Commentary: Randomized Phase II Study of Duligotuzumab (MEHD7945A) vs. Cetuximab in Squamous Cell Carcinoma of the Head and Neck (MEHGAN Study)
 Jérôme Fayette1*
Jérôme Fayette1* Lori Wirth2
Lori Wirth2 Cristina Oprean3Anghel Udrea4Antonio Jimeno5Danny Rischin6Christopher Nutting7Paul M. Harari8
Cristina Oprean3Anghel Udrea4Antonio Jimeno5Danny Rischin6Christopher Nutting7Paul M. Harari8 Tibor Csoszi9
Tibor Csoszi9 Dana Cernea10Paul O’Brien11William D. Hanley12Amy V. Kapp12Maria Anderson12Elicia Penuel12Bruce McCall12Andrea Pirzkall12
Dana Cernea10Paul O’Brien11William D. Hanley12Amy V. Kapp12Maria Anderson12Elicia Penuel12Bruce McCall12Andrea Pirzkall12 Jan B. Vermorken13
Jan B. Vermorken13
- 1Centre Léon Bérard, Université de Lyon, Lyon, France
- 2Massachusetts General Hospital, Boston, MA, USA
- 3Oncomed SRL, Timisoara, Romania
- 4Medisprof SRL, Cluj-Napoca, Romania
- 5University of Colorado Cancer Center, Aurora, CO, USA
- 6Peter MacCallum Cancer Centre, University of Melbourne, Melbourne, VIC, Australia
- 7Royal Marsden NHS Trust, The Institute of Cancer Research London, Sutton, UK
- 8University of Wisconsin Hospital and Clinics, Madison, WI, USA
- 9Jász-Nagykun-Szolnok Megyei Hetényi Géza Kórház, Szolnok, Hungary
- 10Institutul Oncologic Prof. Dr. Ion Chiricuta Cluj-Napoca, Cluj-Napoca, Romania
- 11Medical University of South Carolina, Charleston, SC, USA
- 12Genentech, South San Francisco, CA, USA
- 13Antwerp University Hospital, Edegem, Belgium
Background: Duligotuzumab, a novel dual-action humanized IgG1 antibody that blocks ligand binding to epidermal growth factor receptor (EGFR) and human epidermal growth factor receptor 3 (HER3), inhibits signaling from all ligand-dependent HER dimers, and can elicit antibody-dependent cell-mediated cytotoxicity. High tumor-expression of neuregulin 1 (NRG1), a ligand to HER3, may enhance sensitivity to duligotuzumab.
Methods: This multicenter, open-label, randomized phase II study (MEHGAN) evaluated drug efficacy in patients with recurrent/metastatic (R/M) squamous cell carcinoma of the head and neck (SCCHN) progressive on/after chemotherapy and among patients with NRG1-high tumors. Patients received duligotuzumab (1100 mg IV, q2w) or cetuximab (400 mg/m2 load, 250 mg/m2 IV, q1w) until progression or intolerable toxicity. Tumor samples were assayed for biomarkers [NRG1, ERBB3, and human papillomavirus (HPV) status].
Results: Patients (N = 121) were randomized (duligotuzumab:cetuximab; 59:62), median age 62 years; ECOG 0–2. Both arms (duligotuzumab vs. cetuximab, respectively) showed comparable progression-free survival [4.2 vs. 4.0 months; HR: 1.23 (90% confidence interval (CI): 0.89–1.70)], overall survival [7.2 vs. 8.7 months; HR 1.15 (90% CI: 0.81–1.63)], and objective response rate (12 vs. 14.5%), with no difference between patients with NRG1-high tumors or ERBB3-low tumors. Responses in both arms were confined to HPV-negative patients. Grade ≥3 adverse events (AEs) (duligotuzumab vs. cetuximab, respectively) included infections (22 vs. 11.5%) and GI disorders (17 vs. 7%), contributing to higher rates of serious AEs (41 vs. 29.5%). Metabolic disorders were less frequent with duligotuzumab (10 vs. 16%); any grade rash-related events were less with duligotuzumab (49 vs. 67%).
Conclusion: While several lines of preclinical evidence had supported the premise that the blockade of HER3 in addition to that of EGFR may improve outcomes for patients with R/M SCCHN overall or specifically in those patients whose tumors express high levels of NRG1, this study provided definitive clinical evidence refuting this hypothesis. Duligotuzumab did not improve patient outcomes in comparison to cetuximab despite frequent expression of NRG1. These data indicate that inhibition of EGFR alone is sufficient to block EGFR–HER3 signaling, suggesting that HER2 plays a minimal role in this disease. Extensive biomarker analyses further show that HPV-negative SCCHN but not HPV-positive SCCHN are most likely to respond to EGFR blockage by cetuximab or duligotuzumab.
Introduction
Multiple members of the HER family receptor tyrosine kinases, including epidermal growth factor receptor (EGFR), HER1, and HER2, are established therapeutic targets in several epithelial malignancies (1). EGFR is a rational focus for squamous cell carcinoma of the head and neck (SCCHN) given the prevalence of its overexpression and crucial role in SCCHN pathogenesis (2, 3). Moreover, EGFR is a clinically validated therapeutic target in recurrent/metastatic SCCHN with approval of cetuximab as a single agent (4), concurrent with platinum-based chemotherapy (5), and in combination with radiotherapy in the curative SCCHN setting (6). Many SCCHN patients do not respond to cetuximab therapy, and for those who do, they commonly manifest acquired resistance following prolonged exposure to the drug. These findings have prompted the design of next-generation EGFR inhibitors and approaches that may serve to overcome resistance to cetuximab.
Factors thought to contribute to cetuximab resistance in SCCHN patients include upregulation of ligands for EGFR and human epidermal growth factor receptor 3 (HER3) (7, 8), heterodimerization of EGFR and HER2 with HER3 (9), overexpression of HER2 and HER3 (10), and overexpression and aberrant nuclear localization of EGFR (11). Interestingly, a subset of SCCHN cell lines are resistant to anti-EGFR tyrosine kinase inhibitor (TKI) treatment and do not overexpress HER2 but are sensitive to combined anti-EGFR/anti-HER2 TKI inhibition (12). Many of these cell lines were found to have high expression of heregulin (HRG), the ligand binding to HER3, and activation of HER3 signaling. It was hypothesized that such cells may escape the effects of anti-EGFR therapy via HRG-dependent signaling of a HER2/HER3 dimer. An analysis of >700 tumor samples from patients with non-small cell lung cancer (NSCLC), SCCHN, colorectal, breast, or ovarian cancer found that median HRG mRNA expression is significantly higher in SCCHN tumors than in the other tumor types (13). HRG represents alpha and beta forms of neuregulin 1 (14) and is here forth referred to as NRG1.
Duligotuzumab (MEHD7945A) is a novel dual-action human IgG1 monoclonal antibody that simultaneously targets HER3 and EGFR (15). HER3 is encoded by the ERBB3 gene. Duligotuzumab demonstrated superior activity compared with mono-specific EGFR- or HER3-targeting antibodies in the non-clinical FaDu SCCHN model (16), as well as in human xenograft models derived from SCCHN and NSCLC tumors with acquired resistance to EGFR inhibitors (17). Preliminary evidence of clinical activity included two confirmed partial responses (PRs) in SCCHN patients (18) who had entered the duligotuzumab phase Ia study after progressing on prior therapy, one having relapsed after multiple prior treatment regimens including an EGFR inhibitor. Both patients’ tumors were found to have NRG1 expression near the top of the range observed in the analysis of tumor samples described above.
Taken together, these observations suggested that the addition of HER3 blockade to EGFR blockade with duligotuzumab may improve clinical outcomes in patients with recurrent or metastatic (R/M) SCCHN overall or specifically in those patients whose tumors express high levels of NRG1. This phase II study evaluated the efficacy of duligotuzumab vs. cetuximab in patients with R/M SCCHN progressive on/after chemotherapy and included post hoc analyses by NRG1 expression levels, ERBB3 expression levels, and human papillomavirus (HPV) status.
Methods
Patients
Eligible patients were ≥18 years of age with histologically confirmed R/M SCCHN who had progressed after one or more lines of treatment, at least one platinum-based regimen for R/M disease, and not suitable for local therapy. Patients with ECOG performance status of 0, 1, or 2, disease measurable per RECIST v1.1, adequate hematologic, renal, or hepatic function, no prior HER targeted therapy with exception of EGFR inhibitor given in upfront setting and as long as discontinued ≥3 months prior to enrollment were included. Patients were excluded if they had nasopharyngeal cancer.
Study Design
This was a phase II, randomized, multicenter, open-label study with two arms (Figure 1) assessing duligotuzumab vs. cetuximab in R/M SCCHN patients. Institutional review boards at all participating institutions approved the study protocol. All patients gave written informed consent. The study was conducted according to good clinical practice (GCP), and the Declaration of Helsinki and its amendments, and was registered at http://ClinicalTrials.gov, number NCT01577173 (19).
FIGURE 1
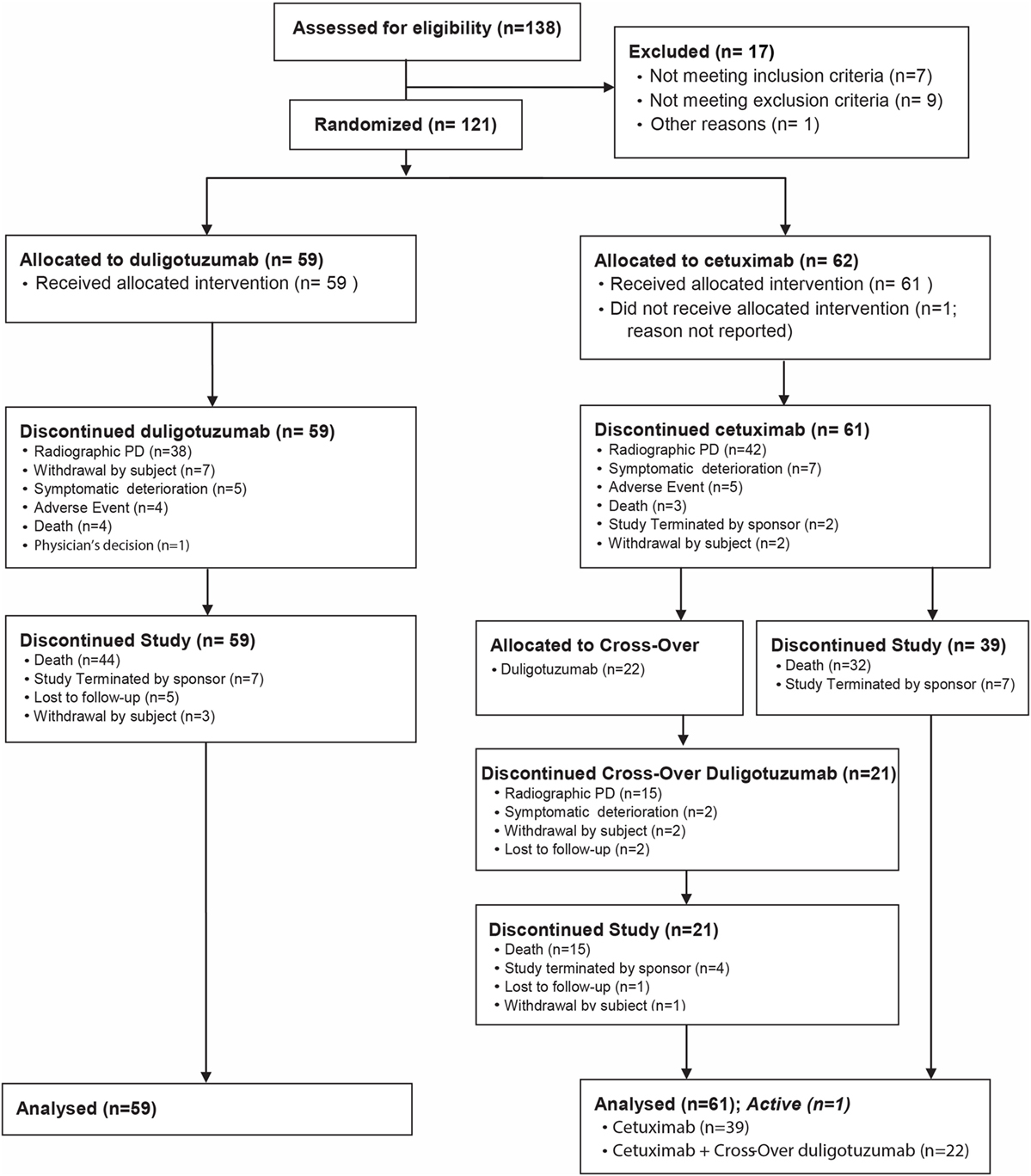
Figure 1. Study design.
Patients received duligotuzumab, 1100 mg IV, administered every 2 weeks (Arm A), or cetuximab, 400 mg/m2 loading dose, 250 mg/m2 IV, administered weekly (q1w) (Arm B). Patients were randomized to one of the two treatment arms in a 1:1 ratio using an interactive voice response system (IVRS). Stratification factors included ECOG 0/1 vs. 2 and time to platinum failure (≤2 vs. >2 months). Patients were treated with either study drug until disease progression or other unacceptable toxicity. Patients with disease progression on Arm B (cetuximab) could cross over to Arm A (duligotuzumab) upon central confirmation of progressive disease (PD) (RECIST v1.1), and as long as principal eligibility criteria were met.
The primary endpoint was progression-free survival (PFS) by investigator assessment in all randomized patients [intention to treat (ITT) population] and in the subset with highest NRG1 expression in the tumor. NRG1 was assessed by qRT-PCR at Genentech. Secondary objectives included overall survival (OS), overall response rate (ORR), safety/tolerability, and characterization of pharmacokinetics (PKs) and anti-therapeutic antibodies (ATA) from patients treated on Arm A. Exploratory objectives included assessing tumor samples from patients for the prevalence and potential prognostic significance of NRG1 and ERBB3, and HPV status and its potential association with antitumor activity.
Safety
Safety was assessed by incidence, nature, severity, and relatedness of adverse events (AEs) and graded for severity (NCI-CTCAE v4.0). All patients who received ≥1 dose of study treatment were included in the safety evaluation. The following events were categorized as of special interest: grade ≥3 events associated with infusion-related reactions (defined as AEs within 24 h of infusion and attributed to study drug), grade ≥3 rash, and grade ≥3 diarrhea.
Pharmacokinetics
Serum samples were collected at screening, day 1 of cycles 1–8, and treatment completion. Duligotuzumab concentration was determined using a qualified enzyme-linked immunosorbent assay with the minimum quantifiable concentration of 150 ng/mL. PK parameters were derived from non-compartmental analysis (NCA) (WinNonlin version 5.2.1.). A population PK analysis of duligotuzumab from phase Ia study DAF4873g (data on file) demonstrated that body weight has only a minor impact on PK parameters [volume of distribution (Vd) and clearance (CL)], thus supporting that flat dosing would have little effect on duligotuzumab PK variability in comparison with weight-based dosing.
Serum anti-duligotuzumab antibody (ATA) samples were collected prior to duligotuzumab infusion on day 1 of cycles 1–8, and at the study termination visit, and were analyzed using a validated bridging antibody immunoassay that could detect surrogate anti-duligotuzumab positive-control antibody (249 ng/mL) in the absence of duligotuzumab.
Biomarker Analyses
Mandatory archival (or fresh as available) tumor tissues were evaluated to characterize the disease biology and to identify potential predictive biomarkers for improved outcomes with duligotuzumab compared to cetuximab, with particular attention to the HER3 ligand, NRG1. For NRG1 and receptor tyrosine kinase erbB-3 (ERBB3), RNA expressions were measured by both qRT-PCR and by dual-colored in situ hybridization (ISH). Additionally, HPV detection was performed by qRT-PCR.
Efficacy
Tumor assessments were performed at screening and during every 6 weeks of study treatment (e.g., prior to cycle 4 and every 6 weeks thereafter), and at the treatment completion visit for patients who discontinue for reason other than PD. Response assessments were performed by the investigators according to RECIST v1.1. The primary endpoint was PFS, defined as the time from randomization to the first occurrence of progression or death, whichever occurred first. Secondary endpoints included OS (defined as the time from randomization to death) and objective response defined as complete response (CR) or PR confirmed ≥4 weeks after initial documentation. Unless stated otherwise, analyses excluded data after crossover.
Sample Size
This trial was designed to obtain informative estimates of the PFS hazard ratios in the overall patient population, and the NRG1-high patient population to enable further decision making, without adequate power to detect the minimum clinically meaningful difference between the treatment arms at a statistically significant type 1 error level (α = 0.05). Therefore, the utility of formal hypothesis testing was limited because statistically negative outcomes did not necessarily exclude clinically significant treatment effects. Consequently, 90% CIs for the PFS hazard ratios were calculated. In order to observe 90 disease progression or death events in all patients and 35 disease progression or death events in the NRG1-high patients, the study was planned to enroll 110 patients, assuming the prevalence of NRG1-high patients was 40%. For a lower prevalence, additional patients could be enrolled to meet the required number of disease progression or death events in the HRG-high patient population.
Statistical Analysis
Safety analyses included all patients who received any amount of study treatment. Efficacy analyses were conducted on all randomized patients and all randomized NRG1-high patients. For each time-to-event endpoint, Kaplan–Meier analysis was used to estimate the medians in each treatment arm, and Cox regression was used to estimate the hazard ratio.
Results
Patient Population
From July 13, 2012 to July 09, 2013, 121 patients were randomized (59 Arm A, 62 Arm B), of whom 120 were evaluable for safety, 108 for biomarker analysis, and 22 during the crossover phase. The cutoff date for analysis was March 02, 2015, resulting in a minimum follow-up of 19.8 months.
Key baseline characteristics included the stratification factors, ECOG, and time to PD, since most recent platinum treatment were well-balanced overall (Table 1) with the exception of fewer HPV-positive patients and fewer patients with locoregional recurrence only who enrolled on the experimental duligotuzumab arm, as compared to the cetuximab arm. Upon review of staging and prior medical history, it was identified that 25/121 patients were enrolled in the first line (1L) rather than the protocol specified 2L + R/M setting. Those patients had not received prior platinum-based therapy for de novo metastatic (Stage IVc) or for recurrence of locally advanced disease, but rather in the adjuvant or definitive setting. Subset analyses excluding those 25 patients showed no significant impact on the efficacy results.
TABLE 1
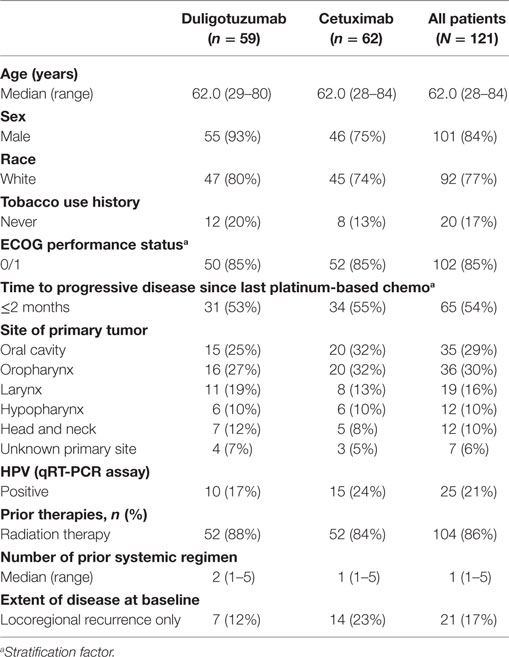
Table 1. Patient characteristics.
Study Treatment
The median number of doses given of duligotuzumab was 7 (range 1–24) and of cetuximab 12 (range 1–59). The median treatment duration for duligotuzumab and cetuximab was 12.4 and 12.0 weeks, respectively. The median relative cumulative dose intensity for duligotuzumab and cetuximab was 87.5 and 89.8%, respectively. Treatment modification or interruption was similar for duligotuzumab and cetuximab, with 42 (71%) patients missing at least one dose in the duligotuzumab arm and 49 (80%) in the cetuximab arm. There were 2 (3%) dose modifications in the duligotuzumab arm and 11 (18%) in the cetuximab arm.
The majority of study treatment discontinuations were due to radiographic disease progression or symptomatic deterioration [73% duligotuzumab (radiographic PD: 64%); 80% cetuximab (radiographic PD: 69%)]. Twenty-two patients crossed over to duligotuzumab after central confirmation of progression on cetuximab. Median treatment duration and cumulative dose intensity were 7.6 months and 88.9% for duligotuzumab, respectively. One patient continues duligotuzumab in the crossover arm.
Safety
The nature and incidence of AEs in the 120 patients evaluable for safety regardless of attribution are summarized (Table 2). The most common AEs were rash (and related terms), infections (MedDRA System Order Class), diarrhea, fatigue, and nausea. The safety profile of duligotuzumab was largely similar to that of cetuximab, however, relative to cetuximab, duligotuzumab was associated with less rash (49 vs. 65%), but more diarrhea (42 vs. 25%), mucosal inflammation (22 vs. 8%), and infection (59 vs. 49%). Grade ≥3 AEs were more frequent in the duligotuzumab arm (61%) vs. the cetuximab arm (51%). Seven deaths (five in the duligotuzumab arm; two in the cetuximab arm), none of which were assessed as related to study treatment, were attributed to underlying disease, disease progression, or an unknown cause.
TABLE 2
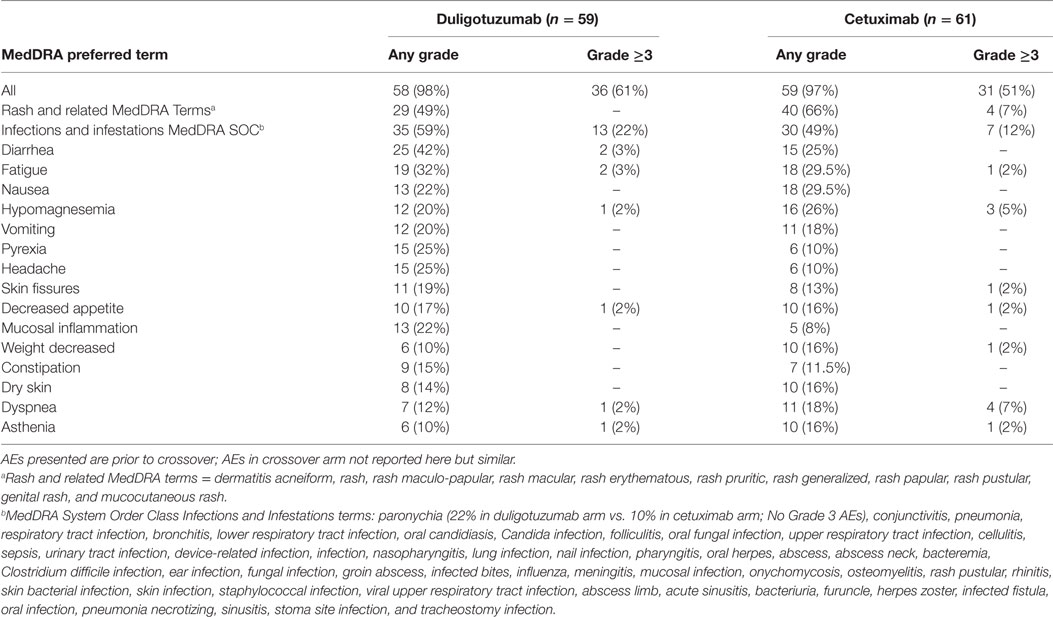
Table 2. Adverse events reported in ≥15% of patients in either arm regardless of attribution.
Infusion-related reactions of headache and fever (events observed within 24 h of treatment and reported as related to study treatment; grade 1–2) had a higher incidence in the duligotuzumab arm (13 vs. 3% for headache and 10 vs. 5% for fever). No allergic type infusion-related reactions were observed in the duligotuzumab arm; anaphylactic reactions to cetuximab were reported in 3% of patients. Discontinuations due to AEs were higher in the cetuximab arm (7% duligotuzumab and 13.5% cetuximab).
Pharmacokinetics
Target exposures of duligotuzumab were achieved in 100% of patients. The mean steady state (cycle 4) duligotuzumab PK parameter values (SD) for predose and Cmax were 82.4 (40.4) and 366 (106) μg/mL, respectively. There was a weak trend observed in PK vs. body weight. No PK differences were detected in patient subpopulations (NRG1 high/low or HPV+/−). ATAs were detected in 2/61 patients (3.3%) and had no impact on PK or safety.
Clinical Activity
In the ITT population, duligotuzumab and cetuximab showed comparable PFS [median 4.2 vs. 4.0 months, respectively, unstratified HR 1.23 (90% CI 0.89–1.70)] and OS [median 7.2 vs. 8.7 months, respectively, unstratified HR 1.15 (90% CI 0.81–1.63)] (Figure 2). PFS and OS subgroup analysis by patient and disease characteristics and stratification factors (ECOG and time to PD since most recent platinum treatment) did not show benefit for duligotuzumab over cetuximab. Objective response and treatment duration were comparable: ORR 12% (7 patients) duligotuzumab vs. 14.5% (9 patients) cetuximab, duration of objective response was median 5.4 months (duligotuzumab) vs. 4.3 months (cetuximab). There was limited evidence of activity in crossover patients (n = 22) (Figure 3).
FIGURE 2
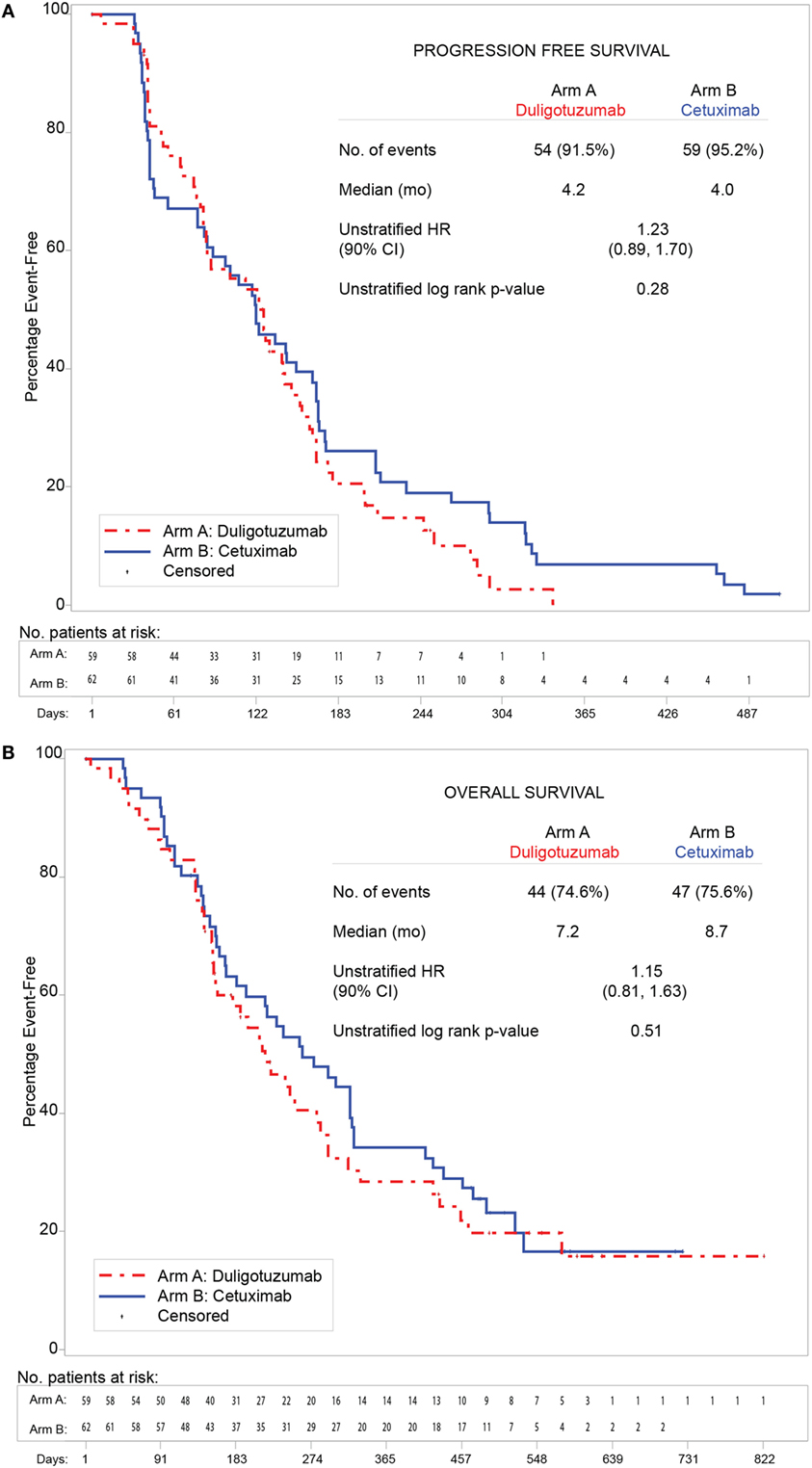
Figure 2. Duligotuzumab vs. cetuximab in intention to treat (ITT) population showing comparable antitumor activity. (A) Progression-free survival. (B) Overall survival.
FIGURE 3
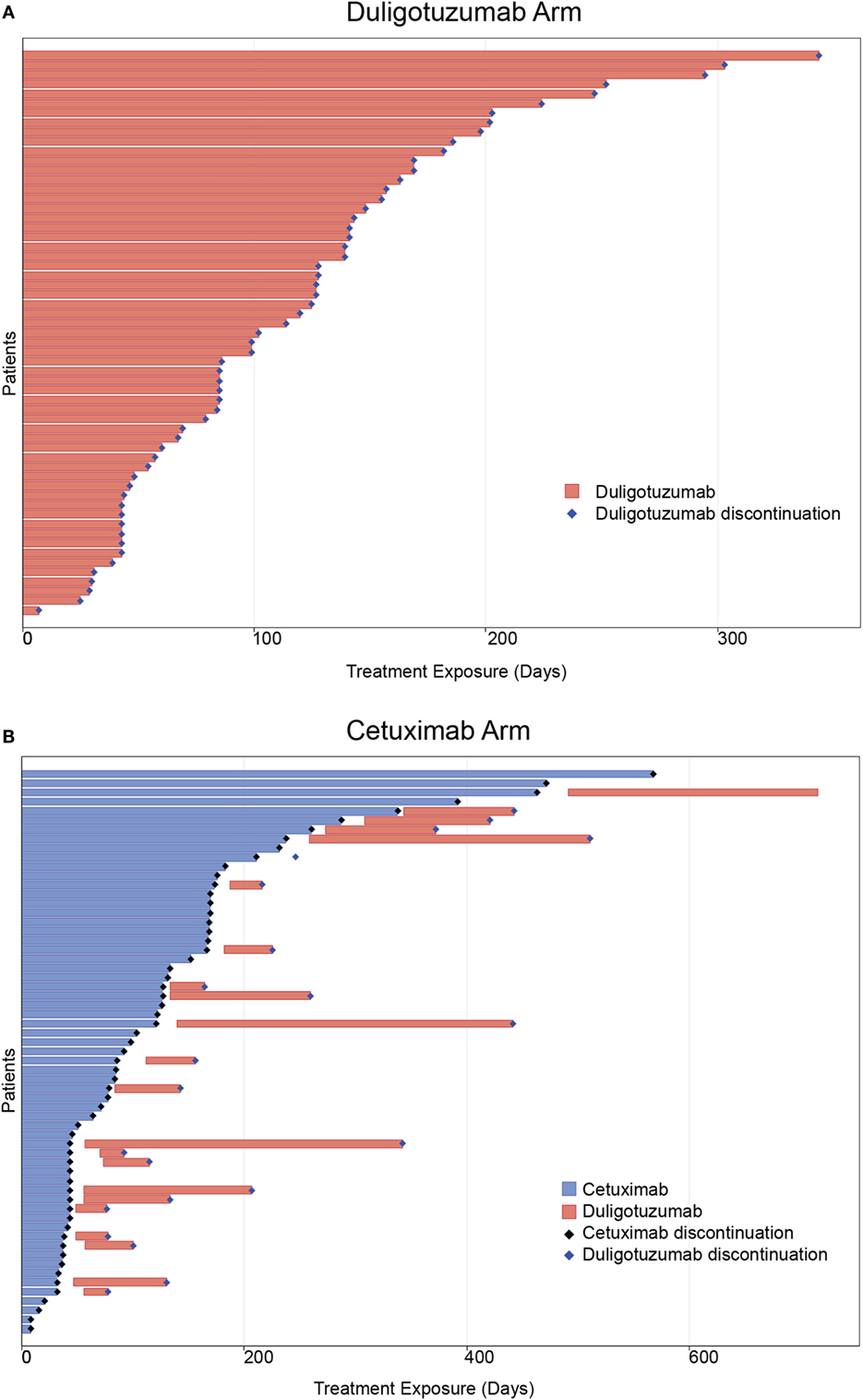
Figure 3. ORR and treatment duration for primary treatment arms and crossover patients. (A) Duligotuzumab arm. (B) Cetuximab arm.
Best responses in the duligotuzumab arm included 1 (2%) CR, 8 (14%) PRs, and 36 (61%) individuals with stable disease. The cetuximab arm included 2 (3%) CRs, 11 (18%) PRs, and 25 (40%) individuals with stable disease. Of 22 patients who crossed over to duligotuzumab after cetuximab failure, 10 showed stable disease (45%), exceeding prior PFS on cetuximab in 5 patients, and with one patient remaining active on study.
Biomarker Subset Analyses
Biomarker subtype analysis was performed for NRG1 and ERBB3 in 108 tumor samples (89%; 51/59 in the duligotuzumab arm and 57/62 in the cetuximab arm), both potential indicators of HER3 activity. Baseline expression using median and quartile cutoffs, respectively, was assessed relative to best change in sum of longest diameters of lesions from baseline and PFS. While there appeared to be a trend toward elevated NRG1 levels and an increase in tumor shrinkage (Figure 4A), neither elevated NRG1 nor reduced ERBB3 expression predicted for response to duligotuzumab or against response to cetuximab (Figure 4B). Moreover, the trend toward elevated NRG1 expression and increased tumor shrinkage was observed in both study arms. Similar observations were made for OS. Of note, NRG1 expression levels were comparable to those in the phase Ia study (including responders) (18). To further address the hypothesized and preclinically supported role for NRG1 autocrine expression in SCCHN, dual-colored ISH (NRG1 and ERBB3) was performed and the biomarker analysis was repeated. Similar to expression analysis, co-localized expression of NRG1 and ERBB3 did not predict for response to duligotuzumab (Figure 4C).
FIGURE 4
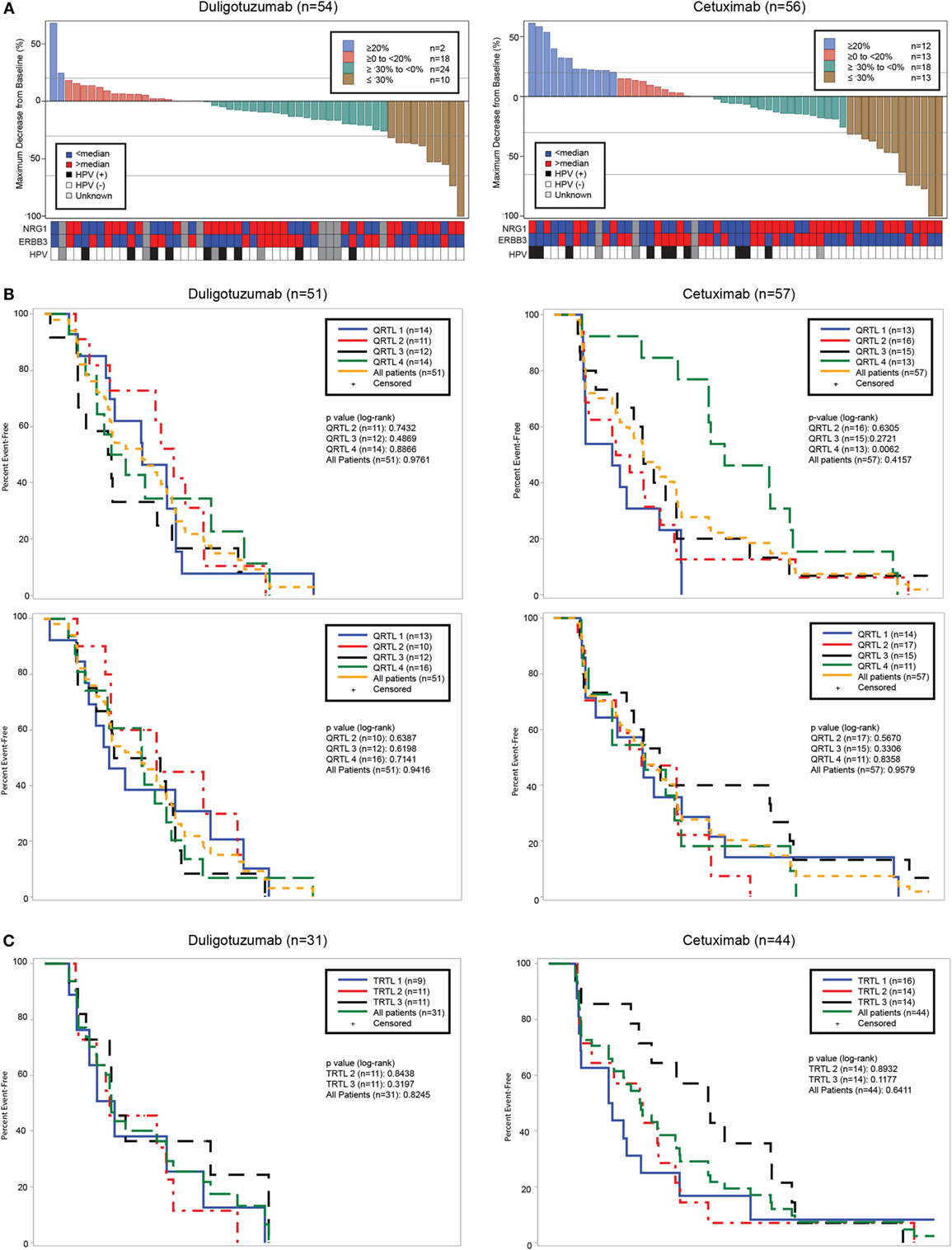
Figure 4. Efficacy relative to key biomarkers: (A) best change in target lesion sum of longest dimension (SLD) and corresponding NRG1, ERBB3, and HPV status; (B) PFS by NRG1 and ERBB3 expression levels by quartiles; and (C) NRG1 measured by qRT-PCR or by ISH does not predict response to duligotuzumab.
In addition to molecular biomarkers, HPV status based on qRT-PCR methodology was performed. Of 110 evaluable tumor samples from both treatment arms, 25 were HPV-positive and 85 HPV-negative. HPV-negative samples tended to have higher NRG1 ligand expression. Of the 25 patients with HPV-positive tumors, the site of primary tumor was oropharynx (14), oral cavity (4), larynx (1), and other or unknown locations (6). Among HPV-positive patients treated with either duligotuzumab or cetuximab, there were no responses (Figure 5).
FIGURE 5
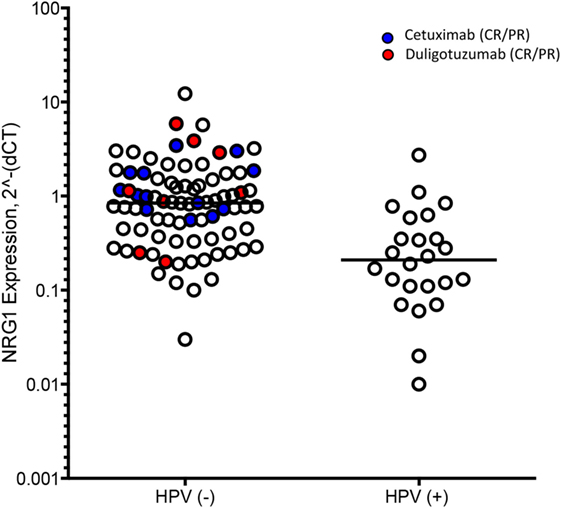
Figure 5. HER family ligand expression by HPV status. Ligand expression was higher in HPV-negative (−) subjects, with no responses in HPV-positive (+).
Discussion
The results of this phase II study show that dual inhibition of HER3 and EGFR by single-agent duligotuzumab demonstrated activity comparable, but not superior, to single-agent cetuximab in second or more line R/M SCCHN. High NRG1 gene expression in tumor (primary biomarker hypothesis) was not associated with duligotuzumab efficacy as response rates, and PFS was similar between groups. Similarly, no association was found with ERBB3 gene expression. Target study drug exposures were achieved for duligotuzumab. The phase II fixed dose of 1100 mg q2w duligotuzumab, which provides equivalent exposure to the phase Ia expansion dose of 14 mg/kg q2w, was selected based on achieving PK targets in >80% of patients. PK targets included an AUC based on xenograft models (equivalent to 300 day × μg/ml) and a C-trough of 5.3 μg/ml, which is predicted to correspond to 90% target saturation and 95% receptor binding. There was no clear relationship between exposure to duligotuzumab and safety or efficacy.
The safety profile of duligotuzumab was largely similar to cetuximab, with few exceptions. While duligotuzumab was associated with fewer rash events (49 vs. 65%) compared to cetuximab, GI disorders were more frequent with duligotuzumab vs. cetuximab (diarrhea 42 vs. 25%; mucosal inflammation 22 vs. 8%). These observations are consistent with other regimens targeting multiple HER receptors, and likely indicative of HER3-mediated toxicity [e.g., pan-HER TKI afatinib vs. cetuximab in R/M SCCHN (20); addition of pertuzumab (inhibitor of the dimerization of HER2/HER3) to trastuzumab and chemotherapy in 1L HER2 + breast cancer (21)]. MedDRA System Order Class “Infections and Infestations” were more frequent in the duligotuzumab arm (all grades: 59 vs. 49%; grades ≥3: 22 vs. 12%) with no particular pattern of infection identified in either treatment arm. The higher frequency in duligotuzumab-treated patients may be related to this groups’ higher rate of mucosal inflammation.
Despite strong preclinical data coupled with activity in phase I suggesting a potential role of HER3 signaling in SCCHN (16, 18), the dual inhibition of EGFR and HER3 was not associated with improved efficacy in this study, neither in all randomized nor biomarker positive patients. The outcome was similar in study of the pan-HER TKI, afatinib vs. cetuximab in all-comer ≥1L SCCHN (20), with median PFS 13.0 vs. 15.0 weeks (HR 0.93, 95% CI 0.62–1.38, p = 0.71). Median PFS for patients who crossed over to afatinib was 9.3 and 5.7 weeks for those crossing to cetuximab (HR 0.64, 95% CI 0.38–1.05, p = 0.08). Taken together, these data suggest that the inhibition of HER3 in addition to EGFR does not significantly improve response in recurrent/metastatic SCCHN. Alternatively, these data may indicate that inhibition of EGFR alone may be sufficient to block EGFR–HER3 signaling, suggesting that HER2 plays a minimal role in this disease. A better understanding of receptor dimerization following exposure to different agents may provide critical insights to this mechanism. It is also possible that HER3 signaling has a moderate role in SCCHN and inhibition of HER3 by duligotuzumab compensated for its slightly lower affinity for EGFR (Kd of 0.4 nM vs. 0.39 nM for cetuximab) (16, 22). Finally, there is no evidence for differential ADCC activity as duligotuzumab demonstrated mediated ADCC activity in cell lines with high EGFR expression that was similar to what has been described with cetuximab (16).
The potential for enhanced chemosensitization and radiosensitization with dual HER3/EGFR inhibition remains an unanswered question. Preclinical studies showed enhanced radiation response with dual HER3/EGFR inhibition in SCCHN and lung cancer model systems (23). Chemotherapy-induced upregulation of NRG1 and activation of HER3 have been reported in vitro (24). A phase Ib study combining duligotuzumab with either cisplatin/5FU or carboplatin/paclitaxel in 1L R/M, SCCHN showed encouraging activity with ORR of 67% though without clear relationship with evaluated biomarkers and hence no means for patient selection (25, 26). While the phase Ib study showed high antitumor efficacy and a higher frequency and severity of select AEs in comparison to historical phase III data on combination of chemotherapy and EGFR inhibitors, it is not clear if such was owed to chemo sensitization or rather was reflective of the small sample size.
The role of EGFR inhibition in HPV-associated oropharyngeal cancer vs. HPV-negative head and neck cancer remains controversial and may differ depending on whether given as monotherapy or combined with chemotherapy or radiotherapy. Our findings of no objective responses in the HPV-positive group with either agent are consistent with those recently reported with afatanib (27), with no objective responses in the p16-positive population and a 13.5% response rate in the p16-negative population, and raise further doubts about the role of anti-EGFR monotherapy for R/M HPV-associated oropharyngeal cancer.
Conclusion
Dual inhibition of EGFR and HER3 by duligotuzumab was not associated with improved efficacy compared to cetuximab, neither in all randomized nor biomarker positive patients. Our data suggest that HPV-negative SCCHN but not HPV-positive SCCHN may respond to cetuximab or duligotuzumab, though the addition of HER3 inhibition does not significantly improve response but may increase the frequency of select lower grade GI toxicities.
Author Contributions
Conception and design: PH, AK, BM, EP, AP, DR, and JV. Collection and assembly of data: MA, DC, JF, AJ, BM, CN, PO, CO, EP, AP, DR, AU, and LW. All authors contributed to data analysis and interpretation. All authors contributed to manuscript writing. All authors provided final approval of manuscript and its content.
Conflict of Interest Statement
JF had leadership at Glycotope GmbH; LW had consultant roles at Ashion, Eisai, and Loxo; CO received research funding from Genentech, Inc., and participated as PI in different clinical studies; AU received honoraria from BMS, Astrazeneca, Amgen, and Teva, had consulting or advisory role at Teva and BMS, and received travel and/or accommodation expenses from Astellas and Teva; AJ has no disclosures; DR received research funding from Genentech, Merck, and Threshold; CN has no disclosures; PH and the University of Wisconsin received laboratory research support from Genentech, Inc.; TC has no disclosures; DC has no disclosures; PO has no disclosures; WH, AK, MA, EP, BM, and AP are employees of Genentech, Inc., South San Francisco, CA, USA and stockholders of Roche; JV participated in Advisory Boards at AstraZeneca, Boehringer-Ingelheim, Debiopharma, Merck-Serono, PCI Biotech, Merck Sharp & Dome Corp., Genentech, Pierre Fabre, Vaccinogen, Innate Pharma, Synthon Biopharmaceuticals, F-Star Biotechnology Ltd., and SMS-Oncology and received lecturer fees from Merck-Serono and Vaccinogen.
Acknowledgments
We acknowledge our appreciation for sites that enrolled patients for this study in Australia (Newcastle Mater Misericordiae Hospital and Wollongong Hospital Cancer Care Center, New South Wales; St. Vincent’s Hospital, Darlinghurst; Royal Brisbane Hospital, Herston; Peter MacCullum Cancer Centre, Melbourne; Ashford Cancer Center Research, Kurralta Park), Belgium (UZ Antwerpen, Edegem), Bulgaria (Complex Oncological Center-Ruse EOOD, Vratsa; Umhat Dr Georgi Stranski, Pleven; MHAT Serdika, Sofia), France (Centre Leon Berard, Lyon; Institut Gustave Roussy, Villejuif), Germany (Uniklinik Essen, Essen), Hungary (Jász-Nagykun-Szolnok Megyei Hetényi Géza Kórház, Szolnok; Debreceni Egyetem Orvos-és Egészségtudományi Centrum, Debrecen), Italy (Ospedale S. Giovanni Battista, Torino), Romania (Sf. Constantin Hospital, Brasov; Institutul Oncologic, Cluj-Napoca; Oncomed SRL, Timisoara; Medisprof SRL, Cluj-Napoca), Spain (Centro Integral Oncologico Clara Campal and Hospital Universitario 12 de Octubre, Madrid), United Kingdom (University Hospital Coventry, Coventry; Beatson West of Scotland Cancer, Glasgow; Royal Marsden NHS Trust, London; The Royal Marsden Hospital, Sutton), United States (Stanford University Medical Center, Stanford; Center for Biomedical Research LLC, Knoxville; University of Wisconsin Hospital and Clinics, Madison; University of Colorado – Anschutz Cancer Pavilion, Aurora; Medical University of South Carolina, Charleston; University of Chicago Department of Medicine, Chicago; West Kentucky Hem/Onc Group, Paducah; Advanced Medical Specialties, Miami; Massachusetts General Hospital and Dana-Faber Cancer Institute, Boston). Editing and writing support was provided by A. Daisy Goodrich (Genentech, Inc., South San Francisco, CA, USA) and was funded by Genentech, Inc.
Funding
This work was supported by Genentech, Inc., South San Francisco, CA, USA. CN was supported by Cancer Research UK Programme Grant A13407 and the RM/ICR NIHR Biomedical Research Centre.
References
1. Brand TM, Iida M, Li C, Wheeler DL. The nuclear epidermal growth factor receptor signaling network and its role in cancer. Discov Med (2011) 12(66):419–32.
2. Kalyankrishna S, Grandis JR. Epidermal growth factor receptor biology in head and neck cancer. J Clin Oncol (2006) 24(17):2666–72. doi: 10.1200/jco.2005.04.8306
3. Normanno N, De Luca A, Bianco C, Strizzi L, Mancino M, Maiello MR, et al. Epidermal growth factor receptor (EGFR) signaling in cancer. Gene (2006) 366(1):2–16. doi:10.1016/j.gene.2005.10.018
4. Vermorken JB, Trigo J, Hitt R, Koralewski P, Diaz-Rubio E, Rolland F, et al. Open-label, uncontrolled, multicenter phase II study to evaluate the efficacy and toxicity of cetuximab as a single agent in patients with recurrent and/or metastatic squamous cell carcinoma of the head and neck who failed to respond to platinum-based therapy. J Clin Oncol (2007) 25(16):2171–7. doi:10.1200/jco.2006.06.7447
5. Vermorken JB, Mesia R, Rivera F, Remenar E, Kawecki A, Rottey S, et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N Engl J Med (2008) 359(11):1116–27. doi:10.1056/NEJMoa0802656
6. Bonner JA, Harari PM, Giralt J, Cohen RB, Jones CU, Sur RK, et al. Radiotherapy plus cetuximab for locoregionally advanced head and neck cancer: 5-year survival data from a phase 3 randomised trial, and relation between cetuximab-induced rash and survival. Lancet Oncol (2010) 11(1):21–8. doi:10.1016/s1470-2045(09)70311-0
7. Tinhofer I, Klinghammer K, Weichert W, Knodler M, Stenzinger A, Gauler T, et al. Expression of amphiregulin and EGFRvIII affect outcome of patients with squamous cell carcinoma of the head and neck receiving cetuximab-docetaxel treatment. Clin Cancer Res (2011) 17(15):5197–204. doi:10.1158/1078-0432.ccr-10-3338
8. Yonesaka K, Zejnullahu K, Okamoto I, Satoh T, Cappuzzo F, Souglakos J, et al. Activation of ERBB2 signaling causes resistance to the EGFR-directed therapeutic antibody cetuximab. Sci Transl Med (2011) 3(99):99ra86. doi:10.1126/scitranslmed.3002442
9. Jain A, Penuel E, Mink S, Schmidt J, Hodge A, Favero K, et al. HER kinase axis receptor dimer partner switching occurs in response to EGFR tyrosine kinase inhibition despite failure to block cellular proliferation. Cancer Res (2010) 70(5):1989–99. doi:10.1158/0008-5472.can-09-3326
10. Wheeler DL, Huang S, Kruser TJ, Nechrebecki MM, Armstrong EA, Benavente S, et al. Mechanisms of acquired resistance to cetuximab: role of HER (ErbB) family members. Oncogene (2008) 27(28):3944–56. doi:10.1038/onc.2008.19
11. Li C, Iida M, Dunn EF, Ghia AJ, Wheeler DL. Nuclear EGFR contributes to acquired resistance to cetuximab. Oncogene (2009) 28(43):3801–13. doi:10.1038/onc.2009.234
12. Wilson TR, Lee DY, Berry L, Shames DS, Settleman J. Neuregulin-1-mediated autocrine signaling underlies sensitivity to HER2 kinase inhibitors in a subset of human cancers. Cancer Cell (2011) 20(2):158–72. doi:10.1016/j.ccr.2011.07.011
13. Shames DS, Carbon J, Walter K, Jubb AM, Kozlowski C, Januario T, et al. High heregulin expression is associated with activated HER3 and may define an actionable biomarker in patients with squamous cell carcinomas of the head and neck. PLoS One (2013) 8(2):e56765. doi:10.1371/journal.pone.0056765
14. Sliwkowski MX, Schaefer G, Akita RW, Lofgren JA, Fitzpatrick VD, Nuijens A, et al. Coexpression of erbB2 and erbB3 proteins reconstitutes a high affinity receptor for heregulin. J Biol Chem (1994) 269(20):14661–5.
15. Bostrom J, Yu SF, Kan D, Appleton BA, Lee CV, Billeci K, et al. Variants of the antibody herceptin that interact with HER2 and VEGF at the antigen binding site. Science (2009) 323(5921):1610–4. doi:10.1126/science.1165480
16. Schaefer G, Haber L, Crocker LM, Shia S, Shao L, Dowbenko D, et al. A two-in-one antibody against HER3 and EGFR has superior inhibitory activity compared with monospecific antibodies. Cancer Cell (2011) 20(4):472–86. doi:10.1016/j.ccr.2011.09.003
17. Huang S, Li C, Sliwkowski MX, Harari PM. MEHD7945A, an EGFR/ErbB3 dual specific antibody, overcomes acquired resistance to EGFR inhibitors in head and neck and lung tumors. Cancer Res (2011) 71(8 Suppl):637–637. doi:10.1158/1538-7445.AM2011-637
18. Juric D, Dienstmann R, Cervantes A, Hidalgo M, Messersmith W, Blumenschein GR Jr, et al. Safety and pharmacokinetics/pharmacodynamics of the first-in-class dual action HER3/EGFR antibody MEHD7945A in locally advanced or metastatic epithelial tumors. Clin Cancer Res (2015) 21(11):2462–70. doi:10.1158/1078-0432.ccr-14-2412
19. ClinicalTrials.gov. A Study of MEHD7945A Versus Cetuximab in Patients with Recurrent/Metastatic Squamous Cell Carcinoma of the Head and Neck. ClinicalTrials.gov (2016). Available from: https://clinicaltrials.gov/ct2/show/NCT01577173
20. Seiwert TY, Fayette J, Cupissol D, Del Campo JM, Clement PM, Hitt R, et al. A randomized, phase II study of afatinib versus cetuximab in metastatic or recurrent squamous cell carcinoma of the head and neck. Ann Oncol (2014) 25(9):1813–20. doi:10.1093/annonc/mdu216
21. Swain SM, Baselga J, Kim SB, Ro J, Semiglazov V, Campone M, et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med (2015) 372(8):724–34. doi:10.1056/NEJMoa1413513
22. Patel D, Lahiji A, Patel S, Franklin M, Jimenez X, Hicklin DJ, et al. Monoclonal antibody cetuximab binds to and down-regulates constitutively activated epidermal growth factor receptor vIII on the cell surface. Anticancer Res (2007) 27(5a):3355–66.
23. Li C, Huang S, Armstrong EA, Francis DM, Werner LR, Sliwkowski MX, et al. Antitumor effects of MEHD7945A, a dual-specific antibody against EGFR and HER3, in combination with radiation in lung and head and neck cancers. Mol Cancer Ther (2015) 14(9):2049–59. doi:10.1158/1535-7163.mct-15-0155
24. Hegde GV, de la Cruz CC, Chiu C, Alag N, Schaefer G, Crocker L, et al. Blocking NRG1 and other ligand-mediated Her4 signaling enhances the magnitude and duration of the chemotherapeutic response of non-small cell lung cancer. Sci Transl Med (2013) 5(171):171ra118. doi:10.1126/scitranslmed.3004438
25. Clement P, Machiels J, Wirth L, Specenier P, Seiwert T, Mardjuadi F, et al. Phase 1b study of MEHD7945A (DULIGOTUZUMAB) plus cisplatin/fluorouracil or carboplatin/paclitaxel for first-line treatment of recurrent/metastatic squamous cell carcinoma of head and neck. Presented at the European Society for Medical Oncology. (2014).
26. Jimeno A, Machiels JP, Wirth L, Specenier P, Seiwert TY, Mardjuadi F, et al. Phase Ib study of duligotuzumab (MEHD7945A) plus cisplatin/5-fluorouracil or carboplatin/paclitaxel for first-line treatment of recurrent/metastatic squamous cell carcinoma of the head and neck. Cancer (2016). doi:10.1002/cncr.30256
27. Machiels JP, Haddad RI, Fayette J, Licitra LF, Tahara M, Vermorken JB, et al. Afatinib versus methotrexate as second-line treatment in patients with recurrent or metastatic squamous-cell carcinoma of the head and neck progressing on or after platinum-based therapy (LUX-Head & Neck 1): an open-label, randomised phase 3 trial. Lancet Oncol (2015) 16(5):583–94. doi:10.1016/s1470-2045(15)70124-5
Keywords: NRG1, HER3, EGFR, SCCHN, HPV, duligotuzumab, MEHD7945A, cetuximab
Citation: Fayette J, Wirth L, Oprean C, Udrea A, Jimeno A, Rischin D, Nutting C, Harari PM, Csoszi T, Cernea D, O’Brien P, Hanley WD, Kapp AV, Anderson M, Penuel E, McCall B, Pirzkall A and Vermorken JB (2016) Randomized Phase II Study of Duligotuzumab (MEHD7945A) vs. Cetuximab in Squamous Cell Carcinoma of the Head and Neck (MEHGAN Study). Front. Oncol. 6:232. doi: 10.3389/fonc.2016.00232
Received: 29 August 2016; Accepted: 14 October 2016;
Published: 31 October 2016
Edited by:
Elise Kohn, National Cancer Institute, USAReviewed by:
Susumu Okano, National Cancer Centre Hospital East, JapanKenji Okami, Tokai University, Japan
Copyright: © 2016 Fayette, Wirth, Oprean, Udrea, Jimeno, Rischin, Nutting, Harari, Csoszi, Cernea, O’Brien, Hanley, Kapp, Anderson, Penuel, McCall, Pirzkall and Vermorken. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jérôme Fayette, jerome.fayette@lyon.unicancer.fr