 James C. Moon1
James C. Moon1 Brian Godman2,3,4*Max Petzold5
Brian Godman2,3,4*Max Petzold5 Samantha Alvarez-Madrazo3Kathleen Bennett6Iain Bishop7
Samantha Alvarez-Madrazo3Kathleen Bennett6Iain Bishop7 Anna Bucsics8,9
Anna Bucsics8,9 Ulrik Hesse10Andrew Martin11
Ulrik Hesse10Andrew Martin11 Steven Simoens12
Steven Simoens12 Corinne Zara13Rickard E. Malmström14
Corinne Zara13Rickard E. Malmström14- 1Heart Hospital Imaging Centre, The Heart Hospital, University College Hospital, London, UK
- 2Division of Clinical Pharmacology, Department of Laboratory Medicine, Karolinska Institutet, Karolinska University Hospital Huddinge, Stockholm, Sweden
- 3Medicine Use and Health, Strathclyde Institute of Pharmacy and Biomedical Sciences, University of Strathclyde, Glasgow, UK
- 4National Institute for Science and Technology on Innovation on Neglected Diseases, Centre for Technological Development in Health, Oswaldo Cruz Foundation (Fiocruz), Rio de Janeiro, Brazil
- 5Occupational and Environmental Medicine, Centre for Applied Biostatistics, University of Gothenburg, Gothenburg, Sweden
- 6Department of Pharmacology and Therapeutics, Trinity Centre for Health Sciences, St. James Hospital, Dublin, Ireland
- 7Public Health and Intelligence Business Unit, NHS National Services Scotland, Edinburgh, UK
- 8Department of Finance, Faculty of Business, Economics and Statistics, University of Vienna, Vienna, Austria
- 9Hauptverband der Österreichischen Sozialversicherungsträger, Vienna, Austria
- 10National Institute for Health Data and Disease Control, Copenhagen, Denmark
- 11NHS Greater Manchester Commissioning Support Unit, Salford, Manchester, UK
- 12KU Leuven Department of Pharmaceutical and Pharmacological Sciences, Leuven, Belgium
- 13Barcelona Health Region, Catalan Health Service, Barcelona, Spain
- 14Clinical Pharmacology Unit, Department of Medicine, Karolinska Institutet, Karolinska University Hospital Solna, Stockholm, Sweden
Introduction: There is an urgent need for health authorities across Europe to fully realize potential savings from increased use of generics to sustain their healthcare systems. A variety of strategies were used across Europe following the availability of generic losartan, the first angiotensin receptor blocker (ARB) to be approved and marketed, to enhance its prescribing vs. single-sourced drugs in the class. Demand-side strategies ranged from 100% co-payment for single-sourced ARBs in Denmark to no specific measures. We hypothesized this heterogeneity of approaches would provide opportunities to explore prescribing in a class following patent expiry.
Objective: Contrast the impact of the different approaches among European countries and regions to the availability of generic losartan to provide future guidance.
Methodology: Retrospective segmented regression analyses applying linear random coefficient models with country specific intercepts and slopes were used to assess the impact of the various initiatives across Europe following the availability of generic losartan. Utilization measured in defined daily doses (DDDs). Price reductions for generic losartan were also measured.
Results: Utilization of losartan was over 90% of all ARBs in Denmark by the study end. Multiple measures in Sweden and one English primary care group also appreciably enhanced losartan utilization. Losartan utilization actually fell in some countries with no specific demand-side measures. Considerable differences were seen in the prices of generic losartan.
Conclusion: Delisting single-sourced ARBs produced the greatest increase in losartan utilization. Overall, multiple demand-side measures are needed to change physician prescribing habits to fully realize savings from generics. There is no apparent “spill over” effect from one class to another to influence future prescribing patterns even if these are closely related.
Introduction
Health authorities across Europe could realize considerable savings through greater use of generic medicines. Between 2008 and 2013, the global annual sales of medicines losing their exclusivity was US$50 to 100 billion (€35–70 billion), reaching US$255 billion by 2016 (Frank, 2007; Jack, 2008; Godman et al., 2014). Once one or more drugs in a class lose their patent, and all drugs in the class are seen as essentially therapeutically similar at appropriate doses, it is legitimate for health authorities to encourage physicians to preferentially prescribe low cost generics to realize considerable savings without compromising care (Voncina et al., 2011; Godman et al., 2014). However, physicians and authorities do not always take full advantage of the availability of generics (Godman et al., 2010a, 2014). The availability of generic losartan provides an exemplar case to review health authority activities across Europe and the subsequent implications.
Renin-angiotensin inhibitor drugs had global sales of US$27.3 billion in 2010, 24% in Europe, much of this for single-sourced angiotensin receptor blockers (ARBs) (IMS Institute for Health Informatics, 2011). Broadly speaking, all angiotensin converting enzyme inhibitors (ACEIs) and ARBs are seen as having similar effectiveness for the management of hypertension and heart failure at appropriate dose titration (Heran et al., 2008; Moon et al., 2010; Voncina et al., 2011; Bucsics et al., 2012; Svanstrom et al., 2012; Godman et al., 2013a; Simoens et al., 2013). Patients in the UK have also been successfully switched between different ARBs without compromising care (Usher-Smith et al., 2008; Moon et al., 2010). However, other authors disagree believing losartan is inferior to other ARBs (Makani et al., 2014).
A variety of strategies were instigated by national and regional health authorities across Europe to preferentially encourage the prescribing of losartan once generic losartan became available. These included 100% co-payment for single-sourced ARBs in Denmark unless there was a good medical rationale, which effectively de-listed single-sourced ARBs (Hesse et al., 2013). Other strategies including removing prescribing restrictions for losartan but not for single-sourced ARBs, instigating prescribing targets for losartan vs. single-sourced ARBs, physician financial incentive schemes and therapeutic switching programmes (Bucsics et al., 2012; Godman et al., 2013a; Simoens et al., 2013; Martin et al., 2014). However, some authorities did nothing (Bennie et al., 2013; Godman et al., 2013b). We hypothesized this heterogeneity of approaches offers the opportunity for a “natural experiment” of prescribing in a class following patent expiry, and to benchmark the effectiveness and financial utility of different interventions to provide insight for future opportunities.
Consequently, the aim of the study is to compare and contrast the impact of the many different demand-side approaches among European countries following the availability of generic losartan. Only Western European countries and regions were chosen as typically losartan was available as a generic much earlier among Central and Eastern European countries; alternatively only generic losartan was reimbursed and not single-sourced ARBs (Voncina et al., 2011; Kalaba et al., 2012; Markovic-Pekovic et al., 2012). The objective being to provide guidance on potential future approaches that the authorities could consider as they seek to introduce additional measures to further enhance their prescribing efficiency.
Methodology
The utilization of the different ARBs was calculated in terms of defined daily doses (DDDs), with 2011 DDDs used in line with International guidance (Ronning et al., 2000; Vlahovic-Palcevski et al., 2010). DDDs are recognized as the international standard to assess utilization patterns within and between countries (WHO, 2003; Bennie et al., 2013). Only administrative databases were used to assess utilization patterns. Details of these are included in Box 1.
Box 1. Details of administrative databases use in the study and the date when generic losartan first reimbursed/included in the drug tariff (Coma et al., 2009; Bucsics et al., 2012; Cahir et al., 2012; Bennie et al., 2013; Godman et al., 2013a; Hesse et al., 2013; Simoens et al., 2013).
• Austria: Internal data warehouse of the HVB (Hauptverband der Österreichischen Sozialversicherungsträger)—BIG—coupled with Cube HMSTAT, based on the “maschinelle Heilmittelabrechnung,” which covers approximately 98% of the Austrian population. Generic losartan was reimbursed from October 2008.
• Belgium: Pharmanet—a database of reimbursed medicines dispensed in ambulatory care in Belgium. This database is maintained by the National Institute for Health and Disability Insurance and covers the whole Belgian population. Generic losartan was reimbursed from July 2010.
• Denmark: Danish Prescription Registry covering the entire Danish population. Generic losartan was reimbursed from April 2010.
• Ireland: The National Shared Services Primary Care Reimbursement Service of the Health Service Executive in Ireland (HSE-PCRS) pharmacy claims database. This database provides details on monthly dispensed medications for each individual within the General Medical Services (GMS) population. The GMS population covers approximately 30% of the population of Ireland with higher morbidity than the general population—reflected in consuming approximately 65% of total pharmaceutical expenditure in Ireland. Generic losartan was reimbursed in Ireland from March 2010.
• Scotland: NHS National Services Scotland Corporate Warehouse covering the entire population in Scotland. Generic losartan was reimbursed (in the Drug Tariff) from July 2010.
• Spain (Catalonia): DMART (Catalan Health Service) database covering all patients in the public system in Catalonia. Generic losartan was reimbursed from July 2006.
• Sweden: National Swedish Pharmacy Register covering the entire Swedish population. Generic losartan was reimbursed from March 2010.
Losartan utilization was subsequently converted into a percentage of total ARB utilization (DDD basis) before and after the availability of generic losartan (time zero) to enable meaningful comparisons between the various European countries factoring in differences in population sizes, time when generic losartan became available (Table 1) and the database characteristics between the countries (Box 1). The xtmixed command in Stata versions 12/13 (StataCorp, College Station, Texas, USA) was used to fit a linear random coefficient model with country specific intercepts and slopes. The model included a change in the slope at the time of introducing generic losartan in each country. Data on the number of monthly reimbursed prescriptions for all patients within each country's health service prescribed a minimum of one ARB (C09CA01 to 09) (Bucsics et al., 2012; Godman et al., 2013a; Simoens et al., 2013; WHO Collaborating Centre for Drug Statistics Methodology, 2013) at least 7 months before the availability of generic losartan in each country until at least 13 months after was used in the analysis.
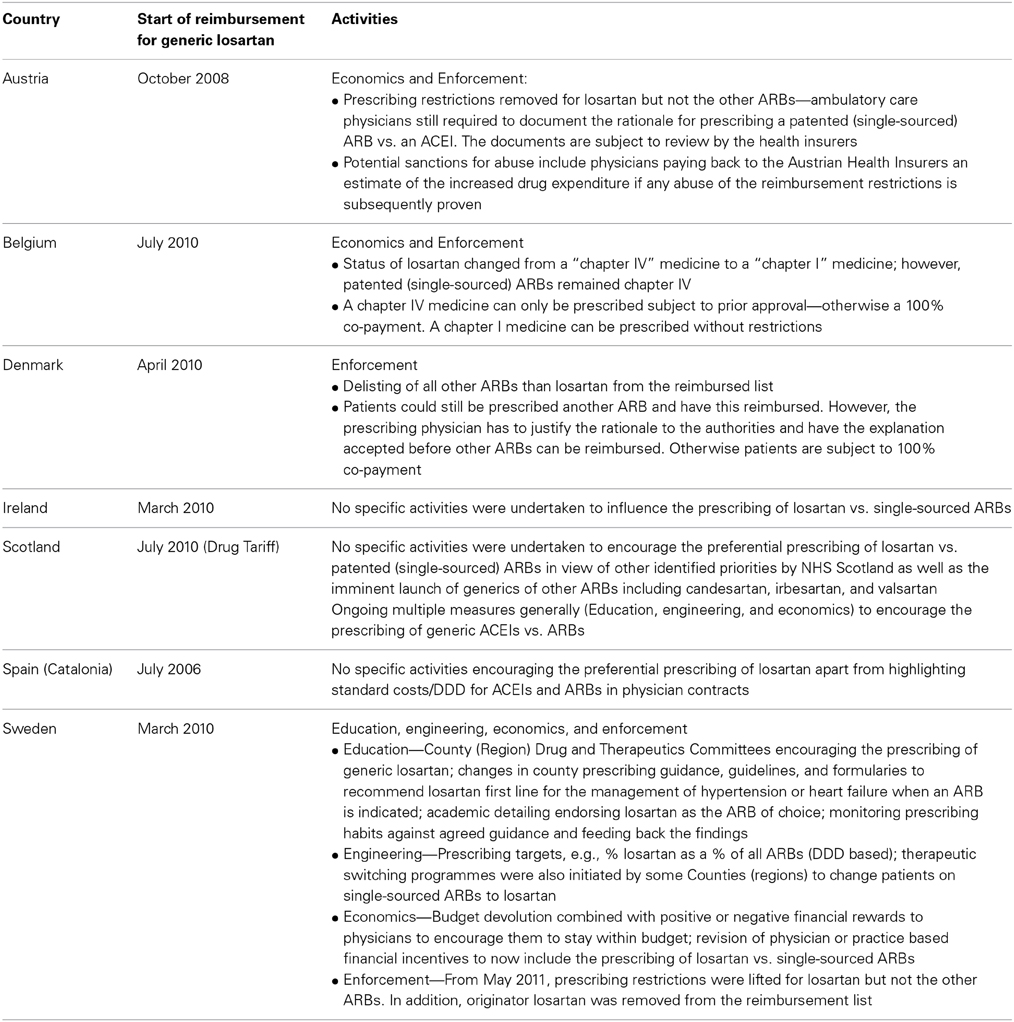
Table 1. Details of specific policies initiated among European countries following the availability of generic losartan.
Separate analyses were undertaken in Austria, Belgium, Denmark, Scotland and Sweden to assess whether the changes in losartan utilization patterns post generics were significant or not (Bucsics et al., 2012; Bennie et al., 2013; Godman et al., 2013a; Hesse et al., 2013; Simoens et al., 2013). These were retrospective segmented regression analyses of an interrupted time series design following the availability of generic losartan (Wagner et al., 2002). In three of the countries, serial autocorrelations of losartan prescription items dispensed were assessed with an ARIMA model using a Box-Jenkins-Tiao strategy (McDowall et al., 1980; Bennie et al., 2013; Godman et al., 2013a; Simoens et al., 2013), with common segmented regression models used to fit a least-squares regression line to each segment (Ross-Degnan et al., 1993). The Durbin-Watson statistic was calculated in each country to test for a serial autocorrelation of the error terms in the regression models to see whether significance was reached (P < 0.05) (Durbin and Watson, 1951; Brennan and Croft, 1994). In Austria, regression analyses were undertaken using the “R Development Core Team” methodology to ascertain whether the change in losartan utilization post generics was significant (Bucsics et al., 2012; R Development Core Team, 2012). In the linear regression analysis in Denmark, dummy variables were added to allow a change in intercept and in slope in April 2010, when generic losartan was reimbursed, to test for significance (Wagner et al., 2002; Hesse et al., 2013). Further details can be found in the country specific publications.
A separate analysis was also undertaken in one English primary care organization, NHS Bury, using a similar methodology to Belgium, Scotland and Sweden (Martin et al., 2014). However in this case, the unit of measurement was prescription items dispensed rather than DDDs as this is the typical metric used to assess and compare utilization patterns in England between different primary care groups (Martin et al., 2014). The rationale for including this regional primary care organization was that initially there were no specific demand-side measures introduced following the availability of generic losartan; however, multifaceted measures were introduced 7 months later including therapeutic switching to help realize considerable savings (Martin et al., 2014). Consequently this provides an additional exemplar case history of a regional health authority changing its policies over time.
The percentage of losartan dispensed as generics vs. the originator was also calculated in all the European countries and regions studied apart from Belgium to ascertain whether there were any problems with generic losartan in clinical practice. Fixed dose ARB combinations (FDCs) were not included in this research as FDC utilization can be as low as 2% of total renin-angiotensin inhibitor drug utilization in some countries (Voncina et al., 2011; Bennie et al., 2013). There is also continuing controversy surrounding the patient benefits of FDCs vs. titrating single agents separately, especially if FDCs have higher drug acquisition costs than the combination of each agent separately (Regional Drugs and Therapeutics Centre (NHS), 2008; Voncina et al., 2011; Kalaba et al., 2012).
We also calculated the percentage reduction in reimbursed expenditure/ DDD for generic losartan vs. pre-patent loss originator prices over time as well as the influence of generic losartan on subsequent ARB expenditure in separate analyses in a number of countries. As a result, compare the influence of the different policies on overall ARB prescribing efficiency with all ARBs seen as essentially similar at appropriate dose titration (Heran et al., 2008; Moon et al., 2010; Svanstrom et al., 2012).
The European countries and regions chosen for the study provided a range of geographical locations, different population sizes, different approaches to the financing of health care, i.e., taxation or health insurance based, as well as different approaches to enhancing the utilization of generics vs. originators and their pricing (Godman et al., 2009, 2014; Abuelkhair et al., 2012; Simoens, 2012; Vogler, 2012). Policies to encourage the prescribing of generics vs. originators included prescribing targets, e.g., Belgium, financial incentives either for physicians, patients, or both, e.g., Austria, Belgium and Spain, encouraging voluntary International non-proprietary name (INN) prescribing, e.g., UK, and compulsory generic substitution, e.g., Sweden (Godman et al., 2009, 2013c; Simoens, 2012; Simoens et al., 2013). Pricing policies for generics included prescriptive pricing policies as well as market forces encouraging their prescribing and dispensing (Godman et al., 2012a, 2013c; Vogler, 2012). This methodology is in line with recommended guidance for undertaking cross national comparisons (Cacace et al., 2013).
The demand-side measures were collated under the 4Es—Education, engineering, economics, and enforcement (Wettermark et al., 2009). These include (Godman et al., 2009, 2014; Wettermark et al., 2009, 2010; Garuoliene et al., 2011; Gustafsson et al., 2011; Voncina et al., 2011; Markovic-Pekovic et al., 2012):
• Education: Activities range from printed guidelines to more intensive strategies including academic detailing and benchmarking physician prescribing habits.
• Engineering: Refers to organizational or managerial interventions, e.g., prescribing targets and therapeutic switching initiatives.
• Economics: includes financial incentives for physicians, patients or pharmacists.
• Enforcement: includes regulations by law such as prescribing restrictions for ARBs in Austria, the Republic of Srpska and Sweden as well as compulsory generic substitution or compulsory INN prescribing.
A narrative review of health policies was undertaken in each country and region following the availability of generic losartan by one of the co-authors (Brian Godman). This was subsequently checked with each co-author, in line with previous cross-national studies (Godman et al., 2010a; Voncina et al., 2011).
Results
The various European countries and regions approached the opportunity of generic losartan differently (Table 1). These policies were in addition to general policies to enhance the prescribing of generics which, as mentioned, included financial incentives for physicians and patients, prescribing targets, compulsory generic substitution and high voluntary INN prescribing (Godman et al., 2008, 2009; Coma et al., 2009; Bennie et al., 2013; Simoens et al., 2013).
This resulted in substantial differences in the subsequent utilization of losartan vs. other ARBs (Figure 1). By changing the reimbursement status of patented (single-sourced) ARBs, e.g., Denmark, the utilization of losartan rose to over 90% of all ARBs (DDD basis) by the end of the study period.
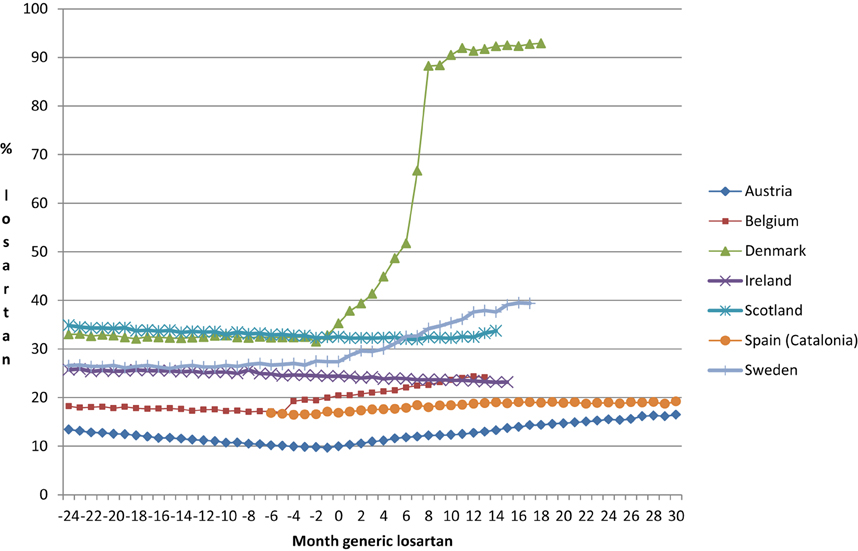
Figure 1. Percentage utilization of losartan vs. all single ARBs (DDD basis) before and after the availability of generic losartan (Time 0) on a monthly basis.
There was an average increase in the utilization of losartan of 0.82% units per month among the various European countries and regions after the introduction of generic losartan (month 0), with a large variability among them (Figure 1). The standard deviation (SD) was 1.33% per month (Table 2).
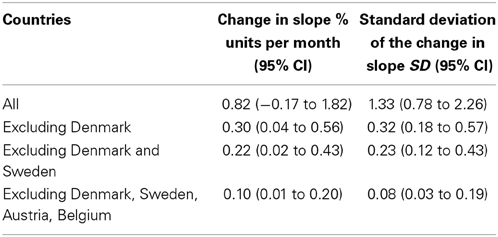
Table 2. Average change in regression slopes after the introduction of generic losartan and corresponding standard deviations over different groupings of the included countries.
Separate country analyses showed a significant difference in the utilization of losartan post generics in Austria, Belgium, Denmark, and Sweden but not Scotland (further details can be found in the country specific publications: Bucsics et al., 2012; Bennie et al., 2013; Godman et al., 2013a; Hesse et al., 2013; Simoens et al., 2013).
Some countries instigated few or no specific demand-side measures to stimulate the preferential prescribing of losartan following generic availability. These were Ireland, Scotland, and Spain (Catalonia) (Table 1). This resulted in no change or even a fall in losartan use in Ireland as well as initially in Scotland (Figure 2). There was appreciable consistency between these three countries (Table 2), i.e., excluding the European countries that had instigated multiple demand-side measures from the analysis (Denmark, Sweden, Belgium, and Austria) resulted in very limited change in the post-generic utilization slopes with an average of 0.10% and an SD of 0.08% (Table 2).
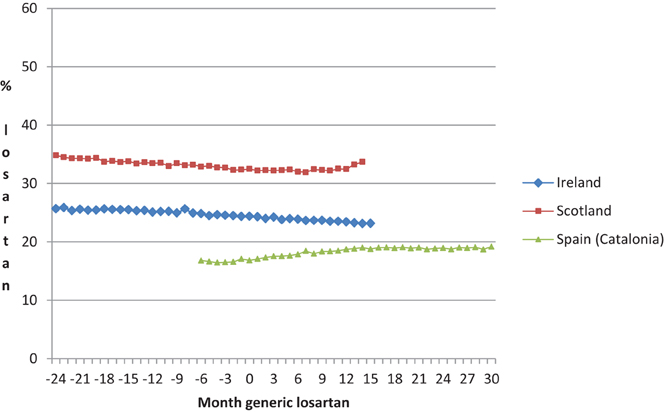
Figure 2. Percentage utilization losartan vs. all single ARBs (DDD based) among the European countries with no multiple demand-side measures to preferentially enhance the prescribing of losartan (Table 1) before and after the availability of generic losartan (Time 0) on a monthly basis.
Losartan utilization increased significantly in NHS Bury following the instigation of multiple demand-side measures, which were similar to Sweden (Table 1). These principally centered on the therapeutic switching of patients with hypertension from single-sourced ARBs to losartan (Martin et al., 2014). These multiple demand-side measures were introduced seven months after the availability of generic losartan. Prior to that, there was no change in the utilization of losartan post generic availability (Time Zero—Table 3) with no specific demand-side measures encouraging the preferential prescribing of losartan vs. single-sourced ARBs. Following the multiple demand-side measures (DM0) introduced in month eight after generic losartan, the utilization of losartan significantly increased from 26% of all single ARB items dispensed to 65% by the end of the study period (Table 3).

Table 3. Utilization of losartan and other ARBs in NHS Bury (items dispensed) before and after generic losartan (month 0) and before and after multiple demand-side measures (MDM).
Generic losartan accounted for up to 97–99% of total losartan (DDD basis) by the end of the study in Sweden and Scotland respectively. This was due to compulsory generic substitution in Sweden (Godman et al., 2009, 2013a) and high voluntary INN prescribing in Scotland (Bennie et al., 2013; Godman et al., 2013c). High INN prescribing rates were already seen in Scotland before generic losartan became available. There was lower utilization of generic losartan as a percentage of total losartan utilization (DDD basis) in Spain, Austria and Ireland. This was 80% in Spain (26% after 1 year), 46% in Austria and 24% in Ireland by the end of the study in each country.
The price of generic losartan (expenditure/ DDD) also varied considerably among the different European countries and regions. In Sweden, Denmark (total losartan), Scotland, and Austria, the price of generic losartan was 10, 12, 12, and 17% respectively of pre-patent loss prices by the end of the study. Prices for generic losartan were higher in Spain (Catalonia), Belgium (total losartan including both generic and originator losartan) and Ireland at 32, 54, and 56% respectively of pre-patent loss prices by the end of the study.
The combination of supply- and demand-side measures in Denmark resulted in a 77% reduction in overall ARB expenditure by the end of the study despite a 16% increase in utilization. Drug acquisition cost savings were estimated at over 290 million Danish Kroner (€40 million) per annum. In Sweden, total expenditure on single ARBs fell by 26% by the end of the study despite a 16% increase in utilization and in Belgium ARB expenditure fell by 15% by the end of the study despite a 1% increase in utilization. NHS Bury realized annual net savings of GB£290,000 (€348,000) for a population of 186,000 following the instigation of its multiple demand-side measures. This was eight times the cost of implementing their multifaceted approach. In Scotland, drug acquisition cost savings from low cost generics were estimated at GB£8 million (€9.6 million) per annum from the prescribing of generic vs. single-sourced losartan. These savings are growing in Scotland as more ARBs lose their patents.
Discussion
Generic losartan created an opportunity for health authorities across Europe to realize considerable savings without compromising care. This is because separate studies, including therapeutic switching programmes, have shown that patient outcomes should not be compromised with such measures (Usher-Smith et al., 2008; Moon et al., 2010; Martin et al., 2014). A number of similar opportunities are pending with other patent expiries to provide future opportunities to health authorities (Jack, 2008; Godman et al., 2013d). The approach of some countries, e.g., Denmark, shows that these savings can be fully realized for pertinent classes. Aggressive changes in the reimbursement status of the single-sourced ARBs resulted in the prescribing of generic ARBs, i.e., losartan, in over 90% of cases. Without specific demand-side measures preferentially encouraging the prescribing of losartan, its prescribing remained stable or actually fell following generics (Figures 1, 2, Table 2).
Replicating the activities in Denmark throughout Europe would result in considerable savings with generic losartan priced at one 10th of the price of single-sourced products as seen in Scotland (Bennie et al., 2013). In other circumstances, such differences in the use of taxpayers' monies would result in serious public debate. Here, it is more likely that the influence of pharmaceutical companies promoting their single-sourced ARBs, the potential dissociation of the prescriber from the budget holder, other health authority priorities or a combination of these, resulted in the appreciable differences in physician prescribing behavior post generic losartan (Figure 1). It is perhaps sufficient to say that if all European countries mirrored the activities in Denmark (Table 1), billions of euros could have been redirected without compromising care with all ARBs seen as therapeutically similar at appropriate doses. Multiple demand-side measures in NHS Bury and Sweden, including therapeutic switching, also produced considerable savings even when factoring in the cost of implementation including physician time from switching patients from single-sourced ARBs to losartan (Godman et al., 2013a; Martin et al., 2014). These two countries and regions provide examples where it is difficult for health authorities to delist single-sourced products in a class from the reimbursement list.
Some interventions were less effective than others. Lifting prescribing restrictions for losartan but not the other ARBs in Austria and Belgium (Table 1) significantly enhanced its use (Figure 1) (Bucsics et al., 2012; Simoens et al., 2013). However, the resultant change in its utilization was lower than the changes seen in either Denmark, Sweden, or NHS Bury post generic losartan (Figure 1, Table 3). Having said this, Figures 1, 2 and Tables 1, 2 demonstrate again that multiple demand-side measures are needed to change physician prescribing habits (Austria, Belgium, Denmark and Sweden vs. Ireland, Scotland, and Spain [Catalonia]). This has previously been seen with the proton pump inhibitors and statins following the availability of generic omeprazole and simvastatin respectively (Godman et al., 2010a,b), as well as with demand-side measures to enhance the prescribing of generic ACEIs vs. single-sourced ARBs (Voncina et al., 2011; Godman et al., 2013c). This has also been seen in other situations (Bero et al., 1998; Barton, 2001).
The findings in Scotland and initially NHS Bury also suggest there is no “spill over” learning from one class to another to effect changes in physician prescribing habits even if the classes are closely related. Multiple demand-side measures (education, engineering', and economics) had appreciably limited the utilization of single-sourced ARBs vs. generic ACEIs in Scotland compared with countries with few demand-side measures (Voncina et al., 2011; Godman et al., 2013c). However, these learnings were not carried through into the preferential prescribing of losartan vs. single-sourced ARBs once it became available (Bennie et al., 2013; Martin et al., 2014). This changed in NHS Bury once multiple demand-side measures were introduced to significantly enhance the prescribing of losartan vs. single-sourced ARBs (Martin et al., 2014). One mitigating reason for the lack of a “spill over” effect in Scotland, and initially in NHS Bury, could be that the complexity of the message is enhanced, i.e., health authorities going from advocating ACEIs first line vs. ARBs to advocating ACEIs and low cost ARB first line vs. single-sourced ARBs (Bennie et al., 2013).
There appeared to be no problems with generic losartan in clinical practice as it accounted for up to 97–99% of total losartan (DDD basis) by the end of the study period in Sweden and Scotland respectively (Bennie et al., 2013; Godman et al., 2013a). However, we cannot say this with certainty as we did not have access to patient data. The high voluntary INN prescribing rates with losartan in Scotland mirror those seen with other products and classes (Godman et al., 2013c). This starts with educating students in medical school (Voncina et al., 2011; Godman et al., 2013c), and provides guidance to countries where the dispensing of different branded generics without adequate explanations can cause confusion if patients do not receive adequate information about their medicines (Godman et al., 2009; Olsson and Kalvemark Sporrong, 2012). This can lead to either duplication of medicines; alternatively, patients not taking their prescribed treatments as directed. Consequently, not gaining the most benefit from the medicines prescribed (Olsson et al., 2014). These scenarios are exacerbated if pharmacists lack training on how to handle concerns with substitution and/ or do not receive adequate payment for providing relevant information to patients potentially limiting their time with them (Olsson and Kalvemark Sporrong, 2012; Martin et al., 2014). INN prescribing, apart from a limited number of well-known situations, is one way to address this, which has worked well in the UK (McGinn et al., 2010; Godman et al., 2013c).
There were also considerable differences in prices of generic losartan among the different countries and regions. This reflects differences in their policies to enhance the utilization of generics as well as the different pricing policies for generics. The low prices for generic losartan in Scotland, which is similar to those for other generics, follows reforms in the UK to enhance transparency in the cost of producing generics as well as the discounts offered by manufacturers to wholesalers and pharmacists to preferentially dispense their generic (Voncina et al., 2011; Bennie et al., 2012, 2013; Godman et al., 2013c). The price reduction in Sweden, which is also similar to other generics, is a result of introducing compulsory generic substitution with the lowest priced molecule (Andersson et al., 2005; Godman et al., 2009, 2013a). Generic prices are falling further in Sweden with the recent introduction of monthly auctions, with the manufacturer winning the auction guaranteed a considerable proportion of dispensed generics the following month (Godman et al., 2012a,b). The modest price reduction for generic losartan in Belgium reflects the current situation where generic companies only have to lower their prices to the reference price level to be reimbursed. This was only 16% vs. pre-patent loss prices until 2002, 20% until 2003, 26% until 2005, and currently 31% (Godman et al., 2013e; Simoens et al., 2013). The relatively high price for generic losartan in Ireland reflects limited measures to date to reduce generic prices, although this is now changing (Godman et al., 2010a; Cahir et al., 2012). Consequently, measures to increase the attractiveness of the generic market, as well as enhance the transparency in their pricing as seen in Sweden and the UK, provide guidance to countries seeking ways to achieve further savings from the availability of generics.
We appreciate that we have not measured patient outcomes in any of the European countries and regions following the various initiatives apart from NHS Bury. However as stated, surveillance and other studies have shown no compromise on patient outcomes following measures to increase the prescribing of low cost ARBs (Usher-Smith et al., 2008; Moon et al., 2010; Svanstrom et al., 2012; Martin et al., 2014).
Conclusion
The loss of market exclusivity for medicines can create considerable opportunities for European health authorities to save resources to help fund increased drug volumes and new premium priced drugs (Godman et al., 2014). This losartan case study shows that multiple demand-side measures can be extremely effective with influencing subsequent physician prescribing. Without these, prescribing rates for multiple sourced products in a class can actually fall. However, some interventions are less effective than others. If all European countries followed the example of Denmark, NHS Bury in later years, or Sweden, considerable resources could have been saved. Having said this, there does appear at times to be a disconnect between the physician prescriber and the payer of medicines, creating a dissociation of responsibility which is reducing cost-effective prescribing. If we are to maintain the European ideals of comprehensive and equitable healthcare, we must urgently address this.
Funding
The analysis and report writing was in part funded by a grant from the Karolinska Institutet.
Author Contributions
Details of the contributions are as follows: James C. Moon, Brian Godman, and Rickard E. Malmström devised the concept for the paper and produced the first and subsequent drafts. Max Petzold performed the statistical analyses and critiqued successive drafts. Samantha Alvarez-Madrazo, Kathleen Bennett, Iain Bishop, Anna Bucsics, Ulrik Hesse, Andrew Martin, Steven Simoens, Corinne Zara, and Rickard E. Malmström provided the utilization and expenditure data for their respective countries as well as details on the demand-side measures. They also critiqued successive drafts.
Conflict of Interest Statement
Some co-authors are employed by health authorities or health insurance companies. These include: Iain Bishop (Scotland), Anna Bucsics (Austria), Ulrik Hesse (Denmark), Corinne Zara (Barcelona, Spain), and Rickard E. Malmström (Stockholm, Sweden). Steven Simoens holds the European Generic Medicines Association (EGA) Chair “European policy toward generic medicines.” Otherwise the authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Abuelkhair, M., Abdu, S., Godman, B., Fahmy, S., Malmstrom, R. E., and Gustafsson, L. L. (2012). Imperative to consider multiple initiatives to maximize prescribing efficiency from generic availability: case history from Abu Dhabi. Expert Rev. Pharmacoecon. Outcomes Res. 12, 115–124. doi: 10.1586/14737167.9.1.65
Andersson, K., Sonesson, C., Petzold, M., Carlsten, A., and Lonnroth, K. (2005). What are the obstacles to generic substitution? An assessment of the behaviour of prescribers, patients and pharmacies during the first year of generic substitution in Sweden. Pharmacoepidemiol. Drug Saf. 14, 341–348. doi: 10.1002/pds.1055
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Barton, S. (2001). Using clinical evidence. BMJ 322, 503–504. doi: 10.1136/bmj.322.7285.503
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Bennie, M., Bishop, I., Godman, B. Campbell, S., Miranda, J., Finlayson, A. E., et al. (2013). Are prescribing initiatives readily transferable across classes: the case of generic losartan in Scotland? Qual. Prim. Care 21, 7–15.
Bennie, M., Godman, B., Bishop, I., and Campbell, S. (2012). Multiple initiatives continue to enhance the prescribing efficiency for the proton pump inhibitors and statins in Scotland. Expert Rev. Pharmacoecon. Outcomes Res. 12, 125–130. doi: 10.1586/erp.11.98
Bero, L. A., Grilli, R., Grimshaw, J. M., Harvey, E., Oxman, A. D., and Thomson, M. A. (1998). Closing the gap between research and practice: an overview of systematic reviews of interventions to promote the implementation of research findings. The cochrane effective practice and organization of care review group. BMJ 317, 465–468.
Brennan, P., and Croft, P. (1994). Interpreting the results of observational research: chance is not such a fine thing. BMJ 309, 727–730. doi: 10.1136/bmj.309.6956.727
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Bucsics, A., Godman, B., Burkhardt, T., Schmitzer, M., and Malmstrom, R. E. (2012). Influence of lifting prescribing restrictions for losartan on subsequent sartan utilization patterns in Austria: implications for other countries. Expert Rev. Pharmacoecon. Outcomes Res. 12, 809–819. doi: 10.1586/erp.12.71
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Cacace, M., Ettelt, S., Mays, N., and Nolte, E. (2013). Assessing quality in cross-country comparisons of health systems and policies: towards a set of generic quality criteria. Health Policy 112, 156–162. doi: 10.1016/j.healthpol.2013.03.020
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Cahir, C., Fahey, T., Tilson, L., Teljeur, C., and Bennett, K. (2012). Proton pump inhibitors: potential cost reductions by applying prescribing guidelines. BMC Health Serv Res. 12:408. doi: 10.1186/1472-6963-12-408
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Coma, A., Zara, C., Godman, B., Agusti, A., Diogene, E., Wettermark, B., et al. (2009). Policies to enhance the efficiency of prescribing in the Spanish Catalan region: impact and future direction. Expert Rev. Pharmacoecon. Outcomes Res. 9, 569–581. doi: 10.1586/erp.09.58
Durbin, J., and Watson, G. (1951). Testing for serial correlation in least square regression. Biometrika 37, 409–428.
Frank, R. G. (2007). The ongoing regulation of generic drugs. N. Engl. J. Med. 357, 1993–1996. doi: 10.1056/NEJMp078193
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Garuoliene, K., Godman, B., Gulbinovic, J., Wettermark, B., and Haycox, A. (2011). European countries with small populations can obtain low prices for drugs: Lithuania as a case history. Expert Rev. Pharmacoecon. Outcomes Res. 11, 343–349. doi: 10.1586/erp.11.24
Godman, B., Abuelkhair, M., Vitry, A., Abdu, S., Bennie, M., Bishop, I., et al. (2012a). Payers endorse generics to enhance prescribing efficiency; impact and future implications, a case history approach. GaBI J. 1, 21–35. doi: 10.5639/gabij.2012.0102.017
Godman, B., Bennie, M., Baumgärtel, C., Sović Brkičić, L., Burkhardt, T., Furst, J., et al. (2012b). Essential to increase the use of generics in Europe to maintain comprehensive healthcare? Farmeconomia 13, 5–20.
Godman, B., Bennie, M., Bucsics, A., Hesse, U., Martin, A., Miranda, J., et al. (2013b). Variable approaches in Europe to the availability of generic losartan; implications for the future. Clin. Ther. 35, e36–e37. doi: 10.1016/j.clinthera.2013.07.088
Godman, B., Bishop, I., Finlayson, A. E., Campbell, S., Kwon, H. Y., and Bennie, M. (2013c). Reforms and initiatives in Scotland in recent years to encourage the prescribing of generic drugs, their influence and implications for other countries. Expert Rev. Pharmacoecon. Outcomes Res. 13, 469–482. doi: 10.1586/14737167.2013.820956
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Godman, B., Bucsics, A., Burkhardt, T., Haycox, A., Seyfried, H., and Wieninger, P. (2008). Insight into recent reforms and initiatives in Austria: implications for key stakeholders. Expert Rev. Pharmacoecon. Outcomes Res. 8, 357–371. doi: 10.1586/14737167.8.4.357
Godman, B., De Bruyn, K., Miranda, J., Raschi, E., Bennie, M., Barbui, C., et al. (2013e). Generic atypical antipsychotic drugs in Belgium: their influence and implications. J. Comp. Eff. Res. 2, 551–561. doi: 10.2217/cer.13.75
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Godman, B., Shrank, W., Andersen, M., Berg, C., Bishop, I., Burkhardt, T., et al. (2010a). Policies to enhance prescribing efficiency in europe: findings and future implications. Front. Pharmacol. 1:141. doi: 10.3389/fphar.2010.00141
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Godman, B., Shrank, W., Andersen, M., Berg, C., Bishop, I., Burkhardt, T., et al. (2010b). Comparing policies to enhance prescribing efficiency in Europe through increasing generic utilization: changes seen and global implications. Expert Rev. Pharmacoecon. Outcomes Res. 10, 707–722. doi: 10.1586/erp.10.72
Godman, B., Wettermark, B., Hoffmann, M., Andersson, K., Haycox, A., and Gustafsson, L. L. (2009). Multifaceted national and regional drug reforms and initiatives in ambulatory care in Sweden: global relevance. Expert Rev. Pharmacoecon. Outcomes Res. 9, 65–83. doi: 10.1586/14737167.9.1.65
Godman, B., Wettermark, B., Miranda, J., Bennie, M., Martin, A., and Malmstrom, R. E. (2013a). Influence of multiple initiatives in Sweden to enhance ARB prescribing efficiency following generic losartan; findings and implications for other countries. Int. J. Clin. Pract. 67, 853–862. doi: 10.1111/ijcp.12130
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Godman, B., Wettermark, B., van Woerkom, M., Fraeyman, J., Alvarez-Madrazo, S., Berg, C., et al. (2014). Multiple policies to enhance prescribing efficiency for established medicines in Europe with a particular focus on demand-side measures: findings and future implications. Front. Pharmacol. Focused Rev. 5:106. doi: 10.3389/fphar.2014.00106
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Godman, B., Campbell, S., Suh, H. S., Finlayson, A., Bennie, M., and Gustafsson, L. (2013d). Ongoing measures to enhance prescribing efficiency across Europe: implications for other countries. J. Health Tech. Assess 1, 27–42.
Gustafsson, L. L., Wettermark, B., Godman, B., Andersen-Karlsson, E., Bergman, U., Hasselstrom, J., et al. (2011). The “wise list”- a comprehensive concept to select, communicate and achieve adherence to recommendations of essential drugs in ambulatory care in Stockholm. Basic Clin. Pharmacol. Toxicol. 108, 224–233. doi: 10.1111/j.1742-7843.2011.00682.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Heran, B. S., Wong, M. M., Heran, I. K., and Wright, J. M. (2008). Blood pressure lowering efficacy of angiotensin receptor blockers for primary hypertension. Cochrane Database Syst. Rev. Cd003822. doi: 10.1002/14651858.CD003822.pub2
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Hesse, U., Godman, B., Petzold, M., Martin, A., and Malmstrom, R. E. (2013). Impact of delisting ARBs, apart from losartan, on ARB utilisation patterns in Denmark: implications for other countries. Appl. Health Econ. Health Policy 11, 677–685. doi: 10.1007/s40258-013-0059-4
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
IMS Institute for Health Informatics. (2011). The Global Use of Medicines: Outlook Through 2015. Available online at: http://www.imshealth.com/deployedfiles/ims/Global/Content/Insights/IMS%20Institute%20for%20Healthcare%20Informatics/Global_Use_of_Medicines_Report.pdf (Accessed May 2011).
Jack, A. (2008). Balancing big pharma's books. BMJ 336, 418–419. doi: 10.1136/bmj.39491.469005.94
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Kalaba, M., Godman, B., Vuksanovic, A., Bennie, M., and Malmstrom, R. E. (2012). Possible ways to enhance renin-angiotensin prescribing efficiency: republic of Serbia as a case history? J. Comp. Eff. Res. 1, 539–549. doi: 10.2217/cer.12.62
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Makani, H., Bangalore, S., Supariwala, A., Romero, J., Argulian, E., and Messerli, F. H. (2014). Antihypertensive efficacy of angiotensin receptor blockers as monotherapy as evaluated by ambulatory blood pressure monitoring: a meta-analysis. Eur. Heart J. 35, 1732–1742. doi: 10.1093/eurheartj/eht333
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Markovic-Pekovic, V., Skrbic, R., Godman, B., and Gustafsson, L. L. (2012). Ongoing initiatives in the Republic of Srpska to enhance prescribing efficiency: influence and future directions. Expert Rev. Pharmacoecon. Outcomes Res. 12, 661–671. doi: 10.1586/erp.12.48
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Martin, A., Godman, B., Miranda, J., Tilstone, J., Saleem, N., Olsson, E., et al. (2014). Measures to improve angiotensin receptor blocker prescribing efficiency in the UK: findings and implications. J. Comp. Eff. Res. 3, 41–51. doi: 10.2217/cer.13.83
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
McDowall, D., McCleary, R., Meidinger, E. E., and Hay, R. A. (1980). Interrupted Time Series Analysis. Sage University Papers Series on Quantitative Applications in the Social Sciences, 07–021. Thousand Oakes, CA: Sage Publications Inc.
McGinn, D., Godman, B., Lonsdale, J., Way, R., Wettermark, B., and Haycox, A. (2010). Initiatives to enhance the quality and efficiency of statin and PPI prescribing in the UK: impact and implications. Expert Rev. Pharmacoecon. Outcomes Res. 10, 73–85. doi: 10.1586/erp.09.73
Moon, J. C., Flett, A. S., Godman, B. B., Grosso, A. M., and Wierzbicki, A. S. (2010). Getting better value from the NHS drug budget. BMJ 341:c6449. doi: 10.1136/bmj.c6449
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Olsson, E., Ingman, P., Ahmed, B., and Kalvemark Sporrong, S. (2014). Pharmacist-patient communication in Swedish community pharmacies. Res. Social Adm. Pharm. 10, 149–155. doi: 10.1016/j.sapharm.2013.03.001
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Olsson, E., and Kalvemark Sporrong, S. (2012). Pharmacists' experiences and attitudes regarding generic drugs and generic substitution: two sides of the coin. Int. J. Pharm. Pract. 20, 377–383. doi: 10.1111/j.2042-7174.2012.00214.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
R Development Core Team. (2012). A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing. Available online at: http://www.R-project.org/
Regional Drugs and Therapeutics Centre (NHS). (2008). Fixed-Dose Combinations (Part 2) - Use in Specific Medical Conditions. Available online at: http://www.formulary.cht.nhs.uk/pdf,_doc_files_etc/RDTC/Drug_Updates/062_Fixed-Dose_Combinations_(2).pdf
Ronning, M., Blix, H. S., Harbo, B. T., and Strom, H. (2000). Different versions of the anatomical therapeutic chemical classification system and the defined daily dose–are drug utilisation data comparable? Eur. J. Clin. Pharmacol. 56, 723–727. doi: 10.1007/s002280000200
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Ross-Degnan, D., Soumerai, S. B., Fortess, E. E., and Gurwitz, J. H. (1993). Examining product risk in context. Market withdrawal of zomepirac as a case study. JAMA 270, 1937–1942. doi: 10.1001/jama.270.16.1937
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Simoens, S. (2012). A reviewof genericmedicine pricing in Europe. GaBI J. 1, 8–12. doi: 10.5639/gabij.2012.0101.004
Simoens, S. D., Bruyn, K., Miranda, J., Bennie, M., Malmström, R. E., and Godman, B. (2013). Measures to enhance ARB prescribing efficiency in Belgium following generic losartan: impact and implications for the future. J. Pharm. Health Serv. Res. 4, 173–181. doi: 10.1111/jphs.12024
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Svanstrom, H., Pasternak, B., and Hviid, A. (2012). Association of treatment with losartan vs candesartan and mortality among patients with heart failure. JAMA 307, 1506–1512. doi: 10.1001/jama.2012.452
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Usher-Smith, J., Ramsbottom, T., Pearmain, H., and Kirby, M. (2008). Evaluation of the clinical outcomes of switching patients from atorvastatin to simvastatin and losartan to candesartan in a primary care setting: 2 years on. Int. J. Clin. Pract. 62, 480–484. doi: 10.1111/j.1742-1241.2007.01690.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Vlahovic-Palcevski, V., Gantumur, M., Radosevic, N., Palcevski, G., and Vander Stichele, R. (2010). Coping with changes in the defined daily dose in a longitudinal drug consumption database. Pharm. World Sci. 32, 125–129. doi: 10.1007/s11096-010-9366-0
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Vogler, S. (2012). The impact of pharmaceutical pricing and reimbursement policies on generics uptake: implementation of policy options on generics in 29 European countries-an overview. GaBI J. 1, 93–100. doi: 10.5639/gabij.2012.0102.020
Voncina, L., Strizrep, T., Godman, B., Bennie, M., Bishop, I., Campbell, S., et al. (2011). Influence of demand-side measures to enhance renin-angiotensin prescribing efficiency in Europe: implications for the future. Expert Rev. Pharmacoecon. Outcomes Res. 11, 469–479. doi: 10.1586/erp.11.42
Wagner, A. K., Soumerai, S. B., Zhang, F., and Ross-Degnan, D. (2002). Segmented regression analysis of interrupted time series studies in medication use research. J. Clin. Pharm. Ther. 27, 299–309. doi: 10.1046/j.1365-2710.2002.00430.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Wettermark, B., Godman, B., Jacobsson, B., and Haaijer-Ruskamp, F. M. (2009). Soft regulations in pharmaceutical policy making: an overview of current approaches and their consequences. Appl. Health Econ. Health Policy 7, 137–147. doi: 10.1007/BF03256147
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Wettermark, B., Godman, B., Neovius, M., Hedberg, N., Mellgren, T. O., and Kahan, T. (2010). Initial effects of a reimbursement restriction to improve the cost-effectiveness of antihypertensive treatment. Health Policy 94, 221–229. doi: 10.1016/j.healthpol.2009.09.014
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
WHO. (2003). Introduction to Drug Utilisation Research. WHO International Working Group for Drug Statistics Methodology, WHO Collaborating Centre for Drug Statistics Methodology, WHO Collaborating Centre for Drug Utilization Research and Clinical Pharmacological Services. Available online at: http://www.who.int/medicines/areas/quality_safety/safety_efficacy/Drug%20utilization%20research.pdf
WHO Collaborating Centre for Drug Statistics Methodology. (2013). ATC/DDD Index 2011. Oslo: WHO. Available online at: http://www.whocc.no/atc_ddd_index/
Keywords: losartan, generics, demand-side measures, cross-national study, drug utilisation, Europe
Citation: Moon JC, Godman B, Petzold M, Alvarez-Madrazo S, Bennett K, Bishop I, Bucsics A, Hesse U, Martin A, Simoens S, Zara C and Malmström RE (2014) Different initiatives across Europe to enhance losartan utilization post generics: impact and implications. Front. Pharmacol. 5:219. doi: 10.3389/fphar.2014.00219
Received: 06 July 2014; Accepted: 09 September 2014;
Published online: 08 October 2014.
Edited by:
Dominique J. Dubois, Université Libre de Bruxelles, BelgiumReviewed by:
Keith Tolley, Tolley Health Economics, UKNora Ibargoyen, Basque Office for Health Technology Assessment, Spain
Copyright © 2014 Moon, Godman, Petzold, Alvarez-Madrazo, Bennett, Bishop, Bucsics, Hesse, Martin, Simoens, Zara and Malmström. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Brian Godman, Division of Clinical Pharmacology, Department of Laboratory Medicine, Karolinska Institutet, Karolinska University Hospital Huddinge, Stockholm SE-141 86, Sweden e-mail: brian.godman@ki.se