 Heikki M. Karinen1,2* Arja Uusitalo2 Henri Vähä-Ypyä3 Mika Kähönen4 Juha E. Peltonen2,7 Phyllis K. Stein5 Jari Viik6 Heikki O. Tikkanen2,7
Heikki M. Karinen1,2* Arja Uusitalo2 Henri Vähä-Ypyä3 Mika Kähönen4 Juha E. Peltonen2,7 Phyllis K. Stein5 Jari Viik6 Heikki O. Tikkanen2,7- 1Unit for Occupational Health, Department of Health Sciences, University of Tampere, Tampere, Finland
- 2Department of Sports and Exercise Medicine, Institute of Clinical Medicine, University of Helsinki, Helsinki, Finland
- 3Department of Biology of Physical Activity, University of Jyväskylä, Jyväskylä, Finland
- 4Department of Clinical Physiology, University of Tampere and Tampere University Hospital, Tampere, Finland
- 5Division of Cardiology, Washington University School of Medicine, St. Louis, MO, USA
- 6Department of Biomedical Engineering, Tampere University of Technology, Tampere, Finland
- 7Clinic for Sports and Exercise Medicine, Foundation for Sports and Exercise Medicine, Helsinki, Finland
Objective: If the body fails to acclimatize at high altitude, acute mountain sickness (AMS) may result. For the early detection of AMS, changes in cardiac autonomic function measured by heart rate variability (HRV) may be more sensitive than clinical symptoms alone. The purpose of this study was to ascertain if the changes in HRV during ascent are related to AMS. Methods: We followed Lake Louise Score (LLS), arterial oxygen saturation at rest (R-SpO2) and exercise (Ex-SpO2) and HRV parameters daily in 36 different healthy climbers ascending from 2400 m to 6300 m altitudes during five different expeditions. Results: After an ascent to 2400 m, root mean square successive differences, high-frequency power (HF2 min) of HRV were 17–51% and Ex-SpO2 was 3% lower in those climbers who suffered from AMS at 3000 to 4300 m than in those only developing AMS later (≥5000 m) or not at all (all p < 0.01). At the altitude of 2400 m RMSSD2 min ≤ 30 ms and Ex-SpO2 ≤ 91% both had 92% sensitivity for AMS if ascent continued without extra acclimatization days. Conclusions: Changes in supine HRV parameters at 2400 m were related to AMS at 3000–4300 m Thus, analyses of HRV could offer potential markers for identifying the climbers at risk for AMS.
Introduction
When ascending to high altitude, the body needs to acclimatize to low atmospheric pressure and hypoxic hypoxia (Hackett and Roach, 2001). If the adaptation process fails due to too rapid ascent rate or susceptibility of the climber, one or more of three illnesses may result: acute mountain sickness (AMS), high altitude cerebral edema (HACE) or high altitude pulmonary edema (HAPE). AMS is the most common of these problems affecting 25% of those who ascend to altitudes of 1850–2750 m (Honigman et al., 1993), 42% at altitudes of 3000 m (Hackett and Roach, 2001) and as many as 75% among those attempting Mount Kilimanjaro (5984 m) (Karinen et al., 2008). AMS is a non-specific syndrome characterized by the presence of headache and at least one of the following: gastrointestinal symptoms (loss of appetite, nausea, and vomiting), insomnia, dizziness, and weakness or fatigue. It is a self-limiting syndrome, which usually resolves in 1–2 days if properly treated (rest, descent to lower altitude, medication etc.) but may sometimes progress to more serious altitude illnesses such as HAPE and HACE (Hackett and Roach, 2001; Imray et al., 2011).
The exact mechanism causing AMS is unknown, but a marked increase in peripheral sympathetic activity is a common feature of AMS (Kamimori et al., 2009) and may be involved in the pathogenesis of HAPE (Mazzeo et al., 1998; Duplain et al., 1999; West, 2004). Heart rate variability (HRV) reflects sympathetic and parasympathetic cardiac autonomic nervous system regulation. Several studies have shown a transient reduction in parasympathetic and increased sympathetic activity during acute exposure to hypobaric hypoxia (Zuzewicz et al., 1999; Sevre et al., 2001; Saito et al., 2005; Hainsworth et al., 2007) which tended to be reversed with acclimatization (Cornolo et al., 2004).
There is a need for a non-invasive, specific and convenient method under field conditions for the detection of inadequate acclimatization and impending AMS. The arterial oxygen saturation (SpO2) measurement is useful in anticipating AMS (Roach et al., 1998; Karinen et al., 2010) but use of pulse oximetry under field conditions is susceptible to many disruptive factors e.g., temperature (Luks and Swenson, 2011). Reduction in parasympathetic and increased sympathetic activity during acclimatization and AMS at 3180–4559 m altitudes have been shown in several studies (Loeppky et al., 2003; Lanfranchi et al., 2005; Chen et al., 2008; Huang et al., 2010). To the best of our knowledge, studies on HRV conducted in the field at extreme altitudes (>5000 m) are still lacking, despite two studies at simulated altitude (Yamamoto et al., 1993; Wille et al., 2012). Therefore the purpose of this study was to evaluate whether HRV is related to AMS during ascent and provides new information on the changes in cardiac autonomic function as measured by HRV and not limited to altitudes between 2400 and 5000 m, which are most frequent among climbers, but also at extreme altitudes above 5000 m under field conditions.
Materials and Methods
The study group consisted of participants in four different expeditions to Denali (Denali 1, Denali 2), Shisha Pangma and Mount Everest. All subjects were informed about the objective of the study and the experimental protocol. The Ethics Committee of Tampere University Hospital, Finland, approved the study protocol, and all subjects gave informed consent prior to the measurements, as stipulated in the Declaration of Helsinki. Thirty six different healthy volunteers (2 women and 34 men) with an age range of 24–45 years participated in this study. Subjects' mean age was 32 (SD 6) years, body mass index (BMI) 25 (3) kg/m2 and maximal oxygen uptake () 59 (7) ml/kg/min. None of the subjects had been exposed to an altitude above 1000 m within the 6 months prior to this study. They were all lowland dwellers and recreational mountaineers, and during the expeditions none had taken acetazolamide as an AMS prophylaxis. Two climbers were taking regular medication for asthma but no one was using oral steroids, salmeterol, sildenafil or nifedipin. All expeditions were organized in April-May. Ascent profiles were similar at sleeping altitudes, but three expeditions had faster and two slower ascent rate. Before the expeditions, all members underwent a medical examination including resting ECG and flow volume spirometry. To examine their exercise responses and to measure maximal oxygen uptake (), they performed an incremental clinical exercise test on a cycle ergometer (Ergoline 800S, Ergoline GmbH, Bitz, Germany). They started cycling at 20 W and work rate was increased stepwise 20 W/min up to volitional fatigue. A 12-lead ECG was obtained at rest before the exercise, and during the exercise test. All subjects had a normal EKG and none developed arrhythmias during the exercise test.
Data Collection During Ascent
Autonomic cardiac function was assessed by analysis of R-R intervals (RRI). In power spectral analysis of HRV total variability of RRI is divided into low and high frequency bands. High frequency power (HF power, 0.15–0.40 Hz) reflects cardiac parasympathetic modulation and is influenced by respiration. Low frequency power (LF power, 0.04–0.15 Hz) reflects both cardiac sympathetic and parasympathetic modulation. The ratio of LF and HF powers (LF/HF) has been reported to reflect sympathovagal balance. RMSSD is the square root of the mean squared differences of successive RRI and it is considered to be an index of cardiac parasympathetic modulation (Task Force, 1996).
In the present study, HRV and SpO2 data were collected every day during ascent at altitudes of 2400, 3000, 3500, 4300, 5000, and 5300 m in all expeditions, and up to 5600 and 6300 m at Shisha Pangma. Data collection was continued until the base camp of each mountain was reached. Measurements were done every morning after 7–8 h night rest at that altitude by heart rate monitors (Suunto T6, Suunto, Vantaa, Finland or S810, Polar Electro, Kempele, Finland). HR recordings were made in the supine position, after at least 15 min of rest in the same position while each subject laid quietly and breathed spontaneously. Then subjects started their HR monitors and continued lying down for 3 min. The last 2 min were chosen for data analysis. According to the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology (Task Force, 1996), the preferred duration of ECG recordings for computing short-term HRV components is 5 min. The recording should last at least 10 times the wavelength of the lowest frequency bound of the investigated component (Task Force, 1996). Thus a recording of approximately 1 min is needed to assess the HF and approximately 2 min are needed to address the LF component. In our study the duration of stationary RRI time series was 2 min, which should be adequate for the determination of the HRV components evaluated (Koskinen et al., 2009). The arterial oxygen saturation at rest (R-SpO2) was measured by finger oximetry (Nonin Medical, Onyx 9500, Plymouth MN, USA) after 15 min rest while the subject was seated for an additional 2 min. During this period, R-SpO2 was observed four times at 15 s intervals and the average R-SpO2 of these was recorded for data analysis. The arterial oxygen saturation during exercise (Ex-SpO2) at altitude was measured with a standard walking test (Karinen et al., 2010). The climber walked and controlled his speed with the HR monitor so that HR was approximately 150 beats/min during 3–5 min walking. Temperature varied between +20 and −15°C and hands were covered by mittens during walking, which ended inside a tent. The inside temperature was mostly between +5 and 20°C because of extensive solar radiation or a stove. Immediately after the cessation of walking, SpO2 was measured in sitting position by finger oximetry four times at 5 s intervals during the first 15 s of recovery starting immediately after stopping the exercise test. The average of these values was recorded as Ex-SpO2 for data analysis. We observed that SpO2 decreased 15 s after the exercise began. During the first 15 s the SpO2 values remained very steady, varying just 0–1% unit, thus quite accurately reflecting also SpO2 during exercise.
Data Analysis
Data processing and analysis were performed after the expeditions by Polar Precision Performance software (version 3.02.007) and Kubios software (version 2.0) (Niskanen et al., 2004). Areas of ectopy or artifact were identified and fixed by manual or automatic error correction. Corrected segments were less than 5% of the analyzed data. Analysis of HRV was done for stationary 2 min data segments. The power spectra were quantified by measuring the area in two frequency bands. The HF2 min power was calculated for frequency band 0.15–0.40 Hz and LF2 min power for frequency band 0.04–0.15 Hz.
After the HRV and SpO2 measurements subjects were scored according to the Lake Louise scoring (LLS) AMS system, which include a self-report questionnaire related to the presence and severity of symptoms and a clinical assessment (Hackett and Oelz, 1992). The LLS was obtained by adding the score of the clinical section to the self-report questionnaire. AMS was diagnosed according to a recent gain in altitude, the presence of headaches and at least one of the following symptoms: gastrointestinal (GI) upset, fatigue, dizziness or insomnia. To study, retrospectively, whether HRV changes could have predicted AMS at higher altitudes, we divided the study group into two groups: (1) If the LLS was ≥ 3 at any altitude the subject was assigned to the AMS group, and (2) If the LLS was ≤ 2 at every altitude measured, the subject was assigned to the no-AMS group.
Statistical Analysis
Continuous values are presented as means ± standard deviation (SD). The frequency of parameters was assessed by x2 tests with Yates' correction. Differences between AMS and no-AMS groups were compared by nonparametric t-test. Correlations between the LLS and clinical and autonomic variables were assessed by Pearson's correlation. In all tests p ≤ 0.05 was considered significant.
Results
In total, 36 subjects were studied up to the altitude of 4300 m. Three discontinued because of AMS and the remaining 33 continued up to 5000 and 5300 m altitudes. Five made all measurements at 5600 and one at 6300 m altitude. The Denali 1 and Shisha expeditions reached the altitude of 5000 m in 7 days (n = 16) and the Denali 2 and Everest expeditions took 11–17 days to reach the same altitude (n = 20) (Figure 1). Acute mountain sickness developed in 24 out of 36 (66%) subjects at some altitude between 3000 and 5600 m, including both women and 22 of 34 men, while 12 men (34%) did not get AMS at any altitude (no-AMS group). There were 11 AMS cases in the faster group and 13 AMS cases in the slower group. The groups did not differ in age, BMI or . The descriptive data of participants and ascents for each expedition are presented in Table 1 and Figure 1.
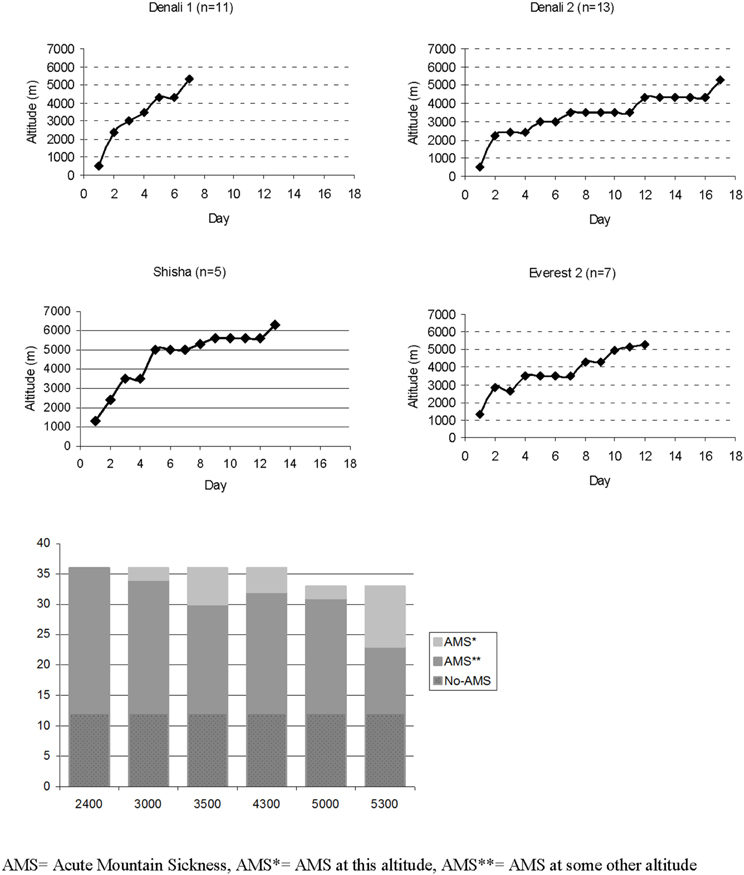
Figure 1. Ascent profiles of different expeditions and number of AMS cases at different altitudes. Three climbers descended after 4300 m because of AMS. Measurements were made daily up to 5300 m except on Shisha Pangma, where measurements were made up to 5600 m. AMS, Acute Mountain Sickness; AMS*, AMS at this altitude; AMS**, AMS at some other altitude.
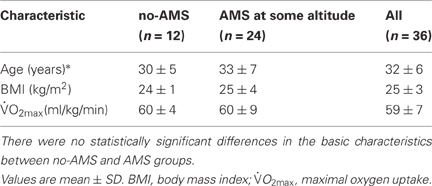
Table 1. Demographic data (age, BMI, and ) of the study population.
During this study, the daily ascent rates were mostly higher than what is generally recommended (300 m/day) but quite common for these mountains (range 400–1500 m). In the no-AMS group, RMSSD2 min, LF2 min and HF2 min increased in the first few days of the ascent. Above 3500 m all HRV parameters decreased while HR increased.
The number of AMS cases at different altitudes is presented in Figure 1. Among those who suffered from AMS, LLS scores varied between 3 and 8. Most of the AMS cases occurred at 5300 m (n = 10), and the prevalence of AMS increased significantly with altitude and fast ascent rate on the day before onset (both p < 0.001) (Figure 1). Headache and difficulty in sleeping were the most frequent symptoms of AMS followed by GI symptoms, fatigue, and dizziness.
At 2400 m altitude, RMSSD2 min and HF2 min were lower among those climbers who got AMS at lower altitudes (3000–4300 m) (n = 12) than in those who got AMS 3–7 days later at higher altitude (≥5000 m) (n = 12) or not at all (n = 12) (Table 2). HR2 min, lnHF2 min and RMSSD2 min at 2400 m correlated with the lowest altitude at which a climber suffered AMS (AMS altitude) (Figure 2). There were no differences between R-SpO2 at 2400 m and later onset of AMS, but Ex-SpO2 was statistically higher in the no-AMS than the AMS group at 3000–4300 m (p < 0.01) (95% CI 3 (1–5) and in the AMS at ≥ 5000 m group (p < 0.05). However, Ex-SpO2 did not correlate with the AMS altitude (r = −0.028). At the altitude of 2400 m RMSSD2 min ≤ 30 ms and Ex-SpO2 ≤ 91% both had 92% sensitivity for AMS at 3000–4300 m if the ascent continued without extra acclimatization days (Figure 3). The sensitivity, specificity, positive, and negative predicative values for chosen cut-off values are presented in Table 3.
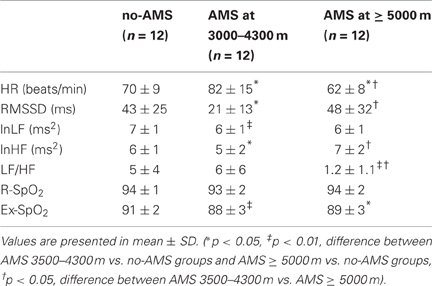
Table 2. Resting heart rate (HR) and HRV parameters at 2400 m among the climbers who subsequently developed AMS at two different altitude ranges, and those who had no subsequent AMS.
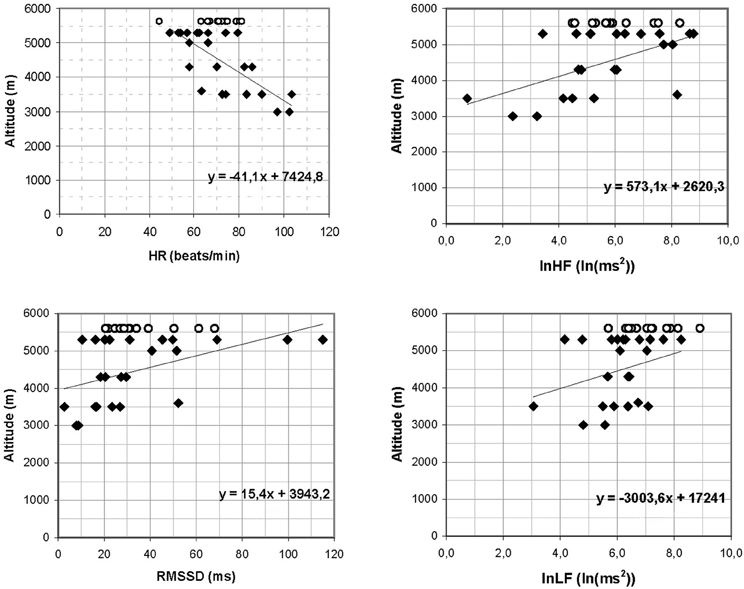
Figure 2. Negative correlation between HR and positive correlation between lnHF, lnLF, and RMSSD at 2400 m altitude and the lowest altitude at which a climber got AMS (HR r = −0.743, p < 0.01; lnHF r = 0.558, p < 0.05, lnLF r = 0.302, p > 0.05, RMSSD r = 0.495, p < 0.05). no-AMS subjects datapoints are added at 5600 m level.
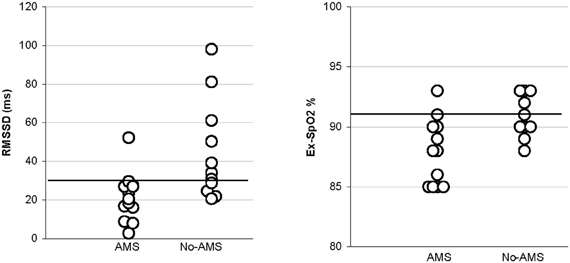
Figure 3. Scattergram showing the distribution of values of RMSSD and Ex-SpO2 measured in 24 study subjects at 2400 m in AMS and no-AMS. The cut-off lines RMSSD2min ≤ 30 ms and Ex-SpO2 ≤ 91% are for 92% sensitivity for AMS.

Table 3. Sensitivity and specificity of chosen parameters at 2400 m altitude for AMS at 3000–4300 m.
Discussion
Our most important finding was that subjects susceptible to AMS had lower HRV before the clinical manifestations of AMS than those who acclimatized well and did not get AMS. This is a new finding and offers fascinating options for predicting AMS at high altitude in field conditions.
The diagnosis of AMS is clinical, but some specific changes in cardiac autonomic function measured by HRV have been estimated to be more sensitive in the detection of the early signs of AMS than clinical symptoms alone at high altitudes (Saito et al., 2005). HRV is reported to decrease in absolute units (Hughson et al., 1994; Bernardi et al., 1998; Kanai et al., 2001) and LF/HF mostly increased when subject got AMS (Loeppky et al., 2003; Lanfranchi et al., 2005; Chen et al., 2008; Huang et al., 2010). There are, however, also opposite findings reported about HRV (Koehle et al., 2010). However, studies conducted in the field at high and extreme altitudes (>5000 m) are still lacking.
During mild sympathetic activation, the observed increase in HR has been reported to be associated with an increase in LF power (Elghozi and Julien, 2007). However, with more intense sympathetic stimulation, the increase in HR was reported to be associated with an overall decrease in HRV, including its LF component. Our present findings on changes in HRV values at extremely high altitudes support this concept.
At 2400 m the no-AMS group had higher HRV and lower HR2 min than the AMS group. The differences are not related to differences in physical fitness in the AMS and no-AMS groups because the basic maximum oxygen uptake did not differ significantly between the groups (59 ± 11 vs. 60 ± 4, p > 0.05). Furthermore, clear changes did not come in connection with the ascent. However, in the no-AMS group HF2 min tended to be lower, while LF2 min tended to be higher than in the AMS group. The physiologic significance of these findings remains uncertain, but they do not directly support the earlier assumption that AMS is simply connected with higher cardiac sympathetic activity. Rather, it seemed that a rise in cardiac sympathetic activity would have been a protective phenomenon against altitude illness. However, altitude illness is a dynamic process. It may be that as the AMS proceeds, HRV could further decrease. In other words, changes in HRV were related to higher altitudes in all climbers, but also notably to acclimatization and especially to failure to acclimatize.
The present findings are still generally in agreement with those of earlier studies and provide further insights into the usefulness of HRV in the prediction of AMS under field conditions. Several studies have shown that of SpO2 measurements at rest (R-SpO2) and immediately after exercise (Ex-SpO2) are predictors of AMS (Roach et al., 1998; Saito et al., 2005; Burtscher et al., 2008; Karinen et al., 2010). Our study supports this. At 2400 m altitude the Ex-SpO2 was statistically higher in no-AMS group than AMS 3000–4300 group (p < 0.01) and AMS ≥ 5000 m group (p < 0.05). However, the SpO2 measurements made by pulse oximetry under field conditions may be susceptible to many disruptive factors (temperature, bright light, cold fingers etc.) (Luks and Swenson, 2011). Therefore, it is desirable to have an another parameter(s) to follow-up for AMS susceptibility. Our findings support the possibility that HRV could be used along with commonly measured physiological parameters, HR and SpO2, clinical status and Lake Louise questionnaire for AMS prediction in the short time period at moderate altitudes. The altitude of 5000 m was reached mainly 1–2 weeks after the measurements at 2400 m and the ascent rates per day were high just before reaching this altitude (700–1500 m/day). This may explain better the high prevalence of AMS at 5000–5300 m than a predominant vagal modulation at rest at 2400 m.
The limitations of the present study include the relatively small study group (n = 33) at extreme altitude (>5000 m). The correlations between HRV parameters and AMS are rather weak. Thus, further studies with larger populations are needed to verify the early changes in HRV between subjects with and without AMS and/or other high-altitude illnesses, especially at extreme altitudes, where the consequences of AMS, HACE, and HAPE may dramatic. The length of measurements at high altitude may have been too short to fully observe trends of changes in HRV variables between subjects with and without AMS or to capture other HRV measures that could reflect more severe periodic breathing. The differences in ascent rates, the places studied and the altitudes studied may in part explain the differences between the different results. Environmental and/or cardiovascular effects of previous exercise may have been factors in the autonomic patterns observed in subjects with AMS in our study. However, subjects with and without AMS were studied under the same field conditions and after similar recovery times as regards ascent. The ascent rates during the expeditions were normal and widely used in the mountains. Therefore, exercise and environmental factors may not explain the differences in autonomic cardiovascular function observed in association with AMS in our study. HRV is also partially influenced by respiratory rate and depth (Task Force, 1996; Penttilä et al., 2001). In the HRV frequency spectrum, too, power in the entire frequency area, not just the HF band, is decreased if the respiration rate increases (Task Force, 1996). Normally respiration rates will increase somewhat at high altitude, but we do not know if the respiration rate is higher in subjects with AMS than in subjects with no AMS. In this study, the subjects were breathing spontaneously and some of the subjects may have had breathing rate close to or below 0.15 Hz, which is the lowest boundary for the HF band. For this reason, if altitude or AMS changed respiratory HRV, it cannot be exclusively judged by changes in HF or LF/HF. Unfortunately, we do not have sea-level HRV data for all subjects, so we cannot estimate whether those climbers whose basic level of HF is higher could acclimatize better than those whose HF level is lower at sea-level.
Periodic breathing has reported to exist at high altitude mainly during the sleep, but also in some extent during wake (Insalaco et al., 1996; Fan et al., 2012). Because the breathing frequency was not measured in our study, we cannot exclude it totally (McMullen et al., 2012). However, the visual analysis of RRI tachograms, AR spectrum and Poincare plots do not support the existence of periodic breathing during the measurements. The measurement periods were 2 min so we can assume that any significant periodic breathing was not seen when lying down during this measurement period.
The strengths of the present study are that the rate of ascent, altitude of origin and time of day of testing were known. Also, within each group every climber had a similar diet, they were relatively homogenous in their exercise capacity and they climbed the same route on mountains over a short period of time with essentially the same snow and weather conditions. Barometric pressure varied from day to day but during measurements it was stable.
In conclusion, at 2400 m decreased RMSSD2 min and HF2 min both predicted AMS in a few days if the ascent continued without rest days. Autonomic cardiac response to increasing altitude could be a low-cost non-invasive test to predict impending AMS and to help distinguish those who are at risk for AMS and those who are acclimatizing well. The trigger values typical for impending AMS await further studies.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Bernardi, L., Passino, C., Spadacini, G., Calciati, A., Robergs, R., Greene, R., Martignon, I E., Anand, I., and Appenzeller, O. (1998). Cardiovascular autonomic modulation and activity of carotid baroreceptors at altitude. Clin. Sci. 95, 565–573.
Burtscher, M., Szubski, C., and Faulhaber, M. (2008). Prediction of the susceptibility to AMS in simulated altitude. Sleep Breath 12, 103–108.
Chen, Y. C., Lin, F. C., Shiao, G. M., and Chang, S. C. (2008). Effect of rapid ascent to high altitude on autonomic cardiovascular modulation. Am. J. Med. Sci. 336, 248–353.
Cornolo, J., Mollard, P., Brugniaux, J. V., Robach, P., and Richalet, J. P. (2004). Autonomic control of the cardiovascular system during acclimatization to high altitude: effects of sildenafil. J. Appl. Physiol. 97, 935–940.
Duplain, H., Vollenweider, L., Delabays, A., Nicod, P., Bärtsch, P., and Scherrer, U. (1999). Augmented sympathetic activation during short-term hypoxia and high-altitude exposure in subjects susceptible to high-altitude pulmonary edema. Circulation 99, 1713–1718.
Elghozi, J.-L., and Julien, C. (2007). Sympathetic control of short-term heart rate variability and its pharmacological modulation. Fund. Clin. Pharmacol. 21, 337–347.
Fan, J. L., Burgess, K. R., Thomas, K. N., Lucas, S. J., Cotter, J. D., Kayser, B., Peebles, K. C., and Ainslie, P. N. (2012). Effects of acetazolamide on cerebrovascular function and breathing stability at 5050 m. J. Physiol. 590, 1213–1225.
Hackett, P. H., and Oelz, O. (1992). “The Lake Louise consensus on the definition and qualification of altitude illness,” in Hypoxia Mountain Medicine, eds J. Sutton, G. Goates, and C. Houston (Burlington, VT: Queen City Printers), 327–330.
Hainsworth, R., Drinkhill, M. J., and Rivera-Chira, M. (2007). The autonomic nervous system at high altitude. Clin. Auton. Res. 17, 13–19.
Honigman, B., Theis, M. K., Koziol-McLain, J., Roach, R., Yip, R., Houston, C., Moore, L. G., and Pearce, P. (1993). Acute mountain sickness in a general tourist population at moderate altitudes. Ann. Intern. Med. 118, 587–592.
Huang, H. H., Tseng, C. Y., Fan, J. S., Yen, D. H., Kao, W. F., Chang, S. C., Kuo, T. B., Huang, C. I., and Lee, C. H. (2010). Alternations of heart rate variability at lower altitude in the predication of trekkers with acute mountain sickness at high altitude. Clin. J. Sport Med. 20, 58–63.
Hughson, R. L., Yamamoto, Y., McCullough, R. E., Sutton, J. R., and Reeves, J. T. (1994). Sympathetic and parasympathetic indicators of heart rate control at altitude studied by spectral analysis. J. Appl. Physiol. 77, 2537–2542.
Imray, C., Booth, A., Wright, A., and Bradwell, A. (2011). Acute altitude illnesses. BMJ 343, 411–417.
Insalaco, G., Romano, S., Salvaggio, A., Braghiroli, A., Lanfranchi, P., Patruno, V., Donner, C. F., and Bonsignore, G. (1996). Cardiovascular and ventilatory response to isocapnic hypoxia at sea level and at 5,050 m. J. Appl. Physiol. 80, 1724–1730.
Kamimori, G. H., Ryan, E. J., Otterstetter, R., Barkley, J. E., Glickman, E. L., and Davis, H. Q. (2009). Catecholamine levels in hypoxia-lnduced acute mountain sickness. Aviat. Space Environ. Med. 80, 376–380.
Kanai, M., Nishihara, F., Shiga, T., Shimada, H., and Saito, S. (2001). Alterations in autonomic nervous control of heart rate among tourists at 2700 and 3700 m above sea level. Wilderness Environ. Med. 12, 8–12.
Karinen, H., Peltonen, J., Kähönen, M., and Tikkanen, H. (2010). Prediction of acute mountain sickness by monitoring arterial oxygen saturation during ascent. High Alt. Med. Biol. 4, 325–332.
Karinen, H., Peltonen, J., and Tikkanen, H. (2008). Prevalence of acute mountain sickness among Finnish trekkers on Mount Kilimanjaro, Tanzania: an observational study. High Alt. Med. Biol. 4, 301–306.
Koehle, M. S., Guenette, J. A., and Warburton, D. E. (2010). Oximetry, heart rate variability, and the diagnosis of mild-to-moderate acute mountain sickness. Eur. J. Emerg. Med. 17, 119–122.
Koskinen, T., Kähönen, M., Jula, A., Mattsson, N., Laitinen, T., Keltikangas-Järvinen, L., Viikari, J., Välimäki, I., Rönnemaa, T., and Raitakari, O. T. (2009). Metabolic syndrome and short-term heart rate variability in young adults. The cardiovascular risk in young Finns study. Diabet. Med. 26, 354–361.
Lanfranchi, P. A., Colombo, R., Cremona, G., Baderna, P., Spagnolatti, L., Mazzuero, G., Wagner, P., Perini, L., Wagner, H., Cavallaro, C., and Giannuzzi, P. (2005). Autonomic cardiovascular regulation in subjects with acute mountain sickness. Am. J. Physiol. Heart Circ. Physiol. 289, 2364–2372.
Loeppky, J. A., Icenogle, M. V., Maes, D., Riboni, K., Scotto, P., and Roach, R. C. (2003). Body temperature, autonomic responses, and acute mountain sickness. High Alt. Med. Biol. 4, 367–373.
Luks, A. M., and Swenson, E. R. (2011). Clinician's corner: pulse oximetry at high altitude. High Alt. Med. Biol. 12, 109–119.
Mazzeo, R. S., Child, A., Butterfield, G. E., Mawson, J. T., Zamudio, S., and Moore, L. G. (1998). Catecholamine response during 12 days of high-altitude exposure (4 300 m) in women. J. Appl. Physiol. 84, 1151–1157.
McMullen, M. K., Whitehouse, J. M., Shine, G., and Towell, A. (2012). Respiratory and non-respiratory sinus arrhythmia: implications for heart rate variability. J. Clin. Monit. Comput. 26, 21–28.
Niskanen, J. P., Tarvainen, M. P., Ranta-Aho, P. O., and Karjalainen, P. A. (2004). Software for advanced HRV analysis. Comput. Methods Programs Biomed. 76, 73–81.
Penttilä, J., Helminen, A., Jartti, T., Kuusela, T., Huikuri, H. V., Tulppo, M. P., Coffeng, R., and Scheinin, H. (2001). Time domain, geometrical and frequency domain analysis of cardiac vagal outflow: effects of various respiratory patterns. Clin. Physiol. 21, 365–376.
Roach, R. C., Greene, E. R., Schoene, R. B., and Hackett, P. H. (1998). Arterial oxygen saturation for prediction of acute mountain sickness. Aviat. Space Environ. Med. 69, 1182–1185.
Saito, S., Tanobe, K., Yamada, M., and Nishihara, F. (2005). Relationship between arterial oxygen saturation and heart rate variability at high altitudes. Am. J. Emerg. Med. 23, 8–12.
Sevre, K., Bendz, B., Hankø, E., Nakstad, A. R., Hauge, A., Kåsin, J. I., Lefrandt, J. D., Smit, A. J., Eide, I., and Rostrup, M. (2001). Reduced autonomic activity during stepwise exposure to high altitude. Acta. Physiol. Scand. 173, 409–417.
Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. (1996). Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 93, 1043–1065.
West, J. B. (2004). The physiologic basis of high-altitude diseases. Ann. Intern. Med. 141, 789–800.
Wille, M., Mairer, K., Gatterer, H., Philippe, M., Faulhaber, M., and Burtscher, M. (2012). Changes in cardiac autonomic activity during a passive 8 hour acute exposure to 5 500 m normobaric hypoxia are not related to the development of acute mountain sickness. Int. J. Sports Med. 33, 186–191.
Yamamoto, Y., Hughson, R. L., Sutton, J. R., Houston, C. S., Cymerman, A., Fallen, E. L., and Kamath, M. V. (1993). Operation Everest II: an indication of deterministic chaos in human heart rate variability at simulated extreme altitude. Biol. Cybern. 69, 205–212.
Keywords: extreme altitude, altitude illness, heart rate variation, mountaineering
Citation: Karinen HM, Uusitalo A, Vähä-Ypyä H, Kähönen M, Peltonen JE, Stein PK, Viik J and Tikkanen HO (2012) Heart rate variability changes at 2400 m altitude predicts acute mountain sickness on further ascent at 3000–4300 m altitudes. Front. Physio. 3:336. doi: 10.3389/fphys.2012.00336
Received: 10 February 2012; Paper pending published: 21 March 2012;
Accepted: 31 July 2012; Published online: 30 August 2012.
Edited by:
Federico Lombardi, University of Milan, ItalyReviewed by:
Federico Lombardi, University of Milan, ItalyRobert Boushel, University of Copenhagen, Denmark
Copyright © 2012 Karinen, Uusitalo, Vähä-Ypyä, Kähönen, Peltonen, Stein, Viik and Tikkanen. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits use, distribution and reproduction in other forums, provided the original authors and source are credited and subject to any copyright notices concerning any third-party graphics etc.
*Correspondence: Heikki M. Karinen, Department of Health Sciences, University of Tampere, Medisiinarinkatu 3, 33521 Tampere, Finland. e-mail: heikki.karinen@uta.fi