 Carola Maggiora Vergano
Carola Maggiora Vergano Marco Lauriola
Marco Lauriola Anna M. Speranza
Anna M. Speranza- 1Department of Dynamic and Clinical Psychology, Sapienza University, Rome, Italy
- 2Department of Developmental Processes and Socialization, Sapienza University, Rome, Italy
Research on the etiology of adult psychopathology and its relationship with childhood trauma has focused primarily on specific forms of maltreatment. This study developed an instrument for the assessment of childhood and adolescence trauma that would aid in identifying the role of co-occurring childhood stressors and chronic adverse conditions. The Complex Trauma Questionnaire (ComplexTQ), in both clinician and self-report versions, is a measure for the assessment of multi-type maltreatment: physical, psychological, and sexual abuse; physical and emotional neglect as well as other traumatic experiences, such rejection, role reversal, witnessing domestic violence, separations, and losses. The four-point Likert scale allows to specifically indicate with which caregiver the traumatic experience has occurred. A total of 229 participants, a sample of 79 nonclinical and that of 150 high-risk and clinical participants, were assessed with the ComplexTQ clinician version applied to Adult Attachment Interview (AAI) transcripts. Initial analyses indicate acceptable inter-rater reliability. A good fit to a 6-factor model regarding the experience with the mother and to a 5-factor model with the experience with the father was obtained; the internal consistency of factors derived was good. Convergent validity was provided with the AAI scales. ComplexTQ factors discriminated normative from high-risk and clinical samples. The findings suggest a promising, reliable, and valid measurement of early relational trauma that is reported; furthermore, it is easy to complete and is useful for both research and clinical practice.
Introduction
Over the past two decades, evidence regarding the harmful impact of early maltreatment has accumulated significantly. Two-thirds of adolescents and adults report having suffered from child relational trauma, which represents a root cause of major public health issues (Copeland et al., 2007; van der Kolk and d'Andrea, 2010). Previous research has primarily focused on single types of maltreatment sequelae; however, most maltreated children experience more than one form of abuse and neglect (Kessler, 2000; Spinazzola et al., 2005; Pynoos et al., 2008). Indeed, in literature on child abuse, the focus has shifted from individual and specific conditions of risk to a multi-determined etiology of the traumatic experience: initially, the literature focused on a punctiform trauma but now investigates the concept of complex trauma, describing a traumatic developmental context in which the child is immersed. Complex trauma can be understood as experiences of cumulative, chronic, and prolonged traumatic events, most often of an interpersonal nature, involving primary caregiving system, and frequently arising in early childhood or adolescence (Cook et al., 2005; Courtois, 2008). Till date, growing evidence has acknowledged the co-occurrence of multiple types of severe adversities (Mullen et al., 1996; Higgins and McCabe, 2001; Diaz et al., 2002; Clemmons et al., 2003; Dong et al., 2004; Stevens et al., 2005; Arata et al., 2007; Finkelhor et al., 2007, 2009; Turner et al., 2010; Greeson et al., 2011; Trickett et al., 2011) and their greater risk for subsequent trauma exposure and cumulative clinical impairment compared with singly traumatized youth (Schumm et al., 2006; Finkelhor et al., 2007, 2009; Cloitre et al., 2009; Margolin et al., 2009; Shen, 2009; Heim et al., 2010). However, numerous studies highlight the additive effect of child and adolescent multi-type maltreatment on later symptom complexity and psychopathology, including internalizing (Danielson et al., 2005; Schumm et al., 2006; Anda et al., 2007; Sachs-Ericsson et al., 2007; Widom et al., 2007; Ford et al., 2010), externalizing (Brown and Anderson, 1991; Herrenkohl et al., 1997; Finkelhor et al., 2009; Ford et al., 2009, 2010; Shen, 2009), and trauma symptoms (Boney-McCoy and Finkelhor, 1996; Mulder et al., 1998; Schaaf and McCanne, 1998; Finkelhor et al., 2007, 2009; Vranceanu et al., 2007; Shen, 2009; Ford et al., 2010). Following this large amount of studies, it is understandable that trauma may be referred not only as a present-or-absent construct but also includes dimensional aspects, considering the multiplicity of maltreatment forms observed as well as the frequency of traumatic exposure.
Literature on attachment has generated stimulating outcomes regarding early traumatic experiences and how they shape later responses in adulthood, becoming a framework that enables a more sophisticated comprehension of the relational trauma sequelae on mental health (Lyons-Ruth and Jacobvitz, 2008). Occurrence of abuse and neglect in early life may interfere with the development of a healthy secure attachment relationship (Baer and Martinez, 2006). Research findings suggest that traumatized children are at risk for attachment disruption, specifically developing an insecure disorganized attachment pattern (Lyons-Ruth et al., 1987; Carlson et al., 1989; Cicchetti and Barnett, 1991; Beeghly and Cicchetti, 1994; Barnett et al., 1999; van IJzendoorn et al., 1999; Cicchetti et al., 2006; Cyr et al., 2010). Similarly, during the administration of the Adult Attachment Interview (AAI; George et al., 1984; Main et al., 2003), the surfacing of memories of attachment-related traumatic experiences is not rare. In such cases, disorganized attachment pattern is most typically detected in adult respondents with a history of complex trauma (Lyons-Ruth and Jacobvitz, 2008; Bakermans-Kranenburg and van IJzendoorn, 2009; Murphy et al., 2014).
The assessment of complex trauma is by definition “complex,” as it involves both a delineation of a wide range of traumatic events as well as their appraisal, and because these types of experiences rarely occur in isolation and are highly interrelated (Felitti et al., 1998; U.S. Department of Health and Human Services, Administration on Children, Youth, and Families, 2011). Ascertaining the presence and degree of early maltreatment required for clinically based studies and epidemiological research has been enabled by observer-rated interviews and self-report questionnaires, though retrospective reports usually provide underestimates of the trauma incidence (Hardt and Rutter, 2004). Self-reports generally inquire about limited types and generate quantitative rating of trauma, and are unable to detect when defense mechanisms may distort responses (Ravitz et al., 2010). However, this format requires less time to complete and may elicit more disclosure facilitating valid responses to questions on sensitive issues (Newman et al., 1996). Several guided or semi-structured interviews have been developed to measure a broader range of potential trauma areas to reduce response biases (Roy and Perry, 2004), allowing investigators to obtain uniform information in an interpersonal interaction context. Nevertheless, these instruments are usually time-consuming and require administration and scoring by trained investigators.
Given the pervasiveness of the trauma reported and the outcomes that arise, these findings emphasize the vitality of a comprehensive assessment of early trauma history for making appropriate service recommendations and interventions within child and adolescent welfare (Kisiel et al., 2009; Briggs et al., 2013). Despite several measures that have been created to assess the occurrence of childhood trauma, researchers often base assessment tools on a narrowed conceptualization of maltreatment and focus on creating a single or limited abuse types-instrument (Bremner et al., 2007; DiLillo et al., 2010), making it difficult to extend the investigation of the multiple aspects of traumatic experience and to compare the impact of specific forms of trauma. Moreover, most studies use a priori categorical or dimensional descriptions of complex trauma, while only few define polyvictimization empirically using statistical techniques. Lastly, although evidence regarding the nature and frequency of traumatic exposure is significant to research and practice on child maltreatment (Manly et al., 2001; English et al., 2005), many instruments restrict assessment to the occurrence of trauma in a dichotomous (presence vs. absence) classification. In response to these gaps in measurement, this study aimed to develop a retrospective questionnaire concerning early history of interpersonal trauma and to outline its preliminary psychometric characteristics by presenting data which support its reliability and validity. In this paper, the Complex Trauma Questionnaire (ComplexTQ) was particularly applied to AAI transcripts conceived as a stimulus which would enable activation of the attachment system at emotional levels through an intensive series of probes regarding the interviewee's history with the attachment figures (Dozier and Kobak, 1992; Dias et al., 2011; Farina et al., 2014).
Materials and Methods
Development and Features of the Complex Trauma Questionnaire
The Complex Trauma Questionnaire (ComplexTQ) was developed to enable researchers and clinicians to measure adverse childhood experiences displayed in their major forms and frequency of occurrence, to cover multidimensional aspects of complex trauma, including child neglect which represents one of the most widespread forms of maltreatment (Gilbert et al., 2009; U.S. Department of Health and Human Services, Administration on Children, Youth, and Families, 2011), which appears as a deceitful phenomenon and is less easily detectable and assessable compared with active types of abuse.
The ComplexTQ was designed in both clinician and self-report versions1. In this study, the questionnaire is completed by a clinician and is applied to interview transcripts for evaluation of trauma history prior to age 15. Item construction was based on clinical experience and performed following an extensive review of the literature on child abuse and neglect. Clinician responds to a series of specific screener questions that reveal whether the participant experienced a range of caregiver's behaviors encompassing acts of both commission and omission. To capture the intensity of these experiences, clinician provides ratings on a 4-point Likert scale (from 1 = never to 4 = often) reflecting how frequently the episodes occurred, except for the last item concerning the occurrence of significant bereavements (yes/no). Thus, scoring allows detecting presence and severity (sum and mean of frequency scores) of each maltreatment type. Cumulative occurrence across all single forms of traumatic experience is provided through a total score. Given research and theory suggesting that the caregiver gender may be relevant to trauma effects (Schore, 1999; Briere and Rickards, 2007), scores are differentiated between relationship with the mother, that with the father as well as with another significant figure.
Based on the literature on childhood trauma, nine domains of interpersonal maltreatment experiences were considered and operationalized. Items regarding the Neglect domain are intended to measure withdrawal of caretaking and failure to respond and engage in behavior that is necessary to meet the developmental needs of a child, such as physical needs (e.g., providing food, clothing, and medical treatment), supervision and educational needs (e.g., checking on friendship environment and leisure activities, monitoring school attendance, or assisting with homework), and emotional needs (e.g., demonstrating affection, support, and companionship). These conducts attempt to capture the heterogeneity of child neglect, ranging from a caregiver who is unavailable, inattentive, uninvolved, or psychologically inaccessible (e.g., lacking of love expressions) to the one whose acts involve abandonment of the child. Consequently, the child may feel unloved, unnoticed, or invisible to the caregiver. Reject items describe a cold or hostile caregiving (e.g., episodes of child's distress and illness are minimized or ridiculed) as an active turning away of the child's expression of need and attachment. The caregiver seems to prefer the child's absence by acting on feelings of anger, enmity, irritation, bitterness, or resentment. The child may feel disliked, avoided, and unwanted. Items referring to Role reversal behaviors label caregiver who seeks comfort, intimacy, and physical or psychological unmet needs from the child. Child's presence and attention seem essential for the caregiver's sense of welfare. The child is thus expected to take the role of a parent, spouse, or peer toward the caregiver and attempts to reduce his/her distress. Items of Psychological abuse assess verbal and demonstrative acts by the caregiver intended to cause psychological pain or fear, as excessive and repeated ridiculing, blaming, insults, isolation, threats, and coercive attitudes toward the child. The caregiver's intent seems the control or intimidation of the child, and items range from shaming or embarrassing the child to parental alienation syndrome, intrusive and excessive medical care, or emotional cruelties (e.g., threat to hurt the child or the child's loved one or to force him/her to violate the law). Questions regarding Physical abuse inquire about the occurrence of physically aggressive behaviors (e.g., hitting, grabbing, knocking down, beating with an object, tying, and burning), resulting injuries (e.g., cuts, bruises, broken bones, and burns), and medical treatment needed. Supplementary queries probe regarding the nonabusive caregiver's responses to maltreatment perpetrated by other household members (e.g., defending, reassuring, and comforting the child). The Sexual abuse domain includes any sexual intercourse that involves (e.g., inappropriate touching, kissing, fondling, and penetration) or does not involve (e.g., voyeurism, exposure to erotic language, and participation in pornographic activities) physical contact. In addition, items explore if the participant has been threatened not to recount, if the caregiver did not believe the report, or failed to comfort and protect the child from abuse. Items regarding the Witnessing domestic violence area describe verbal/emotional abuse and aggressive behaviors that occur between parents to which the child is exposed. Finally, significant Separations and Losses up to age 14 are explored.
Participants
The study has been conducted among 229 individuals, including participants at high-risk and with psychiatric diagnoses (dissociative disorders, N = 14; parents of maltreated children, N = 53; gender identity disorder in the procedure of sex reassignment surgery, N = 41; personality disorders, N = 42), and a nonclinical sample (N = 79). Subjects were recruited from clinical centers in Rome (Italy) and took part in different research projects (Mirizio et al., 2011; Farina et al., 2014; Speranza and Maggiora Vergano, 2015; Lingiardi et al., submitted). Although important differences characterize participants within the clinical/at-risk sample, we decided to combine those groups due to their history of trauma exposure as suggested by literature. Indeed, several studies highlighted early trauma in dissociative patients (Dutra et al., 2009; Schmahl et al., 2010), parents of maltreated children (Dixon et al., 2005a,b, 2009), participants with gender identity disorder (Kersting et al., 2003; Gehring and Knudson, 2005; Veale et al., 2010), and those with personality disorders (Afifi et al., 2011). The combined clinical/at-risk sample (N = 150) was composed of 37 men, 72 women, 27 male-to-female and 15 female-to-male transsexuals, ranging from 16 to 62 years of age (M = 30.44; SD = 11.24), and mostly Italians (94%). The majority of nonclinical participants were females (82%) and Italian (99%) with the mean age of 31.87 years (SD = 5.76) and age range of 25–65 years. The nonclinical participants were recruited from previous longitudinal studies regarding the quality of parenting (Ammaniti et al., 2005, 2006), representing the control group which had no depressive or psychosocial risks.
The overall sample was recruited from different research studies expressively asking for a participation secured through a written informed consent procedure that required active consent from participants. The current study has been attended within the Ph.D. context at the Department of Dynamic and Clinical Psychology (Faculty of Medicine and Psychology, Sapienza University of Rome) and received the approval from the Ethical Committee of the Department.
Instruments
Adult Attachment Interview
Adult Attachment Interview (AAI; George et al., 1984; Main et al., 2003). The AAI is a semi-structured interview, an hour-long protocol, which explores adult's mental representations of attachment while discussing childhood experiences. After an overview of the family composition, respondents are asked to describe their early relationship with each parent, supplying five adjectives to be supported by providing specific descriptive incidents. Interviewees are additionally probed regarding situations of distress (e.g., emotionally upset, hurt, or ill), and instances of threat or abuse. Following questions concern reaction to separations from the caregiver and significant losses. Two types of variables are rated on 9-point Likert scales. Narratives of parent–child relationships are coded on scales for “probable childhood experiences” which describe rejecting, involving/role reversing, neglecting when present, pressuring to achieve, and loving behaviors of each attachment figure. Likewise, “present state of mind” with respect to attachment is rated on scales defining idealization of parents, dismissing derogation of attachment figures or relationships, insistence on lack of recall, fear of loss of the child, passivity or vagueness in discourse, current involving/preoccupying anger toward caregivers, metacognitive monitoring, coherence of transcript, and overall coherence of mind. AAI scoring system is based on the participant's ability to produce coherent narratives regarding childhood experiences with caregivers, thus classifying interviewee as Secure/Autonomous (F), Dismissing (Ds), Preoccupied with respect to attachment (E), or “Cannot classify” category (CC) when a global breakdown in the organization of discourse arises. An interview may also be assigned an Unresolved/disorganized state of mind (Ud) concerning past abuse or loss in association with a best-fitting primary classification. Psychometric testing and meta-analyses have provided evidence of stability and discriminant and predictive validity of the AAI in both clinical and nonclinical populations (Bakermans-Kranenburg and van IJzendoorn, 1993, 2009; Sagi et al., 1994; van IJzendoorn, 1995; Roisman et al., 2007; Hesse, 2008; van IJzendoorn and Bakermans-Kranenburg, 2008). Each Adult Attachment Interview was conducted by researchers trained by A.M. Speranza to administer the AAI, recorded and transcribed verbatim. The interviews were classified using Main et al. (2003) coding system2 by the first and the third author who are certified AAI coders. A hundred and thirty-five transcripts (59%) were double-coded, blind to subject conditions: percent agreement for the 4-way classification (F, Ds, E, Ud/CC) was 81% (k = 0.77). When there was disagreement, a third independent coder also categorized the transcript, with final agreement reached after discussion by all three coders.
Complex Trauma Questionnaire
Complex Trauma Questionnaire (ComplexTQ). The ComplexTQ is a 70-item scale for the retrospective assessment of multi-type maltreatment, measuring lack of care (physical and emotional neglect), abuse (psychological, physical, and sexual abuse), and other traumatic experiences, such as rejection, role reversal, exposure to domestic violence, separations, and losses. The instrument is available in two different versions, clinician and self-report. The questionnaire assesses adverse experiences from childhood to usage of 14 years separately involving maternal, paternal, and other attachment figures. The clinician version, compiled by the first and the third author, requires approximately 15–20 min to complete (depending on the length of the interview's transcript) and scores for presence and frequency of traumatic experiences in each domain are automatically provided by the software.
Statistical Analyses
Inter-rater Reliability
Although the data used in the present study were collected by a single rater who evaluated all transcripts, we conducted a preliminary analysis aimed to test rater's ability to code data. This analysis was based on a pilot study of 54 participants later included in this study, each evaluated by the first and the third author of the manuscript, blind to each other, using the complete 70-item set. The inter-rater reliability for ComplexTQ ratings was assessed based on the Intraclass Correlation Coefficient (ICC), a measure of similarity of ComplexTQ ratings made by independent coders. The analysis yielded good inter-rater reliability for the 70 items (ICC-s = 0.85 and 0.89 for items concerning mother and father, respectively) as well as for the items retained after factor analysis (ICC-s = 0.81 and 0.87 for items concerning mother and father, respectively).
Factor Analysis
Polychoric Correlations
A preliminary descriptive analyses of ComplexTQ items revealed that 27 and 30 items, for patients' traumatic experience with mother and father, respectively, had near zero variance in the samples studied. These items were excluded from the analyses that were completed on 40 and 37 items. However, the retained items not only were ordered categorical variables but the inspection of the item response pattern also revealed in most cases an asymmetric response distribution. Standard factor analysis assumes a multivariate normal distribution and item distributions that approach an equal intervals scale. As both the assumptions were violated, we analyzed the polychoric correlation matrix, instead of the standard Pearson's correlation matrix. This procedure is strongly recommended for ordered categorical items from two to five response categories (Panter et al., 1997; Holgado-Tello et al., 2008; Timmerman and Lorenzo-Seva, 2011; Garrido et al., 2013). Specifically, a polychoric correlation is based on the assumption that each of the ordered categorical items represents an approximation of an underlying continuous variable. Accordingly, the computational procedure estimates what would be the correlation between these underlying variables based on the collected empirical approximation. An unweighted least square factor analysis with promax rotation was conducted by Factor 9.3 (Lorenzo-Seva and Ferrando, 2006). The Kaiser–Meyer–Olkin measure of sampling adequacy attained a fairly high value for both mother and father datasets (KMO = 0.72 and 0.80, respectively), thus showing that the sample correlation matrix was appropriate for factor analysis to proceed.
Factor retention criteria
Despite there being no “gold standard” for determining the “true” number of factors to retain in exploratory factor analysis, we integrated the scree-plot with information from Minimum Average Partial (MAP) and Parallel Analysis (PA), which are considered the most accurate diagnostics (Ruscio and Roche, 2012). The MAP test is based on a series of factor analyses, each followed up by a quantitative assessment of partial correlations. Specifically, as the first step, a factor analysis is performed and the first factor is partialed out of the correlation matrix among questionnaire items. Then, the squared off-diagonals partial correlations are averaged to obtain a summary index of the variance in the correlation matrix that is due to systematic sources. As the second step, both first and second extracted factors are partialed out and again the squared off-diagonals partial correlations are averaged, and this procedure is repeated up to k-1 factors are partialed out. The MAP test lines up the average squared partial correlation indexes obtained on each step, and the minimum value is considered as indication of the appropriate number of factors in the dataset. PA is based on comparing eigenvalues resulting from a factor analysis of real data to those resulting from a Monte Carlo simulation study. Specifically, repeated factor analyses are performed on a large number of randomly generated data matrices (e.g., 1000) that are parallel to the real data (i.e., have the same number of variables and cases). Factors whose eigenvalues are greater than the average random ones are deemed as reflecting systematic sources and therefore, retained as meaningful psychological dimensions (for a recent review of factor retention criteria see Courtney, 2013).
ROC Curve Analysis
The clinical validity of the ComplexTQ was assessed by plotting the performance of each factor's derived scale score as a classifier of clinical vs. nonclinical group membership (see participants). A Receiver Operating Characteristic (ROC) curve analysis of these plots was performed by SPSS 23 to determine the optimal threshold for ComplexTQ. On each analysis, the “true positive” rate at different threshold is plotted against the “false positive” rate and the resulting curve connecting data points was drawn. The area under the curve (AUC) is a measure of the scale score classification accuracy, and its statistical significance supports clinical validity.
Convergent Validity
The transcripts were also coded through AAI scales for inferred experiences in infancy with mother and father. Convergent validity of ComplexTQ scales was then assessed as correlation coefficients with AAI scales.
Results
Factor Analysis
The analysis of ComplexTQ items yielded 16 and 15 eigenvalues that were greater than one for mother and father datasets, respectively. Regarding mother dataset, the scree-plot showed three major drops in eigenvalue size after the third, the sixth, and the eighth eigenvalue. The MAP test suggested two factors to be retained, while the PA criterion indicated six factors. Regarding father dataset, the scree-plot showed two major drops in eigenvalue size after the second and the fifth eigenvalue. The MAP test suggested three factors to be retained, while the PA criterion indicated five factors. Thus, there is agreement between scree-plot and PA on six and five factors for mother and father, respectively. Besides that, the six- and five-factor solutions also had a better fit than solutions based on a smaller number of factors (GFI-s = 0.94 and 0.95 for mother and father datasets, respectively).
The mother dataset showed the following factors accounting for 49% of the variance in trauma experience (see Table 1). (F1) Role Reversal loaded on eight items evaluating the extent to which the mother placed herself in the center of child's attention, involving the child in her physical and/or psychological care, or making the child feel responsible for her own wellbeing. Moreover, other items inform about situations of domestic conflict and violence witnessed by the child. (F2) Physical Abuse loaded on seven items describing forms of maltreatment and physical abuse perpetrated by the mother. Furthermore, the caregiver tended to deride or get angry at the child's signals of attachment needs, arousing child's fear and worries. (F3) Psychological Abuse/Rejection loaded on eight items assessing rejection and avoidance of the child, especially child's expression of affection, attention, dependence, and attachment. The mother's abuse and aversion, exhibited through criticism, insults, or humiliations, made the child feel unwanted and disliked. (F4) Emotional Neglect loaded on seven items describing indifference, inattention, or psychological unavailability to the child's emotional needs. It includes failure to provide nurturance or companionship within child–caregiver relationship and lack of emotional support to the child when expecting comfort and reassurance. Therefore, the child may not rely upon the mother for sharing difficult or painful experiences. (F5) Failure of Protection loaded on three items regarding a parent who abdicated the role of caregiving, by failing to defend and reassure the child in abusive situations perpetrated by other caretaking figures. (F6) Material Neglect loaded on seven items considering physical neglect (e.g., failure to provide adequate food, clothing, shelter, and medical care), educational neglect (e.g., failure to ensure proper education and learning opportunities), and supervisory/social neglect (e.g., unawareness/inattention to child's whereabouts and socializing).
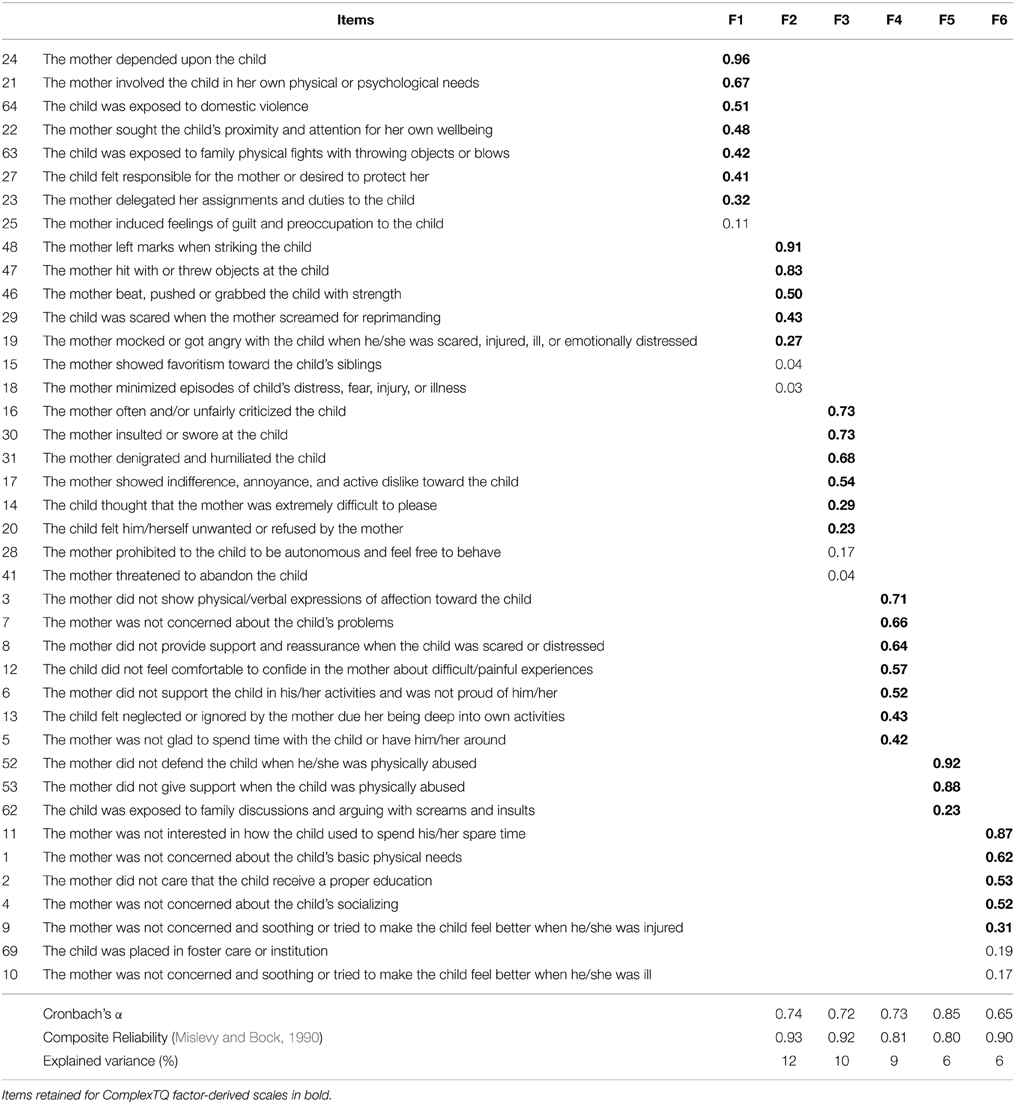
Table 1. Six-factor model of ComplexTQ items for the mother.
The father dataset showed similar factors that emerged, accounting for 51% of the variance in trauma experience (see Table 2). Unlike the mother dataset, no role-reversal factor was identified, the factor ordering was different and the factors loaded on different number of items but preserved the original meaning: (F1) Emotional Neglect (9 items), (F2) Failure of Protection (3 items), (F3) Material Neglect (7 items), (F4) Psychological Abuse/Rejection (7 items), and (F5) Physical Abuse (11 items).
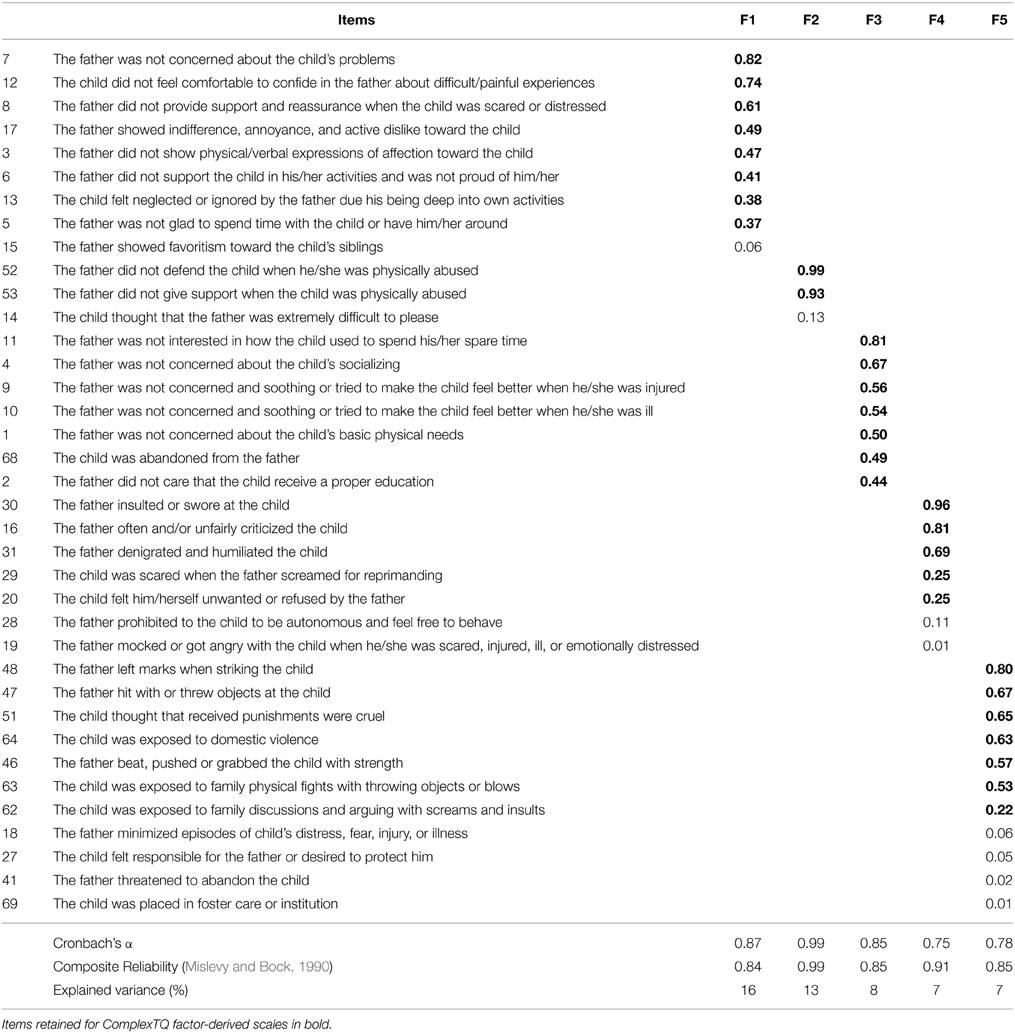
Table 2. Five-factor model of ComplexTQ items for the father.
ComplexTQ Factor-derived Scales
Factor markers with factor loadings greater than 0.20 were selected based on inspection of the factor loading matrix. Our aim was to retain most representative items for each factor and to discard items that failed to load any factors. Then, selected items were resubmitted to factor analysis to verify whether item selection biased factor interpretation. Since no substantial changes in factor labeling and content emerged, ComplexTQ factor-derived scales were based on 33 and 29 items respectively for mother and father datasets (reported in bold font on Tables 1, 2).
ROC Curves
As one can see from Table 3, ComplexTQ factor-derived scales were used as predictors of group membership and discriminant properties were assessed as AUC-s. For mother and father data, ComplexTQ scores were significantly different for clinical and nonclinical participants. In particular, fairly high AUC values were found for the Emotional Neglect scale for both the mother and the father, while Material Neglect attained the fair AUC threshold for father only. It is worth noting that AUC values for the total scores approached the standard for good diagnostic accuracy.
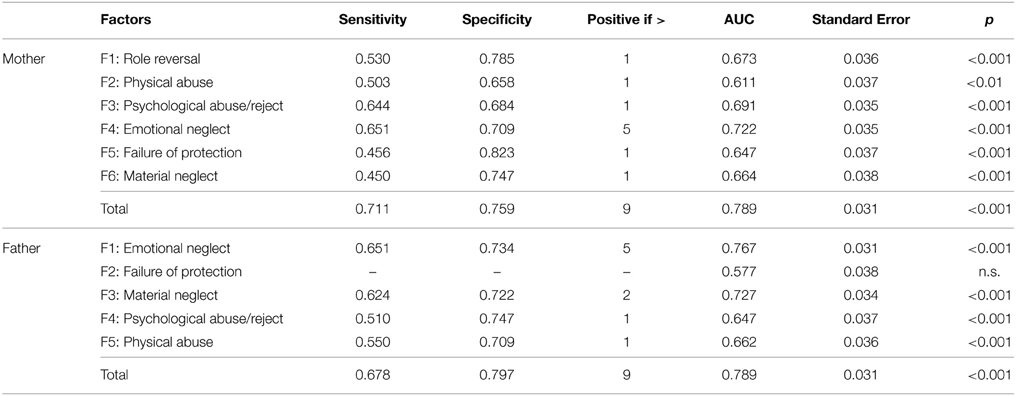
Table 3. Analysis of ROC curves to assess diagnostic accuracy for ComplexTQ factor-derived scales and total scores.
Convergent Validity
As shown in Table 4, the mother's ComplexTQ factors were correlated with AAI scales for inferred experiences. AAI “Pressure to achieve” probable experience scale was omitted as no correlations were found with ComplexTQ factor-derived scales. We reviewed correlation coefficients following Cohen's (1988) “rule of thumb.” There was a very large overlapping between ComplexTQ Role Reversal factor and AAI Involving/role reversing scale. Physical Abuse factor showed a medium-large correlation with AAI Rejecting scale. Psychological Abuse factor showed a large and small-medium correlation with AAI Rejecting and Neglecting scales, respectively. Emotional Neglect factor showed a very large correlation with AAI Neglecting and Rejecting scales. Failure of Protection factor showed a small-medium correlation with AAI Rejecting and Neglecting scales. Material Neglect showed a large correlation with AAI Rejecting and Neglecting scales. It is noteworthy that all ComplexTQ factors were negatively associated with the AAI Loving scale, although the effect size varied from small (Role Reversal) to very large (Emotional Neglect).
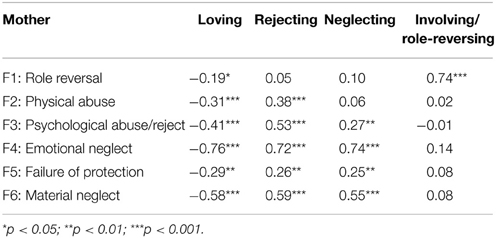
Table 4. Correlations with AAI scales for inferred experiences with mother.
The father's ComplexTQ factors (see Table 5) had similar correlation patterns as mother for Neglect and Psychological Abuse factors. Instead, Failure of Protection factor was significant only with AAI Rejecting scale showing a small effect size, and Physical Abuse factor was medium-large with both AAI Neglecting and Rejecting scales. All ComplexTQ factors were negatively associated with the AAI Loving scale.
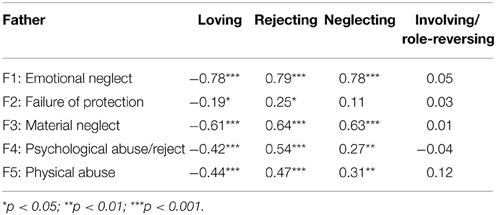
Table 5. Correlations with AAI scales for inferred experiences with father.
Discussion
In response to the need for psychometrically based trauma instruments, this study describes the development and the preliminary psychometric properties of the ComplexTQ, confirming satisfactory reliability and validity of the measure.
This study mainly aimed to evaluate the validity of the ComplexTQ. Multiple trauma dimensions were validated through factor analysis, which provided coherent outcomes for both mother and father ratings. Dealing with a priori developed ComplexTQ scales, Neglect subscale was divided into a material form—reflecting physical, educational, and supervisory/social negligence—and the caregiver's unavailability or inattention which mainly involves emotional level. In this regard, several studies highlighted the need for an articulated conceptualization of neglect due to the heterogeneity of the phenomenon (e.g., Dubowitz et al., 1993; Slack et al., 2003), since they observed different consequences on child's well-being and different approaches to primary prevention and treatment with respect to the form in which neglect is declined (Straus and Kaufman Kantor, 2005). Despite the need of a comprehensive definition and assessment, the choice of splitting neglect in different dimensions has been noticed in few childhood trauma measures, as the Childhood Trauma Questionnaire (CTQ; Bernstein et al., 1994), the Interview for Traumatic Events in Childhood (ITEC; Lobbestael et al., 2009), the questionnaire used in the Adverse Childhood Experiences Study (Felitti et al., 1998), or the Multidimensional Neglectful Behavior Scale (MNBS; Straus et al., 1995). Conversely, Rejection and Psychological Abuse aspects converged into a single factor, therefore associating caregiver's cold and hostile attitude to manifestations of abuse which cause psychological suffering and fear with the intent to control and intimidate the child. This process of inclusion also arose between Role Reversal and Witnessing Domestic Violence items concerning early experiences with the mother. In this matter, it is interesting to underline that the child's exposure to conflicts and violent episodes that occurred within the family were used to represent a form of psychological abuse. Only recently, it has been recognized as a type of maltreatment (Higgins, 2004). Due to the emerged outcomes of this study, we can speculate that deep in an intra-familiar violent climate—in which the father often constitutes the abusing figure—the child may feel responsible for and involved in the physical or psychological care of the caregiver who is subjected to aggressions. Effects of exposure to domestic violence, reflected on the child's desire to comfort and protect the mother, seems to endure even when episodes of abuse end (Macfie et al., 2008). In a similar vein, it has not been pinpointed a factor including aspects of Role Reversal in relation to childhood experience with the father. Moreover, referring to early relationship with both the caregivers, factor analysis did not identify a Sexual Abuse factor. This result is presumably due to the lack of frequency of sexual abuse episodes in the analyzed reports. Based on our data, we may not exclude that sexual abuse is important to assess, but rather it is underrepresented as an early traumatic experience in participants of this study. Finally, a substantial development of our investigation consisted of an emergent new factor, defined as Failure of Protection of the child, which mainly arises when physical abuse perpetrated by another caregiver occurs. This factor identification is in accordance with the context described by George and Solomon (1996); George and Solomon (2008), referring to a mother who psychologically abdicates her caregiving role whenever the child shows attachment needs. Therefore, it is reasonable to believe that many of the psychological maltreatment correlates are not an exclusive effect of the traumatic experiences occurrence, but rather are a consequence of the impact of caregiver's inadequate dealing with his/her relationship with the child and affect regulation needs.
The ComplexTQ's multifactorial structure has the advantage to cover a wide range of traumatic experiences occurred in early attachment relationships, including aspects of neglect that have been for a long time poorly considered by child abuse research—“The Neglect of Neglect” (Wolock and Horowitz, 1984; Dubowitz, 1994, 2007; Kaplan et al., 1999; Stoltenborgh et al., 2013). Therefore, ComplexTQ enables identifying and assessing multifaceted aspects of trauma in early life, thereby grasping a dysfunctional and disorganized emotional climate rather than focusing on single or non-relational adverse experiences and on a specific dimension of trauma. An accurate identification of multiple traumatic forms appears to be essential, even at a prevention level, considering the consequences in terms of intergenerational transmission of trauma and developmental trajectories, in which scientific literature underlines the transversal nature of trauma as a risk factor for later psychopathology. Research on therapeutic treatment of maltreated children has not yet highlighted a distinction for complex trauma victims, which would allow establishing a different response to focused intervention for the co-occurrence of cumulative traumatic experiences (Harvey and Taylor, 2010; Ford et al., 2012). Studies comprising adult population suggest a adjustment oriented therapeutic process using the results of early exposure to multiple traumas (Ford and Kidd, 1998; Nemeroff et al., 2003).
Concerning the diagnostic accuracy, ComplexTQ total scores discriminated clinical/at-risk vs. nonclinical participants, thus being a valid measure to evaluate traumatic experiences occurred in early attachment relationships. This aspect seems to be particularly relevant, since different studies emphasized the utility of some instruments (e.g., CTQ and ACE Questionnaire) in evaluating high levels of early trauma exposure and in associating them to a major risk of developing a later psychopathology (Teicher and Parigger, 2015).
Regarding correlation with AAI scales for inferred experiences, except Role Reversal and Failure to Protection, factor-derived ComplexTQ scales deal with same aspects of rejecting and neglecting, providing a more articulated vision and, therefore, converging with the latest scientific studies which recognize multifaceted expressions of constructs (e.g., Hart et al., 2002; Dubowitz et al., 2005; Baker, 2009). Moreover, all factors were negatively associated with the AAI Loving scale, which describes an active process of caregiver's involvement, support, and nurturance with respect to the child. Similar to active forms of maltreatment, lack of emotional support from caregivers has been associated with externalizing and internalizing symptoms across life span (McCarty et al., 2004; Shaw et al., 2004).
Limitations and Final Remarks
The limitations of the study displayed future directions for the confirmatory validation and use of the ComplexTQ. The present study outcomes are based on a factor analysis that needs additional confirmation with an independent and wider sample. A larger sample is also required to unable an invariance analysis by gender in the relationship with both caregivers. Since this is a preliminary study, all 70 items in the current version should be retained, and choice to exclude the less representative items from scales should be delayed till future analyses. A second limitation concerns the absence of convergence with an independent retrospective measure of childhood trauma, which could therefore better verify ComplexTQ's construct validity. The intraclass correlation assessed on 54 questionnaires may represent another limitation, although it is not unusual that the inter-rater reliability is tested on a subset of participants to be generalized to the full sample (see Hallgren, 2012). Moreover, among the different parameters used to quantify the traumas, ComplexTQ does not inquire about other aspects, such as age at the onset and the duration of traumatic experiences, which seem to have an impact on later psychopathology (Bifulco et al., 2002; Roy and Perry, 2004; English et al., 2005). Finally, diagnostic accuracy has been verified comparing clinical/at-risk and nonclinical participants, therefore not disclosing if ComplexTQ factors could be useful to discriminate different types of psychopathology. To present the state of affairs, we can consider ComplexTQ scores only as trans-diagnostic indicators, hence related to several aspects of psychopathology.
The ComplexTQ clinician report version has been applied to AAI transcripts, a protocol which represents an emotional stimulus able to activate attachment system and conceived by the authors as an attempt to “surprise the unconscious” (Main, 1991, p. 141). Considering this premise, ComplexTQ offers the facilitation, compared with the AAI-based studies, to use the interview as an instrument that gives specific and detailed information about the presence and severity of trauma in participant history, without requiring training for the reliability to code attachment mental states. Moreover, ComplexTQ enables to distinguish with which attachment figure the participant experienced specific traumatic events. This specificity allows evaluating the influence of other significant figures and, moreover, the different effects of trauma on development due to the relevance of the caregiver's gender regarding later outcomes (Schore, 1999; Briere and Rickards, 2007). In addition to the nature of trauma and the perpetrator's identity, the scoring system also enables to assess the occurrence as well as the frequency of each different type of maltreatment. Finally, the questionnaire is easy to complete and to code, owing to a program specifically created for this research that shows a profile of the child relational history. Unlike most of the studies assessing early interpersonal trauma (Briere et al., 2012), reported results were based on heterogeneous clinical groups and nonclinical sample, permitting more generalizability of findings. Therefore, ComplexTQ is a promising tool for the retrospective measurement of early trauma which can be used for clinical and research purposes and enables to discriminate clinical and nonclinical outcomes, supplying a contribution to the understanding of the link between childhood trauma and psychopathology.
Author Contributions
We state that all authors have participated in the work with a substantial contribution to conception, design, acquisition, analysis and interpretation of data. Moreover, all authors have been involved in drafting the article and approved the final version of the manuscript. Agreement has been accountable for all aspects of the manuscript in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
1 ^The self-report version of ComplexTQ is not presented in this paper.
2 ^C. Maggiora Vergano has been trained to reliability at the AAI Training Institute of Rome, 2010, by D. Jacobvitz and N. Dazzi; A. M. Speranza at the AAI Training Institute of Rome, 1990, by M. Main and E. Hesse; C. Trentini (third coder) at the AAI Training Institute of Rome, 2008, by D. Jacobvitz and N. Dazzi.
References
Afifi, T. O., Mather, A., Boman, J., Fleisher, W., Enns, M. W., MacMillan, H., et al. (2011). Childhood adversity and personality disorders: results from a nationally representative population-based study. J. Psychiatr. Res. 45, 814–822. doi: 10.1016/j.jpsychires.2010.11.008
Ammaniti, M., Speranza, A. M., and Fedele, S. (2005). “Attachment in infancy, early and late childhood: a longitudinal study,” in Attachment in Middle Childhood, eds K. Kerns and R. A. Richardson (New York, NY: Guilford Press), 115–136.
Ammaniti, M., Speranza, A. M., Tambelli, R., Muscetta, S., Lucarelli, L., Vismara, L., et al. (2006). A prevention and promotion intervention program in the field of mother–infant relationship. Infant Ment. Health J. 27, 70–90. doi: 10.1002/imhj.20081
Anda, R. F., Brown, D. W., Felitti, V. J., Bremner, J. D., Dube, S. R., and Giles, W. H. (2007). Adverse childhood experiences and prescribed psychotropic medications in adults. Am. J. Prev. Med. 32, 389–394. doi: 10.1016/j.amepre.2007.01.005
Arata, C. M., Langhinrichsen-Rohling, J., Bowers, D., and O'Brien, N. (2007). Differential correlates of multi-type maltreatment among urban youth. Child Abuse Negl. 31, 393–415. doi: 10.1016/j.chiabu.2006.09.006
Baer, J. C., and Martinez, C. D. (2006). Child maltreatment and insecure attachment: a meta-analysis. J. Reprod. Infant Psychol. 24, 187–197. doi: 10.1080/02646830600821231
Baker, A. J. L. (2009). Adult recall of childhood psychological maltreatment: definitional strategies and challenges. Child. Youth Serv. Rev. 31, 703–714. doi: 10.1016/j.childyouth.2009.03.001
Bakermans-Kranenburg, M. J., and van IJzendoorn, M. H. (1993). A psychometric study of the Adult Attachment Interview: reliability and discriminant validity. Dev. Psychol. 29, 870–879. doi: 10.1037/0012-1649.29.5.870
Bakermans-Kranenburg, M. J., and van IJzendoorn, M. H. (2009). The first 10,000 adult attachment interviews: distributions of adult attachment representations in clinical and non-clinical groups. Attach. Hum. Dev. 11, 223–263. doi: 10.1080/14616730902814762
Barnett, D., Ganiban, J., and Cicchetti, D. (1999). Maltreatment, negative expressivity, and the development of type D attachments from 12 to 24 months of age. Monogr. Soc. Res. Child Dev. 64, 97–118. doi: 10.1111/1540-5834.00035
Beeghly, M., and Cicchetti, D. (1994). Child maltreatment, attachment, and the self system: emergence of an internal state lexicon in toddlers at high social risk. Dev. Psychopathol. 6, 5–30. doi: 10.1017/S095457940000585X
Bernstein, D. P., Fink, L., Handlesman, L., Foote, J., Lovejoy, M., Wenzel, K., et al. (1994). Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am. J. Psychiatr. 151, 1132–1136. doi: 10.1176/ajp.151.8.1132
Bifulco, A., Moran, P. M., Baines, R., Bunn, A., and Stanford, K. (2002). Exploring psychological abuse in childhood: II. Association with other abuse and adult clinical depression. Bull. Menninger. Clin. 66, 241–266. doi: 10.1521/bumc.66.3.241.23366
Boney-McCoy, S., and Finkelhor, D. (1996). Is youth victimization related to trauma symptoms and depression after controlling for prior symptoms and family relationships? A longitudinal, prospective study. J. Consult. Clin. Psychol. 64, 1406–1416. doi: 10.1037/0022-006X.64.6.1406
Bremner, J. D., Bolus, R., and Mayer, E. A. (2007). Psychometric properties of the early trauma inventory–self report. J. Nerv. Ment. Dis. 195, 211–218. doi: 10.1097/01.nmd.0000243824.84651.6c
Briere, J., Godbout, N., and Runtz, M. (2012). The Psychological Maltreatment Review (PMR): initial reliability and association with insecure attachment in adults. J. Aggress. Maltreat. Trauma 21, 300–320. doi: 10.1080/10926771.2012.659801
Briere, J., and Rickards, S. (2007). Self-awareness, affect regulation, and relatedness: differential sequels of childhood versus adult victimization experiences. J. Nerv. Ment. Dis. 195, 497–503. doi: 10.1097/NMD.0b013e31803044e2
Briggs, E. C., Fairbank, J. A., Greeson, J. K. P., Layne, C. M., Steinberg, A. M., Amaya-Jackson, L. M., et al. (2013). Links between child and adolescent trauma exposure and service use histories in a national clinic-referred sample. Psychol. Trauma 5, 101–109. doi: 10.1037/a0027312
Brown, G. R., and Anderson, B. (1991). Psychiatric morbidity in adult inpatients with childhood histories of sexual and physical abuse. Am. J. Psychiatry 148, 55–61. doi: 10.1176/ajp.148.1.55
Carlson, V., Cicchetti, D., Barnett, D., and Braunwald, K. (1989). Disorganized/disoriented attachment relationships in maltreated infants. Dev. Psychol. 25, 525–531. doi: 10.1037/0012-1649.25.4.525
Cicchetti, D., and Barnett, D. (1991). Attachment organization in maltreated preschoolers. Dev. Psychopathol. 3, 397–411. doi: 10.1017/S0954579400007598
Cicchetti, D., Rogosch, F. A., and Toth, S. L. (2006). Fostering secure attachment in infants in maltreating families through preventative interventions. Dev. Psychopathol. 18, 623–649. doi: 10.1017/S0954579406060329
Clemmons, J. C., DiLillo, D., Martinez, I. G., DeGue, S., and Jeffcott, M. (2003). Co-occurring forms of child maltreatment and adult adjustment reported by Latina college students. Child Abuse Negl. 27, 751–767. doi: 10.1016/S0145-2134(03)00112-1
Cloitre, M., Stolbach, B. C., Herman, J. L., van der Kolk, B. A., Pynoos, R., Wang, J., et al. (2009). A developmental approach to complex PTSD: childhood and adult cumulative trauma as predictors of symptom complexity. J. Trauma. Stress 22, 399–408. doi: 10.1002/jts.20444
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences, 2nd Edn. Hillsdale, NJ: Erlbaum.
Cook, A., Spinazzola, J., Ford, J., Lanktree, C., Blaustein, M., Cloitre, M., et al. (2005). Complex trauma in children and adolescents. Psychiatr. Ann. 35, 390–398.
Copeland, W. E., Keeler, G., Angold, A., and Costello, E. J. (2007). Traumatic events and posttraumatic stress in childhood. Arch. Gen. Psychiatr. 64, 577–584. doi: 10.1001/archpsyc.64.5.577
Courtney, M. G. R. (2013). Determining the number of factors to retain in EFA: using the SPSS R-Menu v2.0 to make more judicious estimations. Practical Assess. Res. Eval. 18, 1–14.
Courtois, C. A. (2008). Complex trauma, complex reactions: assessment and treatment. Psychol. Trauma S, 86–100. doi: 10.1037/1942-9681.S.1.86
Cyr, C., Euser, E. M., Bakermans-Kranenburg, M. J., and van IJzendoorn, M. H. (2010). Attachment security and disorganization in maltreating and high-risk family: a series of meta-analyses. Dev. Psychopathol. 22, 87–108. doi: 10.1017/S0954579409990289
Danielson, C. K., de Arellano, M. A., Kilpatrick, D. G., Saunders, B. E., and Resnick, H. S. (2005). Child maltreatment in depressed adolescents: differences in symptomatology based on history of abuse. Child Maltreat. 10, 37–48. doi: 10.1177/1077559504271630
Dias, P., Soares, I., Klein, J., Cunha, J. P., and Roisman, G. I. (2011). Autonomic correlates of attachment insecurity in a sample of women with eating disorders. Attach. Hum. Dev. 13, 155–167. doi: 10.1080/14616734.2011.554005
Diaz, A., Simantov, E., and Rickert, V. I. (2002). Effect of abuse on health results of a national survey. Arch. Pediatr. Adolesc. Med. 156, 811–817. doi: 10.1001/archpedi.156.8.811
DiLillo, D., Hayes-Skelton, S. A., Fortier, M. A., Perry, A. R., Evans, S. E., Messman-Moore, T. L., et al. (2010). Development and initial psychometric properties of the Computer Assisted Maltreatment Inventory (CAMI): a comprehensive self-report measure of child maltreatment history. Child Abuse Negl. 34, 305–317. doi: 10.1016/j.chiabu.2009.09.015
Dixon, L., Browne, K., and Hamilton-Giachritsis, C. (2005a). Risk factors of parents abused as children: a mediational analysis of the intergenerational continuity of child maltreatment (Part I). J. Child Psychol. Psychiatr. 46, 47–57. doi: 10.1111/j.1469-7610.2004.00339.x
Dixon, L., Browne, K. D., and Hamilton-Giachritsis, C. (2009). Patterns of risk and protective factors in the intergenerational cycle of maltreatment. J. Family Violence 24, 111–122. doi: 10.1007/s10896-008-9215-2
Dixon, L., Hamilton-Giachritsis, C., and Browne, K. (2005b). Attributions and behaviours of parents abused as children: a mediational analysis of the intergenerational continuity of child maltreatment (Part II). J. Child Psychol. Psychiatr. 46, 58–68. doi: 10.1111/j.1469-7610.2004.00340.x
Dong, M., Anda, R. F., Felitti, V. J., Dube, S. R., Williamson, D. F., Thompson, T. J., et al. (2004). The interrelatedness of multiple forms of childhood abuse, neglect, and household dysfunction. Child Abuse Negl. 28, 771–784. doi: 10.1016/j.chiabu.2004.01.008
Dozier, M., and Kobak, R. R. (1992). Psychophysiology in attachment interviews: converging evidence for deactivating strategies. Child Dev. 63, 1473–1480. doi: 10.2307/1131569
Dubowitz, H. (1994). Neglecting the neglect of neglect. J. Interpers. Violence 9, 556–560. doi: 10.1177/088626094009004010
Dubowitz, H. (2007). Understanding and addressing the “neglect of neglect”: digging into the molehill. Child Abuse Negl. 31, 603–606. doi: 10.1016/j.chiabu.2007.04.002
Dubowitz, H., Black, M., Starr, R. H., and Zuravin, S. (1993). A conceptual definition of child neglect. Crim. Justice Behav. 20, 8–26. doi: 10.1177/0093854893020001003
Dubowitz, H., Pitts, S. C., Litrownik, A. J., Cox, C. E., Runyan, D., and Black, M. M. (2005). Defining child neglect based on child protective services data. Child Abuse Negl. 29, 493–511. doi: 10.1016/j.chiabu.2003.09.024
Dutra, L., Bureau, J. F., Holmes, B., Lyubchik, A., and Lyons-Ruth, K. (2009). Quality of early care and childhood trauma: a prospective study of developmental pathways to dissociation. J. Nerv. Ment. Dis. 197, 383–390. doi: 10.1097/NMD.0b013e3181a653b7
English, D. J., Upadhyaya, M. P., Litrownik, A. J., Marshall, J. M., Runyan, D. K., Graham, J. C., et al. (2005). Maltreatment's wake: the relationship of maltreatment dimensions to child outcomes. Child Abuse Negl. 29, 597–619. doi: 10.1016/j.chiabu.2004.12.008
Farina, B., Speranza, A. M., Dittoni, S., Gnoni, V., Trentini, C., Vergano, C. M., et al. (2014). Memories of attachment hamper EEG in cortical connectivity dissociative patients. Eur. Arch. Psychiatry Clin. Neurosci. 264, 449–458. doi: 10.1007/s00406-013-0461-9
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., et al. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 14, 245–258. doi: 10.1016/S0749-3797(98)00017-8
Finkelhor, D., Ormrod, R. K., and Turner, H. A. (2007). Poly-victimization: a neglected component in child victimization. Child Abuse Negl. 31, 7–26. doi: 10.1016/j.chiabu.2006.06.008
Finkelhor, D., Ormrod, R. K., and Turner, H. A. (2009). Lifetime assessment of poly-victimization in a national sample of children and youth. Child Abuse Negl. 33, 403–411. doi: 10.1016/j.chiabu.2008.09.012
Ford, J. D., Connor, D. F., and Hawke, J. (2009). Complex trauma among psychiatrically impaired children. J. Clin. Psychiatr. 70, 1155–1163. doi: 10.4088/JCP.08m04783
Ford, J. D., Elhai, J. D., Connor, D. F., and Frueh, B. C. (2010). Poly-victimization and risk of posttraumatic, depressive, and substance use disorders and involvement in delinquency in a national sample of adolescents. J. Adolesc. Health 46, 545–552. doi: 10.1016/j.jadohealth.2009.11.212
Ford, J. D., and Kidd, P. (1998). Early childhood trauma and disorders of extreme stress as predictors of treatment outcome with chronic post-traumatic stress disorder. J. Trauma. Stress 11, 743–761. doi: 10.1023/A:1024497400891
Ford, J. D., Steinberg, K. L., Hawke, J., Levine, J., and Zhang, W. (2012). Randomized trial comparison of emotion regulation and relational psychotherapies for PTSD with girls involved in delinquency. J. Clin. Child Adolesc. Psychol. 41, 27–37. doi: 10.1080/15374416.2012.632343
Garrido, L. E., Abad, F. J., and Ponsoda, V. (2013). A new look at Horn's parallel analysis with ordinal variables. Psychol. Methods 18, 454–474. doi: 10.1037/a0030005
Gehring, D., and Knudson, G. (2005). Prevalence of childhood trauma in a clinical population of transsexual people. Int. J. Transgend 8, 23–30. doi: 10.1300/J485v08n01_03
George, C., Kaplan, N., and Main, M. (1984). Adult Attachment Interview. Berkeley, CA: University of California.
George, C., and Solomon, J. (1996). Representational models of relationships: links between caregiving and attachment. Infant Ment. Health J. 17, 198–216. doi: 10.1002/(SICI)1097-0355(199623)17:3%3C198::AID-IMHJ2%3E3.0.CO;2-L
George, C., and Solomon, J. (2008). “The caregiving system: a behavioral systems approach to parenting,” in Handbook of Attachment: Theory, Research, and Clinical Applications, 2nd Edn., eds J. Cassidy, and P. H. Shaver (New York, NY: Guilford Press), 833–856.
Gilbert, R., Widom, C. S., Browne, K., Fergusson, D., Webb, E., and Janson, S. (2009). Burden and consequences of child maltreatment in high-income countries. Lancet 373, 68–81. doi: 10.1016/S0140-6736(08)61706-7
Greeson, J. K. P., Briggs, E. C., Kisiel, C. L., Layne, C. M., Ake, G. S. III., Ko, S. J., et al. (2011). Complex trauma and mental health in children and adolescents placed in foster care: findings from the National Child Traumatic Stress Network. Child Welfare 90, 91–108.
Hallgren, K. A. (2012). Computing inter-rater reliability for observational data: an overview and tutorial. Tutor. Quant. Methods Psychol. 8, 23–34.
Hardt, J., and Rutter, M. (2004). Validity of adult retrospective reports of adverse childhood experiences: review of the evidence. J. Child Psychol. Psychiatr. 45, 260–273. doi: 10.1111/j.1469-7610.2004.00218.x
Hart, S. N., Brassard, M., Binggeli, N., and Davidson, H. (2002). “Psychological maltreatment,” in The APSAC Handbook on Child Maltreatment, eds J. Myers, L. Berliner, J. Briere, C. T. Hendrix, C. Jenny, and T. A. Reid (Thousand Oaks, CA: Sage), 79–103.
Harvey, S. T., and Taylor, J. E. (2010). A meta-analysis of the effects of psychotherapy with sexually abused children and adolescents. Clin. Psychol. Rev. 30, 517–535. doi: 10.1016/j.cpr.2010.03.006
Heim, C., Shugart, M., Craighead, W. E., and Nemeroff, C. B. (2010). Neurobiological and psychiatric consequences of child abuse and neglect. Dev. Psychobiol. 52, 671–690. doi: 10.1002/dev.20494
Herrenkohl, R. C., Egolf, B. P., and Herrenkohl, E. C. (1997). Preschool antecedents of adolescent assaultive behavior: a longitudinal study. Am. J. Orthopsychiatry 67, 422–432. doi: 10.1037/h0080244
Hesse, E. (2008). “The adult attachment interview: protocol, method of analysis, and empirical studies,” in Handbook of Attachment, eds J. Cassidy and P. R. Shaver (New York, NY: Guilford Press), 552–598.
Higgins, D. J. (2004). Differentiating between child maltreatment experiences. Fam. Matters 69, 50–55.
Higgins, D. J., and McCabe, M. P. (2001). Multiple forms of child abuse and neglect: adult retrospective reports. Aggress. Violent Beh. 6, 547–578. doi: 10.1016/S1359-1789(00)00030-6
Holgado-Tello, F. P., Chacón-Moscoso, S., Barbero-García, I., and Vila-Abad, E. (2008). Polychoric versus Pearson correlations in exploratory and confirmatory factor analysis of ordinal variables. Qual. Quant. 44, 153–156. doi: 10.1007/s11135-008-9190-y
Kaplan, S. J., Pelcovitz, D., and Labruna, V. (1999). Child and adolescent abuse and neglect research: a review of the past 10 years. Part 1: physical and emotional abuse and neglect. J. Am. Acad. Child Adolesc. Psychiatr. 38, 1214–1222. doi: 10.1097/00004583-199910000-00009
Kersting, A., Reutemann, M., Gast, U., Ohrmann, P., Suslow, T., Michael, N., et al. (2003). Dissociative disorders and traumatic childhood experiences in transsexuals. J. Nerv. Ment. Dis. 191, 182–189. doi: 10.1097/01.NMD.0000054932.22929.5D
Kessler, R. C. (2000). Posttraumatic stress disorder: the burden to the individual and to society. J. Clin. Psychiatr. 61, 4–14.
Kisiel, C. L., Fehrenbach, T., Small, L., and Lyons, J. (2009). Assessment of complex trauma exposure, responses, and service needs among children and adolescents in child welfare. J. Child Adolesc. Trauma 2, 143–160. doi: 10.1080/19361520903120467
Lobbestael, J., Arntz, A., Harkema-Schouten, P., and Bernstein, D. (2009). Development and psychometric evaluation of a new assessment method for childhood maltreatment experiences: the interview for traumatic events in childhood (ITEC). Child Abuse Negl. 33, 505–517. doi: 10.1016/j.chiabu.2009.03.002
Lorenzo-Seva, U., and Ferrando, P. J. (2006). FACTOR: a computer program to fit the exploratory factor analysis model. Behav. Res. Meth. 38, 88–91. doi: 10.3758/BF03192753
Lyons-Ruth, K., Connell, D., Zoll, D., and Stahl, J. (1987). Infants at social risk: relations among infant maltreatment, maternal behavior, and infant attachment behavior. Dev. Psychopathol. 23, 223–232. doi: 10.1037/0012-1649.23.2.223
Lyons-Ruth, K., and Jacobvitz, D. (2008). “Attachment disorganization: genetic factors, parenting contexts, and developmental transformation from infancy to adulthood,” in Handbook of Attachment: Theory, Research, and Clinical Applications, 2nd Edn., eds J. Cassidy and P. H. Shaver (New York, NY: Guilford Press), 666–697.
Macfie, J., Houts, R. M., Pressel, A. S., and Cox, M. J. (2008). Pathways from infant exposure to marital conflict to parent-toddler role reversal. Infant Ment. Health J. 29, 297–319. doi: 10.1002/imhj.20181
Main, M. (1991). “Metacognitive knowledge, metacognitive monitoring, and singular (coherent) vs. multiple (incoherent) model of attachment,” in Attachment Across Life Cycle, eds C. M. Parkes, J. Stevenson-Hinde, and P. Marris (London: Routledge), 127–159.
Main, M., Goldwyn, R., and Hesse, E. (2003). Adult Attachment Scoring and Classification System (Version 7.2). Berkeley, CA: University of California.
Manly, J. T., Kim, J. E., Rogosch, F. A., and Cicchetti, D. (2001). Dimensions of child maltreatment and children's adjustment: contributions of developmental timing and subtype. Dev. Psychopathol. 13, 759–782.
Margolin, G., Vickerman, K. A., Ramos, M. C., Serrano, S. D., Gordis, E. B., Iturralde, E., et al. (2009). Youth exposed to violence: stability, co-occurrence, and context. Clin. Child Fam. Psychol. Rev. 12, 39–54. doi: 10.1007/s10567-009-0040-9
McCarty, C. A., Zimmerman, F. J., Digiuseppe, D. L., and Christakis, D. A. (2004). Parental emotional support and subsequent internalizing and externalizing problems among children. J. Dev. Behav. Pediatr. 26, 267–275. doi: 10.1097/00004703-200508000-00002
Mirizio, V., Lombardi, F., Luoni, G., Ciolfi, F., Fenu, M. A., Fuortes, G., et al. (2011). Regolazione affettiva e psicopatologia nei giovani adulti: una ricerca clinica. Infanzia e Adolescenza 10, 71–86.
Mislevy, R. J., and Bock, R. D. (1990). BILOG 3 Item Analysis and Test Scoring with Binary Logistic Models. Mooresville, NC: Scientific Software.
Mulder, R. T., Beautrais, A. L., Joyce, P. R., and Fergusson, D. M. (1998). Relationship between dissociation, childhood sexual abuse, childhood physical abuse, and mental illness in a general population sample. Am. J. Psychiatr. 155, 806–811.
Mullen, P. E., Martin, J. L., Anderson, J. C., Romans, S. E., and Herbison, G. P. (1996). The long-term impact of the physical, emotional, and sexual abuse of children: a community study. Child Abuse Negl. 20, 7–21. doi: 10.1016/0145-2134(95)00112-3
Murphy, A., Steele, M., Dube, S. R., Bate, J., Bonuck, K., Meissner, P., et al. (2014). Adverse Childhood Experiences (ACEs) Questionnaire and Adult Attachment Interview (AAI): implications for parent child relationships. Child Abuse Negl. 38, 224–233. doi: 10.1016/j.chiabu.2013.09.004
Nemeroff, C. B., Heim, C. M., Thase, M. E., Klein, D. N., Rush, A. J., Schatzberg, A. F., et al. (2003). Differential responses to psychotherapy versus pharmacotherapy in patients with chronic forms of major depression and childhood trauma. Proc. Natl. Acad. Sci. U.S.A. 100, 14293–14296. doi: 10.1073/pnas.2336126100
Newman, E., Kaloupek, D. G., and Keane, T. M. (1996). “Assessment of posttraumatic stress disorder in clinical and research settings,” in Traumatic Stress: The Effects of Overwhelming Experience on Mind, Body and Society, eds B. A. van der Kolk, A. C. McFarlane, and L. Weisaeth (New York, NY: Guilford Press), 242–275.
Panter, A. T., Swygert, K. A., Grant Dahlstrom, W., and Tanaka, J. S. (1997). Factor analytic approaches to personality item-level data. J. Pers. Assess. 68, 561–589. doi: 10.1207/s15327752jpa6803_6
Pynoos, R. S., Fairbank, J. A., Steinberg, A. M., Amaya-Jackson, L., Gerrity, E., Mount, M. L., et al. (2008). The national child traumatic stress network: collaborating to improve the standard of care. Prof. Psychol. Res. Pract. 39, 389–395. doi: 10.1037/a0012551
Ravitz, P., Maunder, R., Hunter, J., Sthankiya, B., and Lancee, W. (2010). Adult attachment measures: a 25-year review. J. Psychosom. Res. 69, 419–432. doi: 10.1016/j.jpsychores.2009.08.006
Roisman, G. I., Holland, A., Fortuna, K., Fraley, R. C., Clausell, E., and Clarke, A. (2007). The Adult Attachment Interview and self-reports of attachment style: an empirical rapprochement. J. Pers. Soc. Psychol. 92, 678–697. doi: 10.1037/0022-3514.92.4.678
Roy, C. A., and Perry, J. C. (2004). Instruments for the assessment of childhood trauma in adults. J. Nerv. Ment. Dis. 192, 343–351. doi: 10.1097/01.nmd.0000126701.23121.fa
Ruscio, J., and Roche, B. (2012). Determining the number of factors to retain in an exploratory factor analysis using comparison data of known factorial structure. Psychol. Assess. 24, 282–292. doi: 10.1037/a0025697
Sachs-Ericsson, N., Kendall-Tackett, K., and Hernandez, A. (2007). Childhood abuse, chronic pain, and depression in the National Comorbidity Survey. Child Abuse Negl. 31, 531–547. doi: 10.1016/j.chiabu.2006.12.007
Sagi, A., van IJzendoorn, M. H., Scharf, M., Koren-Karie, N., Joels, T., and Mayseless, O. (1994). Stability and discriminant validity of the Adult Attachment Interview: a psychometric study in young Israeli adults. Dev. Psychol. 30, 771–777. doi: 10.1037/0012-1649.30.5.771
Schaaf, K. K., and McCanne, T. R. (1998). Relationship of childhood sexual, physical, and combined sexual and physical abuse to adult victimization and posttraumatic stress disorder. Child Abuse Negl. 22, 1119–1133. doi: 10.1016/S0145-2134(98)00090-8
Schmahl, C., Lanius, R. A., Pain, C., and Vermetten, E. (2010). “Biological framework for traumatic dissociation related to early life trauma,” in The Impact of Early Relational Trauma on Health and Disease. The Hidden Epidemic, eds R. A. Lanius, E. Vermetten, and C. Pain (Cambridge: Cambridge University Press), 178–188.
Schore, A. N. (1999). Affect Regulation and the Origin of the Self: The Neurobiology of Emotional Development. Hillsdale, NJ: Erlbaum.
Schumm, J. A., Briggs-Phillips, M., and Hobfoll, S. E. (2006). Cumulative interpersonal traumas and social support as risk and resiliency factors in predicting PTSD and depression among inner-city women. J. Trauma. Stress 19, 825–836. doi: 10.1002/jts.20159
Shaw, B. A., Krause, N., Chatters, L. M., Connell, C. M., and Ingersoll-Dayton, B. (2004). Emotional support from parents early in life, aging, and health. Psychol. Aging 19, 4–12. doi: 10.1037/0882-7974.19.1.4
Shen, A. C. T. (2009). Long-term effects of interparental violence and child physical maltreatment experiences on PTSD and behavior problems: a national survey of Taiwanese college students. Child Abuse Negl. 33, 148–160. doi: 10.1016/j.chiabu.2008.07.006
Slack, K. S., Holl, J., Altenbernd, L., McDaniel, M., and Stevens, A. B. (2003). Improving the measurement of child neglect for survey research: issues and recommendations. Child Maltreat. 8, 98–111. doi: 10.1177/1077559502250827
Speranza, A. M., and Maggiora Vergano, C. (2015). Le rappresentazioni mentali e il trauma pregresso nei genitori di bambini maltrattati. Infanzia e Adolescenza 14, 22–44. doi: 10.1710/1862.20338
Spinazzola, J., Ford, J. D., Zucker, M., van der Kolk, B. A., Silva, S., Smith, S. F., et al. (2005). Survey evaluates complex trauma exposure, outcome, and intervention among children and adolescents. Psychiatr. Ann. 35, 433–439.
Stevens, T. N., Ruggiero, K. J., Kilpatrick, D. G., Resnick, H. S., and Saunders, B. E. (2005). Variables differentiating singly and multiply victimized youth: results from the national survey of adolescents and implications for secondary prevention. Child Maltreat. 10, 211–223. doi: 10.1177/1077559505274675
Stoltenborgh, M., Bakermans-Kranenburg, M. J., and van IJzendoorn, M. H. (2013). The neglect of child neglect: a meta-analytic review of the prevalence of neglect. Soc. Psychiatr. Psychiatr. Epidemiol. 48, 345–355. doi: 10.1007/s00127-012-0549-y
Straus, M. A., and Kantor, G. K. (2005). Definition and measurement of neglectful behavior: some principles and guidelines. Child Abuse Negl. 29, 19–29. doi: 10.1016/j.chiabu.2004.08.005
Straus, M. A., Kinard, E. M., and Williams, L. M. (1995). The Multidimensional Neglectful Behavior Scale, Form A: Adolescent and Adult-recall Version. Durham, NH: University of New Hampshire, Family Research Laboratory.
Teicher, M. H., and Parigger, A. (2015). The ‘Maltreatment and Abuse Chronology of Exposure’ (MACE) Scale for the retrospective assessment of abuse and neglect during development. PLoS ONE 10:e0117423. doi: 10.1371/journal.pone.0117423
Timmerman, M. E., and Lorenzo-Seva, U. (2011). Dimensionality assessment of ordered polytomous items with parallel analysis. Psychol. Methods 16, 209–220. doi: 10.1037/a0023353
Trickett, P. K., Kim, K., and Prindle, J. (2011). Variations in emotional abuse experiences among multiply maltreated young adolescents and relations with developmental outcomes. Child Abuse Negl. 35, 876–886. doi: 10.1016/j.chiabu.2011.08.001
Turner, H. A., Finkelhor, D., and Ormrod, R. (2010). Poly-victimization in a national sample of children and youth. Am. J. Prev. Med. 38, 323–330. doi: 10.1016/j.amepre.2009.11.012
U.S. Department of Health Human Services, Administration on Children, Youth, Families. (2011). Child Maltreatment 2010. Washington, DC: U.S. Government Printing Office.
van der Kolk, B. A., and d'Andrea, W. (2010). “Towards a developmental trauma disorder diagnosis for childhood interpersonal trauma,” in The Impact of Early Life Trauma on Health and Disease: The Hidden Epidemic, eds R. A. Lanius, E. Vermetten, and C. Pain (New York, NY: Cambridge University Press), 57–68.
van IJzendoorn, M. H. (1995). Adult attachment representations, parental responsiveness, and infant attachment: a meta-analysis on the predictive validity of the Adult Attachment Interview. Psychol. Bull. 117, 387–403. doi: 10.1037/0033-2909.117.3.387
van IJzendoorn, M. H., and Bakermans-Kranenburg, M. J. (2008). “The distribution of adult attachment representations in clinical groups: a meta-analytic search for patterns of attachment in 105 AAI studies,” in Clinical Applications of the Adult Attachment Interview, eds H. Steele, and M. Steele (New York, NY: Guilford Press), 69–96.
van IJzendoorn, M. H., Schuengel, C., and Bakermans-Kranenburg, M. J. (1999). Disorganized attachment in early childhood: Meta-analysis of precursors, concomitants, and sequelae. Dev. Psychopathol. 11, 225–249. doi: 10.1017/S0954579499002035
Veale, J. F., Clarke, D. E., and Lomax, T. C. (2010). Biological and psychosocial correlates of adult gender-variant identities: a review. Pers. Indiv. Differ. 48, 357–366. doi: 10.1016/j.paid.2009.09.018
Vranceanu, A.-M., Hobfoll, S. E., and Johnson, R. J. (2007). Child multi-type maltreatment and associated depression and PTSD symptoms: the role of social support and stress. Child Abuse Negl. 31, 71–84. doi: 10.1016/j.chiabu.2006.04.010
Widom, C. S., DuMont, K., and Czaja, S. J. (2007). A prospective investigation of major depressive disorder and comorbidity in abused and neglected children grown up. Arch. Gen. Psychiatr. 64, 49–56. doi: 10.1001/archpsyc.64.1.49
Keywords: Complex Trauma Questionnaire, relational trauma, attachment, assessment, psychometric properties
Citation: Maggiora Vergano C, Lauriola M and Speranza AM (2015) The Complex Trauma Questionnaire (ComplexTQ): development and preliminary psychometric properties of an instrument for measuring early relational trauma. Front. Psychol. 6:1323. doi: 10.3389/fpsyg.2015.01323
Received: 20 April 2015; Accepted: 18 August 2015;
Published: 01 September 2015.
Edited by:
Alessandra Simonelli, University of Padova, ItalyReviewed by:
Inez Myin-Germeys, University of Maastricht, NetherlandsWolfgang Tschacher, University of Bern, Switzerland
Copyright © 2015 Maggiora Vergano, Lauriola and Speranza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carola Maggiora Vergano, Department of Dynamic and Clinical Psychology, Faculty of Medicine and Psychology, Sapienza University, Via dei Marsi 78, 00185 Rome, Italy, carolamv@fastwebnet.it