 Fabrizio Carinci1*
Fabrizio Carinci1* Iztok Štotl2,3
Iztok Štotl2,3 Scott G. Cunningham4
Scott G. Cunningham4 Tamara Poljicanin5
Tamara Poljicanin5 Ivan Pristas5Vivie Traynor6George Olympios6
Ivan Pristas5Vivie Traynor6George Olympios6 Vasos Scoutellas6,7Joseph Azzopardi8Kris Doggen9
Vasos Scoutellas6,7Joseph Azzopardi8Kris Doggen9 János Sandor10
János Sandor10 Roza Adany10Karianne F. Løvaas11Przemka Jarosz-Chobot12
Roza Adany10Karianne F. Løvaas11Przemka Jarosz-Chobot12 Joanna Polanska13
Joanna Polanska13 Simion Pruna14
Simion Pruna14 Simon de Lusignan15Marcello Monesi16,17Paolo Di Bartolo17,18
Simon de Lusignan15Marcello Monesi16,17Paolo Di Bartolo17,18 Christa Scheidt-Nave19Christin Heidemann19Inbar Zucker20,21Anita Maurina22Jana Lepiksone22
Christa Scheidt-Nave19Christin Heidemann19Inbar Zucker20,21Anita Maurina22Jana Lepiksone22 Peter Rossing23Martti Arffman24Ilmo Keskimäki24,25Soffia Gudbjornsdottir26Concetta Tania Di Iorio27Elisabeth Dupont28Stella de Sabata28Niek Klazinga29Massimo Massi Benedetti28,30
Peter Rossing23Martti Arffman24Ilmo Keskimäki24,25Soffia Gudbjornsdottir26Concetta Tania Di Iorio27Elisabeth Dupont28Stella de Sabata28Niek Klazinga29Massimo Massi Benedetti28,30- 1Department of Statistical Sciences, University of Bologna, Bologna, Italy
- 2Department of Endocrinology, Diabetes and Metabolic Diseases, University Medical Centre Ljubljana, Ljubljana, Slovenia
- 3Faculty of Medicine, University of Ljubljana, Ljubljana, Slovenia
- 4Department of Population Health and Genomics, University of Dundee, Dundee, United Kingdom
- 5Division for Health Informatics and Biostatistics, Croatian Institute of Public Health, Zagreb, Croatia
- 6Diabetes Department, Larnaca Hospital Cyprus, Larnaca, Cyprus
- 7Health Monitoring Unit, Ministry of Health, Nicosia, Cyprus
- 8Department of Medicine, University of Malta, Msida, Malta
- 9Health Services Research, Sciensano, Brussels, Belgium
- 10Department of Public Health and Epidemiology, School of Health Sciences, University of Debrecen, Debrecen, Hungary
- 11Norwegian Diabetes Register for Adults, Norwegian Organisation for Quality Improvement of Laboratory Examinations (Noklus), Haraldsplass Deaconess Hospital, Bergen, Norway
- 12Department of Children’s Diabetology, Medical University of Silesia, Katowice, Poland
- 13Department of Data Science and Engineering, The Silesian University of Technology, Gliwice, Poland
- 14Telemedica Consulting, Bucharest, Romania
- 15Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, United Kingdom
- 16Diabetes Unit “Sant’Anna” Hospital Ferrara, Ferrara, Italy
- 17Associazione Medici Diabetologi (AMD), Rome, Italy
- 18Azienda Unità Sanitaria Locale (AUSL) Diabetes Unit Romagna, Ravenna, Italy
- 19Department of Epidemiology and Health Monitoring, Robert Koch Institute, Berlin, Germany
- 20Israel Center for Disease Control, Ministry of Health, Ramat Gan, Israel
- 21Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
- 22Research and Health Statistics Department, Centre for Disease Prevention and Control of Latvia, Riga, Latvia
- 23Steno Diabetes Center Copenhagen, Gentofte, Denmark
- 24Welfare State Research and Reform Unit, Finnish Institute for Health and Welfare (THL), Helsinki, Finland
- 25Faculty of Social Sciences, Tampere University, Tampere, Finland
- 26Department of Molecular and Clinical Medicine, University of Gothenburg and Sahlgrenska Hospital, Gothenburg, Sweden
- 27Serectrix snc, Pescara, Italy
- 28International Diabetes Federation European Region, Brussels, Belgium
- 29Department of Public and Occupational Health, Amsterdam UMC, Amsterdam Public Health Research Institute, Amsterdam, Netherlands
- 30Hub for International Health Research, Perugia, Italy
Background: Registries and data sources contain information that can be used on an ongoing basis to improve quality of care and outcomes of people with diabetes. As a specific task of the EU Bridge Health project, we carried out a survey of diabetes-related data sources in Europe.
Objectives: We aimed to report on the organization of different sources of diabetes information, including their governance, information infrastructure and dissemination strategies for quality control, service planning, public health, policy and research.
Methods: Survey using a structured questionnaire to collect targeted data from a network of collaborating institutions managing registries and data sources in 17 countries in the year 2017.
Results: The 18 data sources participating in the study were most frequently academic centres (44.4%), national (72.2%), targeting all types of diabetes (61.1%) covering no more than 10% of the target population (44.4%). Although population-based in over a quarter of cases (27.8%), sources relied predominantly on provider-based datasets (38.5%), fewer using administrative data (16.6%). Data collection was continuous in the majority of cases (61.1%), but 50% could not perform data linkage. Public reports were more frequent (72.2%) as well as quality reports (77.8%), but one third did not provide feedback to policy and only half published ten or more peer reviewed papers during the last 5 years.
Conclusions: The heterogeneous implementation of diabetes registries and data sources hampers the comparability of quality and outcomes across Europe. Best practices exist but need to be shared more effectively to accelerate progress and deliver equitable results for people with diabetes.
Introduction
The continuous use of comparative health indicators (1) may effectively improve quality of care and outcomes by using targeted strategies including monitoring, benchmarking, audit and feedback (2). Specific experiences show that such approaches work particularly well in diabetes (3), although there is still no general consensus regarding best practices for the design of registries and information systems (4). For this reason, their adoption on a national level still seems quite limited (5).
As a result, many countries use different data sources for the production of indicators at national, regional or provider level (6). This hampers the implementation of common platforms (7) and make international comparisons particularly challenging (8).
To overcome the problem, the European Commission financed specific initiatives addressing the comparability of diabetes indicators across Member States (MS) (9). Between 2004-2017, the EU Directorate of Health and Consumers (DG-SANCO) co-funded three consecutive projects run by the EUBIROD network (10), a coalition of centres maintaining diabetes registries and data sources in 18 countries (11, 12). The aim of the network was to implement common data standards using a federated approach for the systematic production of evidence-based diabetes indicators (11, 13).
In 2012, the network delivered the first fully automated international report using novel distributed analytical software (14). Between 2013-16, the method was further refined as a general platform for the calculation of EU health indicators across all chronic diseases (15).
In 2017, as part of the EU project Bridge Health (16), we carried out a qualitative survey of diabetes registries and data sources in Europe, with the aim of evaluating their organization in terms of coordination, geographical coverage, governance and information infrastructure.
In the present study, we will report the main results emerging from the survey and discuss the availability of comparable diabetes indicators across Europe, on the basis of methodological requirements identified by our previous international projects.
Materials and Methods
The present study was conducted as part of WP Task 8.2 of Bridge Health (16, 17), a EU co-funded project aimed at defining an overarching framework for the EU Health Information System, run between May 2015 - November 2017. The coordination of this work was facilitated by the Hub for International Health Research (HIRS) and subcontractor Serectrix snc., in collaboration with the EUBIROD network.
The task started with the delivery of a scoping report, presenting the state of the art of 12 collaborating registries and data sources at the first general assembly of the EUBIROD network, held at the University of Surrey, Guildford, UK, 24-25th August 2015. In this session, partners discussed the information collected so far, agreeing to carry out a qualitative survey to collect more structured information on the contents of data sources, through the use of a targeted questionnaire. The details of the instrument were agreed at the first investigators’ meeting, held in Rome on 24-25th November 2015 (http://www.eubirod.eu/projects/bridge/meetings/rome2015/).
The questionnaire was finalised by the coordinating team and shared with all partners before the second meeting. The final structure of the survey questionnaire is shown in (Table 1).
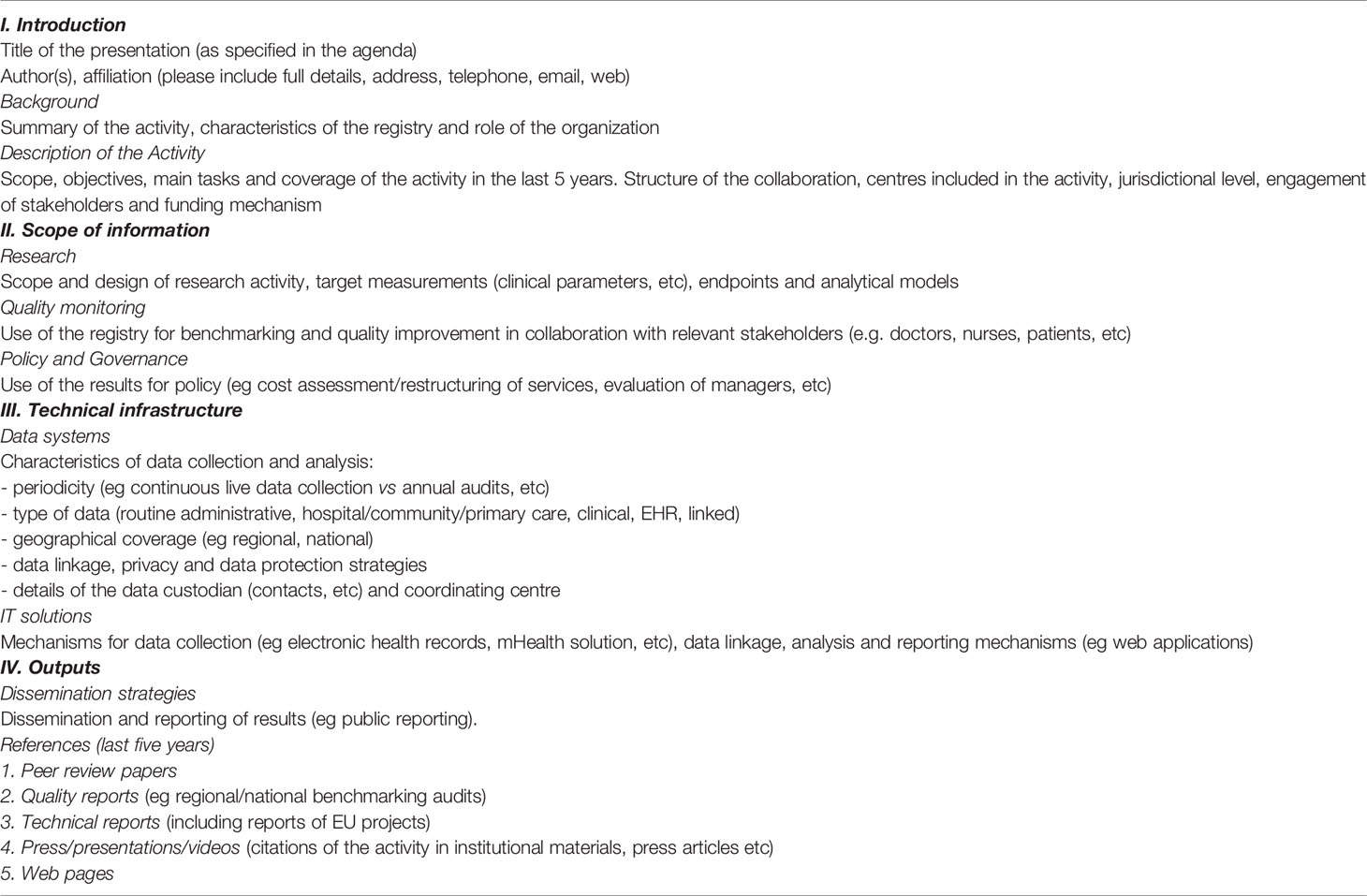
Table 1 Structure of the survey questionnaire.
The questionnaire included four key sections: 1) description; 2) scope of information; 3) technical infrastructure; and 4) outputs. The description was intended to provide an overview of the organizational aspects related to the registry or data source: affiliation, role, scope, jurisdictional level, stakeholders and funding. The scope of information was investigated using three relevant subsections: a) research items (parameters, endpoint and models); b) quality goals (use for quality and benchmarking); and c) use for policy and governance. The latter was considered as a relevant characteristic of continuous data collection, as the network recognised the importance of institutional involvement for health improvement through targeted initiatives e.g. national diabetes plans. The third area of interest was the technical infrastructure, including all aspects that can determine the capacity of the registries/database to process data and enable international comparisons with the required granularity to allow full automated data exchange. The technical elements also included an examination of potential hurdles in the application of privacy and data protection rules, which were also the subject of an annexed activity of the same task (18). Finally, the questionnaire included a section on outputs, targeting the various dissemination strategies and the key references to scientific papers, technical reports and web outputs produced as part of the routine activity of the participating register/data source during the last 5 years.
The implementation of the survey was carried out by the University of Ljubljana, Slovenia, via the open access software infrastructure Redcap (19, 20). The questionnaire was duly implemented to allow the direct contribution of partners via a dedicated web page. The survey was finalised between 19th August - 9th September 2017. Results were saved into an Excel sheet and summarized using frequencies and percentages, visualized using pie charts and histograms.
The percent of the total population with diabetes “on record” in the registry or data source during the last year available was calculated using the most relevant estimate of the total population with diabetes available from an official national report or the WHO country profiles (https://www.who.int/diabetes/country-profiles/diabetes_profiles_explanatory_notes.pdf). Such a measure has been used only to provide a figure of the potential contribution that each data source would be able to make for pooled data analysis of distinct subjects with diabetes. Therefore, it may substantially deviate from the coverage of national quality indicators reported from each data source.
Further results included the qualitative assessment of the materials reported in open format by the countries filling the questionnaire. The results contributed to a technical report describing the functioning of the registry/data source in terms of policy, infrastructure, procedures and outputs. The results were discussed among participants at the second investigators’ meeting, held in Nicosia, Cyprus, on 21st-22nd September 2017 (see http://www.hirs-research.eu/eubirod/meetings/cyprus2017/). Selected contents contributed to the final report, delivered according to the workplan on 9th October 2017 (15).
In preparation of the present report, further updates were requested directly from all participants, regarding the total number of persons with diabetes included in the data source at the most recent date before 31st May 2021.
Results
A total of 18 representatives of registries and data sources from 17 countries successfully completed the questionnaire. The full list of institutions, including links to the relevant portals, whenever available, is shown in (Table 2). The majority of data sources were located in Northern Europe, with 14 out of 27 EU current MS being represented. Institutions that today are located outside the EU included representatives from the United Kingdom, Norway and Israel.
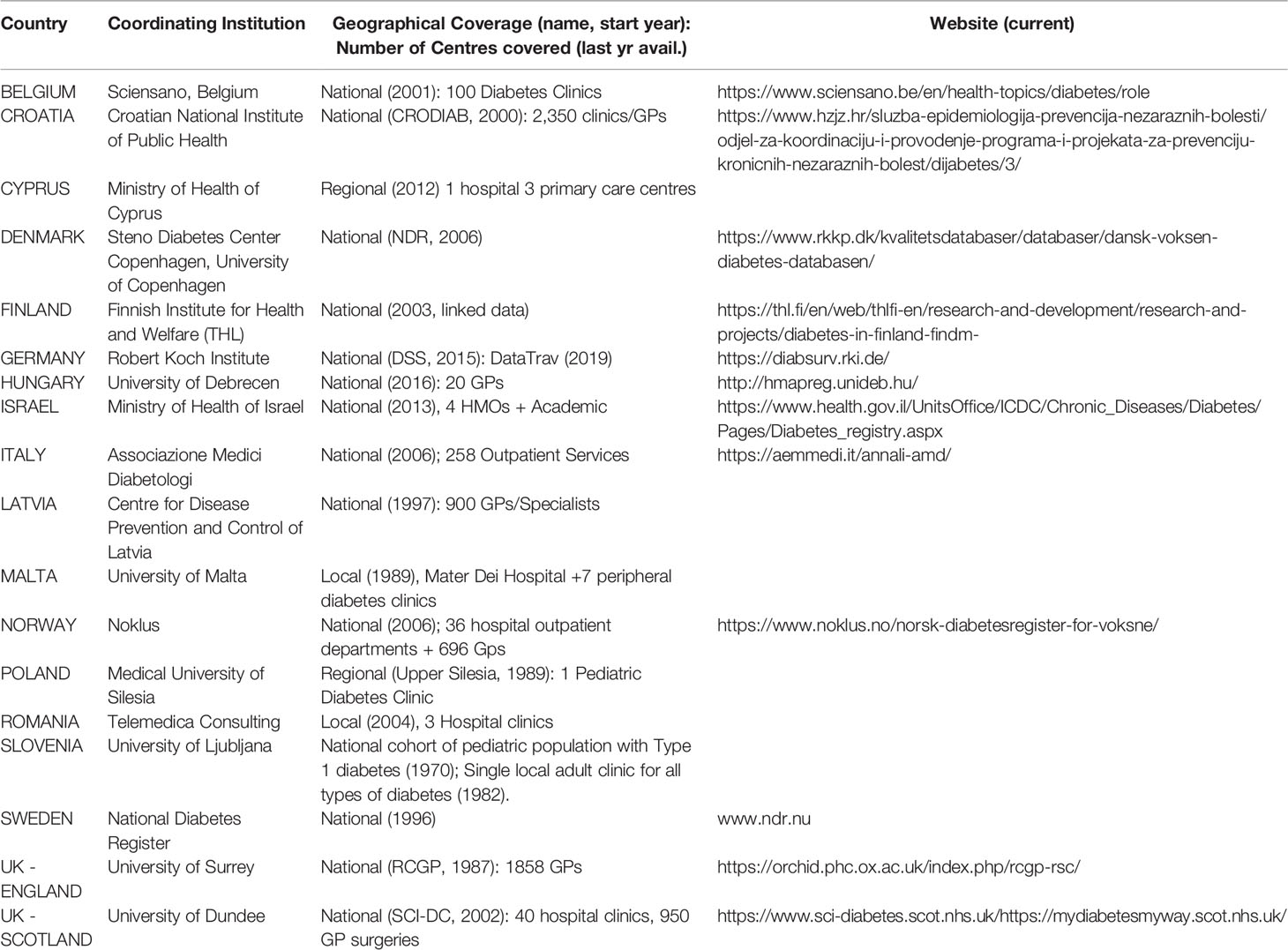
Table 2 Participating countries and coordinating institutions.
The general characteristics of registries and data sources included in the survey are shown in (Figure 1).
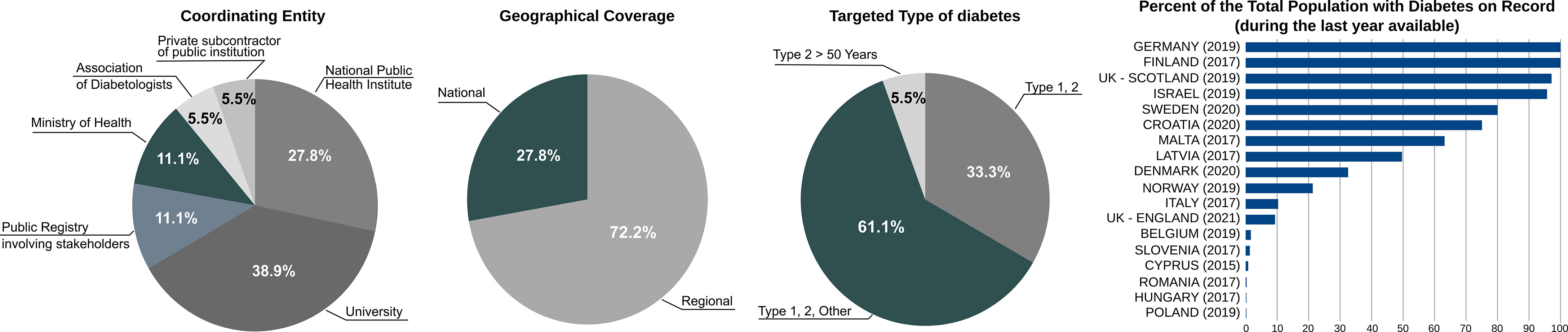
Figure 1 General characteristics of diabetes registries and data sources included in the survey (N=18).
The coordinating entity was most frequently an academic centre (N=7; 38.9%), followed by a national public health institute (N=5; 27.8%), a public registry involving stakeholders (N=2; 11.1%) or a Ministry of Health (N=2; 11.1%). Only in one case (5.5%), the data source was managed either by an association of diabetologists or a private subcontractor. As described directly by participants, the type of coordination originated from the inspirational guidance of the World Health Organization (WHO) and the International Diabetes Federation (IDF) after the Saint Vincent Declaration in 1989 (21), prompting countries to monitor and control the state of the art of diabetes health care through the use of modern technologies for data collection and exchange (22). The goal has been pursued using different solutions, through the creation of National Diabetes Registries (Scotland, Sweden, Norway, Denmark). In these cases, one central organization (sometimes supported by an academic/research centre) coordinates the activity of different sub-national networks (with the direct participation of multiple stakeholders), or national monitoring is assigned directly to institutional agencies nominated by the Government (Finland, Latvia, Croatia, Germany, Belgium). Less frequently, national activities were carried out directly by the Ministry of Health (Cyprus, Israel). To a lesser extent, medical professional associations and national diabetes audits ensured the activity of diabetes monitoring (England, Italy).
The geographical coverage was mostly national (N=13; 72.2%) as opposed to regional (N=5; 27.8%). In general, whenever diabetes monitoring was carried out through governmental action, the geographical coverage was intended to be national, albeit not always the case (see later). The regional emphasis was most often related to academic research conducted on specific cohorts (Poland, Romania, Slovenia, Malta).
All types of diabetes were targeted in 11 cases (61.1%), with only Type 1 and/or Type 2 included in additional 6 cases (33.3%). Only in one case (5.5%), the attention was limited to Type 2 over 50 years of age. However, at least in two cases (Slovenia, Poland) the attention to Type 1 was particularly enhanced, as they are typically smaller groups, where the attention to collect detailed clinical data for care optimisation and research is significantly higher.
The percent of the total population with diabetes at national level on record in the registries and data sources (based on the last date available) varied considerably across the sample: a total of N=8 databases (44.4%) did not exceed 10%, with additional N=5 (27.8%) achieving between 10-70% and only N=5 (27.8%) over 70%. In some cases, the high percent reflected the method applied for the construction of indicators, particularly with the use of secondary data (Germany, Finland, Israel). The downside of this approach was that clinical indicators were not available for a large population, unless obtained through the use of survey sampling (Germany, Belgium, Hungary). In these cases, the coverage of the population with diabetes could actually be much higher. For example, the sample of 12,000 collected in Belgium reportedly corresponds to 114,200 people with diabetes officially used as denominators for national quality indicators. A high percent was reported by countries with population-based registries in Scotland, Sweden, Denmark, Latvia and Croatia. Notably, professional associations e.g. the Royal College of General Practitioners (RCGP) Research and Surveillance Centre (RSC) in England and the Association of Medical Diabetologists (AMD) in Italy achieved a moderate percentage of people with diabetes, while collecting a large number of relevant clinical parameters.
The data characteristics of registries and data sources investigated in the present study are shown in (Figure 2).
Figure 2 Data characteristics of diabetes registries and data sources included in the survey (N=18).
The type of data source was the most fragmented characteristic in the whole sample. The register was population-based in N=5 cases (27.8%), as opposed to a single database from multiple providers in N=4 cases (22.2%). In N=2 cases each (11.1%), it was either a single database from single provider or composed of linked administrative data. All other cases (5.5% each) where either clinical data from the electronic health record (EHR) linked with samples extracted from national databases, combination of national surveys and administrative data, linked data sources from multiple registries and providers, single database or survey. The different types of data sources used in different countries reflected the existing barriers and enablers present in their evolution. These included a range of different aspects, e.g. limitations of the information infrastructure, varying capacity and skills, lack of interoperability between different levels of the health system, administrative boundaries and heterogeneous implementation of privacy and data protection legislation in each jurisdiction. As a result, with the exception of countries using similar population-based schemes (e.g. Croatia, Denmark, Latvia, Scotland, Sweden), all others sources implemented ad hoc solutions.
In the majority of cases, the type of data collection was continuous (N=11; 61.1%), as opposed to annual (N=5; 27.8%) or every two years (N=2; 11.1%). Noticeably, the annual data collection seemed to reflect more the periodicity of extraction of the overall linked database, rather than the actual mode of data collection, which in some cases used ad hoc software installed in care facilities (Norway, Croatia, Italy). The biennial data collection was a specific characteristic of survey samples (Belgium, Hungary).
The procedure of data linkage with other sources was evenly distributed (N=9; 50% either possible or not possible). The extent to which data are not linked across Europe represents a relevant barrier that can limit the information content of diabetes-related databases from a correct epidemiological perspective. This seemed to be directly associated with the type of data source e.g. diabetes clinics (Cyprus, Italy, Malta, Poland, Romania, Slovenia) or general practitioners (Hungary, England). A case in point where administrative and legal issues seemed to be particularly relevant is that of Germany, where different databases were utilised, but could not be linked across.
Finally, a unique identifier for patient-based analysis was separately available through protected access in N=11 cases (61.1%), as opposed to being directly accessible in the database via a pseudo-anonymised code (N=5; 27.8%) or not available in N=2 cases (11.1%). The latter included two sources using survey sampling for the calculation of indicators (Germany, Hungary).
A snapshot of the outputs routinely produced by registries and data sources is provided in (Figure 3).
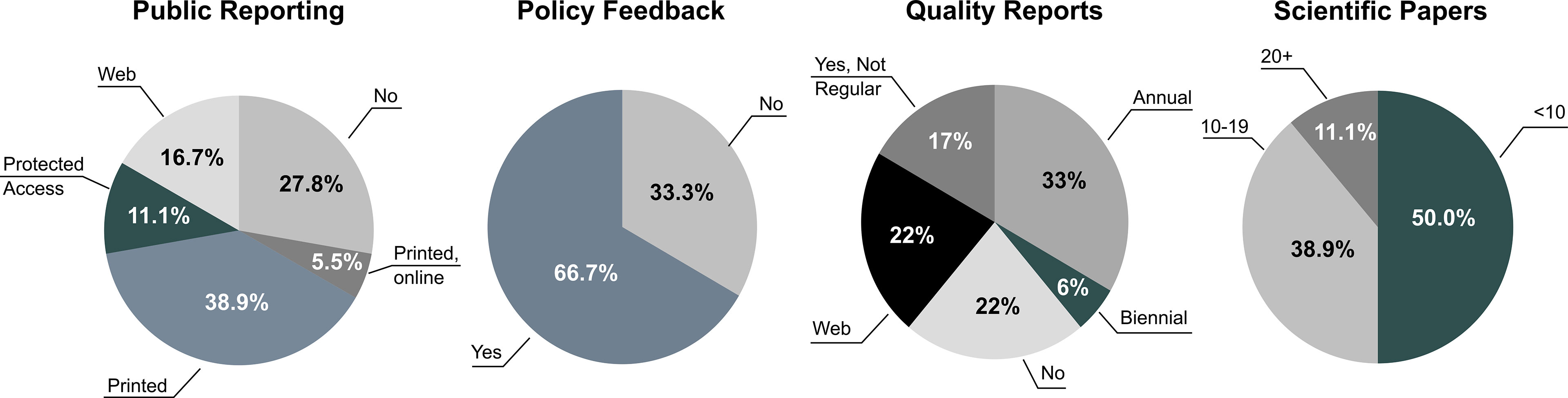
Figure 3 Outputs of diabetes registries and data sources included in the survey (N=18).
Over a quarter of cases (N=5; 27.8%) did not envisage public reporting. Among those producing public reports, the majority delivered results only in “printed pdf” format (N=7; 38.9%), one (5.5%) published the same results in printed and online (interactive format), and N=3 (16.7%) as web pages only. The remaining N=2 sources (11.1%) made reports only available through the use of credentials. Different type of institutions did not regularly deliver public reports, including governmental organizations (Cyprus, Finland) and academic/research entities (Hungary, Poland, Romania) which operate for the production of scientific papers. Reports in pdf were more popular among entities delivering annual outputs for audit and performance comparisons. At the other end, national population-based registries seemed to be definitely oriented towards the production of continuous web outputs (e.g. Denmark, Sweden and Scotland).
Feedback to policy was foreseen in the majority of cases (N=12; 66.7%), as opposed to none (N=6; 33.3%). A common feature of data sources not using their indicators to provide direct feedback to policy was the lack of a specific agreement between the national/regional authorities to coordinate a formally recognised diabetes register (e.g. Finland, Malta, Poland, Romania, Slovenia, England).
Quality reports were available in the majority of cases (N=14; 77.8%), either annually (N=6; 33.3%), biennally (N=1; 5.6%), regularly via web reports (N=4; 22.2%) or not regularly (N=3; 16.7%). In N=4 cases (22.2%) quality reports were not produced. A common trait of those using quality reporting was a clear link with non-academic health professionals. In fact, the only data sources that did not appear to deliver quality reports were those using large scale administrative databases or were university driven (Finland, Germany, Latvia and Malta). Nevertheless, quality of care indicators could still appear among those regularly published in public health reports. In the case of Germany, their calculation was possible through a mix of national health surveys and disease management programs (see https://diabsurv.rki.de/Webs/Diabsurv/EN/project/methodology/indicator_set/indicator_set-node.html).
The scientific production of peer reviewed publications was unevenly distributed, ranging between 0-90 papers during the last 5 years. In fact, one half of the sample published less than 10 papers (N=9; 50%), the other between 10-19 (N=7; 38.9%) or 20 or more (N=2; 11.1%). The latter included two data sources producing different types of papers: while Sweden (reporting 90 peer reviewed papers) produced articles using large cohort for diabetes epidemiology and quality of care, Poland (reporting 37 papers) worked on clinical parameters involving small groups of individuals with Type 1. The mid group including those who were also productive in terms of scientific literature included large collaborative networks (e.g. Italy and Scotland), national institutes (e.g. Croatia, Denmark, Finland and Germany) and a dedicated research entity (Romania), all being active in diabetes for over a decade. For the majority of data sources, the scientific production appeared to be rather limited.
Further details on the technical infrastructure adopted by data sources included in the present review are included in (Table 3).
Table 3 Technical Infrastructure of diabetes registries and data sources in the EUBIROD review (Year 2017).
Discussion
The results of our survey confirmed the substantial activity carried out in the field of diabetes information in many countries, suggesting three key points for discussion.
Firstly, in terms of main targets of our investigation, our study confirmed that there was not a unique notion of “diabetes registry” (4). A recent review carried out by WHO Europe (23) defined it as “a manually or automatically generated list of people with diabetes, developed as a rule-based system based on specific inclusion criteria”. However, we showed that the same concept has been differently implemented to produce outputs that are similar in their goals of quality of care improvement, surveillance, epidemiology, research, and resource optimisation. Therefore, we prefer to refer for these purposes more generally to “diabetes registries and data sources”.
Secondly, in terms of relevance of information content, we found that these initiatives, even when covering only a portion of the target population or a limited set of indicators, may still be valid for monitoring and benchmarking. Our survey included sub-national data sources which involve a range of stakeholders, in many cases including professional networks that collect clinical parameters otherwise not available through registries relying mainly upon administrative data. These attractive features called for more cohesive initiatives, based on mutual respect and joint commitment between coordinating institutions and physician networks.
Thirdly, in terms of methodology for evaluation, given the complexity and rapid evolution of modern information systems, we demonstrated the advantages of requesting details directly from managers, developers and data custodians of diabetes registries and data sources, who are knowledgeable about the actual operating conditions.
Using this approach, our survey confirmed the activity of a number of mature, well organized national networks that are capable of delivering regular reports on the majority of people with diabetes in their own settings and jurisdictions. Seven out of eighteen entities presented in this report were also included in a recent review of national diabetes registries (5), showing that the measurable results of these initiatives were mild in terms of processes and information gain and very limited in terms of clinical outcomes. Our survey highlighted the challenges faced by national registries designed to respond to different stakeholders, including people with diabetes, policy-makers, health care decision makers, health professionals, research institutions and the general population. The lack of focus on relevant complications (24), as opposed to the production of batteries of statistical indicators, may explain the difficulty in achieving selected clinical targets.
Our study also showed large variability in terms of governance, information infrastructure and generated outputs. The results were obtained through the use of a structured questionnaire, consistently with our driving principles of direct inquiry. The limited production of scientific outputs supports the hypothesis that any assessment based on the systematic review of available outputs would likely introduce bias and miss out on many details of interest.
The scoping review recently carried out by WHO Europe (23) attempted to resolve these limitations using a three-pronged strategy, consisting of: a) search of different types of materials; b) consideration of sub-national registries; and c) open consultation on preliminary findings. However, results are difficult to compare, due to the limited overlap with our sample, possibly owing to restrictive inclusion criteria adopted by the WHO e.g. specific definitions of diabetes registries and information systems, search keywords not including “data source” or “database”, and papers only limited to open access journals.
In our survey, we found that the type of data source was the most variable characteristic among those investigated. This can have critical implications on the reliability and comparability of indicators, deserving to be explained in detail using the models presented in (Figure 4).
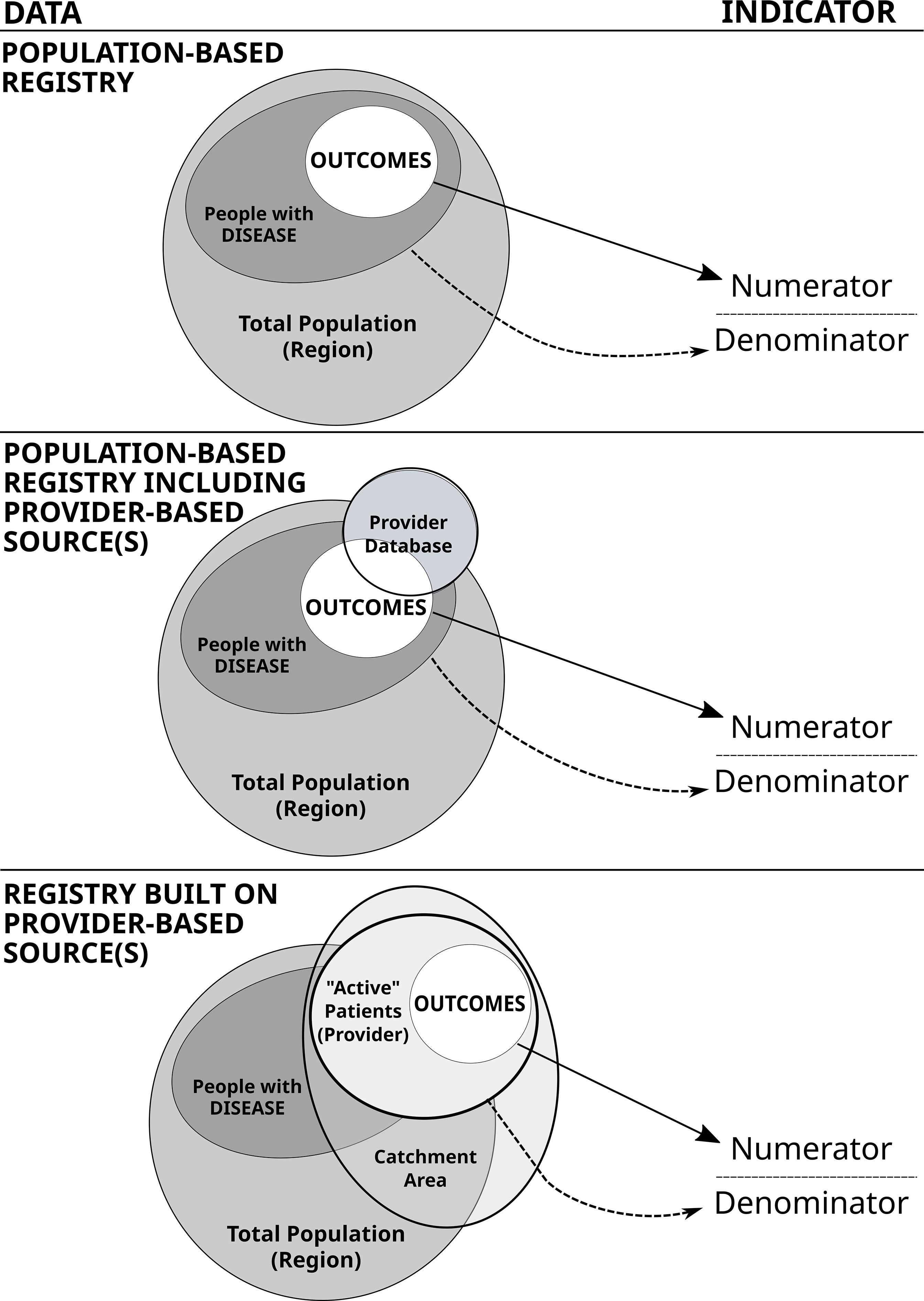
Figure 4 Reliability of indicators derived from different data schemes. At left: different combinations of data sets. At right: the resulting indicator, presented for convenience as the typical quality of care indicator, including the number of cases with negative outcomes in the numerator (e.g. the number of subjects with major amputations) and the reference population in the denominator (e.g. the number of people with diabetes).
The first model represents the ideal setting of a “population-based diabetes registry”. Under these circumstances, the number of outcomes occurring in a specific target population (e.g. any/specific type of diabetes, with/without complication, etc) can directly contribute to a person-based numerator, including a fraction of those belonging to a well-defined total population (e.g. population living in a catchment area, local health authority, region or country). This condition is fully met in national registries that also include clinical parameters e.g. Croatia (25), Denmark (26), Latvia (27), Scotland (28) and Sweden (22).
The second model envisages the inclusion of one or more provider-based sources, within or in addition to an underlying population-based registry (or other type of source directly linked to a specific population e.g. administrative data). In this case, a more complex infrastructure is progressively built to increase the completeness of data collection, for example to incorporate new items e.g. clinical parameters that are difficult to collect as the first instance. Under this scheme, a critical problem is to use only those records in the provider database that match the specifications of the population-based registry in both the numerator and denominator. This is possible through the use of a validated unique ID, which we only found in 50% of cases. A case in point related to the national surveillance is that of Germany (29), in which a variety of data sources have been used, but indicators may be generally difficult to report consistently at population level, due to the impossibility to use a common unique id. We have found this to be structurally achieved in the cases of Finland and Israel.
In the third model, indicators are derived only from one or more provider-based data sources. In this case, the percent of the total population on record can be patchy and prone to bias both in the numerators and denominators (unless a unique ID is thoroughly applied, see above). This is the case in which results may be seriously undermined by opportunistic selection (e.g. dropping high risk patients), incorrect identification of person-based profiles (e.g. double counts and difficulty using repeated measures), or uncertain attribution of indicators to a specified reference population or geographical area. In such situations, a list of “active patients” should be maintained to ensure that denominators are correct. As an exemplary case, one could consider the indicator of the number of subjects with HbA1c test done annually. A correct calculation would require a list of those expected to visit the clinic during the year, rather than those actually visiting it. By discarding those unable to visit, the indicator would automatically ignore high risk patients (e.g. those visually impaired), so that all results would inevitably fall in the surrounding of 100% (the main reason for visiting the diabetes clinic being the annual examination). In our survey, given that we could not find explicit mentioning of such a technical aspect, we could argue that this is a specific area worth further investigation. This model is particularly relevant, as it represents the majority of diabetes registries and data sources included in our study.
The taxonomy described above may serve as general guidance, but various conditions may hold under different circumstances that can rapidly change over time, implying the possibility to switch from one model to another. Nevertheless, it is important to note that the interpretation of statistical indicators cannot ignore the underlying information infrastructure, particularly when person-based analysis is required to evaluate the performance of health services.
A characteristic that was also found to be rather variable in our sample was the coordinating entity. We found that a small fraction of national registries, namely in Denmark (26) and Sweden (22), were organized as a structural collaboration incorporating multiple stakeholders. This type of agreement may have certain advantages, e.g. the high level of standardization of internal procedures allowing to cover a large portion of the target population, facilitated access to a unique ID through opt in-opt procedures and more transparent rules for health data governance. Although coordinated by academic or professional entities, similar conditions are also present in the Scotland Diabetes Registry (28), the RCGP RSC collaboration in England (30) and the AMD database in Italy (31). Alternatively, the highly structured decision making process found in collegial arrangements can make activities, such as bespoke research and developing new analytical models less flexible. The centrality of public entities in certain cases enhanced internal flexibility, conditional on the availability of resources. The availability of complete electronic health records at medical practices, together with the resolution of all regulatory aspects related to data protection, can harness public health and health care services research in more complex frameworks e.g. Germany (29). In this case, using different sources at a national level has been particularly challenging, but the attention towards collaborative environments has grown out of more targeted surveillance activities. In other cases, universities maintain sources in accordance with contractual obligations and/or to continue their dedicated research activity.
The geographical coverage was in almost three quarter of the cases regional, reflecting the diverse characteristics of partners included in the EUBIROD network. Both Type 1 and Type 2 were targeted in almost all cases, with nearly half of the sample covering at least 50% of people with diabetes. Periodic data collection was carried out in over one third of cases, with two thirds ensuring continuous updating of their database. There seemed to be no pattern for this condition, except for policy feedback that was consistently ensured in all cases with annual updates.
On the other hand, the characteristic that was more evenly distributed among participants was the possibility of performing data linkage, which was possible for half of the cases. This confirms the heterogeneous implementation of principles of privacy and data protection in many EU/OECD countries, despite relevant attempts to harmonise approaches (18). However, we noticed that the availability of a unique identifier, either through pseudo-anonymisation or protected access, was indeed possible in nearly 90% of cases. This seems to indicate that the priority given to the uptake of security procedures has not hampered the secondary use of health data (32).
We were able to assess the relevance of a unique ID within the existing technical infrastructure described by participants in the survey. There was a clear role of the master patient index at centres operating in Sweden (22), Croatia (25), Denmark (26), Finland (33), Israel (34), Latvia (27), Norway (35) and Scotland (28). Among them, only Finland was unable to incorporate clinical parameters from medical records, due to the decentralised operations and frequent use of unstructured format. However, the situation is improving and clinical data should be rapidly made available (32). On the other hand, electronic health records collected at the point of care using a valid patient ID were noted in a second group of participants from Belgium (36), Cyprus (37), England (30), Italy (31), Malta (38), Poland (39), Romania (40) and Slovenia (41). For England, the advantages offered by an expanding network of general practitioners included the possibility of linking and comparing items from different comorbid conditions stored in the same database (42). The solution resembles the model of quality registries widely implemented in Nordic countries across different silos (43), with the further advantage of being able to directly access all data in one location. A third group of participants included Hungary (44), where clinical data from the survey were designed to be linked across, and the national surveillance system from Germany (29), in which multiple datasets contributed to different indicators, but could not be linked across using a unique ID.
We found that the information infrastructure determined the type of results that could be delivered by the existing diabetes registries and data sources. Consistently with differences among systems in place, the types of outputs were also quite variable. Static formats e.g. pdf documents appeared to be still very popular, while web formats represented almost a quarter of cases. However, an equal fraction of cases did not present results in any public reporting. Interestingly, no specific characteristic seemed to be associated with either approach. On the other hand, policy feedback was not provided by one third of participants who seemed more oriented towards research. This may indicate a potential gap between research and policy that should be overcome to fully exploit the availability of actionable information. Quality reports were not foreseen by participants who had in common the lack of clinical parameters in the data source and feedback to policy makers. These characteristics confirmed the gap between the availability of health indicators and their direct use in the interest people with diabetes.
In summary, our survey filled the gap between the details available from the literature and the actual operating characteristics on the ground. Previous results from the EUBIROD network showed that the majority of parameters included in the International Consortium for Health Outcomes Measurements (ICHOM) standard set (45) were already present in many sources but presented varying quality and completeness (13). In this study, we showed that the general features, data characteristics and outputs delivered by systems in place may explain much of the variation found before. Although best practices exist, the ecosystem of diabetes information systems appears still fragmented and not immediately related to the expectations of all primary stakeholders.
These problems can be resolved by strengthening international collaboration through a federation of the existing initiatives. Building a European Diabetes Registry could be a convenient strategy to prepare health systems for future emergencies (46), while fulfilling the goal of the EU Parliament “to coordinate, collect, register, monitor and manage comprehensive epidemiological data on diabetes, and economic data on the direct and indirect costs of diabetes prevention and management” (47).
Furthermore, combining multiple large databases can provide essential data for training, testing and validating meaningful predictive models that would enhance strategies for the reduction of diabetes complications. For example, it would be possible to move from monitoring traditional clinical parameters e.g. hypertension (39) to more complex investigation carried out in real time e.g. amputation free survival (48). In this way, people with a moderate complication e.g. diabetic foot ulcers may be systematically followed up using information from their baseline profile (e.g. type and duration of diabetes), in association with clinical parameters (e.g. HbA1c), other diabetes complications (e.g. diabetic retinopathy) and detailed morphological characteristics of foot ulcer (using medical imaging). The infrastructure can be rapidly scaled up to incorporate innovative approaches that are revolutionising the way population-based registers are linked to personal data e.g. those captured via smartphone apps (49). The possibility to provide access to micro-aggregate data extracted from such common data models across Europe would represent an ideal case study for the implementation of the European Health Data Space (50). This is an intrinsic functionality of the software implemented by the EUBIROD network at its inception (15), which respects the principles of making health data findable, accessible, interoperable and reusable (FAIR) that are currently proposed by different networks in Europe (51).
To make this possible, it will be essential to link initiatives, learning from best practices. Countries should learn from the lesson of the COVID-19 pandemic, making the secondary use of health data widespread, shared at minimal cost and highly sustainable. In this way, the convenience of cross-border collaboration would be demonstrated in practice by the immediate availability of data and indicators that cannot be easily gathered out of the boundaries of their own organizations.
Finally, some relevant limitations of our study are outlined below.
Firstly, the study was conducted on a limited sample of partners and collaborating institutions of the EUBIROD network. Although including key partners from 14 out of 27 current Member States of the EU, we cannot claim for our survey to represent a complete overview of the European context. Nevertheless, we included the majority of experiences operating on a permanent basis, which have been influential on the development of diabetes information systems both at national and international level, as shown by their inclusion also in other reviews.
Secondly, the review has been conducted in 2017. In a rapidly changing environment, this means that a substantial update will be needed soon, to ensure that the details we have provided here are still current. However, we have requested further information related to the number of patients relative to the last year available, showing that 10 out of 18 entities were still fully operational at least until 2019.
Thirdly, we did not directly verify the functionality and quality of indicators produced by the data sources, either by conducting interviews with local developers, or by running any statistical analysis on internal data. That is the scope of a new project, implementing the BIRO approach for the purpose of automating the overall analysis of a collaborating network (52). Further research will be required to evaluate procedures in each case.
In conclusion, accurate diabetes information is central to the strategy of quality of care and outcomes improvement in diabetes in many jurisdictions at national and sub-national level. Diabetes registries have demonstrated modern ways to organize, govern and deliver best information at regional, national and international level. However, the heterogeneous implementation across Europe still hampers the ability to provide accurate and comparable information on the achievement of common targets.
Best practices exist, but need to be shared more effectively to ensure that efforts are aligned. An area of particular interest is that of incentivised collaboration between central authorities and physician networks. The strengthening of international collaborations e.g. the EUBIROD network may accelerate the adoption of these approaches, but countries will need to invest more on health information systems that are interoperable and consistent with the expectations of people with diabetes, taking their perspectives into account. Future updates and extensions of the present survey will be needed to monitor progress in this rapidly evolving field.
Author Contributions
The present paper is a collective product of the EUBIROD network, including main authors and other authors who contributed substantially to the conception and delivery of the survey. All authors provided an active contribution in the development of the survey instrument, data collection and production of the manuscript. FC and IS designed the survey questionnaire. IS implemented the online survey tool and extracted the data for analysis. FC has carried out the analysis and wrote the first draft of the manuscript. All authors have contributed to the writing and revision of the manuscript. All authors have read, and confirm that they meet, ICMJE criteria for authorship. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. FC is the guarantor. All authors contributed to the article and approved the submitted version.
Funding
The products presented in this study have been funded through granting provided by DG-SANCO in the EU project Bridge Health (GA 664691).
Conflict of Interest
SL is the Director of the RCGP RSC, as part of his academic work. He has received grants through his institution from AstraZeneca, Eli Lilly, Novo, and Sanofi, for diabetes related research. SC is employed by My Digital Health. CI is employed by Serectrix snc. SP was employed by Telemedica Consulting.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Carinci F, Van Gool K, Mainz J, Veillard JH, Pichora E, Januel JM, et al. Towards Actionable International Comparisons of Health System Performance: Expert Revision of the OECD Framework and Quality Indicators. Int J Qual Health Care (2015) 27(2):137–46. doi: 10.1093/intqhc/mzv004
2. Busse R, Klazinga N, Panteli D, Quentin W. Improving Healthcare Quality in Europe. Characteristics, Effectiveness and Implementation of Different Strategies (2019). World Health Organization and OECD. Available at: https://apps.who.int/iris/rest/bitstreams/1248308/retrieve (Accessed 6th July 2021).
3. McKay AJ, Gunn LH, Vamos EP, Valabhji J, Molina G, Molokhia M, et al. Associations Between Attainment of Incentivised Primary Care Diabetes Indicators and Mortality in an English Cohort. Diabetes Res Clin Pract (2021) 174:108746. doi: 10.1016/j.diabres.2021.108746
4. Carinci F, Di Iorio CT, Massi Benedetti M. Standardized Information Exchange in Diabetes: Integrated Registries for Governance, Research and Clinical Practice, in Bruttomesso D, Grassi G (Eds), Technological Advancements in the Treatment of Type 1 Diabetes. Front Diabetes (2015) 24:236–49. doi: 10.1159/000363520
5. Bak JCG, Serné EH, Kramer MHH, Nieuwdorp M, Verheugt CL. National Diabetes Registries: Do They Make a Difference? Acta Diabetol (2021) 58(3):267–78. doi: 10.1007/s00592-020-01576-8
6. Carinci F, Massi Benedetti M, Klazinga N, Uccioli L. Lower Extremity Amputation Rates in People With Diabetes as an Indicator of Health Systems Performance. A Critical Appraisal of the Data Collection 2000-2011 by the Organization for Economic Cooperation and Development (OECD). Acta Diabetol (2016) 53(5):825–32. doi: 10.1007/s00592-016-0879-4
7. Ali MK, Siegel KR, Laxy M, Gregg EW. Advancing Measurement of Diabetes at the Population Level. Curr Diabetes Rep (2018) 18(11):108. doi: 10.1007/s11892-018-1088-z
8. IDF Diabetes Atlas 2019. Available at: https://www.diabetesatlas.org/en/resources/ (Accessed 19th May 2021).
9. de Beaufort CE, Reunanen A, Raleigh V, Storms F, Kleinebreil L, Gallego R, et al. European Union Diabetes Indicators: Fact or Fiction? Eur J Public Health (2003) 13(3 Suppl):51–4. doi: 10.1093/eurpub/13.suppl_1.51
10. The EUBIROD Project Website. Available at: http://www.eubirod.eu (Accessed 6th July 2021).
11. Di Iorio CT, Carinci F, Azzopardi J, Baglioni V, Beck P, Cunningham S, et al. Privacy Impact Assessment in the Design of Transnational Public Health Information Systems: The BIRO Project. J Med Ethics (2009) 35(12):753–61. doi: 10.1136/jme.2009.029918
12. Di Iorio CT, Carinci F, Brillante M, Azzopardi J, Beck P, Bratina N, et al. Cross-Border Flow of Health Information: Is 'Privacy by Design' Enough? Privacy Performance Assessment in EUBIROD. Eur J Public Health (2013) 23(2):247–53. doi: 10.1093/eurpub/cks043
13. Cunningham SG, Carinci F, Brillante M, Leese GP, McAlpine RR, Azzopardi J, et al. Core Standards of the EUBIROD Project. Defining a European Diabetes Data Dictionary for Clinical Audit and Healthcare Delivery. Methods Inf Med (2016) 55(2):166–76. doi: 10.3414/ME15-01-0016
14. The EUBIROD Diabetes Report (2012). Available at: http://www.eubirod.eu/edr/index.html (Accessed 6th July 2021).
15. Carinci F, Gualdi S, Di Iorio CT, Massi Benedetti M. Bridge Health Task 8.2 Study Group. Blueprint of Open Source Software Platform for Population-Based Chronic Disease Registries. Bridge Health Consortium. Available at: http://www.eubirod.eu/projects/bridge/documents/blueprint_D8.2_final_091017.pdf (Accessed 6th July 2021).
16. The BRIDGE-Health Project, Sponsored by the European Commission, Consumers, Health, Agriculture and Food Executive Agency, Grant Agreement N. 664691. Available at: http://www.bridge-health.eu/ (Accessed 6th July 2021).
17. Carinci F. Essential Levels of Health Information in Europe: An Action Plan for a Coherent and Sustainable Infrastructure. Health Policy (2015) 119(4):530–8. doi: 10.1016/j.healthpol.2014.11.016
18. Di Iorio CT, Carinci F, Oderkirk J, Smith D, Siano M, de Marco DA, et al. Assessing Data Protection and Governance in Health Information Systems: A Novel Methodology of Privacy and Ethics Impact and Performance Assessment (PEIPA). J Med Ethics. doi: 10.1136/medethics-2019-105948
19. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research Electronic Data Capture (REDCap) – A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support. J BioMed Inform (2009) 42(2):377–81. doi: 10.1016/j.jbi.2008.08.010
20. Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, et al. The REDCap Consortium: Building an International Community of Software Partners. J BioMed Inform (2019) 95. doi: 10.1016/j.jbi.2019.103208
21. Diabetes Care and Research in Europe: The Saint Vincent Declaration. Diabetes Med 7(4):360. doi: 10.1111/j.1464-5491.1990.tb01405.x
22. Gudbjörnsdottir S, Cederholm J, Nilsson PM, Eliasson B. Steering Committee of the Swedish National Diabetes Register. The National Diabetes Register in Sweden: An Implementation of the St. Vincent Declaration for Quality Improvement in Diabetes Care. Diabetes Care (1990) 26(4):1270–6. doi: 10.2337/diacare.26.4.1270
23. Agnello D, Tello J. Registries and Information Systems for Diabetes Care in the WHO European Region: Preliminary Findings for Consultation. Europe: WHO. Available at: https://www.euro.who.int/:data/assets/pdf_file/0003/505371/registries-information-systems-diabetes-consultation-eng.pdf (Accessed 6th July 2021).
24. Carinci F, Uccioli L, Massi Benedetti M, Klazinga NS. An in-Depth Assessment of Diabetes-Related Lower Extremity Amputation Rates 2000-2013 Delivered by Twenty-One Countries for the Data Collection 2015 of the Organization for Economic Cooperation and Development (OECD). Acta Diabetol (2020) 57(3):347–57. doi: 10.1007/s00592-019-01423-5
25. Poljicanin T, Bralic Lang V, Mach Z, Svajda M. Croatian Diabetes Registry (CroDiab) and Implementation of Standardised Diabetes Checklists Using Joint Action CHRODIS Recommendations and Criteria. Ann. Ist Super Sanita (2021) 57(1):74–9. doi: 10.4415/ANN_21_01_12
26. Jørgensen ME, Kristensen JK, Reventlov Husted G, Cerqueira C, Rossing P. The Danish Adult Diabetes Registry. Clin. Epidemiol (2016) 8:429–34. doi: 10.2147/CLEP.S99518
27. Strele I, Pildava S, Repsa I, Kojalo U, Vilmanis J, Brigis G. Pre-Existing Diabetes Mellitus and All-Cause Mortality in Cancer Patients: A Register-Based Study in Latvia. Acta Oncol (2018) 57(7):973–82. doi: 10.1080/0284186X.2017.1420909
28. Kennon B, Leese GP, Cochrane L, Colhoun H, Wild S, Stang D, et al. Reduced Incidence of Lower-Extremity Amputations in People With Diabetes in Scotland: A Nationwide Study. Diabetes Care (2012) 35(12):2588–90. doi: 10.2337/dc12-0511
29. Heidemann C, Scheidt-Nave C. Prevalence, Incidence and Mortality of Diabetes Mellitus in Adults in Germany. A Review in the Framework of the Diabetes Surveillance. J Health Monit (2017) 2(3):98–121. doi: 10.17886/RKI-GBE-2017-062
30. de Lusignan S, Correa A, Smith GE, Yonova I, Pebody R, Ferreira F, et al. RCGP Research and Surveillance Centre: 50 Years' Surveillance of Influenza, Infections, and Respiratory Conditions. Br J Gen Pract (2017) 67(663):440–1. doi: 10.3399/bjgp17X692645
31. Rossi MC, Candido R, Ceriello A, Cimino A, Di Bartolo P, Giorda C, et al. Trends Over 8 Years in Quality of Diabetes Care: Results of the AMD Annals Continuous Quality Improvement Initiative. Acta Diabetol (2015) 52(3):557–71. doi: 10.1007/s00592-014-0688-6
32. Oderkirk J, Ronchi E, Klazinga N. International Comparisons of Health System Performance Among OECD Countries: Opportunities and Data Privacy Protection Challenges. Health Policy (2013) 112(1-2):9–18. doi: 10.1016/j.healthpol.2013.06.006
33. Arffman M, Ilanne-Parikka P, Keskimäki I, Kurkela O, Lindström J, Sund R, et al. FinDM Database on Diabetes in Finland. Finnish Institute for Health and Welfare (THL). Discussion Paper 19/2020 (2020). Helsinki, Finland. Available at: https://www.julkari.fi/bitstream/handle/10024/139578/URN_ISBN_978-952-343-492-9.pdf?sequence=1&isAllowed=y (Accessed 15th July 2021).
34. Lutski M, Shohat T, Mery N, Zucker I. Incidence and Risk Factors for Blindness in Adults With Diabetes: The Israeli National Diabetes Registry (INDR). Am J Ophthalmol (2019) 200:57–64. doi: 10.1016/j.ajo.2018.12.008
35. Løvaas KF, Cooper JG, Sandberg S, Røraas T, Thue G. Feasibility of Using Self-Reported Patient Data in a National Diabetes Register. BMC Health Serv Res (2015) 15(1):553. doi: 10.1186/s12913-015-1226-0
36. Lavens A, Doggen K, Mathieu C, Nobels F, Vandemeulebroucke E, Vandenbroucke M, et al. Clinical Action Measures Improve the Reliability of Feedback on Quality of Care in Diabetes Centres: A Retrospective Cohort Study. BMC Health Serv Res (2016) 16(1):424. doi: 10.1186/s12913-016-1670-5
37. Tinelli M, Petrou P, Samoutis G, Traynor V, Olympios G, McGuire A. Implementing Shared-Decision-Making for Diabetes Care Across Country Settings: What Really Matters to People? Health Policy (2017) 121(7):786–92. doi: 10.1016/j.healthpol.2017.05.001
38. Azzopardi J, Fava S. The Department of Health Diabetes Mellitus Health Information Technology Database in Malta. Malta Med School Gazette (2019) 3(2):40–5.
39. Chobot A, Polanska J, Brandt A, Deja G, Glowinska-Olszewska B, Pilecki O, et al. Updated 24-Year Trend of Type 1 Diabetes Incidence in Children in Poland Reveals a Sinusoidal Pattern and Sustained Increase. Diabetes Med (2017) 34(9):1252–8. doi: 10.1111/dme.13345
40. Pruna S, Purtill C, Massi Benedetti M, Carinci F, Di Iorio C, Beck P, et al. Screening for Diabetic Hypertension in Newly Diagnosed Type 2 Diabetes Using a New Technology That Carries Out in Minutes Agregated Data Analysis. Available at: http://www.acad.ro/sectii2002/proceedingsChemistry/doc2013-2/art02Pruna.pdf (Accessed 15th July 2021).
41. Dovc K, Telic SS, Lusa L, Bratanic N, Zerjav-Tansek M, Kotnik P, et al. Improved Metabolic Control in Pediatric Patients With Type 1 Diabetes: A Nationwide Prospective 12-Year Time Trends Analysis (Accessed 15th July 2021).
42. Ansari AS, de Lusignan S, Hinton W, Munro N, McGovern A. The Association Between Diabetes, Level of Glycaemic Control and Eye Infection: Cohort Database Study. Prim Care Diabetes (2017) 11(5):421–9. doi: 10.1016/j.pcd.2017.05.009
43. Rygh LH, Helgeland J, Håheim LL, Saunes IS, Joner G. Performance Indicators Based on Data From National Quality Registries. Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2008 Jan. Report from Norwegian Knowledge Centre for the Health Services (NOKC) No. 04-2008. Available from: https://europepmc.org/article/NBK/nbk464756 (Accessed September 22, 2021).
44. Nagy A, Kovács N, Pálinkás A, Sipos V, Vincze F, Szőllősi G, et al. Exploring Quality of Care and Social Inequalities Related to Type 2 Diabetes in Hungary: Nationwide Representative Survey. Available at: https://pubmed.ncbi.nlm.nih.gov/29326023/ (Accessed 16th July 2021).
45. Nano J, Carinci F, Okunade O, Whittaker S, Walbaum M, Barnard-Kelly K, et al. A Standard Set of Patient-Centered Outcomes for Diabetes Mellitus: Results of an International and Unified Approach (Accessed 6th July 2021).
46. Quinn LM, Davies MJ, Hadjiconstantinou M. Virtual Consultations and the Role of Technology During the COVID-19 Pandemic for People With Type 2 Diabetes: The UK Perspective. J Med Internet Res (2020) 22(8):e21609. doi: 10.2196/21609
47. European Parliament Resolution Addressing the EU Diabetes Epidemic. Available at: http://www.europarl.europa.eu/sides/getDoc.do?pubRef=-//EP//TEXT+TA+P7-TA-2012-0082+0+DOC+XML+V0//en (Accessed 6th July 2021).
48. Meza-Torres B, Cunningham S, Heiss C, Joy M, Leese GP, De Lusignan S, et al. High Quality and Timely Foot Care Predict Amputation-Free Survival Among People With Type 2 Diabetes: Results From a Large Population-Based Longitudinal Cohort in Scotland, Submitted.
49. Conway NT, Bluett M, Shields C, Taylor A, Wake DJ, Cunningham SG. A Longitudinal Perspective on User Uptake of an Electronic Personal Health Record for Diabetes, With Respect To Patient Demographics. J Diabetes Sci Technol (2021) 15(5):993–1004. doi: 10.1177/19322968211005734
50. European Commission. European Health Data Space: Combined Evaluation Roadmap and Inception Impact Assessment. Available at: https://ec.europa.eu/info/law/better-regulation/have-your-say/initiatives/12663-Digital-health-data-and-services-the-European-health-data-space_en (Accessed 15th July 2021).
51. Boeckhout M, Zielhuis GA, Bredenoord AL. The FAIR Guiding Principles for Data Stewardship: Fair Enough?(2018). Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6018669/ (Accessed 15th July 2021).
Keywords: diabetes, diabetes registries, quality of care, performance indicators, risk adjustment, health information
Citation: Carinci F, Štotl I, Cunningham SG, Poljicanin T, Pristas I, Traynor V, Olympios G, Scoutellas V, Azzopardi J, Doggen K, Sandor J, Adany R, Løvaas KF, Jarosz-Chobot P, Polanska J, Pruna S, de Lusignan S, Monesi M, Di Bartolo P, Scheidt-Nave C, Heidemann C, Zucker I, Maurina A, Lepiksone J, Rossing P, Arffman M, Keskimäki I, Gudbjornsdottir S, Di Iorio CT, Dupont E, de Sabata S, Klazinga N and Benedetti MM (2021) Making Use of Comparable Health Data to Improve Quality of Care and Outcomes in Diabetes: The EUBIROD Review of Diabetes Registries and Data Sources in Europe. Front. Clin. Diabetes Healthc. 2:744516. doi: 10.3389/fcdhc.2021.744516
Received: 20 July 2021; Accepted: 08 September 2021;
Published: 11 October 2021.
Edited by:
Panayiotis V. Benos, University of Pittsburgh, United StatesReviewed by:
Ricardo Gómez-Huelgas, Regional University Hospital of Malaga, SpainKlaus Piwernetz, Medimaxx Health Management GmbH, Germany
Copyright © 2021 Carinci, Štotl, Cunningham, Poljicanin, Pristas, Traynor, Olympios, Scoutellas, Azzopardi, Doggen, Sandor, Adany, Løvaas, Jarosz-Chobot, Polanska, Pruna, de Lusignan, Monesi, Di Bartolo, Scheidt-Nave, Heidemann, Zucker, Maurina, Lepiksone, Rossing, Arffman, Keskimäki, Gudbjornsdottir, Di Iorio, Dupont, de Sabata, Klazinga and Benedetti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabrizio Carinci, fabrizio.carinci@unibo.it