Corrigendum: Gender Differences in the Physical and Psychological Manifestation of Childhood Trauma and/or Adversity in People with Psychosis
 Shaun Sweeney
Shaun Sweeney Tracy Air
Tracy Air Lana Zannettino
Lana Zannettino Sonal S. Shah3
Sonal S. Shah3 Cherrie Galletly
Cherrie Galletly- 1Discipline of Psychiatry, University of Adelaide, Adelaide, SA, Australia
- 2School of Nursing and Midwifery, Flinders University, Adelaide, SA, Australia
- 3Neuropsychiatric Epidemiology Research Unit, School of Psychiatry and Clinical Neurosciences Laboratory, University of Western Australia, Perth, WA, Australia
The link between childhood trauma and/or adversity and risk of psychosis is well known. Our aim was to determine the prevalence of childhood trauma and/or adversity in people who have psychotic disorders and to investigate the association between childhood trauma and/or adversity and a range of social and health measures. Participants (n = 391, 42% male) were specifically asked about any experience of childhood trauma and/or adversity. Respondents provided information about education, employment, physical health, and health service utilization. Univariate analyses revealed that childhood trauma and/or adversity was associated with poorer levels of self-reported physical health and social problems. This includes the experience of chronic pain, headaches, arthritis, asthma, and victimization/stigma in men. Participants with a childhood trauma and/or adversity history indicated higher rates of lifetime suicide attempts with women reporting more lifetime depressive symptoms. Multivariate analyses revealed differing profiles in relation to physical and psychological health variable between males and females. Males with the experience of childhood trauma and/or adversity were significantly more likely to report cardiovascular/stroke issues, migraines and anhedonia. Females with the experience of childhood trauma and/or adversity were more likely to report a lifetime history of elevated mood and to be married or in a de facto relationship. There has been very little research into the assessment and treatment of the effects of childhood trauma and/or adversity in adults with psychosis. Childhood trauma and/or adversity may contribute to higher rates of self-reported poor health in men and is associated with increased depression in women. Our findings suggest that interventions to address the effects of past trauma are urgently needed.
Introduction
Psychosis is defined as the presence of hallucinations and delusions and is present in a number of psychiatric disorders including schizophrenia, delusional disorders, schizoaffective disorders, and drug-induced psychosis. These symptoms can result in impaired functioning in work and school, and can affect parenting, self-care, independent living, interpersonal relationships, and leisure time (Mueser and McGurk, 2004). Psychotic disorders are complex illnesses that can have a profound long-term health, psychological and social impact on the individual. Research in the field indicates that complex, interrelated factors can determine the etiology and course of the illness. There is also strong evidence pointing to the relationship between the experiences of trauma and/or adversity and the development of psychosis, including a correlation between trauma and/or adversity in childhood and the development of psychosis (Morgan and Fisher, 2007).
Estimates of the rates of childhood trauma and/or adversity (CTA) worldwide indicate that every year millions of children experience trauma including physical, sexual, emotional abuse, and severe neglect (Krause, 2008). The terminology associated with trauma, adversity, and early life stress is often used interchangeably across numerous social and health contexts. In discussing the different interpretations of trauma and adversity, Brown et al. (1999) provide a definitive definition of trauma and adversity in childhood that encompasses child abuse and neglect. This definition includes the experience of verbal assaults on a child’s sense of worth, bodily assaults that pose risk of injury, sexual contact, failure to provide basic psychological/emotional needs, and a failure to provide basic needs (Bernstein and Fink, 1998; Browne and Winkelman, 2007). CTA is associated with a range of poor health and psychological outcomes, (Spataro et al., 2004) and is associated with the development of psychotic disorders in adulthood (Janssen et al., 2004; Matheson et al., 2013). In particular, the experience(s) of CTA can lead to high levels of anxiety and is associated with hallucinations, psychological withdrawal, depression, and hopelessness (Lysaker and Salyers, 2007). The health and psychosocial outcomes of CTA can vary according to gender, with women being more likely to experience sexual abuse whilst men tend to be subjected to physical abuse and/or bullying (Read et al., 2005). Additionally, in particular cohorts, such as adult women in drug treatment services, as many as 62–81% report CTA (Teets, 1995; Gil-Rivas et al., 1997; Liebschutz et al., 2002).
While research has been conducted into the influence of CTA, particularly child sexual abuse on health, psychological, and social functioning in female populations, CTA in male cohorts has received less attention, primarily due to its seemingly lower prevalence rates and less overt symptomatic presentation(s). There is widespread evidence that psychosis is correlated with poor physical health, lower levels of educational attainment, and poorer socioeconomic outcomes (Lund et al., 2010). People with psychosis can also exhibit higher rates of obesity (Taylor et al., 2012), illness comorbidity (Sim et al., 2004), and substance abuse than in the general population (Addington and Addington, 2007). For those with a history of CTA and who have developed a psychotic disorder, the combination of this serious mental illness along with the challenges of living with the psychological effects of CTA can make health, economic and social functioning extremely difficult (Spataro et al., 2004).
Despite an extensive collection of research into the effects of psychosis on many of the domains of life there has been little exploration of the physical impact of CTA on people living with psychosis. The present study took place in the northern region of Adelaide, South Australia. This is a disadvantaged region with a high proportion of people in receipt of government benefits, high unemployment rates, lower levels of education, and high rates of mental health (Ahern et al., 2006). Within this adverse socioeconomic environment, our aim was to determine the prevalence of CTA in people who have psychotic disorders, and to investigate the associations between CTA and a range of psychiatric, social, and health measures. Given that gender differences in both the nature and adult consequences of CTA were likely, we undertook separate analyses for men and for women.
It was expected that co-existing CTA and psychosis would be associated with a poorer outcome than psychosis alone. Additionally, the role of gender in affecting psychosocial and health outcomes was also explored. We expected participants who experienced CTA to have left school earlier, be more likely to be unemployed, and to have poorer economic functioning. We also expected people subject to CTA to be more likely to abuse drugs and alcohol, self-harm and/or attempt suicide. Given their exposure to abuse and/or violence during childhood, we also considered it likely that they would experience stigma, bullying, and/or violence as adults. We also expected that their physical health (both objective and subjective) would be worse. These assumptions are based on evidence in the CTA literature indicating the correlation between CTA and lower socio-economic status, and poor health compared to non-CTA populations.
Materials and Methods
Participants for the study were randomly selected from people who have been in contact with a mental health service or a non-government organization funded to provide mental health services. The SHIP projected utilized a psychosis screener to identify potential participants. Potential participants were screened for psychosis between April 1st, 2009 and March 31st, 2010. The psychosis screener identified potential SHIP participants who were positive for psychosis on the basis of their contact(s) with mental health services or who recorded ICD-10 diagnosis of psychosis. The psychosis screener identified 1825 adults aged 18–64 years who were residents in the South Australian postcode catchment area. Potential participants needed to have been in contact with public mental health services in the 12 months prior to the survey to be eligible to participate in the SHIP study. The exclusion criteria included severe cognitive impairment, the inability to comprehend English sufficiently to complete the interview without the use of an interpreter. Attempts were made to recruit all of these potential participants. Eight hundred and twenty three were unable to be contacted due to change of personal circumstance (e.g., moved away from the catchment area, changed their phone number, were non-responders to phone/mail contact or did not attend the SHIP interview), 16 were known to have died, 33 did not meet inclusion criteria due to inability to sufficiently communicate in English, 42 did not have capacity to give informed consent, and 507 refused. Potential participants were identified during the SHIP census period and in total 402 participants were interviewed. Comparison of screening data for interviewed participants and those selected for interview but not participating for any reason indicated no systematic selection biases. Both groups were alike in terms of sex (60% of those interviewed were male compared to 62% of those selected but not interviewed) and age group (44% of those interviewed were aged 18–34 years at the time of screening compared with 43% of those not interviewed). The psychosis screening profiles for both groups were similar indicating no marked differences in terms of lifetime symptom profiles based on the screener items.
The SHIP interview schedule consisted of 32 modules and asked participants about psychopathology, substance use, physical health, functioning, disability and quality of life, education, employment, accommodation, and childhood adversity. The social, health, and economic profile information of participants consisted of, but were not limited to: demographic status, socioeconomic and psychosocial status, health and physical functioning, diagnosis, and symptomology. Diagnoses were made using the Diagnostic Interview for Psychosis (DIP; Castle et al., 2006). The DIP contains selected interview questions and probes from the WHO Schedules for Clinical Assessment in Neuropsychiatry (Wing et al., 1990) mapped onto the 90 diagnostic items of the operational criteria checklist for psychotic and affective illness (McGuffin et al., 1991). The DIP measured both lifetime and current illness symptoms for psychosis. A computer algorithm provided the diagnostic classification in accordance with ICD-10, DSM-IV, and other criteria on the basis of the DIP scores. This reduced the subjective bias in the interpretation of symptoms and signs (Shah et al., 2014). No specific analysis was conducted regarding the non-responders to the SHIP research project. Further information regarding the method of the SHIP research project is detailed in Morgan et al. (2012).
Questions regarding the occurrence and nature of CTA were included in the interview. In Australia, all states follow a national framework of guidelines for defining the four types of child abuse (a) sexual abuse, (b) physical abuse, (c) emotional abuse, and (d) neglect. The classification of reported CTA was undertaken in collaboration with staff from the Western Australian Department of Child Protection to ensure conformity to national guidelines. This paper includes only those cases where the CTA is consistent with the standard Australian definitions, took place when the participant was aged 18 years or younger and occurred prior to the onset of psychotic illness.
Ethics Statement
Ethics approval for this research was obtained from the Human Research Ethics Committee of the Queen Elizabeth Hospital (Protocol number: 2009179).
Assessments
The Second Australian Survey of Psychosis 2010 interview schedule was comprised of 32 modules, including the Alcohol Use Disorders Identification Test (Babor et al., 2001), the World Health Organization Schedules for Clinical Assessment in Neuropsychiatry (Kirkpatrick et al., 1989; World Health Organization, 1999). The details for all other measures are described in Morgan et al. (2012).
Childhood Trauma and/or Adversity
Questions about the occurrence and nature of CTA were included in the SHIP interview. CTA was coded on the basis of responses to the question: “Were there any other very distressing or traumatic events in your childhood (not including parental separation or divorce, or loss of a close relative)?”
Statistical Analyses
Statistical analyses were performed using Stata, version 12 (StataCorp, 2011). A two-step model building procedure was used to determine variables associated with CTA. In the first step, we used univariate analyses (chi-squares and t-tests) to examine relationships between CTA and independent variables. In the second step, we used multivariate logistic regressions, including only variables that were significantly associated with CTA status at alpha ≤0.05 in the first step. As the incidence of CTA was much higher in females, the analyses were also stratified by gender to explore gender specific associations. In the final stratified model, only the significant variables were retained, adjusting for possible confounders of health status such as lifetime histories of smoking, heavy alcohol usage and cannabis use.
Given the difference between genders in the numbers reporting CTA, a post hoc power analysis with the program G∗Power, Version 3.1.9.2 (Faul et al., 2009) was conducted. The analysis implied that statistical power (power = 0.96) was sufficient, rendering it unlikely that significant differences between the groups could have been overlooked.
Results
Of the 391 participants, 59.3% of reported experiencing CTA. CTA was reported more in females than males (χ2 = 19.7, df = 1, p < 0.001). Table 1 depicts the results of the univariate analyses comparing CTA and no CTA participants on socio-demographic data. Participants who had experienced CTA were more likely to be married or living in a de facto relationship (χ2 = 13.2, df = 2, p = 0.001), and had left school earlier (t = –3.22, df = 389, p = 0.001). There was no difference in diagnosis or in rates of current smoking, lifetime history of heavy alcohol use, or cannabis use, between those with and without CTA.
TABLE 1
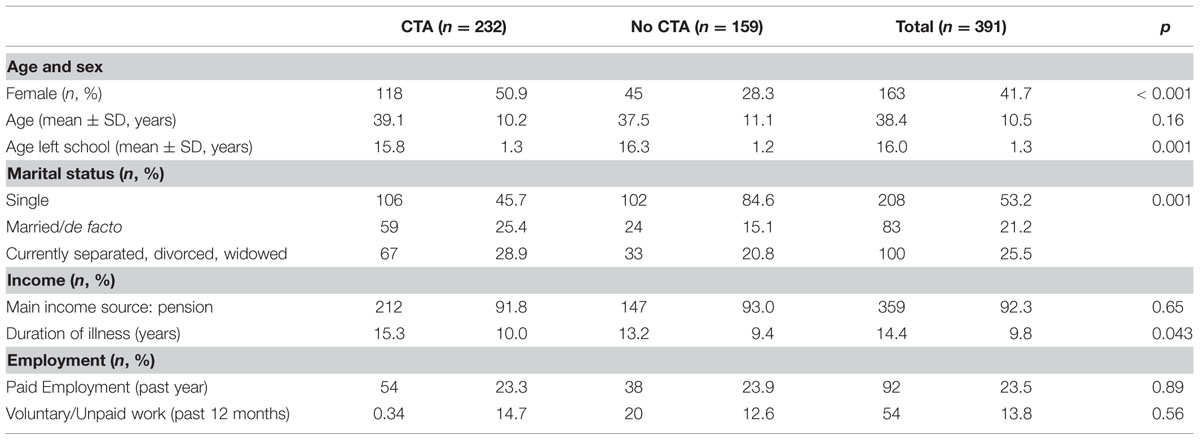
TABLE 1. Socio-demographic data for people with psychosis, comparing those who had experienced childhood trauma and/or adversity (CTA) with those who had not.
Physical and Psychological Health
Table 2 displays the results for the univariate analyses on physical health. The CTA group generally indicated higher rates of reported lifetime physical health conditions. More of the CTA positive group experienced chronic pain (χ2 = 18.24, df = 1, p = 0.001), headaches/migraines (χ2 = 19.73, df = 1, p = 0.001), arthritis (χ2 = 10.88, df = 1, p = 0.001) and asthma (χ2 = 5.52, df = 1, p = 0.019). In the overall sample, cardiovascular disease and/or stroke was also more common in the CTA positive group (χ2 = 9.80, df = 1, p = 0.002).
TABLE 2
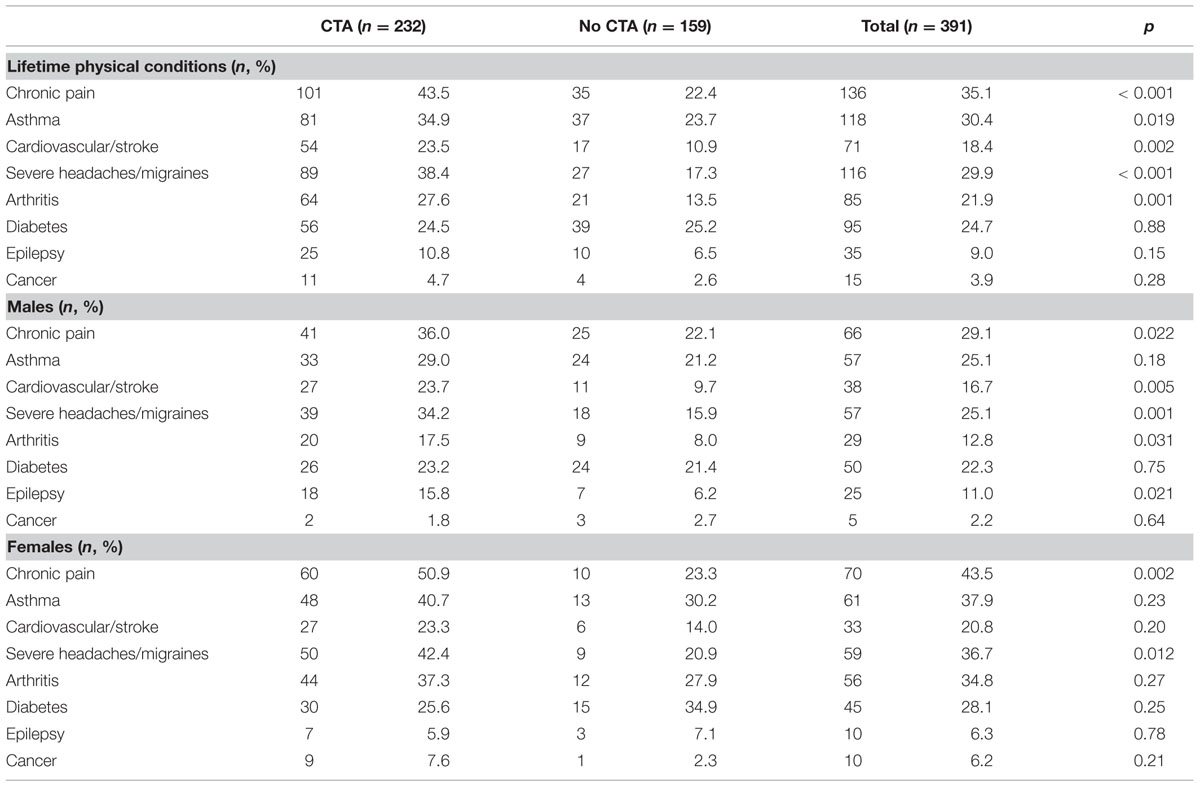
TABLE 2. Lifetime physical conditions.
More males with a history of CTA than expected reported chronic pain (χ2 = 5.2, df = 1, p = 0.022), cardiovascular disease/stroke (χ2 = 7.9, df = 1, p = 0.005), headaches/migraines (χ2 = 10.0, df = 1, p = 0.001), arthritis (χ2 = 4.7, df = 1, p = 0.031) and epilepsy (χ2 = 5.3, df = 1, p = 0.021). More females with CTA than expected reported chronic pain (χ2 = 9.8, df = 1, p = 0.002) and headaches/migraines (χ2 = 6.2, df = 1, p = 0.012).
Univariate analyses revealed that the CTA positive group experienced different rates of lifetime psychological symptoms than the non-CTA group (Table 3). For example, the CTA group were more likely to report a lifetime history of depressive mood (χ2 = 7.96, df = 1, p = 0.005), anhedonia (χ2 = 14.30, df = 1, p = 0.001), poor concentration (χ2 = 4.67, df = 1, p = 0.031), elevated mood (χ2 = 5.16, df = 1, p = 0.023). However, the non-CTA group were more likely to report a lack of insight (χ2 = 5.68, df = 1, p = 0.017). Males with CTA also were more likely to have experienced anhedonia (χ2 = 8.44, df = 1, p = 0.004) and subjective thought disorder (χ2 = 3.87, df = 1, p = 0.049). Conversely, females with CTA were more likely to have reported depressive mood symptoms (χ2 = 5.59, df = 1, p = 0.018) and elevated mood symptoms (χ2 = 4.30, df = 1, p = 0.038).
TABLE 3
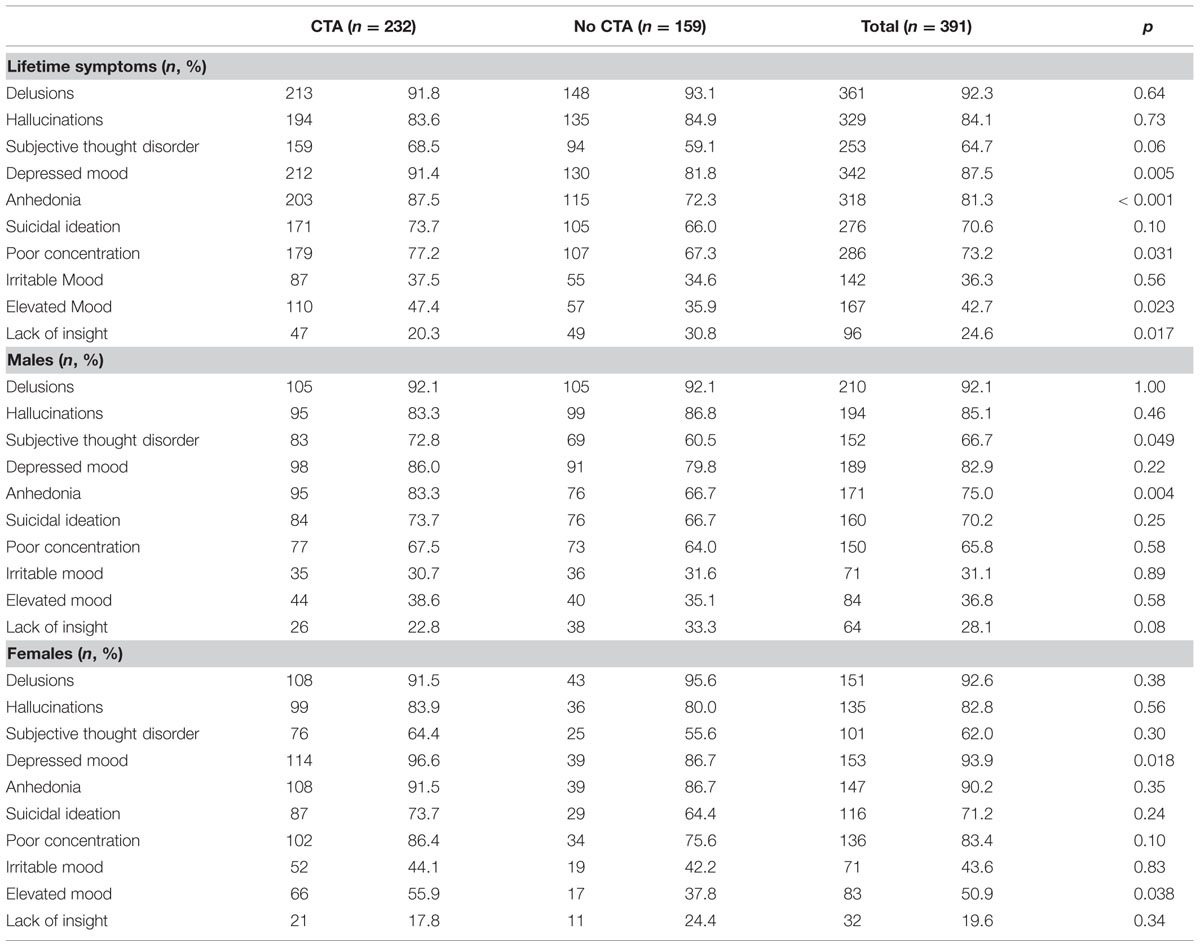
TABLE 3. Psychological symptoms: lifetime.
Physical and Psychological Health Profile
Table 4 displays the results of the final multivariate logistic regression model for men and women, adjusted for age at interview and socioeconomic status. Most of the physical and psychological health variables that had been significant in the univariate analyses were no longer so in the multivariate models for either gender. However, males who had experienced CTA were more likely to report experiencing a lifetime history of cardiovascular/stroke health issues, migraines and anhedonia. Conversely, females who had experienced CTA were significantly more likely to be in a married/de facto relationship and a lifetime history of elevated mood. The physical health measures were not significantly associated with CTA.
TABLE 4
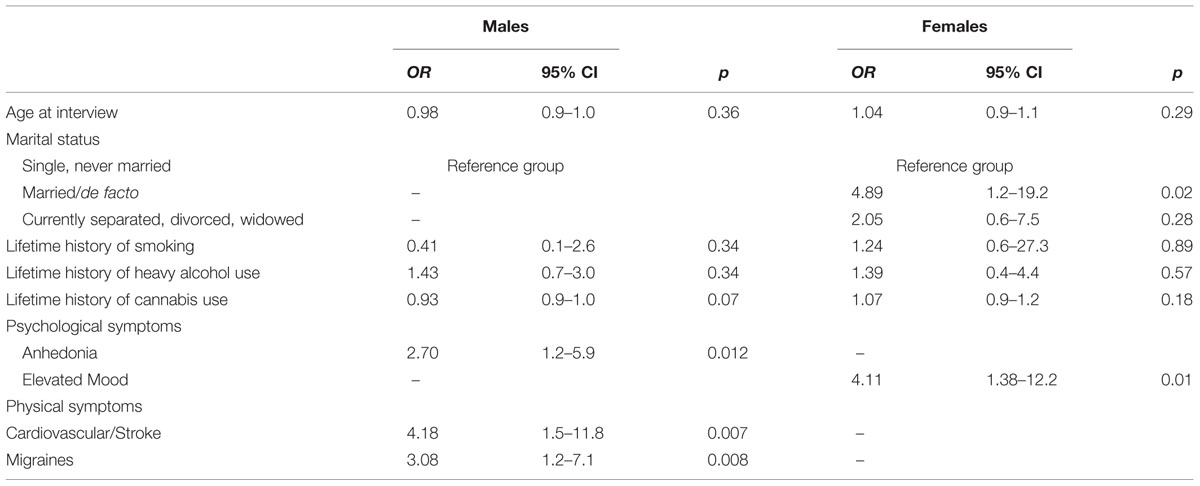
TABLE 4. Relationship between CTA and demographics, psychological and physical health profiles in people with psychosis, stratified by sex.
Discussion
Considerable research has been conducted into the effect of CTA on health, psychological, and social functioning in female populations. Associations between CTA and physical illnesses, including cardiac, respiratory, and gastrointestinal diseases, has also been reported in general population samples (Goodwin and Stein, 2004). However, CTA in male cohorts has received less consideration, primarily due to its seemingly lower prevalence rates and less overt symptomatic presentation(s). The high rate of the self-reporting of physical illness in male psychosis populations such as ours may be evidence of a CTA history. Most significantly, it may characterize a psychological disorder, one that represents a manifestation of an undisclosed CTA experience(s). Self-reported health risks can potentially compound the already high health, psychological, and social burden associated with psychotic illness for this population. These represent deficits that can exacerbate the psychological burden of the experience(s) of CTA. The SHIP cohort presented with a myriad of physical, psychological, and social challenges that did not translate into multivariate explanatory models. Given that the entire sample was in poor physical and psychological health and were socio-economically marginalized, this should not surprise. Overall, prevalence of CTA was high, with over 60% of participants reporting physical, sexual and/or emotional abuse, and neglect. This is consistent with the association between CTA and adult psychotic disorders (Morgan and Fisher, 2007; Matheson et al., 2013). Participants with a CTA history left school earlier and experienced higher rates of employment. Conversely, unlike general population samples where CTA has been associated with higher rates of substance use (Dube et al., 2003), the CTA cohort in this sample did not replicate this research. Furthermore, the CTA cohort was more likely to be married and have children, suggesting a better capacity to form intimate relationships. Additionally, the self-reported poorer physical health, which was more prominent in men, may reflect somatic expression of emotional distress, or poorer self-care with greater vulnerability to physical illness.
Our study accessed a large representative sample of people with psychotic illness living in a disadvantaged region of urban Adelaide, South Australia. The finding that CTA may influence and potentially compromise health functioning among adults with psychosis is intriguing. Despite this, there has been very little research into the assessment and treatment of the effects of CTA in adults with psychosis. Thus, there are unanswered questions about the role of CTA in the symptoms and outcomes of men with psychosis and this awaits future research. Further research is also needed to determine the extent to which the relationship between CTA and health and psychosocial functioning is moderated by other intervening variables, such as cognitive function, substance abuse, and illness symptomology, in psychosis populations. A significant portion of non-psychosis trauma in the literature links CTA to deficits in areas such as psychological and social functioning (Mulvihill, 2005) as well as health functioning (Norman et al., 2006). Nonetheless, our sample unexpectedly did not replicate this association, either at a univariate or multivariate level of analysis. Our findings suggest that interventions are urgently needed. These challenges highlight the importance of an integrated approach to mental health and community based service provision. Such an approach may help to ensure that people with psychosis and the experience(s) of CTA have their health and social needs met in ways that can enhance their illness recovery. Answers to these questions will help in better understanding the processes surrounding health and psychosocial functioning in psychosis populations and to develop and deliver more effective clinical treatments. The population-level data collected as part of the 2010 SHIP research provide a solid empirical foundation to guide health and social policy development and the provision of mental health services regarding many aspects of psychosis/CTA populations.
Limitations
This study has a number of important limitations. Although we were able to explore the temporal relationship between self-reported physical health and clinical outcomes in adulthood, we were unable to determine severity, frequency, duration and perpetrator of the abuse due to the interview design. Therefore, we may have missed important patterns of association. In addition, we acknowledge that longitudinal studies that collect CTA data prospectively are the optimal design for this type of research.
As our data rely on retrospective self-report, the accuracy may be affected by recall bias. However, a number of studies have demonstrated the validity and reliability of retrospective reports of trauma in psychosis populations. These studies indicated that reports of CTA are stable across time, unaffected by current symptoms, and generally correlate well with other sources of information (Arseneault et al., 2011). Additionally, there is evidence that the retrospective assessment of child abuse tends to underestimate rather than over-report real rates, possibly due to poor memory, denial, or embarrassment. Consequently, our data may underestimate the strength of the relationship between CTA and subsequent outcomes.
Author Contributions
SS was primarily responsible for the conception of the research upon which this paper is based. CG, LZ, and TA assisted in the development of the ideas for the paper and in refining the final manuscript. SS produced the first draft of the manuscript and submitted the final manuscript and completed the literature search and wrote the main body of the manuscript. TA analyzed the data. SSS contributed to acquisition, analysis and interpretation of the national SHIP data; was part of initial discussions on the substance of this paper, and critically contributed to the draft of the revised version. All authors approved the final manuscript.
Funding
The 2010 Australian National Survey of Psychosis was funded by the Australian Government Department of Health and Ageing.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group are: V. Morgan (National Project Director), A. Jablensky (Chief Scientific Advisor), A. Waterreus (National Project Coordinator), R. Bush, V. Carr, D. Castle, M. Cohen, C. Galletly, C. Harvey, B. Hocking, A. Mackinnon, P. McGorry, J. McGrath, A. Neil, S. Saw, H. Stain. Ethics approvals for the study were obtained from relevant institutional human research ethics committees.
The Second Australian Survey of Psychosis 2010 acknowledges and thanks the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
References
Addington, J., and Addington, D. (2007). Patterns, predictors and impact of substance use in early psychosis: a longitudinal study. Acta Psychiatr. Scand. 115, 304–309. doi: 10.1111/j.1600-0447.2006.00900.x
Ahern, N. R., Kiehl, E. M., Lou Sole, M., and Byers, J. (2006). A review of instruments measuring resilience. Issues Compr. Pediatr. Nurs. 29, 103–125. doi: 10.1080/01460860600677643
Arseneault, L., Cannon, M., Fisher, H. L., Polanczyk, G., Moffitt, T. E., and Caspi, A. (2011). Childhood trauma and children’s emerging psychotic symptoms: a genetically sensitive longitudinal cohort study. Am. J. Psychiatry 168, 65–72. doi: 10.1176/appi.ajp.2010.10040567
Babor, T. F., Higgins-Biddle, J. C., Saunders, J. B., and Monteiro, M. G. (2001). The Alcohol Use Disorders Identification Test. Guidelines for Use in Primary Care, Vol. 2. Geneva: World Health Organization.
Bernstein, D. P., and Fink, L. (1998). Childhood Trauma Questionnaire: A Retrospective Self-Report: Manual. San Diego, CA: Harcourt Brace & Company.
Brown, J., Cohen, P., Johnson, J. G., and Smailes, E. M. (1999). Childhood abuse and neglect: specificity of effects on adolescent and young adult depression and suicidality. J. Am. Acad. Child Adolesc. Psychiatry 38, 1490–1496. doi: 10.1097/00004583-199912000-00009
Browne, C., and Winkelman, C. (2007). The effect of childhood trauma on later psychological adjustment. J. Interpers. Violence 22, 684–697. doi: 10.1177/0886260507300207
Castle, D. J., Jablensky, A., McGrath, J. J., Carr, V., Morgan, V., Waterreus, A., et al. (2006). The diagnostic interview for psychoses (DIP): development, reliability and applications. Psychol. Med. 36, 69–80. doi: 10.1017/S0033291705005969
Dube, S. R., Felitti, V. J., Dong, M., Chapman, D. P., Giles, W. H., and Anda, R. F. (2003). Childhood abuse, neglect, and household dysfunction and the risk of illicit drug use: the adverse childhood experiences study. Pediatrics 111, 564–572. doi: 10.1542/peds111.3.564
Faul, F., Erdfelder, E., Buchner, A., and Lang, A.-G. (2009). Statistical power analyses using G∗Power 3.1: tests for correlation and regression analysis. Behav. Res. Methods 41, 1149–1160. doi: 10.3758/BRM.41.4.1149
Gil-Rivas, V., Fiorentine, R., Douglas Anglin, M., and Taylor, E. (1997). Sexual and physical abuse: do they compromise drug treatment outcomes? J. Subst. Abuse Treat. 14, 351–358. doi: 10.1016/S0740-5472(97)84631-4
Goodwin, R. D., and Stein, M. B. (2004). Association between childhood trauma and physical disorders among adults in the United States. Psychol. Med. 34, 509–520. doi: 10.1017/S003329170300134X
Janssen, I., Krabbendam, L., Bak, M., Hanssen, M., Vollebergh, W., Graaf, R. D., et al. (2004). Childhood abuse as a risk factor for psychotic experiences. Acta Psychiatr. Scand. 109, 38–45. doi: 10.1046/j.0001-690X.2003.00217.x
Kirkpatrick, B., Buchanan, R. W., McKenny, P. D., Alphs, L. D., and Carpenter, W. T. (1989). The schedule for the deficit syndrome: an instrument for research in schizophrenia. Psychiatry Res. 30, 119–123. doi: 10.1016/0165-1781(89)90153-4
Krause, N. (2008). Lifetime trauma, prayer, and psychological distress in late life. Int. J. Psychol. Religion 19, 55–72. doi: 10.1080/10508610802471112
Liebschutz, J., Savetsky, J. B., Saitz, R., Horton, N. J., Lloyd-Travaglini, C., and Samet, J. H. (2002). The relationship between sexual and physical abuse and substance abuse consequences. J. Subst. Abuse Treat. 22, 121–128. doi: 10.1016/S0740-5472(02)00220-9
Lund, C., Breen, A., Flisher, A. J., Kakuma, R., Corrigall, J., Joska, J. A., et al. (2010). Poverty and common mental disorders in low and middle income countries: a systematic review. Soc. Sci. Med. 71, 517–528. doi: 10.1016/j.socscimed.2010.04.027
Lysaker, P., and Salyers, M. (2007). Anxiety symptoms in schizophrenia spectrum disorders: associations with social function, positive and negative symptoms, hope and trauma history. Acta Psychiatr. Scand. 116, 290–298. doi: 10.1111/j.1600-0447.2007.01067.x
Matheson, S., Shepherd, A., Pinchbeck, R., Laurens, K., and Carr, V. (2013). Childhood adversity in schizophrenia: a systematic meta-analysis. Psychol. Med. 43, 225–238. doi: 10.1017/S0033291712000785
McGuffin, P., Farmer, A., and Harvey, I. (1991). A polydiagnostic application of operational criteria in studies of psychotic illness. Development and reliability of the OPCRIT system. Arch. Gen. Psychiatry 48, 764–770. doi: 10.1001/archpsyc.1991.01810320088015
Morgan, C., and Fisher, H. (2007). Environment and schizophrenia: environmental factors in schizophrenia: childhood trauma—a critical review. Schizophr. Bull. 33, 3–10. doi: 10.1093/schbul/sbl053
Morgan, V. A., Waterreus, A., Jablensky, A., Mackinnon, A., McGrath, J. J., Carr, V., et al. (2012). People living with psychotic illness in 2010: the second Australian national survey of psychosis. Aust. N. Z. J. Psychiatry 46, 735–752. doi: 10.1177/0004867412449877
Mueser, K., and McGurk, S. (2004). Schizophrenia. Lancet 363, 2063–2072. doi: 10.1016/S0140-6736(04)16458-1
Mulvihill, D. (2005). The health impact of childhood trauma: an interdisciplinary review, 1997–2003. Issues Compr. Pediatr. Nurs. 28, 115–136. doi: 10.1080/01460860590950890
Norman, S. B., Means-Christensen, A. J., Craske, M. G., Sherbourne, C. D., Roy-Byrne, P. P., and Stein, M. B. (2006). Associations between psychological trauma and physical illness in primary care. J. Trauma. Stress 19, 461–470. doi: 10.1002/jts.20129
Read, J., van Os, J., Morrison, A., and Ross, C. A. (2005). Childhood trauma, psychosis and schizophrenia: a literature review with theoretical and clinical implications. Acta Psychiatr. Scand. 112, 330–350. doi: 10.1111/j.1600-0447.2005.00634.x
Shah, S., Mackinnon, A., Galletly, C., Carr, V., McGrath, J. J., Stain, H. J., et al. (2014). Prevalence and impact of childhood abuse in people with a psychotic illness. Data from the second Australian National Survey of Psychosis. Schizophr. Res. 159, 20–26. doi: 10.1016/j.schres.2014.07.011
Sim, K., Swapna, V., Mythily, S., Mahendran, R., Kua, E., McGorry, P., et al. (2004). Psychiatric comorbidity in first episode psychosis: the Early Psychosis Intervention Program (EPIP) experience. Acta Psychiatr. Scand. 109, 23–29. doi: 10.1111/j.0001-690X.2004.00196.x
Spataro, J., Mullen, P. E., Burgess, P. M., Wells, D. L., and Moss, S. A. (2004). Impact of child sexual abuse on mental health. Br. J. Psychiatry 184, 416–421. doi: 10.1192/bjp.184.5.416
Taylor, V. H., McIntyre, R. S., Remington, G., Levitan, R. D., Stonehocker, B., and Sharma, A. M. (2012). Beyond pharmacotherapy: understanding the links between obesity and chronic mental illness. Can. J. Psychiatry 57, 5–12.
Teets, J. M. (1995). Childhood sexual trauma of chemically dependent women. J. Psychoactive Drugs 27, 231–238. doi: 10.1080/02791072.1995.10472468
Wing, J. K., Babor, T., Brugha, T., Burke, J., Cooper, J. E., Giel, R., et al. (1990). SCAN. Schedules for clinical assessment in neuropsychiatry. Arch. Gen. Psychiatry 47, 589–593. doi: 10.1001/archpsyc.1990.01810180089012
Keywords: childhood trauma and/or adversity, psychosis, self-reported health status, gender
Citation: Sweeney S, Air T, Zannettino L, Shah SS and Galletly C (2015) Gender Differences in the Physical and Psychological Manifestation of Childhood Trauma and/or Adversity in People with Psychosis. Front. Psychol. 6:1768. doi: 10.3389/fpsyg.2015.01768
Received: 10 August 2015; Accepted: 04 November 2015;
Published: 23 November 2015.
Edited by:
Sayyed Mohsen Fatemi, Harvard University, USAReviewed by:
Michelle Dow Keawphalouk, Harvard and Massachusetts Institute of Technology, USARaffaella Calati, IRCCS Centro San Giovanni di Dio, Fatebenefratelli, Italy
Copyright © 2015 Sweeney, Air, Zannettino, Shah and Galletly. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shaun Sweeney, shaun.sweeney@adelaide.edu.au