The Psychological Effects of Short-Term Fasting in Healthy Women
 Ellen Watkins
Ellen Watkins Lucy Serpell
Lucy Serpell- 1East London and City Foundation NHS Trust, London, UK
- 2University College London, London, UK
- 3North East London Foundation NHS Trust, Dagenham, Essex, UK
Objective: The study aimed to investigate affective responses to 18-h fasting in healthy controls. In particular, the study focused on self-reported mood, irritability, sense of achievement, reward, pride, and control.
Method: Participants were a non-clinical sample of 52 women with a mean age of 25. A repeated-measures design was used, whereby participants provided diary measures of psychological variables throughout both 18-h fasting and non-fasting periods.
Results: Fasting led to increased irritability, and also to positive affective experiences of increased sense of achievement, reward, pride, and control.
Discussion: Even short-term fasting in healthy controls can lead to positive psychological experiences. This lends support to cognitive-behavioral and cognitive-interpersonal models of ANR, which suggest that dietary restriction is maintained through positive reinforcement.
Introduction
By definition, individuals with anorexia nervosa (AN) severely restrict their food intake, which can be seen as a mixture of both short-term food deprivation and chronic malnourishment (1, 2). While short-term fasting in healthy individuals has significant differences from the chronic calorie deprivation seen in AN, fasting in healthy participants can offer some clues to the cognitive and emotional changes in AN (3, 4). There is limited research into the psychological effects of starvation in healthy individuals, however, existing research has mainly focused on negative affective and cognitive changes, such as increased anxiety and irritability and poorer concentration (5–7), and increased rigidity and obsessionality (5). Interestingly, studies have indicated that unintentional weight loss can trigger AN (8, 9). This points toward the possibility that starvation itself may have an impact on the development or maintenance of AN (10).
Several models of the development and treatment of AN inherently assume that dietary restriction leads to positive affective experiences. The cognitive-behavioral model posits that AN is maintained, in part, by positive reinforcement from successful restriction [for example, Ref. (11–14)]. Other models, for example, Schmidt and Treasure (15) cognitive-interpersonal approach, also incorporate positive experiences as a result of dietary restriction as important maintaining factors in AN. However, no studies in healthy individuals have as yet focused on the possible positive emotional consequences of fasting in experimentally induced starvation.
The Current Study and Hypotheses
The study aimed to investigate individual responses to short-term fasting. The study aimed to determine whether fasting would lead to increases in measures of positive mood, reward, hunger, irritability, achievement, pride, and self-control. Due to the scarcity of literature on the psychological consequences of fasting, no directional hypotheses were made.
Materials and Methods
Participants
Participants were 52 female volunteers with a mean age of 25.52 years (range 18–56). Participants were eligible if they were healthy, female, aged over 18, and spoke fluent English. Exclusion criteria included current diagnosis of an eating disorder (ED), pregnancy, or knowingly having any medical condition that would make fasting dangerous, such as diabetes. The largest ethnic group in the sample was Chinese (N = 15, 28.8%), followed by White Other (N = 11, 21.1%), White British (N = 8, 15.4%), and Other (N = 7, 13.5%). All participants were educated to at least GCSE level, and most were current students (N = 31, 59.6%) or employed (N = 7, 13.5%). Participants were paid £15 or, if they were an undergraduate student, had the option of receiving course credits for their time.
Sample Size
A power analysis for this study was carried out based on estimates of effect size from ED research comparing a clinical sample with healthy controls (16, 17). It was estimated that a sample size of 34, with an alpha level of 0.05 would provide 80% power to detect a medium effect size.
Procedure
The study took place at University College London (UCL) from November 2011 to June 2013. Ethical approval was granted by the UCL Research Ethics Committee. To minimize the risks of fasting, participants were given advice and information on fasting and its possible risks, and were informed to immediately stop fasting if they felt unwell.
Study Design
The study used a within subjects, repeated-measures design to test individuals’ responses to 18-h fasting and non-fasting periods. Participants met with researchers on three occasions; the first meeting consisted of a screening questionnaire and completion of ED and mood measures. The second and third meetings followed the fasting and non-fasting conditions.
Participants were required to independently complete both an 18-h fasting and an 18-h non-fasting period, which were at least a week apart to ensure no carry over effects of fasting. During the fasting period, participants were asked not to consume any food or drink other than water. Participants were asked to be truthful about whether they had adhered to fasting conditions. In order to promote adherence, participants were informed that a random sample of participants would be asked to provide a urine sample to check levels of ketones, biological markers of fasting. No urine samples were actually obtained as ketone levels are not an accurate indicator of fasting adherence due to biological homeostatic mechanisms (3, 18). During the non-fasting period, participants were told to eat and drink normally.
Participants completed visual analog scales (VASs) diary measures throughout both fasting and non-fasting periods. At the end of both conditions, participants met with researchers to provide their completed self-report measures and, at the end of the third meeting, participants were reimbursed and debriefed. Figure 1 shows a flow chart of the study process.
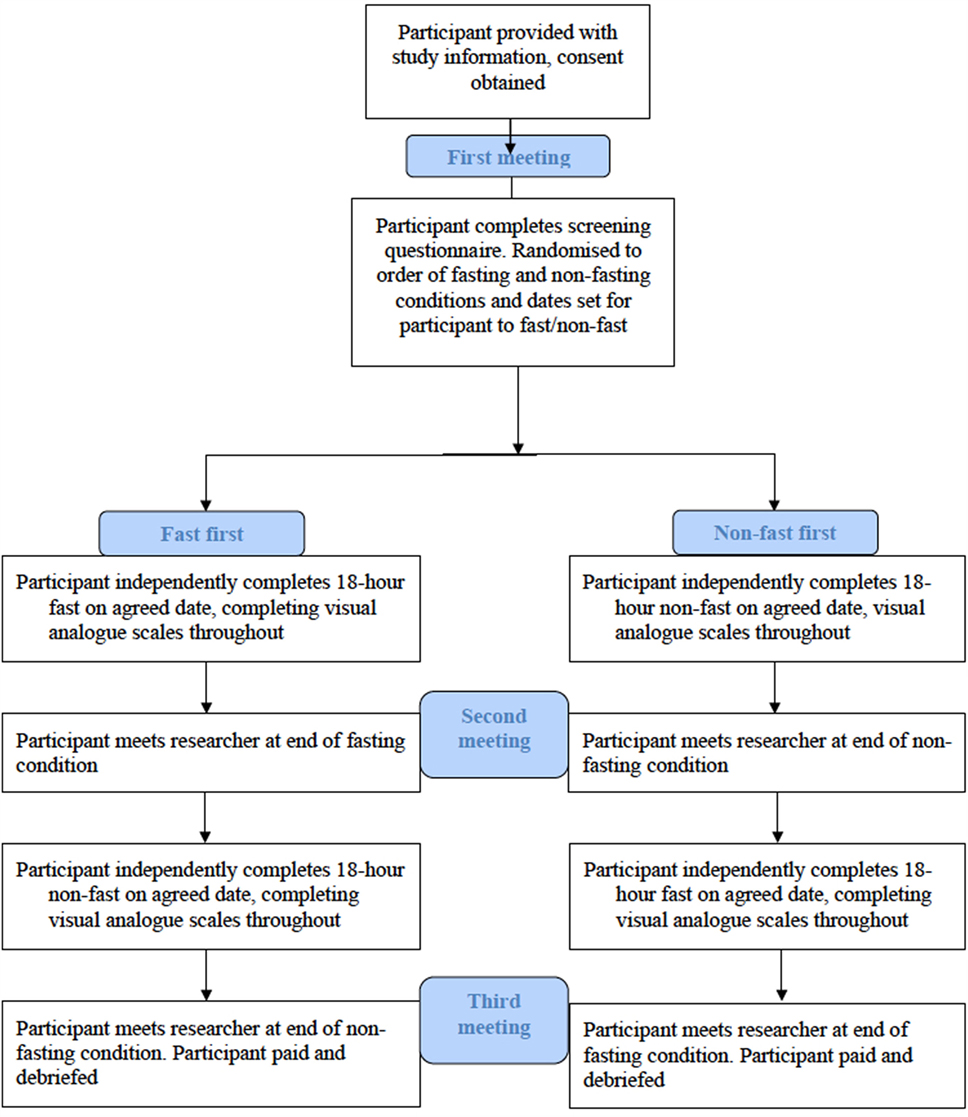
Figure 1. Flow chart of the study design.
Measures
Screening Questionnaire
At the initial meeting, participants completed a screening questionnaire, which included basic demographic questions about current physical and mental health, and history of EDs. Participants were also asked the number of meals they usually ate in a day, whether they had fasted before, and how they anticipated they would find fasting. Additionally, participants were asked to rate their mood on a VAS ranging from 0 (“not at all happy”) to 10 (“happiest I could be”).
Self-Reported ED Pathology
To screen for ED symptomatology, the Eating Disorder Examination Questionnaire [EDE-Q6; (19)] was used. This is a 28-item self-report questionnaire, providing four subscale scores; dietary restraint, shape concern, weight concern, and eating concern, as well as a global score. A study indicated that the EDE-Q6 has adequate reliability and validity in community samples (20).
Self-Reported Depression and Anxiety
Participants completed the Hospital Anxiety and Depression Scale [HADS; (21)], which is a widely used 14-item self-report measure with seven anxiety and seven depression items. It provides separate subscale scores for anxiety and depression, as well as an overall score.
VAS Diary Measures
During the fasting condition, participants were asked to rate mood, reward from fasting, sense of achievement, sense of self-control, and difficulty fasting, using VASs ranging from zero (“not at all”) to 10 (“extremely”). Measures were completed every 2 h throughout the fasting day, giving a total of five measures. Participants also provided VAS scores at the beginning of the fasting period to give a baseline. Similarly, throughout the non-fasting condition, participants were also asked to rate mood, irritability, sense of self-control, and sense of achievement so that participants acted as their own controls by providing data on a non-fasting day.
Randomization
Participants were randomized to complete either the fasting or non-fasting condition first. For allocation to condition, a computer-generated list of random numbers was used, participants of which were assigned to in the order that they entered the study.
Statistical Analyses
Data were analyzed using SPSS 19.0 for Windows. All statistical tests used a 0.5 significance level. All participants’ data were analyzed together, and there were no outliers or data excluded. Effect of fasting was assessed using paired samples t-tests comparing VAS data before and after fasting. A repeated-measures ANOVA was used to assess whether there was a main effect of fasting.
Results
Previous Fasting
Most participants had not fasted before (73.1%, N = 38). Fourteen participants had fasted previously (26.92%). Of these, nine had done so for dietary or health reasons, and five had done so for religion.
Self-Reported Eating Disorders
Mean BMI was 21.19 (SD = 3.22, range 15.80–30.70). Eight participants had a BMI below the World Health Organisation (22) clinical cut-off of <18.5 kg/m2. Of these, none scored in the clinical range on any EDE-Q subscales.
Mean scores on all EDE-Q subscales were higher than in Fairburn and Beglin (19) normative sample. Mean scores on global, restraint, shape concern, and weight concern subscales were within one SD of Fairburn and Beglin’s norms. Mean eating concern score was within two SDs of the norm.
Self-Reported Depression and Anxiety
The mean anxiety score was 5.57 (SD = 4.17, range 0–18) and mean depression score was 2.82 (SD = 2.83, range 0–12). These are within one SD of norms found in non-clinical populations previously (23).
Effect of Fasting
Paired samples t-tests were used to compare mean scores on VAS measures at the start of fasting (F1) and end of fasting (F6). Significance values were Bonferroni corrected to control risk of type-I error. All paired samples t-tests can be seen in Table 1. At the end of fasting, participants were significantly hungrier, more irritable, had a significantly higher sense of achievement, pride, and self-control than at the start of fasting. Participants also rated fasting as increasingly difficult throughout the fasting period. Difficulty rating at the end of the fasting period (F6) was significantly correlated with hunger, r = 0.67, p > 0.001, and irritability, r = 0.68, p > 0.001, at the end of fasting.
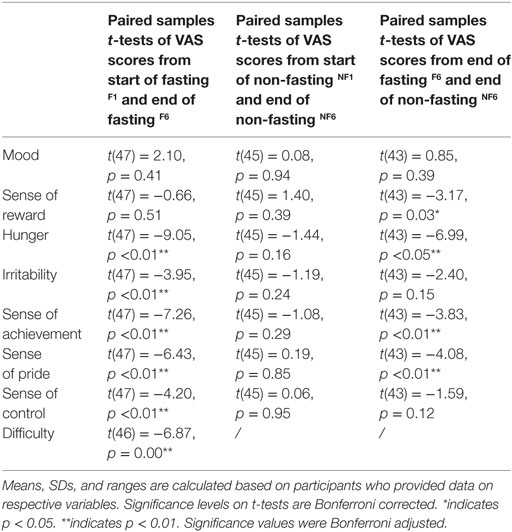
Table 1. Paired samples t-tests comparing mean scores on VAS measures from start of fasting (F1) to end of fasting (F6), start of non-fasting (NF1) to end of non-fasting (NF6) and comparing scores on VAS measures at the end of fasting (F6) and end of non-fasting (NF6).
By contrast, paired samples t-tests showed that there was no significant difference on any VAS measures from the start of the non-fasting period (NF1) to the end of non-fasting (NF6).
T-tests were also performed comparing mean scores on VAS measures from the end of fasting F6 and end of non-fasting NF6 periods. These showed that at the end of fasting compared to the end of non-fasting participants experienced a significantly higher sense of reward, were significantly more hungry, had a significantly higher sense of achievement, and a significantly higher sense of pride.
A repeated-measures ANOVA revealed that there was a significant main effect of fasting on VAS measures, F(1, 41) = 46.92, p < 0.05. There was a significant interaction effect between fasting condition and VAS measure rating, F(4.31, 176.56) = 12.09, p = < 0.05, suggesting that fasting impacted on participants’ subjective psychological experiences.
Discussion
The current study set out to explore the impact of short-term fasting on psychological experiences, including positive moods in healthy participants. The hypothesis that fasting would affect psychological variables was supported. As fasting progressed, participants reported that it was increasingly difficult and they became hungrier, however, they also experienced an increased sense of achievement, pride, and control. Although sense of reward did not increase significantly from start to end of fasting, this may be due to the fact that, even at the very start of fasting, participants reported having a higher sense of reward. Sense of reward did continue to increase throughout fasting, though not significantly. At the start of non-fasting, sense of reward was rated as lower and this decreased throughout non-fasting, leading to a significantly higher sense of reward at the end of fasting than at the end of non-fasting.
Previous research has suggested that fasting results in biological symptoms of depression, such as irritability, mood lability, and low libido (24, 25). The results of the current study support these findings, as participants reported feeling increasingly irritable throughout fasting but did not report significant changes in overall mood.
However, as well as negative emotional correlates, this study also found that positive affective experiences, such as a sense of achievement, were associated with the fasting process. While care must be taken in extrapolating from short-term fasting to AN, these findings are at least consistent with cognitive-behavioral or cognitive-interpersonal models of AN, which postulate that AN is maintained partly by positive reinforcement from successful dietary restriction [for example, Ref. (11–15)]. These authors suggest that food restriction is partly reinforced by a variety of resultant positive feelings, such as a sense of control, power, satisfaction, or pride. Previous research indicates that sufferers of AN experience both pros and cons of the disorder. Pros of AN may include making sufferers feel special through their ability to maintain dietary restriction (26). To our knowledge, this is the first study showing that positive feelings can be generated even from short-term fasting in healthy controls. These findings may go some way to elucidating how extreme dietary restriction in AN may begin in vulnerable individuals from even short-term fasting or normal dieting leading to increases in positive mood states. The results may lend support to cognitive-behavioral or cognitive-interpersonal treatment models of AN, which often incorporate exploration of the factors that positively reinforce dietary restriction, and the pro-anorectic beliefs the individual holds.
Limitations of the Study
The study relied on self-report data, which is potentially more fallible than data from objective assessments or semi-structured interviews due to social desirability bias, distortion, or participants misunderstanding questions. Furthermore, data from the fasting and non-fasting periods was completed independently by participants. Although we asked participants not to retrospectively complete missed data points, they may have done so, and we had no way of checking this. However, many participants missed data at one time point (often first thing in the morning), suggesting that, on the whole, they did not retrospectively complete measures, leaving them blank instead.
Data from the fasting and non-fasting periods were obtained using VASs as it was not possible to repeatedly use standardized measures of constructs, such as low mood, which often refer to longer time periods, such as 2 weeks. The VASs provided a simple, fast, repeatable way of obtaining data without overwhelming participants. However, there were shortcomings to gathering data in this way, such as participants having different conceptualizations of affective labels, and positioning of marks not necessarily being comparable across individuals. This was overcome to some extent with the repeated-measures design, which meant that participants acted as their own controls. However, it may be beneficial to repeat this research with use of more standardized measures.
Researchers did not objectively assess whether participants had EDs, other than by using self-reported ED status and the EDE-Q as a screening tool. Future studies should use a full clinical screen to ensure that no participant meets criteria for an ED. Additionally, researchers had no way of determining whether or not participants had adhered to fasting conditions. However, the difference in VAS measures between fasting and non-fasting suggests that participants did fast. Researchers and participants were aware of the condition; therefore, responses on VAS measures could have been biased by participants’ expectations of the effects of fasting. It was not possible in this brief exploratory study to obtain self-report data on dietary intake on non-fasting days, nor on physical activity. Future studies should include these data.
The study was exploratory in nature. Due to this, and having multiple hypotheses, multiple statistical tests were used, thereby increasing the risk of type-I error. Corrections were performed to account for this, however, it would be of benefit to repeat this research with a larger sample to allow for more rigorous statistical testing.
Generalizability of the results to people with EDs is limited by the fact that the sample was non-clinical and mostly comprised students. It would be of benefit to replicate the research with a clinical sample, although this may raise ethical concerns, in light of research on the effects of starvation.
The largest ethnic group in the sample was Chinese, which may have led to errors in completing questionnaires, although all participants described themselves as fluent English speakers. Furthermore, it may also have resulted in participants having lower overall body weight (27). However, all participants in the study were living and studying in the U.K.
The study may have attracted individuals who liked fasting, or experienced ED pathology. This would bias the results, particularly if participants regularly fasted for religious reasons and associated it with positive effects. However, most participants reported that they had never fasted. Moreover, fasting was rated as increasingly difficult over time, indicating that even those who had fasted before found it difficult. In addition, participants may have been attracted by the monetary reward rather than an interest in EDs or fasting.
Strengths of the Study
Several strengths of the study must also be acknowledged, including the within-subjects design whereby participants acted as their own controls. Additionally, asking participants to provide VAS measures of psychological variables two-hourly throughout the fasting period meant that we obtained rich data. To the best of our knowledge, this is one of the only studies to explore the effect of short-term fasting on psychological variables in healthy controls.
Conclusion
The results showed that fasting led not only to negative affective states, such as irritability, but also to positive psychological experiences, such as increased sense of reward, achievement, pride, and control as participants reported increasing hunger and difficulty of fasting. To our knowledge, this is one of the only studies showing that these positive psychological experiences can result from fasting, even in healthy controls. These findings lend support to cognitive-behavioral and cognitive-interpersonal models of AN, which suggest that fasting is maintained partly through positive reinforcement, and may elucidate how extreme dietary restriction can result from ordinary dieting or fasting.
Ethics Statement
This study was carried out in accordance with the recommendations of the Ethics Committee at University College London with written informed consent from all participants. All participants gave written informed consent in accordance with the Declaration of Helsinki.
Author Contributions
LS and EW conceived of the study and developed the hypotheses. EW drafted the manuscript and LS made substantial contributions to the writing process.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Sidiropoulos M. Anorexia nervosa: the physiological consequences of starvation and the need for primary prevention effects. Mcgill J Med (2007) 10:20–5.
2. Vitousek K, Manke F. Personality variables and disorders in anorexia nervosa and bulimia nervosa. J Abnorm Psychol (1994) 103:137–47. doi:10.1037/0021-843X.103.1.137
3. Bolton H, Burgess P, Gilbert S, Serpell L. Increased set shifting costs in fasted healthy volunteers. PLoS One (2014) 9(7):e101946. doi:10.1371/journal.pone.0101946
4. Pender S, Gilbert S, Serpell L. The neuropsychology of starvation: set-shifting, central coherence in a fasted nonclinical sample. PLoS One (2014) 9(10):e110743. doi:10.1371/journal.pone.0110743
5. Keys A, Brozek J, Henschel A, Mickelson O, Taylor HL. The Biology of Human Starvation. Minneapolis: Minneapolis7 University of Minnesota Press (1950).
6. Laessle RG, Schweiger U, Pirke KM. Depression as a correlate of starvation in patients with eating disorders. Biol Psychiatry (1988) 23:719–25. doi:10.1016/0006-3223(88)90056-X
7. Laessle R, Platte P, Schweiger U, Pirke K. Biological and psychological correlates of intermittent dieting behavior in young women. A model for bulimia nervosa. Physiol Behav (1996) 60:1–5. doi:10.1016/0031-9384(95)02215-5
8. Epling WF, Pierce WD, Stefan L. A theory of activity-based anorexia. Int J Eat Disord (1983) 3:27–46. doi:10.1002/1098-108X(198323)
9. Kingston K, Szmukler G, Andrwes D, Tress B, Desmond P. Neuropsychological and structural brain changes in anorexia nervosa before and after refeeding. Psychol Med (1996) 26:15–28. doi:10.1017/S0033291700033687
10. Serpell L, Treasure J, Teasdale J, Sullivan V. Anorexia nervosa: friend or foe? A qualitative analysis of the themes expressed in letters written by anorexia nervosa patients. Int J Eat Disord (1999) 25:177–86. doi:10.1002/(SICI)1098-108X(199903)25:2<177::AID-EAT7>3.3.CO;2-4
11. Fairburn C, Shafran R, Cooper Z. A cognitive behavioural theory of anorexia nervosa. Behav Res Ther (1998) 37:1–13. doi:10.1016/S0005-7967(98)00102-8
12. Garner DM, Bemis KM. A cognitive-behavioral approach to anorexia nervosa. Cognit Ther Res (1982) 6:123–50. doi:10.1007/BF01183887
13. Slade PD. Towards a functional analysis of anorexia nervosa and bulimia nervosa. Br J Clin Psychol (1982) 21:167–79. doi:10.1111/j.2044-8260.1982.tb00549.x
14. Vitousek KB, Ewald LS. Self-representation in eating disorders: a cognitive perspective. In: Segal ZV, Blatt SJ, editors. The Self in Emotional Distress: Cognitive and Psychodynamic Perspectives. New York: Guilford (1993). p. 221–66.
15. Schmidt U, Treasure J. Anorexia nervosa: valued and visible. A cognitive-interpersonal maintenance model and its implications for research and practice. Br J Clin Psychol (2006) 45(Pt 3):343–66. doi:10.1348/014466505X53902
16. Lopez C, Tchanturia K, Stahl D, Treasure J. Weak central coherence in eating disorders: a step towards looking for an endophenotype of eating disorders. J Clin Exp Neuropsychol (2009) 31:117–25. doi:10.1080/13803390802036092
17. Roberts M, Tchanturia K, Stahl D, Southgate L, Treasure J. A systematic review and meta-analysis of set-shifting ability in eating disorders. Psychol Med (2007) 37:1075–84. doi:10.1017/S0033291707009877
18. Connan F, Stanley S. Biology of appetite and weight regulation. In: Treasure J, Schmidt U, Van Furth E, editors. The Handbook of Eating Disorders. Chichester: John Wiley & Sons (2003). p. 63–88.
19. Fairburn CG, Beglin SJ. Assessment of eating disorder psychopathology: interview or self-report questionnaire? Int J Eat Disord (1994) 16:363–70. doi:10.1002/1098-108X(199412)
20. Passi V, Bryson S, Lock J. Assessment of eating disorders in adolescents with anorexia nervosa: self-report versus interview. Int J Eat Disord (2003) 33:45–54. doi:10.1002/eat.10113
21. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand (1983) 67:361–70. doi:10.1111/j.1600-0447.1983.tb09716.x
22. World Health Organisation. International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10). Geneva: WHO (2010).
23. Crawford JR, Henry JD, Crombie C, Taylor EP. Brief report. Normative data for the HADS from a large non-clinical sample. Br J Clin Psychol (2001) 40:429–34. doi:10.1348/014466501163904
24. Choma CW, Sforzo GA, Keller BA. Impact of rapid weight loss on cognitive function in collegiate wrestlers. Med Sci Sports Exerc (1998) 30(5):746–9. doi:10.1097/00005768-199805000-00016
25. Maridakis V, Herring MP, O’Connor PJ. Sensitivity to change in cognitive performance and mood measures of energy and fatigue in response to differing doses of caffeine or breakfast. Int J Neurosci (2009) 119(7):975–94. doi:10.1080/00207450802333995
26. Serpell L, Teasdale J, Troop N, Treasure J. The development of the P-CAN: a scale to operationalise the pros and cons of anorexia nervosa. Int J Eat Disord (2004) 36:416–33. doi:10.1002/eat.20040
Keywords: healthy individuals, fasting, starvation, psychology, emotions
Citation: Watkins E and Serpell L (2016) The Psychological Effects of Short-Term Fasting in Healthy Women. Front. Nutr. 3:27. doi: 10.3389/fnut.2016.00027
Received: 23 March 2016; Accepted: 28 July 2016;
Published: 22 August 2016
Edited by:
Julia M. Hormes, University at Albany SUNY, USAReviewed by:
Nicholas T. Bello, Rutgers University, USAUlrich Schweiger, Lübeck University Medical School, Germany
Copyright: © 2016 Watkins and Serpell. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lucy Serpell, lucy@serpell.com