (2006). Early-onset dementia: frequency and causes compared to late-onset dementia. Dement. Geriatr. Cogn. Disord. 21, 59–64.
Mendez, M. (2006). The accurate diagnosis of early-onset dementia. Int. J. Psychiatry. Med. 36, 401–412.
Reid, W., Broe, G., Creasey, H., Grayson, D., McCusker, E., Bennett, H., Longley, W., and Sulway, M. (1996). Age at onset and pattern of neuropsychological impairment in mild early stage Alzheimer disease. A study of a community-based population. Arch. Neurol. 53, 1056–1061.
Rogaeva, E. (2002). The solved and unsolved mysteries of the genetics of early-onset Alzheimer’s disease. Neuromolecular Med. 2, 1–10.
Rossor, M. N., Fox, N. C., Mummery, C. J., Schott, J. M., and Warren, J. D. (2010). The diagnosis of young-onset dementia. Lancet Neurol. 9, 793–806.
Sano, M., Devanand, D. P., Richards, M., Miller, L. W., Marder, K., Bell, K., Dooneief, G., Bylsma, F. W., Lafleche, G., Albert, M., Folstein, M., and Stern, Y. (1995). A standardized technique for establishing onset and duration of symptoms of Alzheimer’s disease. Arch. Neurol. 52, 961–966.
Seltzer, B., and Sherwin, I. (1983). A comparison of clinical features in early and late onset primary degenerative dementia: one entity or two? Arch. Neurol. 40, 143–146.
Shinagawa, S., Ikeda, M., Toyota, Y., Matsumoto, T., Matsumoto, N., Mori, T., Ishikawa, T., Fukuhara, R., Komori, K., Hokoishi, K., and Tanabe, H. (2007). Frequency and clinical characteristics of early-onset dementia in consecutive patients in a memory clinic. Dement. Geriatr. Cogn. Disord. 24, 42–47.
Snowden, J. S., Neary, D., and Mann, D. M. (2002). Frontotemporal dementia. Br. J. Psychiatry 180, 140–143.
Suribhatla, S., Baillon, S., Dennis, M., Marudkar, M., Muhammad, S., Munro, D., Spreadbury, C., and Lindesay, J. (2004). Neuropsychological performance in early and late onset Alzheimer’s disease: comparisons in a memory clinic population. Int. J. Geriatr. Psychiatry 19, 1140–1147.
van der Flier, W. M., Pijnenburg, Y. A., Fox, N. C., and Scheltens, P. (2011). Early-onset versus late-onset Alzheimer’s disease: the case of the missing APOE epsilon 4 allele. Lancet Neurol. 10, 280–288.
Wechsler, D. (1987). WMS-R Manual: Wechsler Memory Scale Revised. San Antonio, TX: The Psychological Corporation.
Keywords: early onset Alzheimer’s disease, late-onset Alzheimer’s disease, neuropsychological assessment, cognitive domains
Citation: Sá F, Pinto P, Cunha C, Lemos R, Letra L, Simões M and Santana I (2012) Differences between early and late-onset Alzheimer’s disease in neuropsychological tests. Front. Neur. 3:81. doi: 10.3389/fneur.2012.00081
Received: 08 February 2012; Paper pending published: 16 February 2012;
Accepted: 25 April 2012; Published online: 14 May 2012.
Edited by:
João Massano, Centro Hospitalar de São João, PortugalReviewed by:
Marcelo L. Berthier, University of Malaga, SpainOlivier Piguet, Neuroscience Research Australia, Australia
Copyright: © 2012 Sá, Pinto, Cunha, Lemos, Letra, Simões and Santana. This is an open-access article distributed under the terms of the Creative Commons Attribution Non Commercial License, which permits non-commercial use, distribution, and reproduction in other forums, provided the original authors and source are credited.
*Correspondence: Francisca Sá, Neurology Service of the Hospital de Faro E.P.E, Faro 8000, Portugal. e-mail: franciscavieirasa@gmail.com