The Impact of Medical Terminology in Self-Triage Decision-Making
 Maria C. D’Angelo
Maria C. D’Angelo Karin R. Humphreys
Karin R. Humphreys Timmie Li
Timmie Li Meredith E. Young
Meredith E. Young- 1Department of Psychology, Neuroscience, and Behaviour, McMaster University, Hamilton, ON, Canada
- 2Department of Medicine, McGill University, Montreal, QC, Canada
- 3Center for Medical Education, McGill University, Montreal, QC, Canada
Objective: The present study examined whether medical terminology impacts self-triage decisions (deciding if and when to seek medical treatment) compared to lay terminology.
Methods: Undergraduate psychology student participants read 32 hypothetical health scenarios and reported how urgently they would seek care [“In this situation, when would you seek medical attention?” presented along with a seven-point scale, with anchors at either extreme: “Never (At the next scheduled appointment, if at all)” and “As soon as possible (Within the hour),” reflecting the options coded as 1 and 7, respectively]. Data were collected in person via a paper-based questionnaire. Scenarios included a description of symptoms, which were labeled as consistent with a particular medical disorder using either a lay disease label (e.g. “Heart Attack”) or medical terminology (e.g. “Myocardial Infarction”). The 32 health scenarios represented medical disorders that purposefully reflected a spectrum of severity, commonality, and how recently the medical terminology had entered common use.
Results: For disorders for which medical terminology has been more recently established, participants reported that they would seek care more urgently when the disorder was presented using a medical label [mean (SE) = 4.08 (0.23)] than when they were described using the lay disease labels [3.32 (0.23), t(35) = 5.36, p < 0.001, e.g., “seborrheic dermatitis” versus “chronic dandruff”]. However, this differential response to medical or lay disease labels was not observed for disorders for which medical terminology has been more well established [medical labels = 5.16 (0.18); lay labels = 4.89 (0.18), t(35) = −1.67, p = 0.104, e.g., “heart attack” and “myocardial infarction”].
Conclusion: These results indicate that self-triage decision-making can be readily influenced by the terminology used to identify a disorder; however, this phenomenon appears to be particularly relevant for disorders in which public opinion may still be in flux.
Medical decision-making is a very complex task (Higgs and Jones, 2000; Eva, 2005) and even expert clinicians have difficulty with the ambiguity inherent in many clinical symptoms (Brooks et al., 1991, 2000; Zarin and Earls, 1993; Hatala et al., 1999; LeBlanc et al., 2001, 2002; Groves et al., 2003). Issues of symptom identification and medical decision-making exist for patients as well, as we all have to decide whether something is “strange” or “bad enough” to seek medical attention, and patients often have to make health decisions without the benefit of medical expertise (Redelmeier et al., 1993; MacKichan et al., 2017). While many treatment decisions are made through exercises in shared decision-making (where patients and physicians are both involved in treatment decisions, e.g., Charles et al., 1997; Frosch and Kaplan, 1999; Godolphin, 2009) or patient-centered care (where patients are at the core of medical decisions, e.g., Stewart et al., 2000), one example of decision-making that rests entirely with an individual is deciding when, and how urgently, to seek out medical care (previously labeled as self-triage decision-making; Cooper and Humphreys, 2008; Hall et al., 2010; Morita et al., 2017). To add a layer of complexity, many individuals face the difficulty of making self-triage decisions in the context of high levels of uncertainty, both in deciding whether their symptoms merit medical attention at all, and when faced with a wealth of potential diagnoses. Individual decisions are rendered even more complex and dynamic with the influence of potentially unreliable or overly fear mongering (Gladwell, 1995) information from a variety of health information sources and the unfamiliar language of medical symptoms and diagnoses (Young et al., 2008). Previous work has found that perceptions of the severity of disorders are influenced by the use of medical language (Young et al., 2008), where conditions described using medical terminology were seen as more serious and more representative of a disease. Previous work has also found that self-triage decisions are influenced by uncertainty (Cooper and Humphreys, 2008; Hall et al., 2010); however, we know little regarding how medical terminology and uncertainty interact in the context of self-triage decision-making. The purpose of the present study was to examine whether self-triage decisions are influenced by the terminology used to describe potential diagnoses.
Self-Triage Decision-Making
Difficulty identifying signs and symptoms for the lay individual invariably influences the amount of time before medical care is sought (Burnett et al., 2005) and experimental research demonstrates that uncertainty can influence the hypothetical medical decisions of young, healthy individuals (Cooper and Humphreys, 2008; Hall et al., 2010). These experimental investigations of decision-making suggest that factors such as certainty, severity, and the presence of alternate potential diagnoses influence the self-triage process. By manipulating the certainty [you have (diagnosis X), versus you may have (diagnosis X)] of the suggested diagnosis as well as the severity [(diagnosis X) could be a common cold or a brain aneurysm] of various hypothetical situations, Cooper and Humphreys were able to determine the role of each on the urgency with which participants report they would seek care. As one might predict, participants reported seeking care more urgently when suggested that they might have a more serious condition rather than a less serious one. Interestingly, an interaction was found between the severity of the suggested disorder and the certainty of that suggested diagnosis. Meaning, when participants were given scenarios with moderate or high severity disorders, participants responded with higher urgency ratings (on a 7-point scale) when given definitive diagnoses than when the diagnoses were suggested, and ratings of urgency were even lower when no diagnosis was provided. Conversely, with increasing certainty for low severity disorders, participants responded that they would seek care with less urgency. In summary, if it could be a serious condition (e.g. meningitis), participants reported being willing to seek treatment quickly and when it was most likely not a serious medical condition (e.g. a viral infection), they were less likely to report seeking urgent care. In addition, when given a definitive diagnosis, participants reported being willing to seek treatment more quickly than when given a suggested diagnosis that was less certain.
Hall et al. (2010) examined the influence of presenting multiple possible diagnoses on self-triage decisions. In their study, participants saw hypothetical health scenarios where a cluster of symptoms could be presented with either a high severity disorder, a low severity disorder, or with a differential diagnosis including both the high and low severity disorders. Participants rated that they would seek care more urgently for the high severity disorder (5.0 on a seven-point scale) than for the low severity disorder (3.6). More importantly, when participants saw the differential diagnosis containing both the high and the low severity disorders, they reported that they would seek care less urgently than when presented with the high severity disorder alone (4.6). These results indicate that self-triage decisions can be influenced by something as simple as the number of potential diagnoses listed or considered. In summary, previous research in this domain suggests that uncertainty plays an important role in self-triage decision-making. However, a question that remains is whether other forms of uncertainty, such as uncertainty that is induced by the use of unfamiliar terminology, also influence self-triage decision-making.
The Effects of Using Medical Terminology
In addition to the presentation of multiple possible diagnoses, many potential diagnosis and symptom labels are frequently presented to lay individuals in complex medical language—often referred to as “medicalese” (Eva et al., 2001; Norman et al., 2003; Young et al., 2008). Medicalese refers to the use of specialized language to refer to medical disorders by using Latin or Greek derivatives (e.g., “Myalgic Encephalopathy”) or using English-based technical terms that connote a special medical status (e.g., “Gastroeophageal Reflux Disease”). Overall, a disease presented in medical language is typically considered to be more severe, more representative of a disease, and less prevalent (Eva et al., 2001; Norman et al., 2003; Young et al., 2008). Interestingly, medical language has been demonstrated to influence the perceptions of not only lay individuals (Young et al., 2008), but also early medical learners and practitioners (Eva et al., 2001; Eva and Wood, 2003; Norman et al., 2003). However, some research suggests that this influence of language may be limited to newly medicalized disorders—disorders where the medical language is still quite new, and perhaps poorly recognized (Young et al., 2008) and that this use of medical language may be involved in changing public perceptions of newly medicalized disorders (Young et al., 2008). But perceptions of severity, disease representativeness, prevalence, and personal risk (Young et al., 2013) may not be perfectly analogous to patient decisions of when to seek care (i.e. self-triage decision-making). One might think a disorder is serious and a representative example of a disease, but it may not influence how quickly one would seek medical care. Perhaps even more importantly, it is possible that the use of a medical label for a disorder may increase the urgency with which one would seek care compared to the same disorder when presented using a lay label.
The Present Study
The purpose of the present study was to investigate the role of medical and lay terminology on how urgently individuals report that they would seek care. The use of healthy undergraduates and hypothetical health scenarios to investigate the urgency to seek care has been used previously (Cooper and Humphreys, 2008; Hall et al., 2010), and a similar population and questionnaire-based experimental approach were used here to determine the influence, if any, of medical terminology on self-triage decision-making. If this influence can be established, this will be a clear addition to previous findings indicating that medical terminology can influence perceptions of risk (Song and Schwarz, 2009; Topolinski and Strack, 2010; Young et al., 2013; Dohle and Siegrist, 2014; Tasso et al., 2014), and perceptions of severity and disease status (Young et al., 2008).
Method
Participants
Thirty-six psychology undergraduate students (24 females) from McMaster University participated in exchange for partial course credit. Previous work (Frewer et al., 2002) have found that perceptions of risk are more extreme in lay, older, and less educated populations, and responses are more likely to be heterogeneous within heterogeneous population. Given this study is an initial investigation into the impact of medical terminology on self-reported ratings of urgency, we opted to rely on a healthy undergraduate population in order to isolate, to the best of our ability, the influence of medical terminology on self-triage decision-making. Inclusion criteria included being of native or near-native English fluency. The study was described on the available on-line platform hosted by the Undergraduate Psychology Program at McMaster University (available to all registered students), and potential participants self-selected to participate through the on-line platform, and respondents are typically first or second year students enrolled in courses in the Psychology, Neuroscience, and Behavior Department at McMaster University. This study received approval from the McMaster University Research Ethics Board.
Procedure
Participants were briefed regarding the study protocol and provided written consent. Participants completed a paper and pencil questionnaire including 32 hypothetical health scenarios (see the Appendix for examples of these scenarios). As part of the protocol, the experimenter emphasized that for each scenario, participants were to imagine that they were experiencing the given symptoms and had learned that these symptoms were consistent with a particular medical disorder. For each hypothetical scenario, participants were told to indicate, to the best of their judgment, how urgently they would seek care [on a seven-point scale anchored “Never (At the next scheduled appointment, if at all)” and “As soon as possible (Within the hour)”], a scale previously used within similar study contexts, with a similar study population by Cooper and Humphreys (2008) and Hall et al. (2010). Participants were given an opportunity after each scenario to list any words that they did not recognize. After completing the questionnaire, participants were debriefed regarding the specific purposes of the experiment and invited to ask any questions they might have. Participants were encouraged to complete the study within 1 h, which based on previous studies (Cooper and Humphreys, 2008; Young et al., 2008; Hall et al., 2010) provided ample time. Participants were responsible for self-pacing throughout the study.
Materials
Hypothetical health threat scenarios were created based on the protocol described in Cooper and Humphreys (2008) and modified to investigate the differential influence of medical and lay terminology on self-triage decisions. Disorders included in this study were purposely chosen to represent a breath of severity, commonality, and likely familiarity (specifically how long the medical language label had been in common use). Each scenario contained three to four symptoms along with a suggested diagnosis consistent with the listed symptoms. The symptoms and associated disorder were unique to each hypothetical health scenario. Each scenario ended with the question “In this situation, when would you seek medical attention?” presented along with a seven-point scale, with the following anchors at either extreme: “Never (At the next scheduled appointment, if at all)” and “As soon as possible (Within the hour),” reflecting the options coded as 1 and 7, respectively. Ratings from this seven-point scale are referred to as urgency ratings. Example scenarios are presented in the Appendix.
Four versions of the study questionnaire were created, each containing a total of 34 hypothetical health scenarios, in order to counterbalance the language of presentation (either lay or medical label for each disorder) and the order of presentation of the disorders. Sixteen of the hypothetical health scenarios in each questionnaire were related to the purpose of the present study and are described here. The remaining scenarios were part of a larger, on-going study of factors influencing self-triage decisions, and are unpublished data. To investigate the role of medical language on the reported urgency to seek care, medical and lay language stimuli from Young et al. (2008) were adapted to create hypothetical health scenarios. The medical disorders included eight disorders that were classified as “newly medicalized,” which were defined as having a medical term introduced or come to popular use within approximately the last 15 years (e.g., erectile dysfunction disorder) and eight recognized medical disorders, which were defined as having had a lay and medical term in popular use for more than 15 years (e.g., hypertension). These two types of disorders, along with their respective disorder types and labels are shown in Table 1. Disorders were described using a medical label or a lay label (counterbalanced across participants, so no participant saw both the medical and lay label for the same disorder). Information regarding the justification and verification of these categories can be found elsewhere (Young et al., 2008).
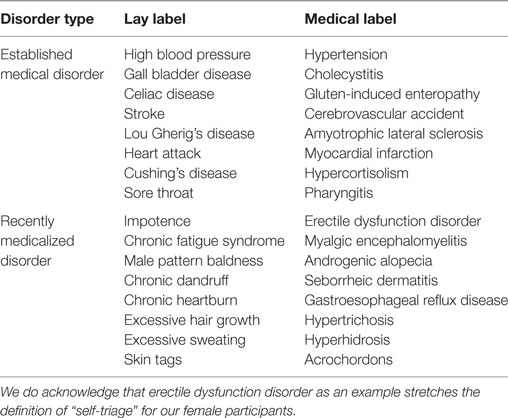
Table 1. List of lay and medical labels used and associated category assignments.
Importantly, every questionnaire contained scenarios describing each of the eight recently medicalized disorders, and eight established disorders (total of 16 hypothetical health scenarios). For each type of disorder (recently medicalized/established) half of these scenarios in each questionnaire described the disorder using the medical label, and other half of the scenarios described the disorder using the lay label.
Analysis
In order to examine the impact of medical terminology on ratings of reported urgency to seek care, an Analysis of Variance was conducted with type of disorder (recently medicalized/established) and terminology (medical/lay) as the within subjects factors of interest. Based on previous work (Young et al., 2008), planned comparisons (t-tests) were conducted for the recently medicalized and established disorders to specifically examine the influence of medical versus lay terminology.
Results
Mean urgency ratings as a function of the type of disorder and type of language used are shown in Table 2. Mean urgency ratings were submitted to an analysis of variance with type of disorder (recently medicalized/established), label type (medical/lay), and symptom cluster (16 clusters, one for each of the disorders listed in Table 1) as within subject factors. Participants reported that they would seek medical care more urgently when the disorder was described using the medical label (mean = 4.59, SE = 0.19) than when described using the lay label (mean = 4.06, SE = 0.19) [F(1, 33) = 33.75, , p < 0.001]. Participants reported that they would seek medical care more urgently for the established medical disorders (mean = 4.99, SE = 0.17) than for the recently medicalized disorders (mean = 3.65, SE = 0.22) [F(1, 33) = 77.89, , p < 0.001]. Despite a larger numerical difference between the means for the lay and medical labels in the recently medicalized disorders, the interaction between language and disorder type was only marginally significant, F(1, 33) = 2.48, , p = 0.063 (one-tailed).
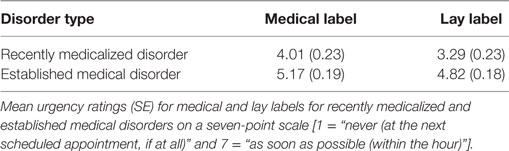
Table 2. Mean urgency ratings as a function of the type of disorder and type of language used.
Although the interaction between label type and type of disorder was only marginally significant, planned t-tests were conducted to compare the effect of label type (medical/lay) on ratings of urgency separately for recently medicalized and established medical disorders, due to findings previously reported (Young et al., 2008). For recently medicalized disorders, participants reported that they would seek medical care more urgently when the disorders were described with the medical labels (mean = 4.08, SE = 0.23) than when they were described using the lay disease labels (mean = 3.32, SE = 0.23), t(35) = 5.36, p < 0.001. For established medical disorders, the difference in urgency ratings did not differ across language of the disorder label [medical labels: mean = 5.16, SE = 0.18; lay labels: mean = 4.89, SE = 0.18, t(35) = −1.67, p = 0.104].
Discussion
The purpose of the present study was to examine whether the use of medical labels influences health-care-seeking behavior in healthy young adults. To that end, we conducted an experimental questionnaire-based study where participants were asked to rate how urgently they would seek medical care after imagining that they were experiencing the listed cluster of symptoms and had learned that their symptoms were consistent with a provided potential diagnosis. In order to isolate the role of medical terminology on reported urgency of care-seeking behavior (or self-triage decision-making), participants were asked to report how quickly they would seek care for disorders that were labeled using either lay-language terminology (e.g., “sore throat”) or medical terminology (e.g., “pharyngitis”). Further, we investigated the magnitude of the influence of medical terminology on both well-established medical disorders (such as “hypertension”) and newly established or newly re-labeled medical disorders (such as “erectile dysfunction disorder”). In summary, the results of the present study indicate that when diseases were presented using their medical terminology label (e.g. “androgenic alopecia”), participants considered the diseases to warrant more urgent care than when the same disease was presented using a lay English label (e.g., “male pattern baldness”). Further, participants appear to demonstrate this differential weighting of medical terminology primarily for medical disorders that have been recently medicalized (e.g., “hyperhidrosis” versus “excessive sweating”). The results from this study support the notion that medical terminology influences the urgency with which individuals report that they would seek medical care.
It is important to note that the recently medicalized and the established diseases do differ in severity (Young et al., 2008), making it unsurprising that participants reported that they would seek health care more urgently for diseases considered to be well established (e.g., “hypertension”) than for newly medicalized disorders (e.g., “gastroesophageal reflux disease”), and the findings of this study are consistent with previous work demonstrating that severity influences self-triage decisions (Cooper and Humphreys, 2008; Hall et al., 2010). It is also possible that participants interpreted the urgency scale in this study inappropriately and relied on perceptions of illness base rates to ground their ratings of urgency, meaning that they may have reported that they would seek care more urgently for disorders they perceived to have higher base rates. This possibility seems unlikely, given that Young et al. (2008) have found that individuals consider the newly medicalized disorders to be more serious, more representative of a disease, and, importantly, less prevalent when presented in the medical rather than lay disease label. Young et al.’s (Young et al., 2008) findings suggest that the increased likelihood to seek care for newly medicalized disorders presented with medical language labels in the present study is not due to an individual thinking that, for example, “gastroesophageal reflux disease” is more common than “chronic heartburn.” Therefore, the increased urgency with which individuals report they would seek care is unlikely to be explained by participants relying on base-rate probabilities (Jemmott et al., 1986), or their personal perceptions of risk (Coombs and Slovic, 1979).
In the present study, medical labels, compared to their lay English equivalent, were associated with higher urgency ratings in recently medicalized disorders, but no such pattern was seen in established disorders. This result replicates a similar pattern of results that was reported by Young et al. (2008) using different measures of the perceptions of illness severity. We propose that medical labels may induce uncertainty in lay populations; perhaps the labels sound unfamiliar, which may underlie the increased urgency ratings seen here. Song and Schwarz (2009) found that food additives were perceived as riskier when their names were harder to pronounce, an effect that was mediated by the perceived familiarity of the names. This fluency of processing acts as a heuristic cue for intuitive judgments of risk (Schwarz et al., 2009). Dohle and Siegrist (2014) also found fluency of name pronunciation to influence perceptions of drug risk. Even when individuals were presented with an attribute that was easier to evaluate, like price, the name of the drug was an important criterion for most participants for evaluating side effects and willingness to purchase. It is important to recognize that this fluency effect is dependent on the context of the initial judgment. Previous studies report reverse fluency effects, where disfluency is interpreted positively, in instances where traits associated with disfluency, like unfamiliarity, were considered positive (Pocheptsova et al., 2010; Galak and Nelson, 2011; Cho, 2015). Cho (2015) replicated Dohle and Siegrist’s (Dohle and Siegrist, 2014) findings that complex drug names were perceived as riskier, but found that the same complex drug names were also perceived as more technologically advanced. When asked to estimate the likelihood of FDA approval, individuals who had rated the drug names for advancedness perceived the complex drug names as more likely to be approved. In contrast, individuals who had rated the names for riskiness perceived complex names as less likely to be approved. The context of a judgment (e.g., advancedness versus risk) determined the direction of effect for fluency on perceptions (Cho, 2015). The present study represents a situation where disfluency may be interpreted as uncertainty and associated with increased urgency to seek medical care. Considering that the effect of heuristic cues is more pronounced when individuals are under stress (Chaiken, 1987) or in the presence of uncertainty (Kahneman, 2003), decision-making, when ill and potentially facing uncertain medical terminology or diagnoses, can be especially prone to biases that may negatively impact individual or public health. Therefore, patient-generated data in the context of actual decisions may show an even greater effect of newly medicalized terms on care-seeking urgency; however, this was beyond the scope of this study.
The lack of differential response to lay and medical labels for disorders with well-established terminology is consistent with Dohle and Siegrist’s (Dohle and Siegrist, 2014) suggestion that heuristics like fluency would have a greater impact on newer drug products. This induction of uncertainty may mimic the pattern of results seen in Cooper and Humphreys (2008), where uncertainty resulted in increased ratings of urgency for disorders that were moderate or high in severity. Interestingly, Hall et al. (2010) demonstrated that the presence of a differential diagnosis (an analog to increasing uncertainty) resulted in a paradoxical drop in ratings of self-reported care-seeking urgency. It is possible then, that the results presented here demonstrate not an uncertainty of diagnosis, but an uncertainty of what the newly medicalized terminology means. Therefore, it may be the case that with increased uncertainty regarding the meaning of a disease label, individuals are more inclined to consult someone who understands what the “jargon”—or medical terminology—means, such as a physician. Consistent with this, Rosen and Knäuper (2009) demonstrated that individuals placed in an uncertain situation regarding a fictitious sexually transmitted infection (STI) were more likely to seek additional information regarding the fictitious STI than individuals who were placed in a more certain situation regarding the same STI. Research on the health communication via medical disclosure and consent documentation also found that patients experienced less uncertainty when viewing documentation with both medical terminology and their corresponding lay terminology, than with just the medical terminology alone (Donovan et al., 2014). Within the taxonomy of uncertainty in health communication established by Babrow et al. (1998), uncertainty arises from five domains: complexity, quality of information, probability, structure of information, and lay epistemology. The uncertainty of what newly medicalized terminology may mean can be described as a lack of clarity, a sub-domain of quality of information, whereas an uncertainty of diagnosis would fall within the domain of probability—the perceived likelihood of a particular outcome or the presence of a range of possibilities (Babrow et al., 1998). The source of uncertainty can influence the impact of uncertainty on decision, as demonstrated by the divergent effects of uncertainty on ratings of self-reported care-seeking urgency observed in this study and Hall et al. (2010), and it is important to recognize the differences in the source of the uncertainty, in order to appropriately manage it (Han et al., 2011).
Finally, recent research has demonstrated a strong role for the linguistic properties of product labels in decisions of risk—if a food additive (Song and Schwarz, 2009) or drug (Dohle and Siegrist, 2014) was difficult to pronounce, it was considered to be more risky than one that was easy to pronounce. If such simple linguistic phenomena, such as ease of pronunciation, or having English language versus Latinate-sounding terminology in medicine (Eva et al., 2001; Norman et al., 2003; Young et al., 2008), can consistently influence our decisions regarding safety, severity, and care-seeking behavior, it offers caution for public communication and presentation of health information. Tasso et al. (2014) warned against the use of drug names that suggested their expected outcome because they were perceived as more effective and less risky than names that had no meaning or alluded to the target health issue. For example, participants perceived drug names like Dermosan, referring to its expected outcome of healthy (san) skin (dermo), to be more effective and less risky than names like Dermomal, referring to its target health issue of unhealthy (mal) skin (dermo). Ethical issues with regards to language choice arise when language is shown to readily bias perceptions and health behavior intention. Bokhour and Kressin (2015) expressed a similar concern toward potentially misinterpreted disorder labels, like hypertension, suggesting individual labels may carry their own semantic and cognitive biases. Despite being an established medical label for high blood pressure due to elevated arterial tension, hypertension is often misinterpreted as excessive general tension or stress. Associations between blood pressure and stress, although commonly held, remain controversial and unclear, especially with regards to the etiology and management of hypertension (Bokhour and Kressin, 2015). As a result, patients may rely on psychological stress relief and discount the value of non-psychological interventions like diet, exercise, or antihypertensive medication. The presentation of this medical label, or other potentially misinterpreted labels, may influence self-triage, self-care management, and medication adherence (Bokhour and Kressin, 2015). New medical labels should consider conflicting perceptions of lay labels and potential misinterpretations, as well as the implicit influence of language on perception and decision-making. Further research should investigate label-specific biases to inform appropriate language choice for health communications, as well as methods for preventing cognitive biases like fluency. Topolinski and Strack (2010) replicated Song and Schwarz’s (Song and Schwarz, 2009) findings of increased risk perceptions for more complex food additive names and found that a simultaneous oral sensorimotor task, like chewing, prevented this bias. Individuals who chewed on a cereal bar while reading food additive names reported similar levels of risk perception for both easy-to-pronounce names and hard-to-pronounce names. Topolinski and Strack (2010) took these findings as support for the notion that the ease of covert sensorimotor simulation drives fluency-based cognitive biases. Secondary sensorimotor tasks block these simulations, thereby reducing fluency effect. Whereas other approaches require additional post hoc processing to correct biases, the process proposed by Topolinski and Strack (2010) prevents the biases by blocking the processes responsible and is more applicable to the context of online health information seeking, where additional judgmental corrections are not convenient or readily available.
This study is not without limitations. A population of healthy undergraduates was used, and asked to imagine hypothetical medical scenarios. While this is not perfectly equivalent to individuals in crisis making decisions of when to seek care, we believe that the protocol used here, and in previous work (Cooper and Humphreys, 2008; Hall et al., 2010), provide a well-controlled environment in which to investigate infrequent and potentially high-risk health decisions, and examine perceptions of medical conditions. Notably, these results do not perfectly generalize to a patient population, an older or less educated population (Frewer et al., 2002), or individuals making health decisions on another’s behalf (e.g., parents making health decisions about their child), this remains an important direction for future research. Additionally, this study was designed as a within-subjects study, with little opportunity to investigate the role of culture (e.g., Kirmayer, 1992), personal experience, nor familiarity with medical terminology. This study was also unable to investigate the likely iterative and interactional effects of individuals seeking information to help support self-triage decision-making. While beyond the scope of this study, the influence of culture, individual differences, and contextual and interactive factors remain important avenues for future research. Finally, any effects of terminology need to be interpreted within a particular linguistic and cultural context, and it remains unclear the extent to which these results would generalize to languages other than English, or other cultural contexts.
Importantly, this study clearly identifies terminology as an influence on self-reported urgency to seek medical care. Understanding the specific factors that underlie the influence of medical terminology, identifying influences on patient decisions to seek care, and evaluating their interactions are important for improving medical communication generally and patient–physician communication specifically, as well as the effective design and use of public health campaigns. Physicians should consider the impact of previous exposure to lay or medical labels on patients’ sense of urgency for care and perceptions of disease characteristics (Young et al., 2008), as well as the impact of their own choice of disease label during patient–physician communication. Patients reported preferring physicians’ use of medical labels because it validated their illness and enhanced their views of their physician’s professionalism (Ogden et al., 2003). Consistent with findings that lay labels are perceived as less severe, less representative of disease, and more prevalent (Young et al., 2008), patients also felt a physician’s use of lay labels indicated that the disease was less worrisome and would subside quickly (Ogden et al., 2003). Based on this growing body of work, physicians should also avoid instances where particular labels may be misinterpreted and as a result, undermine treatment (Bokhour and Kressin, 2015). The optimal terminology to be used by physicians in consultations depends on the language used by patients and the intended outcome. Williams and Ogden (2004) found increased patient–physician rapport, patient communication comfort, and patient compliance intent when physicians used the same labels as their patients.
The importance of medical terminology can also be observed outside of a physical patient–physician interaction. This study focused on the terminology seen in the context of fictional self-triage decisions, the role of uncertainty in light of different self-posited diagnoses is particularly important given our technologically and informationally rich environment, where individuals seek much of their health information online. With individuals reporting self-triage as one of the primary reasons for online health information seeking (Bowes et al., 2012), decisions to seek care are now influenced by publically available information, most of which is found on the Internet (Morahan-Martin, 2004). More specifically, searching for health information may actually escalate health concerns (White and Horvitz, 2009; Fergus, 2013) and health information “facts” are often hard to find and are rarely contained within the same information site (Benigeri and Pluye, 2003). Further, information on the Internet is not always reliable (Diaz et al., 2002), frequently includes multiple possible diagnoses that range in severity, and diseases are often presented in technical or medical terminology (e.g. “medicalese”; Eva et al., 2001; Norman et al., 2003; Young et al., 2008).
With advances in information technology, the importance of terminology also extends to interactions with tools for medical decision-making (Nijland et al., 2008). Decision aids, like the strategy for off-site rapid triage, a web-based decision aid designed in response to the 2009 H1N1 influenza pandemic, aim to provide better informed decision-making during times of medical crisis (Kellermann et al., 2010). Dolan et al. (2015) demonstrated that user decision outcomes varied with the presentation of labels during decision aid use, suggesting that decision aids need to consider conscious and unconscious biases to be maximally effective. The present findings demonstrate that language of presentation can be a crucial consideration for patient communication, including the methods for designing decision-aid tools.
Ethics Statement
This study received approval from the McMaster University Research Ethics Board. Participants were briefed regarding the study protocol by MD and provided written consent. This study was carried out in accordance with the recommendations of the McMaster University Research Ethics Board with written informed consent from all participants. All participants gave written informed consent in accordance with the Declaration of Helsinki.
Author Contributions
MD aided in the conceptualization and execution of the study. She was primarily responsible for data analysis and partial drafting of the manuscript. She critically reviewed the manuscript and approved its final form. KH aided in the conceptualization of the study, and assisted with data analysis and interpretation. She critically revised the manuscript and approved its final form. TL assisted in data interpretation and critical revisions of the manuscript. He approved the final manuscript. MY assisted in the conceptualization of the study, assisted in data analysis and interpretation, critical review of the manuscript, and approved of its final form.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The authors would like to thank the members of the Cognitive Science Laboratory at McMaster University for their assistance throughout this project. This work was supported by Natural Sciences and Engineering Council of Canada (NSERC) grant #293145 to KH, and by a master’s and a doctoral NSERC Canada Graduate Scholarship to MD.
References
Babrow, A. S., Kasch, C. R., and Ford, L. A. (1998). The many meanings of uncertainty in illness: toward a systematic accounting. Health Commun. 10, 1–23. doi: 10.1207/s15327027hc1001_1
Benigeri, M., and Pluye, P. (2003). Shortcomings of health information on the Internet. Health Promot. Int. 18, 381–386. doi:10.1093/heapro/dag409
Bokhour, B. G., and Kressin, N. R. (2015). What is in a name? How biomedical language may derail patient understanding of hypertension. Circ. Cardiovasc. Qual. Outcomes 8, 452–454. doi:10.1161/CIRCOUTCOMES.114.001662
Bowes, P., Stevenson, F., Ahluwalia, S., and Murray, E. (2012). ‘I need her to be a doctor’: patients’ experiences of presenting health information from the Internet in GP consultations. Br. J. Gen. Pract. 62, 732–738. doi:10.3399/bjgp12X658250
Brooks, L. R., LeBlanc, V. R., and Norman, G. R. (2000). On the difficulty in noticing obvious features in patient appearance. Psychol. Sci. 11, 112–117. doi:10.1111/1467-9280.00225
Brooks, L. R., Norman, G. R., and Allen, S. W. (1991). Role of specific similarity in a medical diagnostic task. J. Exp. Psychol. Gen. 120, 278–287. doi:10.1037/0096-3445.120.3.278
Burnett, R. E., Blumenthal, J. A., Mark, D. B., Leimberger, J. D., and Califf, R. M. (2005). Distinguishing between early and late responders to symptoms of acute myocardial-infarction. Am. J. Cardiol. 75, 1019–1022. doi:10.1016/S0002-9149(99)80716-4
Chaiken, S. (1987). “The heuristic model of persuasion,” in Social Influence: The Ontario Symposium, eds M. P. Zanna, J. M. Olson, and C. P. Herman (Hillsdale, NJ: Erlbaum), 3–39.
Charles, C., Gafni, A., and Whelan, T. (1997). Shared decision-making in the medical encounter: what does it mean? (Or it takes at least two to tango). Soc. Sci. Med. 44, 681–692. doi:10.1016/S0277-9536(96)00221-3
Cho, H. (2015). The malleable effect of name fluency on pharmaceutical drug perception. J. Health Psychol. 20, 1369–1374. doi:10.1177/1359105314525486
Coombs, B., and Slovic, P. (1979). Newspaper coverage of causes of death. Journalism Q. 56, 837–843. doi:10.1177/107769907905600420
Cooper, A. A., and Humphreys, K. R. (2008). The uncertainty is killing me: self-triage decision making and information availability. Electron. J. Appl. Psychol. 4, 1–6. doi:10.7790/ejap.v4i1.124
Diaz, J. A., Griffith, R. A., Ng, J. J., Reinert, S. E., Friedmann, P. D., and Moulton, A. W. (2002). Patients’ use of the Internet for medical information. J. Gen. Intern. Med. 17, 180–185. doi:10.1046/j.1525-1497.2002.10603.x
Dohle, S., and Siegrist, M. (2014). Fluency of pharmaceutical drug names predicts perceived hazardousness, assumed side effects and willingness to buy. J. Health Psychol. 19, 1241–1249. doi:10.1177/1359105313488974
Dolan, J., Cherkasky, O., Chin, N., and Veazie, P. (2015). Decision aids: the effect of labeling options on patient choices and decision making. Med. Decis. Making 35, 979–986. doi:10.1177/0272989X15598532
Donovan, E. E., Crook, B., Brown, L. E., Pastorek, A. E., Hall, C. A., Mackert, M. S., et al. (2014). An experimental test of medical disclosure and consent documentation: assessing patient comprehension, self-efficacy, and uncertainty. Commun. Monogr. 81, 239–260. doi:10.1080/03637751.2013.876059
Eva, K. W. (2005). What every teacher needs to know about clinical reasoning. Med. Educ. 39, 98–106. doi:10.1111/j.1365-2929.2004.01972.x
Eva, K. W., Brooks, L. R., and Norman, G. R. (2001). Does “shortness of breath” = “dyspnea”? The biasing effect of feature instantiation in medical diagnosis. Acad. Med. 76, S11–S13. doi:10.1097/00001888-200110001-00005
Eva, K. W., and Wood, T. J. (2003). Can the strength of candidates be discriminated based on ability to circumvent the biasing effect of prose? Implications for evaluation and education. Acad. Med. 78, s78–s81. doi:10.1097/00001888-200310001-00025
Fergus, T. A. (2013). Cyberchondria and intolerance of uncertainty: examining when individuals experience health anxiety in response to Internet searches for medical information. Cyberpsychol. Behav. Soc. Netw. 16, 735–739. doi:10.1089/cyber.2012.0671
Frewer, L. J., Miles, S., and Marsh, R. (2002). The media and genetically modified foods: evidence in support of social amplification of risk. Risk Anal. 22, 701–711. doi:10.1111/0272-4332.00062
Frosch, D. L., and Kaplan, R. M. (1999). Shared decision making in clinical medicine: past research and future directions. Am. J. Prev. Med. 17, 285–294. doi:10.1016/S0749-3797(99)00097-5
Galak, J., and Nelson, L. D. (2011). The virtues of opaque prose: how lay beliefs about fluency influence perceptions of quality. J. Exp. Soc. Psychol. 47, 250–253. doi:10.1016/j.jesp.2010.08.002
Godolphin, G. (2009). Shared decision making. Healthc. Q. 12(Suppl), e186–e190. doi:10.12927/hcq.2009.20947
Groves, M., O’Rourke, P., and Alexander, H. (2003). Clinical reasoning: the relative contribution of identification, interpretation, and hypothesis errors to misdiagnosis. Med. Teach. 25, 621–625. doi:10.1080/01421590310001605688
Hall, E. C., Cooper, A. A., Watter, S., and Humphreys, K. R. (2010). The role of differential diagnoses in self-triage decision making. Appl. Psychol. 2, 35–51. doi:10.1111/j.1758-0854.2009.01021.x
Han, P. K., Klein, W. M., and Arora, N. K. (2011). Varieties of uncertainty in health care: a conceptual taxonomy. Med. Decis. Making 31, 828–838. doi:10.1177/0272989X11393976
Hatala, R., Norman, G. R., and Brooks, L. R. (1999). Research basic to medical education: influence of a single example on subsequent electrocardiogram interpretation. Teach. Learn. Med. 11, 110–117. doi:10.1207/S15328015TL110210
Higgs, J., and Jones, M. (2000). Clinical Reasoning in the Health Professions. Avon, Great Britain: Elsevier Ltd.
Jemmott, J. B., Ditto, P. H., and Croyle, R. T. (1986). Judging health status: effects of perceived prevalence and personal relevance. J. Pers. Soc. Psychol. 50, 899–905. doi:10.1037/0022-3514.50.5.899
Kahneman, D. (2003). A perspective on judgment and choice: mapping bounded rationality. Am. Psychol. 58, 697. doi:10.1037/0003-066X.58.9.697
Kellermann, A. L., Isakov, A. P., Parker, R., Handrigan, M. T., and Foldy, S. (2010). Web-based self-triage of influenza-like illness during the 2009 H1N1 influenza pandemic. Ann. Emerg. Med. 56, 288–294. doi:10.1016/j.annemergmed.2010.04.005
Kirmayer, L. J. (1992). The body’s insistence on meaning: metaphor as presentation and representation in illness experience. Med. Anthropol. Q. 6, 323–346. doi:10.1525/maq.1992.6.4.02a00020
LeBlanc, V. R., Brooks, L. R., and Norman, G. R. (2002). Believing is seeing: the influence of a diagnostic hypothesis on the interpretation of clinical features. Acad. Med. 77, s67–s69. doi:10.1097/00001888-200210001-00022
LeBlanc, V. R., Norman, G. R., and Brooks, L. R. (2001). Effect of a diagnostic suggestion on diagnostic accuracy and clinical feature identification. Acad. Med. 76, s18–s20. doi:10.1097/00001888-200110001-00007
MacKichan, F., Brangan, E., Wye, L., Checkland, K., Lasserson, D., Huntley, A., et al. (2017). Why do patients seek primary medical care in emergency departments? An ethnographic exploration of access to general practice. BMJ Open 7, e013816. doi:10.1136/bmjopen-2016-013816
Morahan-Martin, J. M. (2004). How Internet users find, evaluate, and use online health information: a cross-cultural review. Cyberpsychol. Behav. 7, 497–510. doi:10.1089/cpb.2004.7.497
Morita, T., Rahman, A., Hasegawa, T., Ozaki, A., and Tanimoto, T. (2017). The potential possibility of symptom checker. Int. J. Health Policy Manag. 6, 1–2. doi:10.15171/ijhpm.2017.41
Nijland, N., van Gemert-Pijnen, J., Boer, H., Steehouder, M. F., and Seydel, E. R. (2008). Evaluation of Internet-based technology for supporting self-care: problems encountered by patients and caregivers when using self-care applications. J. Med. Internet Res. 10, e13. doi:10.2196/jmir.957
Norman, G. R., Arfai, B., Gupta, A., Brooks, L. R., and Eva, K. W. (2003). The privileged status of prestigious terminology: impact of “medicalese” on clinical judgments. Acad. Med. 78, S82–S84. doi:10.1097/00001888-200310001-00026
Ogden, J., Branson, R., Bryett, A., Campbell, A., Febles, A., Ferguson, I., et al. (2003). What’s in a name? An experimental study of patients’ views of the impact and function of a diagnosis. Fam. Pract. 20, 248–253. doi:10.1093/fampra/cmg304
Pocheptsova, A., Labroo, A. A., and Dhar, R. (2010). Making products feel special: when metacognitive difficulty enhances evaluation. J. Market. Res. 47, 1059–1069. doi:10.1509/jmkr.47.6.1059
Redelmeier, D. A., Rozin, P., and Kahneman, D. (1993). Understanding patients’ decisions – cognitive and emotional perspectives. J. Am. Med. Assoc. 270, 72–76. doi:10.1001/jama.1993.03510010078034
Rosen, N. O., and Knäuper, B. (2009). A little uncertainty goes a long way: state and trait differences in uncertainty interact to increase information seeking but also increase worry. Health Commun. 24, 228–238. doi:10.1080/10410230902804125
Schwarz, N., Song, H., and Xu, J. (2009). “When thinking is difficult: metacognitive experiences as information,” in The Social Psychology of Consumer Behavior, ed. M. Wänke (New York: Psychology Press), 201–223.
Song, H., and Schwarz, N. (2009). If it’s difficult to pronounce, it must be risky: fluency, familiarity, and risk perception. Psychol. Sci. 20, 135–138. doi:10.1111/j.1467-9280.2009.02267.x
Stewart, M., Brown, J. B., Donner, A., McWhinney, I. R., Oates, J., Weston, W., et al. (2000). The impact of patient-centred care on outcomes. J. Fam. Pract. 49, 796–804.
Tasso, A., Gavaruzzi, T., and Lotto, L. (2014). What is in a name drug names convey implicit information about their riskiness and efficacy. Appl. Cogn. Psychol. 28, 539–544. doi:10.1002/acp.3033
Topolinski, S., and Strack, F. (2010). False fame prevented: avoiding fluency effects without judgmental correction. J. Pers. Soc. Psychol. 98, 721. doi:10.1037/a0019260
White, R. W., and Horvitz, E. (2009). “Cyberchondria: studies of the escalation of medical concerns in web searches,” in ACM Transactions on Information Systems. Redmond: Also Microsoft Research Technical Report MSR-TR-2008-178.
Williams, N., and Ogden, J. (2004). The impact of matching the patient’s vocabulary a randomized control trial. Fam. Pract. 21, 630–635. doi:10.1093/fampra/cmh610
Young, M. E., King, N., Harper, S., and Humphreys, K. R. (2013). The influence of popular media on perceptions of personal and population risk in possible disease outbreaks. Health Risk Soc. 15, 103–114. doi:10.1080/13698575.2012.748884
Young, M. E., Norman, G. R., and Humphreys, K. R. (2008). The role of medical language in changing public perceptions of illness. PLoS ONE 3:e3875. doi:10.1371/journal.pone.0003875
Zarin, D. A., and Earls, F. (1993). Diagnostic decision making in psychiatry. Am. J. Psychiatry 150, 197–206. doi:10.1176/ajp.150.2.197
Appendix
Sample Scenario (Recently Medicalized Disorder)
Language labels were not presented to the participant, but are included here for illustrative purposes. Language of label used to describe the disorder (either medical or lay) was counterbalanced across participants.
Lay Label Version
| You are experiencing itchy flaking skin on your scalp, eyebrows, around your hairline, ears, and nose. These symptoms are consistent with chronic dandruff. In this situation, when would you seek medical attention? | ||||||||
| □ | □ | □ | □ | □ | □ | □ | ||
| Never | As soon as possible | |||||||
| (At the next scheduled appointment, if at all) | (Within the hour) | |||||||
Medical Label Version
| You are experiencing itchy flaking skin on your scalp, eyebrows, around your hairline, ears, and nose. These symptoms are consistent with Seborrheic Dermatitis. In this situation, when would you seek medical attention? | ||||||||
| □ | □ | □ | □ | □ | □ | □ | ||
| Never | As soon as possible | |||||||
| (At the next scheduled appointment, if at all) | (Within the hour) | |||||||
Keywords: decision-making, medical terminology, self-triage, urgency, medicine
Citation: D’Angelo MC, Humphreys KR, Li T and Young ME (2017) The Impact of Medical Terminology in Self-Triage Decision-Making. Front. Commun. 2:6. doi: 10.3389/fcomm.2017.00006
Received: 17 March 2017; Accepted: 04 July 2017;
Published: 26 July 2017
Edited by:
Iccha Basnyat, National University of Singapore, SingaporeCopyright: © 2017 D’Angelo, Humphreys, Li and Young. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Meredith E. Young, meredith.young@mcgill.ca