 Martin Christoph Melchers
Martin Christoph Melchers Thomas Plieger
Thomas Plieger Rolf Meermann2
Rolf Meermann2 Martin Reuter
Martin Reuter- 1Department of Psychology, University of Bonn, Bonn, Germany
- 2AHG Psychosomatic Hospital, Bad Pyrmont, Germany
- 3Center for Economics and Neuroscience (CENs), University of Bonn, Bonn, Germany
Stress-related affective disorders have been identified as a core health problem of the twenty-first century. In the endeavor to identify vulnerability factors, personality has been discussed as a major factor explaining and predicting disorders like depression or burnout. An unsolved question is whether there are specific personality factors allowing differentiation of burnout from depression. The present study tested the relation between one of the most prominent, biological personality theories, Cloninger’s Temperament and Character Inventory, and common measures of burnout (Maslach Burnout Inventory General) and depression (Beck Depression Inventory 2) in a sample of German employees (N = 944) and a sample of inpatients (N = 425). Although the same personality traits (harm avoidance and self-directedness) were predominantly associated with burnout and depression, there was a much stronger association to depression than to burnout in both samples. Besides, we observed specific associations between personality traits and subcomponents of burnout. Our results underline differences in the association of burnout vs. depression to personality, which may mirror differences in scope. While symptoms of depression affect all aspects of life, burnout is supposed to be specifically related to the workplace and its requirements. The much stronger association of personality to depression can be important to select appropriate therapy methods and to develop a more specified treatment for burnout in comparison to depression.
Introduction
Work stress has been defined as occurring when the perceived job demands surpass employees’ resources to get their job done [e.g., Ref. (1)]. Among others, symptoms of permanent work stress include physiological consequences like increased risk for cardiovascular diseases [e.g., Ref. (2)], emotional consequences like mood disorders [e.g., Ref. (3)], or intellectual consequences like loss of attention [e.g., Ref. (4)]. Job stress-related affective problems, especially the burnout syndrome, have been a focus of research for years.
Freudenberger (5) and Maslach (6) were the first to investigate the burnout concept, which has [according to the three dimensions of the Maslach Burnout Inventory General (MBI-GS)] been defined as consisting of emotional exhaustion (job-related symptoms of fatigue), cynicism (indifferent or distant attitude toward the job), and reduced professional efficacy (individual expectations of continued effectiveness at work) (7). Although by now burnout has been identified in virtually all occupational groups, it is still not accepted as an autonomous diagnosis according to DSM or ICD. One of the major reasons for this is the uncertainty whether burnout is an independent disorder apart from depression. Research in this field has predominantly focused on possible distinctions between both concepts by use of factor analytic approaches (8, 9), by investigating the relationship between depression and facets of burnout [e.g., Ref. (10–12)], or by considering changes in the relationship of both dependent on progression (13) and severity (14) of the burnout syndrome.
An important factor, which has been associated with both burnout and depression, is personality [e.g., Ref. (15–17)]. For example, relations have been shown to the Big Five personality concept [positive correlations especially to neuroticism; e.g., Ref. (18, 19)], locus of control [positive correlation to external locus of control; e.g., Ref. (20–22)], or Cloninger’s biosocial model of personality [especially positive correlations with harm avoidance and negative correlations with self-directedness; e.g., Ref. (23, 24)]. Particularly, employees who display high levels of harm avoidance, an external locus of control, passive or defensive coping styles, low levels of hardiness, or poor self-esteem have been identified as vulnerable for burnout [compare Ref. (25)].
Based on the previous research and as the distinction between depression and burnout is still a matter of debate, the current study investigates whether burnout and depression can be differentiated by their relationship to personality. In this paper, we compare the relationship of Cloninger’s Temperament and Character Inventory [TCI; (26)] to burnout (as measured by the MBI) and to depression as measured by the Beck Depression Inventory 2 [BDI 2, (27)] in two independent samples. The first sample consists of 944 German employees, the second sample of 425 patients currently treated in psychosomatic clinics. Our aim is to find out whether the biologically oriented personality theory of Robert Cloninger is suitable to discriminate burnout from depression, and if putative differences between burnout and depression can be found in both the sample of healthy participants and the inpatient sample. Considering two independent samples, which are located in different regions of the health-illness continuum allows making statements about whether associations (and putative differences in association) between personality and depression or burnout, respectively, can be generalized.
To our knowledge, this is the first time that the MBI and the BDI 2 have been simultaneously related to Cloninger’s TCI in a large not occupationally specific sample. Therefore, a second aim of this paper is to replicate findings on the TCI/MBI relationship that have been reported for specific occupational groups [e.g., Ref. (28, 29)], which especially point out the relevance of harm avoidance and self-directedness for burnout.
Materials and Methods
Participants
We investigated two samples in this study: the first sample consisted of N = 944 German employees [362 male, M(age) = 41.0 years; 582 female, M(age) = 39.3 years] from a wide range of professions. The second sample included N = 425 inpatients [146 male, M(age) = 48.0 years; 279 female, M(age) = 47.54 years] from psychosomatic clinics. Both samples were recruited for the Bonn Burnout Research Project (BBRP). Written informed consent to participate was obtained prior to the study, which was approved by the local ethics committee at the University of Bonn. Information on participants’ medical and psychiatric background was collected by use of the SCL-90-R questionnaire (30).
Measures
Participants were recruited for a large scale project on the genetic and epigenetic causes of burnout. For the healthy sample, recruitment of participants was operationalized by contacting German companies spread over the whole country asking for allowance to invite their employees to take part in our research project and by randomly sent postal invitations to participate in the study to private households in the City of Bonn. Main goal was to include participants of diverse vocational backgrounds to obtain results, which are not restricted to a single profession and its specific characteristics. For the sample of patients, we collaborated with several psychosomatic hospitals spread across Germany, most of them belonging to the AHG consortium. The AHG comprises more than 40 hospitals and has an own research department that supported us in this scientific project. All participants completed a battery of questionnaires with separate sections for demographic information, personality (TCI), depression (BDI 2), and burnout (MBI). In case of the latter, we used the MBI-GS version, which allows measurement of burnout in different occupational groups.
The TCI is a seven-dimensional questionnaire consisting of the four temperaments novelty seeking (exploratory activity in response to novel stimulation, impulsive decision making, extravagance in approach to reward cues, quick loss of temper, and avoidance of frustration), harm avoidance (pessimism, shyness, excessive worrying, fearfulness, and easily fatigue), reward dependence (tendency to respond markedly to signals of reward and learning to maintain and pursue behaviors, which were previously associated with such reward), and persistence (perseverance in spite of fatigue or frustration) and the three character dimensions self-directedness (the perceived ability to regulate and adapt behavior to the demands of a situation in order to achieve personally chosen goals and values), cooperativeness (the degree to which a person is generally agreeable in their relations with other people as opposed to aggressively self-centered and hostile) and self-transcendence (the amount of experienced spiritual ideas) (26). According to Cloninger, the temperament dimensions are highly heritable and are based on the activity of the dopaminergic, serotonergic, and noradrenergic neurotransmitter system, while the character dimensions are closely related to environmental influences.
The MBI-GS is a measure for burnout in all professions. It consists of the three subscales: exhaustion (feelings of fatigue), cynicism (indifferent or distanced attitudes toward work), and professional efficacy (expectations of continued effectiveness at work). All of its questions ask specifically for experiences made in a work environment (e.g., “I feel used up at the end of a workday”; “In my opinion I am good at my job”).
Statistical Analysis
Initially, descriptive statistics and internal consistencies were calculated for all measures. Furthermore, the data of both samples were compared for significant differences. The relationships between the seven dimensions of the TCI and the MBI-GS or the BDI 2, respectively, were analyzed by means of correlations. Age was added as a control variable, and correlation coefficients were calculated separately for female and male participants and tested for significant differences. Furthermore, path models were calculated with the TCI subscales as exogenous variables and the MBI scores (we used a sum score as well as the three subscale scores) and the BDI 2 sum score as endogenous variables. Next to an unrestricted model, we tested restricted models assuming the same regression weights (path coefficients) for the relationship of a personality dimension to burnout and depression (e.g., harm avoidance → MBI = harm avoidance → BDI 2). This was done for each of the seven TCI dimensions (only one at a time) in order to test whether solutions with the same weights of personality dimensions for burnout and depression fit significantly worse, which would imply differences in the importance of the respective subscale for burnout vs. depression. Finally, a model comprising all individual constraints described above was tested (harm avoidance → MBI = harm avoidance → BDI 2 + novelty seeking → MBI = novelty seeking → BDI 2…) in order to test a model, which does not assume any differences in the relation of TCI dimensions to burnout vs. depression. As this model showed a significantly poorer fit for all comparisons in both samples, it is not considered further in depth. Models were fitted using the structural equation modeling software package AMOS (31). Compare Figure 1.
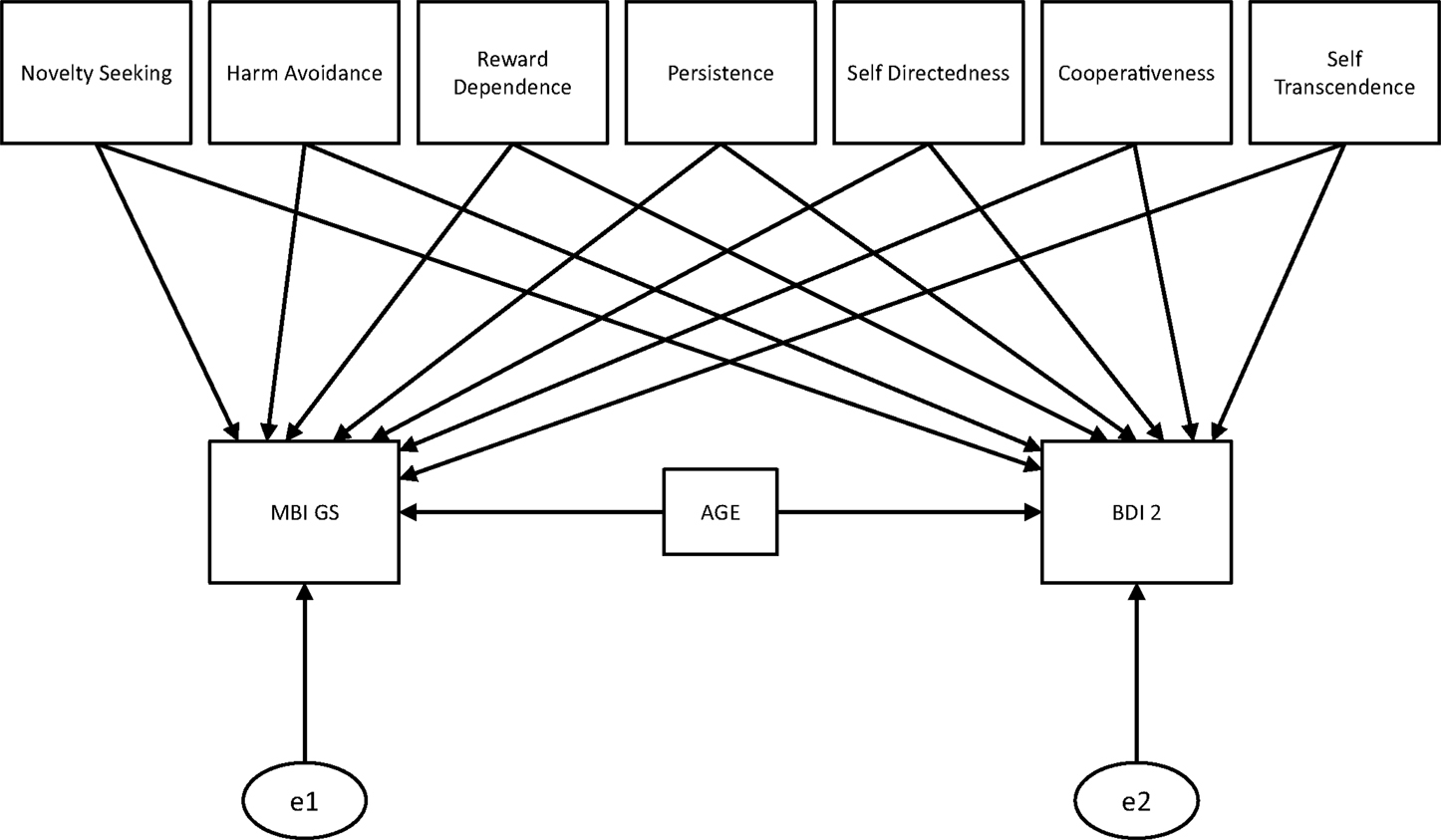
Figure 1. Path model without restrictions. Intercorrelation is expected between all seven dimensions of the TCI. All dimensions and age are used to predict participants values in MBI scores (sum score, and scores for exhaustion, efficacy, and cynicism) and BDI 2 scores. Next to this unrestricted model, models, which assume the same regression weights between a TCI dimension and burnout/depression, were tested. Finally, a model assuming the same regression weights for all TCI-scales was tested.
Results
Questionnaires and Control Variables
Means, SDs, sample comparison, and Cronbach’s alpha of participants’ questionnaire responses are depicted in Table 1. Our results fit nicely with normative data on responses to the TCI (32), the BDI 2 (33), and the MBI (34) in German samples.
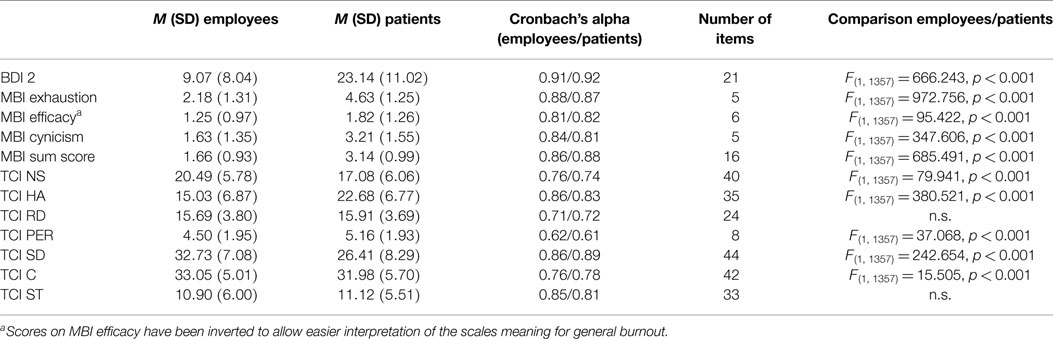
Table 1. Means and SDs of employed participants’ (N = 944) and patients’ (N = 425) questionnaire responses plus reliability (coefficients in terms of Cronbach’s alpha) of the used scales are presented.
After correction for age, comparison of the questionnaire responses of both samples delivered significant results for all measures except reward dependence and self-transcendence.
Relation of Burnout, Depression, and TCI
Table 2 shows the correlations between all questionnaire measures for the healthy and the inpatient sample.
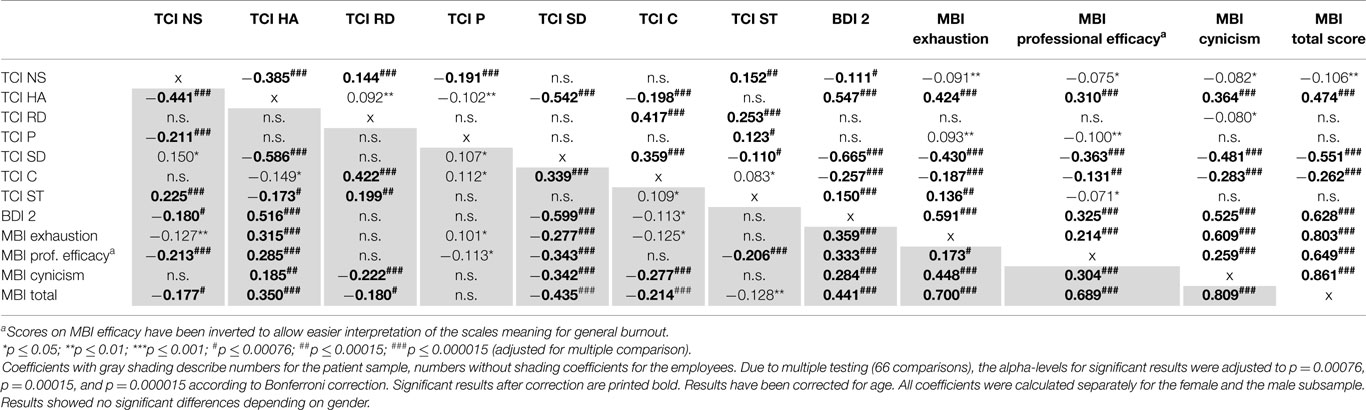
Table 2. Correlations of TCI, BDI 2, and MBI-GS.
Harm avoidance exhibited a medium to large size positive correlation to burnout as well as to depression. Self-directedness and (to a lesser extent in case of the patients) cooperativeness were negatively related to burnout and depression. Novelty seeking, reward dependence, persistence, and self-transcendence revealed very small correlations to both constructs, which in most cases were not significant after Bonferroni correction. Depression and burnout in turn displayed medium to large size correlations (professional efficacy exhibited a much smaller relation to depression than the other two subscales of the MBI-GS in case of the employee sample). Most interestingly, relations between burnout and depression were much smaller in the patient sample compared to the employee sample. There were no significant differences in size of correlations depending on gender for any measure in both samples.
Path Model Analyses
Table 3 represents the path estimations of the path model for BDI 2 and the scores of the MBI-GS (sum score, exhaustion, professional efficacy, and cynicism).
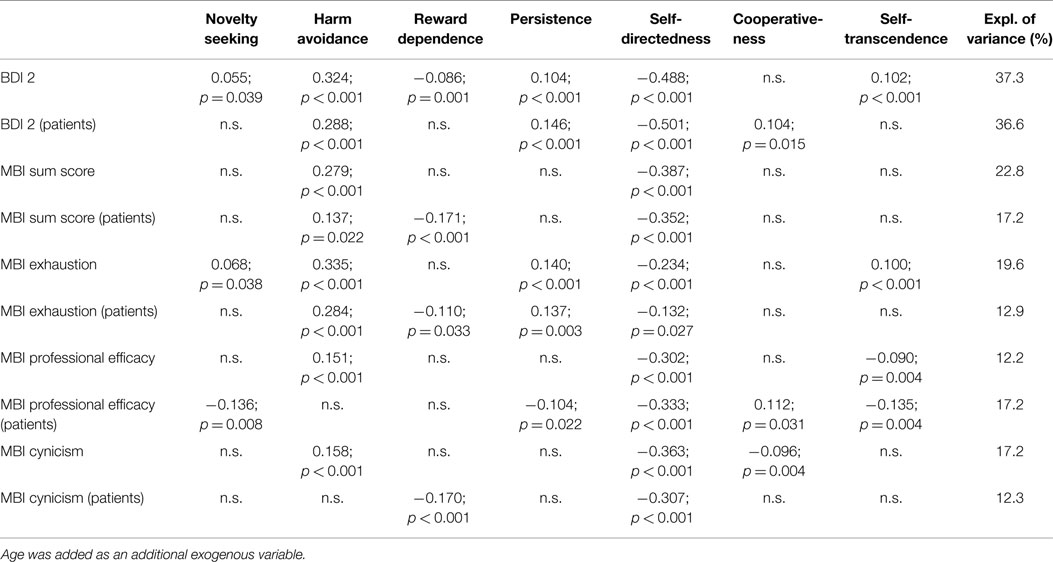
Table 3. Estimated standardized regression weights between the seven TCI dimensions and burnout/depression in the unrestricted model.
With exception of exhaustion in case of the employee sample, low self-directedness turned out to be the by far most important path with up to 25.1% (BDI 2) of explained variance (squared path coefficient). The second most important predictor was high harm avoidance with up to 11.2% explained variance (MBI exhaustion). Overall, the TCI was able to explain much more variance in depression than in burnout.
Results of the model comparison between the restricted and the unrestricted models (for BDI 2 vs. MBI sum score) are shown in Tables 4 and 5. Here, we stepwise set all paths between a TCI dimension and burnout/depression invariant one after another (but only one at a time). Results show that, especially in case of self-directedness, but also in case of harm avoidance, persistence, and self-transcendence, the models assuming differences in paths to burnout and depression fit significantly better to the data than the restricted models (equality constraints), which means we can assume that in these cases the relationship of the respective TCI scale to burnout is significantly smaller than the one to depression. For reward dependence, the difference between depression and burnout is only significant for the employee sample, while in case of cooperativeness the same is true for the patient sample. We performed the same model comparisons for depression vs. the MBI subscales (e.g., BDI 2 vs. exhaustion) as well as within the MBI subscales (e.g., exhaustion vs. cynicism). The summarized results are presented in Tables 6 and 7.
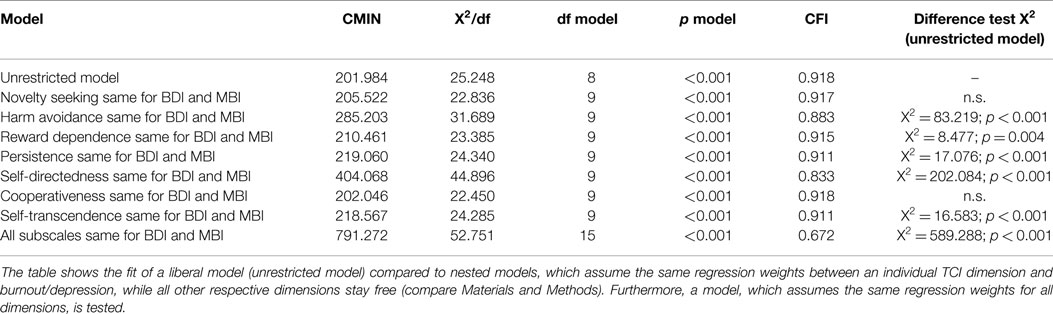
Table 4. Results of the path analyses comparing MBI sum score and BDI 2 for the employee sample.
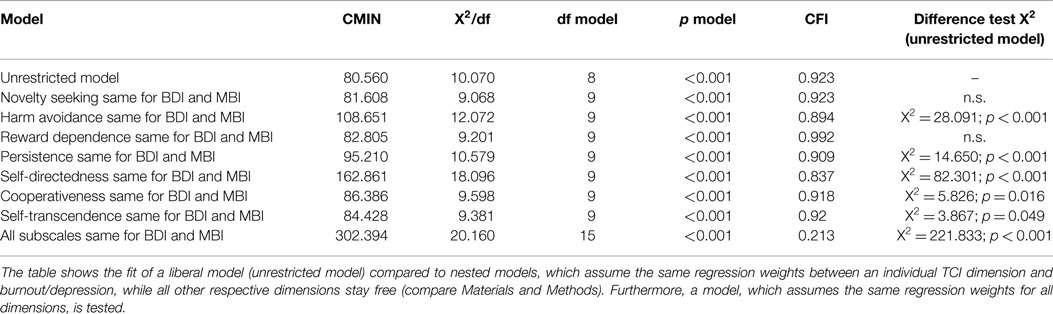
Table 5. Results of the path analyses comparing MBI sum score and BDI 2 for the patient sample.
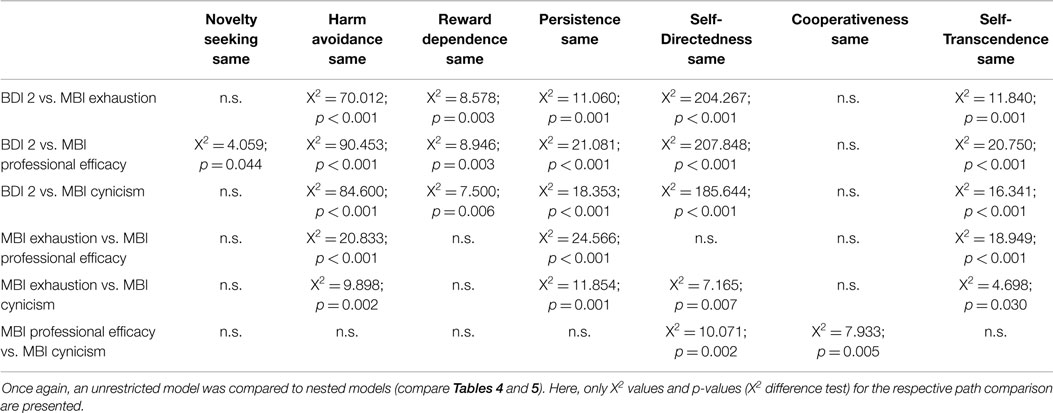
Table 6. Results of the path analyses comparing MBI subscale scores with each other and with the BDI 2 (employee sample).
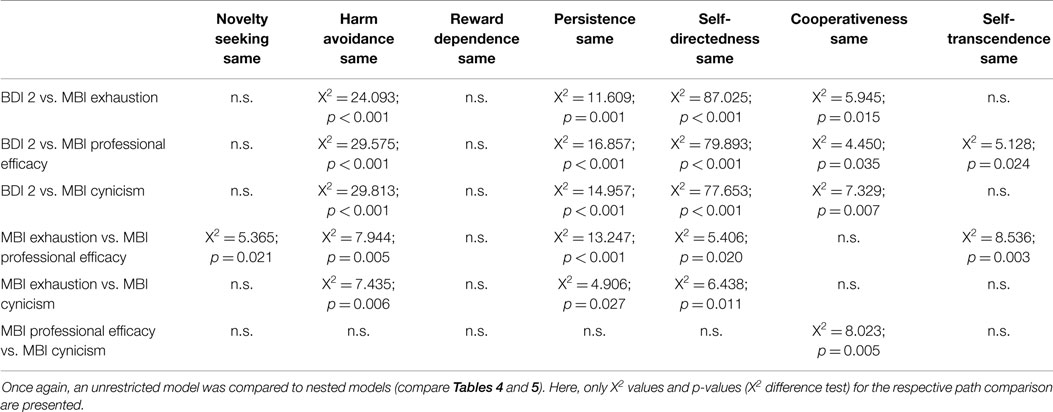
Table 7. Results of the path analyses comparing MBI subscale scores with each other and with the BDI 2 (patient sample).
The analyses once again emphasize the bigger relevance of self-directedness and harm avoidance for depression compared to the three subscales of the MBI. The only exceptions to this are the BDI 2 vs. MBI exhaustion comparisons in case of harm avoidance and persistence (employee sample) as well as the BDI 2 vs. MBI professional efficacy comparison in case of self-transcendence (patient sample). The internal comparison of the subscales of the MBI provides fewer significant results concerning differences in relation to the TCI. Most prominent in this case is the difference in relation between persistence and exhaustion or professional efficacy, respectively. Here, persistence seems especially relevant for prediction of MBI exhaustion.
Discussion
The present study investigated the relationship of Cloninger’s biosocial model of personality (TCI) to burnout (MBI) and depression (BDI 2) in a sample of German employees from various professions and in an independent sample of patients from psychosomatic hospitals. Based on evidence from preceding studies, we expected predominance of the TCI’s subscales harm avoidance and self-directedness to predict participants’ self-reported levels of burnout and depression. Furthermore, we searched for putative differences in the relationship between personality and depression vs. personality and burnout, which we wanted to replicate in two samples of participants with varying degrees of emotional stress.
The descriptive data (Table 1) shows that the employees’ responses to the TCI overall match normative data for the TCI. If we compare our data to the score categorizations (severity of burnout/depression), which have been suggested for the BDI 2 [compare Ref. (27)] and the MBI-GS [compare Ref. (7)], it is evident that our control sample on average exhibits an exposure to depression and burnout. The mean BDI 2 score would be classified as a “minimal depression.” MBI exhaustion and cynicism scores would be classified as “moderate exposure to burnout” or middle third in range of experienced burnout. Notably, these results are primarily driven by a minority of employees with very high scores in depression (2.2% with severe depression and 7.7% with a medium depression) or burnout (17–20% high exposure to burnout on all three subscales). This rather high number of active employees with clinical depression or strong exposure to burnout should be considered in future research and in the development and implementation of prevention programs concerned with affective disorders. As expected, we see a much higher exposure to depression and burnout in the patient sample compared to the employees. Here, the mean BDI 2 score would be classified as a moderate depression, while scores concerning the MBI would be classified as high exposure in case of exhaustion and cynicism and as moderate exposure in case of professional efficacy.
Results of the correlations and path models fit nicely with our expectations: more than one-third of the BDI 2’s variance can be explained by the TCI’s subscales in both samples, with self-directedness and harm avoidance as the by far most important predictors. Prediction of the MBI subscales reveals a similar pattern for the employee sample: once again, self-directedness and harm avoidance are the most important factors to explain the subscales. All other dimensions of the TCI only play a subordinate role in explaining MBI values. Therefore, our study confirms findings from previous studies, which found strong relations between self-directedness/harm avoidance and burnout in specific (healthy) occupational groups. Out of a personality theory perspective, this result is quite interesting because harm avoidance is a temperament dimension, which according to Cloninger et al. (26) originates mainly from genetic–biological causes while self-directedness is a character dimension, which originates primarily from environmental influences, indicating a gene–environment interaction in the association between personality and depression/burnout. Furthermore, although harm avoidance shares some aspects of its definition with depression and to a lesser extend with burnout, overall self-directedness proved to be the more important predictor. In case of the patient sample, results are a little bit more mixed up concerning prediction of the MBI subscales. Here, persistence and reward dependence play a more important role, while the importance of harm avoidance decreases.
A crucial difference between MBI and BDI 2 is the overall amount of variance explained by the respective model: for exhaustion, the TCI explains 19.6%/12.9% of variance, for MBI cynicism 17.2%/12.3%, and for MBI professional efficacy 12.2%/17.2%. Even for the total burnout score, the amount of explained variance (22.8%/17.2%) does not reach values of the BDI 2 (37.3%/36.6%). Obviously, prediction of participants’ burnout-scores is considerably less efficient than prediction of scores in depression, which means that there is a closer relation of the TCI personality concept to depression than to burnout. A possible explanation for this finding could be differences in the controllability of workplace environment conditions vs. private environment conditions: workplace stress (which is supposed to be the major stressor in burnout) differs from personal or environmental stress (which is a major stressor in depression) in such a way that workplace environment offers fewer opportunities to influence framework conditions than personal environment because conditions in the workplace are more predefined than those in private life (14). Individual personality characteristics can have positive or negative effects on the risk for developing an affective disorder, because they influence adaptive or maladaptive behaviors and also internal coping strategies [e.g., Ref. (35, 36)]. This influence can be much more effective if the particular environment offers enough degrees of freedom (for behavior, choices, etc.) to alter the conducive or obstructive environmental conditions by use of personality-specific (adaptive or maladaptive) behavior. Therefore, the fewer degrees of freedom in case of burnout relevant environment compared to depression relevant environment can explain the differences in the strength of association of personality with burnout vs. depression that we found in our study. A second argument concerns potential overlapping genetic influences. It has been shown that depression [e.g., Ref. (37)] as well as personality [e.g., Ref. (38)] is to a substantial amount influenced by genetic makeup. Although there is first evidence that genetic influences are also relevant for burnout [e.g., Ref. (39)], estimations for their effect are significantly lower than in case of depression or personality. Therefore, a second explanation for our findings could be the bigger (and potentially shared) amount of genetic influences for personality and depression.
The differences in explained variance between the subscales of the MBI might reflect differences between the MBI subscales, which have been discussed before in the literature. For example, the positive phrasing of professional efficacy as opposed to the negative phrasing of the other two subscales has been discussed as a cause for differences, because direction of phrasing influences response patterns in the MBI (40). Furthermore, alternative MBI-GS models with an inefficacy scale instead of an efficacy scale exhibit an improved factor structure and higher correlations to the other two subscales (41, 42). A distinction between professional efficacy and the other two subscales of the MBI is also suggested by results concerning the MBI-GS’s factor structure [e.g., Ref. (43–45)].
The comparison of the different prediction models for depression and burnout (compare Tables 4 and 5 and Tables 6 and 7) yields interesting results concerning the relevance of the TCI subscales. First of all, results demonstrate that neither novelty seeking nor cooperativeness play a noteworthy role for the prediction of depression and burnout. Self-directedness on the other hand is the best predictor for both depression and the MBI sum score, but at the same time, its association with the subscales of burnout is rather uneven. For example, self-directedness displays a stronger association to cynicism and professional efficacy than to exhaustion. This also applies to harm avoidance (stronger association to exhaustion than to professional efficacy and cynicism) indicating that the strength of association with both scales might help to distinguish depression from burnout. Finally, the results concerning persistence and reward dependence are interesting. Here, persistence seems especially related to MBI exhaustion but not to the other two subscales of the MBI, which makes perfectly sense as high persistence implies high performance over a long time, which may lead to exhaustion. Reward dependence on the other hand seems to play a role for prediction of burnout in patients, but not in the employee sample. Overall, the latter differences, however, are not of great importance in proportion to the predominating effects of self-directedness and harm avoidance.
In summary, the following picture emerges: self-directedness and harm avoidance are the predominantly associated TCI dimensions for depression as well as for burnout, and this seems true for occupation homogenous samples as well as for groups of mixed occupations. In case of patients, the meaning of harm avoidance seems to be less important. Depression has a much closer relationship to the TCI personality concept than burnout. This difference is once again mainly driven by self-directedness and harm avoidance. There is no personality dimension that shows a strong specific association with either burnout or depression exclusively. Finally, persistence and in case of the patient sample reward dependence seem suited to distinguish between subscales of the MBI.
Our results may have an important impact on choosing the best therapy for depressive vs. burned-out patients. For example, in psychotherapy, personality characteristics have been found to be relevant for interpersonal processes [e.g., Ref. (46)] or learned helplessness [e.g., Ref. (47)]. If depression is much closer related to personality than burnout, consideration of personality-related therapy blocks (like training of positive self-efficacy expectancy for patients with low self-directedness or training to reduce rumination in patients with high harm avoidance) may be important in case of depressive disorders. In case of burnout, other methods (like training of physical stress relief) might fit better to reach the optimal therapeutic success. In order to develop therapy methods, which are adjusted to the specific symptoms of depression and burnout, future studies should also focus on potential biological factors, which differentiate between both diseases. This approach of disentangling psychological concepts by differences in their biological bases has been applied very successful in other areas of psychiatry [compare, for example, Ref. (48)]. Potential areas of study could, for example, be genetic or epigenetic differences, functional differences, differences in transmitter or hormone activity, or structural brain differences.
We have to point out that our study has some limitations. First of all, although we checked for demographic characteristics, we cannot exclude the possibility that our sample includes a selection bias. It is possible that employees with specific characteristics (e.g., specific opinion on or experiences with burnout) are more willing to participate in a study on burnout than others. Furthermore, our data are cross-sectional. A longitudinal design would allow checking for causal pathways. Especially, predictions on first-time employees’ psychic health development and proneness to burnout and depression depending on personality would be of interest. Our current cross-sectional approach involves the risk of underestimating the influence of personality, as burnout develops gradually throughout working life and younger employees with burnout- or depression-prone personality characteristics might not yet be affected. Besides, although personality is defined as rather stable over the life span, research has shown that psychiatric diseases have a tremendous effect on personality self-reports. It can be assumed that the severity of illness is reflected in the extremeness of responses on personality scales in our data. Due to the cross-sectional character of our study, we cannot disentangle causal effects of depression/burnout on personality or vice versa. However, many researchers and clinicians are of the opinion that burnout is a prodromal syndrome of depression, i.e., the strength of the association between personality and burnout/depression can reflect such a process model. A related aspect concerns potential prior depressive or burnout episodes, which could also influence questionnaire responses. For future studies, it could be useful to assess number and duration of these prior episodes to control for their putative influence on questionnaire responses. Finally, it could be useful to replicate and validate the results that we found in our study by alternative assessment tools that do not rely on self-report data because self-report data may be prone to some psychometric disadvantages. Nevertheless, self-report measures have indeed their justification and are therefore applied in countless studies and in clinical settings. Especially, the BDI 2 has become a sort of golden standard in the diagnosis of depression. Moreover, several studies have demonstrated high convergent validity between the BDI 2 and standardized psychiatric interviews [for example, to the SCID-I, r = 0.083; e.g., Ref. (49, 50)].
Author Contributions
All authors agreed on the study design and helped collecting and organizing the data for this study. Separate drafts for parts of the manuscript were written by all authors. All authors read and corrected the manuscript. MM managed the literature searches, performed the statistical analyses, and wrote the final manuscript. All authors contributed to and have approved to the final manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the Daimler Benz Foundation (Ladenburg, Germany) who financed this study by a grant [00-01/12]. Furthermore, we want to thank the colleagues who helped collecting the data for the clinical sample. In particular, we thank (in alphabetical order) Dr. Jürgen Borgart (AHG Hospital Bad Pyrmont, Germany), Dr. Mario Gartmann (AHG Hospital Bad Dürkheim, Germany), Dr. Michael Rolffs (AHG Hospital Daun, Germany), and Dr. Albrecht Schumacher (AHG Hospital Waren, Germany) for organizing the data collection in the respective psychosomatic hospitals.
References
1. Folkman S, Lazarus RS, Pimley S, Novacek J. Age differences in stress and coping processes. Psychol Aging (1987) 2:171–84. doi: 10.1037/0882-7974.2.2.171
2. Vrijkotte TG, van Doornen LJ, de Geus EJ. Effects of work stress on ambulatory blood pressure, heart rate, and heart rate variability. Hypertension (2000) 35(4):880–6. doi:10.1161/01.HYP.35.4.880
3. Duman RS, Monteggia LM. A neurotrophic model for stress-related mood disorders. Biol Psychiatry (2006) 59(12):1116–27. doi:10.1016/j.biopsych.2006.02.013
4. Linden DVD, Keijsers GP, Eling P, Schaijk RV. Work stress and attentional difficulties: an initial study on burnout and cognitive failures. Work Stress (2005) 19(1):23–36. doi:10.1080/02678370500065275
5. Freudenberger HJ. Staff burn-out. J Soc Issues (1974) 30(1):159–65. doi:10.1111/j.1540-4560.1974.tb00706.x
7. Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory Manual. 3rd ed. Palo Alto, CA: Consulting Psychologists Press (1996).
8. Leiter MP, Durup J. The discriminant validity of burnout and depression: a confirmatory factor analytic study. Anxiety Stress Coping (1994) 7(4):357–73. doi:10.1080/10615809408249357
9. Shirom A, Ezrachi Y. On the discriminant validity of burnout, depression and anxiety: a re-examination of the burnout measure. Anxiety Stress Coping (2003) 16(1):83–97. doi:10.1080/1061580021000057059
10. Glass DC, McKnight JD. Perceived control, depressive symptomatology, and professional burnout: a review of the evidence. Psychol Health (1996) 11(1):23–48. doi:10.1080/08870449608401975
11. Nyklíček I, Pop VJ. Past and familial depression predict current symptoms of professional burnout. J Affect Disord (2005) 88(1):63–8. doi:10.1016/j.jad.2005.06.007
12. Peterson U, Demerouti E, Bergström G, Samuelsson M, Asberg M, Nygren A. Burnout and physical and mental health among Swedish healthcare workers. J Adv Nurs (2008) 62(1):84–95. doi:10.1111/j.1365-2648.2007.04580.x
13. Ahola K, Honkonen T, Isometsä E, Kalimo R, Nykyri E, Aromaa A, et al. The relationship between job-related burnout and depressive disorders – results from the finnish health 2000 study. J Affect Disord (2005) 88(1):55–62. doi:10.1016/j.jad.2005.06.004
14. Iacovides A, Fountoulakis KN, Kaprinis S, Kaprinis G. The relationship between job stress, burnout and clinical depression. J Affect Disord (2003) 75(3):209–21. doi:10.1016/S0165-0327(02)00101-5
15. Alarcon G, Eschleman KJ, Bowling NA. Relationships between personality variables and burnout: a meta-analysis. Work Stress (2009) 23(3):244–63. doi:10.1080/02678370903282600
16. Enns MW, Cox BJ. Personality dimensions and depression: review and commentary. Can J Psychiatry (1997) 42(3):274–84.
17. Swider BW, Zimmerman RD. Born to burnout: a meta-analytic path model of personality, job burnout, and work outcomes. J Vocat Behav (2010) 76(3):487–506. doi:10.1016/j.jvb.2010.01.003
18. Bakker AB, Van Der Zee KI, Lewig KA, Dollard MF. The relationship between the big five personality factors and burnout: a study among volunteer counselors. J Soc Psychol (2006) 146(1):31–50. doi:10.3200/SOCP.146.1.31-50
19. Klein DN, Kotov R, Bufferd SJ. Personality and depression: explanatory models and review of the evidence. Annu Rev Clin Psychol (2011) 7:269–95. doi:10.1146/annurev-clinpsy-032210-104540
20. De Hoogh AH, Den Hartog DN. Neuroticism and locus of control as moderators of the relationships of charismatic and autocratic leadership with burnout. J Appl Psychol (2009) 94(4):1058–67. doi:10.1037/a0016253
21. Gray-Stanley JA, Muramatsu N, Heller T, Hughes S, Johnson TP, Ramirez-Valles J. Work stress and depression among direct support professionals: the role of work support and locus of control. J Intellect Disabil Res (2010) 54(8):749–61. doi:10.1111/j.1365-2788.2010.01303.x
22. Wang Q, Bowling NA, Eschleman KJ. A meta-analytic examination of work and general locus of control. J Appl Psychol (2010) 95(4):761–8. doi:10.1037/a0017707
23. Cloninger CR, Svrakic DM, Przybeck TR. Can personality assessment predict future depression? A twelve-month follow-up of 631 subjects. J Affect Disord (2006) 92(1):35–44. doi:10.1016/j.jad.2005.12.034
24. Stoyanov DS, Cloninger CR. Relation of people-centered public health and person-centered healthcare management: a case study to reduce burn-out. Int J Pers Cent Med (2012) 2(1):90–5.
25. Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol (2001) 52:397–422. doi:10.1146/annurev.psych.52.1.397
26. Cloninger CR, Svrakic DM, Przybeck TR. A psychobiological model of temperament and character. Arch Gen Psychiatry (1993) 50:975–90. doi:10.1001/archpsyc.1993.01820240059008
27. Beck AT, Steer RA, Brown GK. Beck Depression Inventory Manual. 2nd ed. San Antonio, TX: Psychological Corporation (1996).
28. Isaksson U, Graneheim UH, Richter J, Eisemann M, Åström S. Exposure to violence in relation to personality traits, coping abilities, and burnout among caregivers in nursing homes: a case-control study. Scand J Caring Sci (2008) 22(4):551–9. doi:10.1111/j.1471-6712.2007.00570.x
29. Pejušković B, Lečić-Toševski D, Priebe S, Tošković O. Burnout syndrome among physicians-the role of personality dimensions and coping strategies. Psychiatr Danub (2011) 23(4):389–95.
30. Derogatis LR. SCL-90-R: Symptom Checklist-90-R: Administration, Scoring, and Procedures Manual. Bloomington, IL: NCS Pearson (1996).
32. Richter J, Eisemann M, Richter G. Zur deutschsprachigen Version des Temperament-und Charakterinventars. Z Klin Psychol Psychother (2000) 29(2):117–26. doi:10.1026//0084-5345.29.2.117
33. Kühner PDC, Bürger C, Keller F, Hautzinger M. Reliabilität und Validität des revidierten Beck-Depressionsinventars (BDI-II). Nervenarzt (2007) 78:651–6. doi:10.1007/s00115-006-2098-7
34. Büssing A, Perrar KM. Die Messung von burnout. Untersuchung einer deutschen Fassung des Maslach burnout Inventory (MBI-D). Diagnostica (1992) 38:4.
35. Carver CS, Connor-Smith J. Personality and coping. Annu Rev Psychol (2010) 61:679–704. doi:10.1146/annurev.psych.093008.100352
36. Connor-Smith JK, Flachsbart C. Relations between personality and coping: a meta-analysis. J Pers Soc Psychol (2007) 93(6):1080–107. doi:10.1037/0022-3514.93.6.1080
37. Sullivan PF, Neale MC, Kendler KS. Genetic epidemiology of major depression: review and meta-analysis. Genet Epidemiol (2000) 157(10):1552–62. doi:10.1176/appi.ajp.157.10.1552
38. Bouchard TJ Jr, Loehlin JC. Genes, evolution, and personality. Behav Genet (2001) 31(3):243–73. doi:10.1023/A:1012294324713
39. Blom V, Bergström G, Hallsten L, Bodin L, Svedberg P. Genetic susceptibility to burnout in a Swedish twin cohort. Eur J Epidemiol (2012) 27(3):225–31. doi:10.1007/s10654-012-9661-2
40. Bouman AM, te Brake HT, Hoogstraten J. Significant effects due to rephrasing the Maslach burnout inventory’s personal accomplishment items. Psychol Rep (2002) 91(3):825–6. doi:10.2466/pr0.2002.91.3.825
41. Bresó E, Salanova M, Schaufeli WB. In search of the “third dimension” of burnout: efficacy or inefficacy? Appl Psychol (2007) 56(3):460–78. doi:10.1111/j.1464-0597.2007.00290.x
42. Schaufeli WB, Salanova M. Efficacy or inefficacy, that’s the question: burnout and work engagement, and their relationships with efficacy beliefs. Anxiety Stress Coping (2007) 20(2):177–96. doi:10.1080/10615800701217878
43. Bakker AB, Demerouti E, Schaufeli WB. Validation of the Maslach burnout inventory-general survey: an internet study. Anxiety Stress Coping (2002) 15(3):245–60. doi:10.1080/1061580021000020716
44. Kitaoka-Higashiguchi K, Nakagawa H, Morikawa Y, Ishizaki M, Miura K, Naruse Y, et al. Construct validity of the Maslach burnout inventory-general survey. Stress Health (2004) 20(5):255–60. doi:10.1002/smi.1030
45. Taris TW, Schreurs PJ, Schaufeli WB. Construct validity of the Maslach burnout inventory-general survey: a two-sample examination of its factor structure and correlates. Work Stress (1999) 13(3):223–37. doi:10.1080/026783799296039
46. Kiesler D. Contemporary Interpersonal Theory and Research: Personality, Psychopathology, and Psychotherapy. Hoboken, NJ: Wiley & Sons (1996).
47. Cemalcilar Z, Canbeyli R, Sunar D. Learned helplessness, therapy, and personality traits: an experimental study. J Soc Psychol (2003) 143(1):65–81. doi:10.1080/00224540309598431
48. Straub RH. Systemic disease sequelae in chronic inflammatory diseases and chronic psychological stress: comparison and pathophysiological model. Ann N Y Acad Sci (2014) 1318(1):7–17. doi:10.1111/nyas.12409
49. Sprinkle SD, Lurie D, Insko SL, Atkinson G, Jones GL, Logan AR, et al. Criterion validity, severity cut scores, and test-retest reliability of the Beck depression inventory-II in a university counseling center sample. J Couns Psychol (2002) 49(3):381–5. doi:10.1037/0022-0167.49.3.381
Keywords: TCI, depression, burnout, path analyses, MBI-GS, BDI 2
Citation: Melchers MC, Plieger T, Meermann R and Reuter M (2015) Differentiating burnout from depression: personality matters! Front. Psychiatry 6:113. doi: 10.3389/fpsyt.2015.00113
Received: 03 June 2015; Accepted: 27 July 2015;
Published: 13 August 2015
Edited by:
Michael Noll-Hussong, University of Ulm, GermanyReviewed by:
Jürg Kesselring, Rehabilitation Centre Valens, SwitzerlandKarl Bechter, University of Ulm, Germany
Copyright: © 2015 Melchers, Plieger, Meermann and Reuter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martin Christoph Melchers, Department of Psychology, University of Bonn, Kaiser-Karl-Ring 9, Bonn D-53111, Germany, martin.melchers@uni-bonn-diff.de