Story of rubidium-82 and advantages for myocardial perfusion PET imaging
 Jean-François Chatal1*
Jean-François Chatal1*
 François Rouzet2
François Rouzet2
 Ferid Haddad1
Ferid Haddad1
 Cécile Bourdeau1
Cécile Bourdeau1
 Cédric Mathieu3
Dominique Le Guludec2
Cédric Mathieu3
Dominique Le Guludec2
- 1Groupement d’Intérêt Public Arronax, University of Nantes, Saint-Herblain, France
- 2UMR 1148, Department of Nuclear Medicine, Bichat Hospital, Assistance Publique Hôpitaux de Paris, DHU FIRE (Fibrosis, Inflammation, Remodeling in Cardiovascular, Respiratory and Renal Diseases), Paris-Diderot University, Paris, France
- 3Department of Nuclear Medicine, Nantes University Hospital, Nantes, France
Rubidium-82 has a long story, starting in 1954. After preclinical studies in dogs showing that myocardial uptake of this radionuclide was directly proportional to myocardial blood flow (MBF), clinical studies were performed in the 80s leading to an approval in the USA in 1989. From that time, thousands of patients have been tested and their results have been reported in three meta-analyses. Pooled patient-based sensitivity and specificity were, respectively, 0.91 and 0.90. By comparison with 99mTc-SPECT, 82Rb PET had a much better diagnostic accuracy, especially in obese patients with body mass index ≥30 kg/m2 (85 versus 67% with SPECT) and in women with large breasts. A great advantage of 82Rb PET is its capacity to accurately quantify MBF. Quite importantly, it has been recently shown that coronary flow reserve is associated with adverse cardiovascular events independently of luminal angiographic severity. Moreover, coronary flow reserve is a functional parameter particularly useful in the estimate of microvascular dysfunction, such as in diabetes mellitus. Due to the very short half-life of rubidium-82, the effective dose calculated for a rest/stress test is roughly equivalent to the annual natural exposure and even less when stress-only is performed with a low activity compatible with a good image quality with the last generation 3D PET scanners. There is still some debate on the relative advantages of 82Rb PET with regard to 99mTc-SPECT. For the last 10 years, great technological advances substantially improved performances of SPECT with its accuracy getting closer to this of 82Rb/PET. Currently, the main advantages of PET are its capacity to accurately quantify MBF and to deliver a low radiation exposure.
Introduction
The story of medical use of rubidium goes back in 1954 when Love et al. showed that the biological behavior of rubidium was comparable to the one of potassium and that its myocardial muscle uptake was proportional to blood flow in coronary arteries (1). Following this paper, several preclinical studies have been performed mainly in dogs and using different radionuclides of rubidium until the early 80s when the first injection in humans took place (2). During the 80s, a few clinical studies, including hundreds of patients, demonstrated the good diagnostic accuracy of 82Rb/PET, which was higher than the one obtained with 99mTc/SPECT (3, 4). Subsequently, a generator 82Sr/82Rb (CardioGen-82®) was approved in 1989 and delivered in the USA by Bracco Diagnostics, Inc., for clinical use.
At that time, the number of PET cameras, their technological performances, and the production capacities of strontium-82 were limited, explaining a slow progression of this technology in the USA. However, despite this limitation, thousands of patients were tested with PET using rubidium-82 allowing three meta-analyses to be performed.
During the last 10 years, with the increased number of PET/CT systems and the higher strontium-82 production capabilities, the number of patients injected with rubidium-82 in the USA dramatically grew even if it still represents a small percentage by comparison with the use of 99mTc-sestamibi and 99mTc-tetrofosmin. Moreover, for the last 10 years, great technological advances have been introduced, including semiconductor detector SPECT scanners, novel collimator design, and novel iterative reconstruction methods allowing to substantially improve count sensitivity and image resolution. Consequently, the diagnostic accuracy of 99mTc/SPECT got closer to this of 82Rb/PET, opening a large debate on the advantages of one technique with regard to the other.
The latest clinical developments zeroed in on the high prognostic value of quantification using PET and allowing to accurately measure myocardial blood flow (MBF) and coronary reserve. Even if there are no real technical limitations to such measurements with SPECT it will take some years before their potential clinical validation (5). Finally, the level of radiation dose is an important parameter to be taken into consideration due to the high number of patients to be tested and the repetition of imaging in the same patients. The aforementioned technological advances allowed to significantly reduce radiation doses with both 99mTc/SPECT and 82Rb/PET even if the latter delivers the smallest dose (6).
Preclinical Studies
Beta- and gamma-emitting rubidium-86 was first used because its long 18.7 days half-life enabled to perform long-lasting kinetic studies. In 1959, Love et al. showed, in 19 dogs, that myocardial uptake of this radionuclide was directly proportional to MBF (7). These results were confirmed 2 years later in 26 dogs by Levy et al. (8).
More than a decade later, Nishiyama et al. compared optimal settings of scintillation camera with 201Tl (T1/2:73.1 h, γ: 167 keV), 43K (T1/2: 22.2h, γ: 373 keV), 129Cs (T1/2: 32.06h, γ:372 keV), and 81Rb, a positron-emitting radioisotope with a half-life of 4.6 h (9). Thallium-201 was considered as the best suited with the available equipment at that time and cesium-129 was next best. High-energy photons from 81Rb largely made it impossible to obtain an interpretable image without the addition of more shielding.
In 1979, Yano et al. compared several ion-exchange columns to be used in an automated 82Sr/82Rb generator for testing in man (10).
Finally, in 1982, Selwyn et al. examined the relation between myocardial perfusion and rubidium-82 uptake during acute ischemia in six dogs after coronary stenosis and in five volunteers and five patients with coronary artery disease. Myocardial tomograms, recorded at rest and after exercise in the volunteers showed homogeneous uptake in reproducible and repeatable scans. An absolute mean decrease of 36 ± 14% in regional myocardial uptake was found after exercise in the patients with coronary artery disease (2).
Clinical Studies
Meta-Analyses of PET Studies
Since the approval by FDA in the USA in 1989, a vast amount of clinical studies have been performed, including thousands of patients. Results have been analyzed in three meta-analyses published in 2008 and 2012 (Table 1). Pooled patient-based sensitivity and specificity were, respectively, 0.91 and 0.90. These excellent results should be tempered by some limitations and biases inherent to meta-analyses. There was heterogeneity between studies in scanning protocols and prevalence stenosis with invasive coronarography. Moreover, baseline characteristics, such as gender or disease prevalence, were different between patient populations resulting in a cautious interpretation.
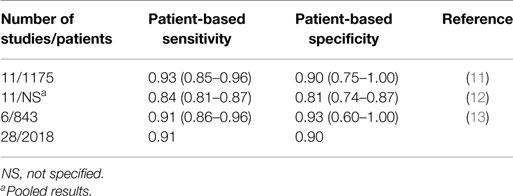
Table 1. Results of meta-analyses with 82Rb PET.
For a long time, PET studies have been performed with two-dimensional cameras needing to inject a relatively high activity of rubidium-82 (40 mCi for stress-only) and resulting in non-negligible radiation exposure. The accuracy, outcomes, and cost-effectiveness of 3D PET technology using a low activity of 20 mCi were recently evaluated in seven centers (14). Through an effective standardization and quality assurance program, the image interpretation was highly repeatable in involved centers.
Meta-Analyses of SPECT Studies
A much larger number of 227 studies using 99mTc/SPECT and including more than 14,500 patients have been considered in 7 meta-analyses published between 1998 and 2012 (Table 2). Pooled patient-based sensitivity and specificity were, respectively, 0.88 and 0.67. The same limitations as with PET studies were applied to SPECT studies.
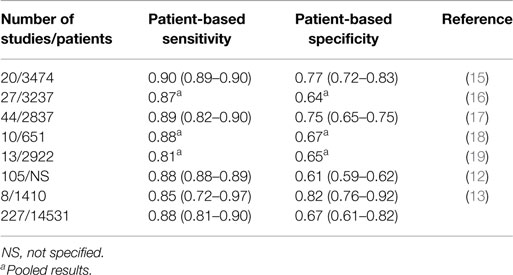
Table 2. Results of meta-analyses with 99mTc SPECT.
Comparison between PET and SPECT
Myocardial perfusion imaging is a real challenge in overweight or obese patients and in women with large breasts due to attenuation artifacts, resulting in decreased specificity using 99mTc SPECT. PET imaging has improved specificity owing to better spatial resolution, coincidence detection, and accurate attenuation correction.
Bateman et al. compared 99mTc SPECT in 112 patients with 82Rb PET in 112 patients (20). They showed a much better diagnostic accuracy using PET, in obese patients with body mass index (BMI) ≥30 kg/m2 (85 versus 67% with SPECT). However, it should be noted that SPECT was performed at that time without attenuation correction. With the introduction of iterative reconstruction, SPECT is now performed with attenuation correction, which may correct some artifacts and improve diagnostic accuracy in the obese population but with a decrease of sensitivity. A recent study reported on the value of 82Rb PET in 2687 obese patients with BMI ≥30 kg/m2 by comparison with 2047 overweight patients (BMI: 25.0–30.0 kg/m2) and 1303 normal patients (BMI: <25.0 kg/m2). Interestingly, the results showed the same prognostic value irrespective of BMI (21).
In the future, 82Rb PET should be compared to contemporary 99mTc SPECT using the last technological advances in the same overweight or obese patients to confirm or not the higher prognostic value of PET to SPECT.
As aforementioned, a large number of clinical studies have been performed using PET and SPECT in different populations of patients allowing to group the results in meta-analyses with the possibility of biases in interpretation of these results.
The most informative comparison between PET and SPECT should be in the same population of patients injected with both radiopharmaceuticals. Such comparisons have been made a long time ago at the time of approval of rubidium-82 in the USA in three studies, including a total of 433 patients (22–24). In fact, these studies used thallium-201 for SPECT, which has been replaced by technetium-99m. Quite recently, a comparison of both modalities has been performed in a small cohort of 27 patients using the most recent hybrid imaging technology, which included CT-based attenuation correction for SPECT and PET (25). 82Rb/PET imaging was performed as a second-line test when previous gated rest/stress 99mTc/SPECT with or without attenuation correction was non-conclusive. In this clinical situation, there were much fewer non-conclusive results with PET than with SPECT. Image quality and interpretive confidence were higher with PET than with SPECT even when SPECT was performed with attenuation correction.
Dosimetric Studies
Radiation dosimetry of rubidium-82 has been recently estimated in 10 healthy volunteers using the OLINDA/EXM 1.0 dosimetry software (26). Using different methodological approach, the estimates were discrepant with the results previously reported. The highest absorbed dose was delivered to the kidneys but remaining at a quite acceptable level of 1.3 cGy for 2220 MBq (60 mCi) of injected activity. The effective dose calculated for a rest/stress test with an injected activity of 2 MBq × 1480 MBq (2 mCi × 40 mCi) was 3.7 mSv that is roughly equivalent to the annual natural exposure.
In 2015, Dorbala et al. reported on the way to reduce radiation dose with myocardial SPECT and PET imaging (6). Considering the use of last generation of 3D PET scanners and software allowing to inject half activity of rubidium-82 (2 MBq × 740 MBq or 2 mCi × 20 mCi) for a preserved image quality, the calculated effective dose was 1.26 mSv for rest or stress. In the clinical situation of stress-only 3D PET with MBF estimate, the radiation dose would be at an acceptable level of around 1 mSv. This is half of the radiation dose with 99mTc-sestamibi or tetrofosmin using last generation of scanners.
Quantification Studies
The clinical use of quantitative MBF assessment with 82Rb/PET started at the end of the previous decade in the USA. In 2009, El Fakhri et al. demonstrated, in 22 subjects including patients with known coronary artery disease or healthy volunteers, that the measurement of absolute quantitation of MBF was feasible, reproducible, and accurate (27). Two years later, Ziadi et al. prospectively evaluated the prognostic value of coronary flow reserve using 82Rb/PET in 704 patients and compared the results with semi-quantitative assessment using summed stress scores (28). They showed that quantitative myocardial flow reserve (MFR) was a good predictor of adverse cardiac events independent of the summed stress scores. The same added prognostic value of blood flow quantitation was confirmed 2 years later by Farhad et al. in 351 patients (29).
Several software packages are available for quantification of MBF. A study (RUBY-10) compared them in 48 patients from 10 centers and showed that, using the most common kinetic model, they may be used interchangeably (30).
The value of quantification of absolute MBF using rubidium-82 has been studied in 140 patients after heart transplant and for whom the prognosis depends on allograft vasculopathy (31). It was clearly shown that mean MFR was a significant predictor of future adverse events.
The great interest of blood flow quantification has been documented in diabetes mellitus (32). Among diabetic patients without coronary artery disease, those with impaired coronary reserve had cardiac event rates comparable to those with prior coronary artery disease, whereas those with preserved coronary reserve had cardiac event rates comparable to those of non-diabetics. Moreover, it has been recently shown that “global coronary flow reserve is associated with adverse cardiovascular events independently of luminal angiographic severity and modifies the effect of early revascularization” (33). The angiographic severity was evaluated using the coronary artery disease prognostic index. This important result documents the complementary but distinct association of functional and anatomic coronary abnormalities. A significant interaction was shown between coronary flow reserve and revascularization strategy, which could have large implications in the future for therapeutic strategy.
One other cardiac PET perfusion tracer, 13N-ammonia, has been approved in the USA and is being clinically used at a relatively modest level. Its positron range is favorable resulting in a good image resolution and the myocardial extraction fraction is also favorable but its short physical half-life of 9.96 min requires an onsite cyclotron, which is a great limitation for a routine clinical use. Another PET radiotracer, 18F-flurpiridaz is currently undergoing a clinical phase III evaluation and is quite promising after its potential approval. It could then be a real competitor to 82Rb. A recent excellent review described in depth the characteristics of all PET perfusion radiotracers (34).
Advantages
Daily Availability of Rubidium-82 in Nuclear Cardiology Departments
Like with all generators, rubidium-82 is daily available in a department of nuclear medicine after elution of the column loaded with strontium-82 (Table 3). Such elution can be repeated every 10 min making possible to inject up to 10–15 patients per day depending on the availability of a dedicated cardiac PET/CT and of patient recruitment rate. A 82Sr/82Rb generator can currently be used for 28–42 days according to the loaded strontium-82 activity. It can be expected that this use will be extended to 60 days in a near future allowing to increase the number of tested patients with the same generator and consequently to decrease the cost of rubidium-82 examination for each patient.
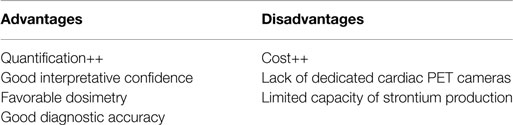
Table 3. Advantages and disadvantages of the use of 82Rb PET myocardial imaging.
Easy Interpretation of Images due to High Count Density
The count density and the uniformity of distribution of rubidium-82 in the myocardium are higher with PET than with SPECT using technetium-99m, even using the last technological advances of both techniques (25). Consequently, the interpretative confidence and interreader agreement are higher with PET leading to a higher accuracy. PET cameras do not need the use of collimators, resulting in higher sensitivity and spatial resolution (35).
Measurement of Myocardial Blood Flow and Coronary Reserve
Interpretation of SPECT and PET images is visual or semi-quantitative and based on relative uptake. Myocardial areas with the highest uptake are supposed to be supplied by non-obstructive coronary arteries while those with decreased uptake during stress are considered as being supplied by obstructive arteries. A stenosis with a luminal diameter around 50% may be undetected by this visual interpretation. Moreover, patients with subclinical coronary ischemia or microvascular diffuse disease may present only a mild heterogeneous or even homogeneous myocardial uptake. Finally, in the situation of three-vessel coronary disease, a reduction of myocardial uptake may be balanced in all coronary arteries, resulting in a homogeneous left ventricle myocardium at stress (Figure 1).

Figure 1. A 56-year-old woman with a history of obesity (BMI: 31.2 cm/kg2), hypertension, hyperlipemia, and type 2 diabetes complicated of retinopathy and renal failure. The patient was referred to the Nuclear Medicine department for detection of coronary artery disease and underwent both Tc-99m-sestamibi SPECT (D-SPECT, Spectrum Dynamics, Haifa) and rubidium-82 PET/CT (Discovery 690 VCT, GEMS, Buc, France) as part of a clinical trial. SPECT (93% of the predicted maximal heart rate, no symptoms, EKG positive) was normal with a homogeneous uptake of the tracer both at stress and at rest (A). 82Rb PET performed after Dipyridamole infusion showed a mild decrease of the tracer uptake in the lateral wall (arrow), completely reversible at rest, raising the suspicion of ischemia in the territory of the circumflex artery (B). This hypothesis was then confirmed by quantitative data derived from myocardial blood flow measurement with a coronary steal phenomenon in the same territory [coronary flow reserve (CFR) <1; (C)]. In addition, the CFR was markedly decreased (<1.5) in the territory of both the left descending artery and the right coronary artery, suggesting the presence of significant stenosis of these two coronary arteries. The coronary angiography confirmed the diagnosis of three-vessel disease and the patient underwent surgical revascularization. This case report underlines the greatest sensitivity of 82Rb PET over SPECT in the setting of balanced ischemia, in relation with the ability to perform absolute quantification of myocardial blood flow.
The measurements of absolute MBF in milliliter per gram per minute and MFR, which is the maximum increase in blood flow above the normal resting volume, allows to complete the field of application of conventional perfusion imaging by identifying subclinical coronary ischemia and characterizing extent and severity in multi-vessel disease. Moreover, it has been clearly shown during the last years that the measurement of hyperemic MBF and MFR using PET/CT may predict, better than other parameters, the occurrence of hard cardiac events.
Today, there is no doubt that absolute myocardial perfusion quantification has been fully validated using PET/CT with 82Rb or 13N. There is a great debate about the same possibility using 99mTc/SPECT. In a quite recent editorial, Garcia considered the current situation taking into account the most recent technological advances in instrumentation and quantification software (5). New heart-centered SPECT systems have a high count sensitivity and iterative reconstruction enables an efficient correction of attenuation, scatter, and resolution changes with depth. In 2013, Ben-Haim et al. (36) showed the feasibility of measuring MBF and MFR with SPECT. Today, it can be stated that there is no real limitation to the quantification of MBF and MBF reserve with SPECT. The first results on clinical efficacy using conventional SPECT/CT systems have been reported (37) but these preliminary results should be confirmed in large studies and it will take some years before full validation for clinical use. Today, there is no doubt that only PET technology allows to measure rapidly and accurately the MBF.
Low Radiation Exposure for Patients
Given the high and still increasing number of patients who have myocardial perfusion imaging all over the world each year, the radiation exposure for patients and medical staff is a real concern and should be reduced at the lowest level compatible with a good image quality.
Effective radiation dose is directly related to the physical half-life of the radiopharmaceutical, its biodistribution and injected activity. In this respect, the very short half-life of 82Rb of 1.26 min in comparison of 6 h of 99mTc is quite favorable for a low radiation dose, especially if new technologies enable to substantially decrease injected activity. For a long time, using 2D imaging mode, injected activity of rubidium-82 for rest and stress was 1480 MBq (40 mCi), resulting in an estimated dose of 2.5 and 5 mSv, respectively (6). Shifting from 2D to 3D imaging mode allowed to inject half activity (740 MBq or 20 mCi) for the same image quality and then to reduce the dose to 1.3 mSv for stress or rest and even to <1 mSv using new estimates of rubidium-82 dose (26). Such a dose is acceptable when compared to an average natural annual radiation dose of about 3 mSv. Stress-only PET 3D imaging, allowing to measure hyperemic MBF with <1 mSv, would be the preferred strategy for risk stratification if this measurement is clinically validated with regard to the measurement of myocardial blood reserve, which needs both stress and rest tests.
By comparison, effective radiation doses are higher with 99mTc-based radiopharmaceuticals partially owing to the longer half-life of this radionuclide with regard to rubidium-82. Using the most recent advances in cardiac SPECT technology allowing to inject half activity for the same image quality [148–444 MBq (4–12 mCi)], the estimated doses are 2.3 and 8 mSv for rest/stress with 99mTc sestamibi and 2.0 and 6.1 mSv with 99mTc-tetrofosmin (6). Stress-only SPECT 3D imaging would deliver twice higher effective dose than with stress-only PET 3D imaging even if such dose remains moderate.
A recent study reported on projected population cancer risks in the USA using myocardial perfusion scintigraphy (38). The authors considered estimated effective doses ranging from 9 mSv for stress-only technetium-99m to 35 mSv for a rest/stress dual-isotope study associating thallium-201 and technetium-99m and using conventional SPECT equipment. For rubidium-82 PET imaging, they considered an estimated effective dose of 15 mSv for a rest/stress test using an injected activity of 1480–2250 MBq and a 2D PET camera. Cancer risk projection models were based on the National Research Council Biological Effects of Ionizing Radiation VII report assuming a linear relationship with radiation exposure. In these conditions and considering the 9.1 million tests performed each year in the USA, the number of additional future cancers would be about 7400. This number should be viewed with great caution because, from the time of Berrington’s publication, estimated effective doses have been substantially decreased with the use of most advanced instrumentation allowing to dramatically decrease injected activities.
Considering the lower injected activity, which is now possible with 3D SPECT and PET cameras, which results in low effective doses, the number of additional and supposed cancers should be significantly lowered. Finally, the risk/benefit ratio should be taken into consideration for each individual patient before performing a myocardial perfusion test and the lowest activity should be injected compatible with a good image quality leading to an accurate diagnosis.
Limitations
Cost
Currently, the cost for one test with rubidium-82 is higher than with a 99mTc-labeled radiopharmaceutical even in the favorable situation of a nuclear cardiology center with a high recruitment rate (Table 3). In the USA, sestamibi-99mTc is currently reimbursed at about $70 per dose, usually using 2 doses. However, in the hospital setting, the entire procedure including the drug is paid at $1139. Rubidium-82 is reimbursed at approximately $250 per dose. In the hospital setting, the entire procedure is reimbursed $1286.
This relative low cost of technetium-99m is partly due to the fact that Mo-99/Tc-99m is not paid at full cost which explains some of the problems encountered nowadays with aging reactors and the difficulties to build new ones. Consequently, the use of rubidium-82 should be, at least at short term, limited to patients who are unable to complete exercise stress test, who are obese or who had a previous equivocal and non-conclusive SPECT test. Moreover, rubidium-82 should be used, despite its cost, when MBF and coronary flow reserve quantitation are required, for example, in patients with multi-vessel coronary disease.
Some new high-energy cyclotrons will be installed shortly and will enable to extend strontium-82 availability, and then provide generators in a cost effective model.
Limited Number and Availability of PET 3D Systems
To be as cost-effective as possible with a 82Sr/82Rb generator, it is necessary to test a high number of patients before its expiration date (presently 28–42 days) but this situation needs to have available a dedicated cardiac PET/CT camera. In Europe, where a 82Sr/82Rb generator has not been approved yet, there is no such dedicated PET/CT cameras and the conventional PET/CT cameras are mainly used in oncology with fluorodeoxyglucose (FDG). A minimum of 8–10 patients are tested each day with this radiopharmaceutical and up to a maximum of 15–20 patients. Consequently, a quite limited number of patients could be injected with rubidium-82 per day making each test relatively expensive. This situation reinforces the fact that, at the beginning, Rb-82 will be probably limited to selective cases (see Cost). It will take probably a few years before some dedicated cardiac PET/CT cameras are available in large cardiology centers with a recruitment rate warranting such equipment.
Perspectives
Strontium-82, which is the parent nucleus of rubidium-82, is produced using proton beam interacting on a target containing stable rubidium. To be economically viable, an accelerator with proton beam of energy higher than 70 MeV and intensity >100 μA must be used. There are only few places in the world where such accelerators are available: Brookaven National Laboratory (BNL-USA), Los Alamos National Laboratory (LANL-USA), iThemba labs (South Africa), INR (Russia), Triumf (Canada), and Arronax (France). These accelerators are not dedicated facilities and only part of the beam time is devoted to this production. Recently, based on the success of the first prototype of a 70 MeV machine built by a commercial cyclotron provider and installed in Nantes (France), several private companies are considering the use of such commercial cyclotron for strontium-82 production. Zevacor (USA) is one of them and CDNM (Russia) is the other one. In parallel, a 70 MeV cyclotron is being installed at Legnaro (Italy) for research purpose but one of the two available beam lines may be used for radionuclide production. This indicates that the availability of strontium-82 in the future will be higher allowing to secure the supply chain and enlarge the use of this radionuclide to other countries (at the moment only north America is using it routinely), especially in Europe.
From a technological point of view, another advance will enlarge strontium-82 production, which is the use of rubidium metal target instead of the rubidium chloride target. With such change, higher yields can be obtained at the price of a more technical radiochemical process.
Finally, several designs of strontium-82/rubidium-82 generators are being studied and may reach the market in the future. This will allow to get generators with extended lifetime (up to 60 days) or lower activity which will better fit the need of users.
Conclusion
There is no doubt that the advantages of 82Rb/PET myocardial imaging have been clearly documented since its routine clinical use after approval in the USA nearly 30 years ago. For a long time, its accuracy was significantly better than that obtained with the SPECT/99mTc technology particularly in obese or overweight patients and women with large breasts due to attenuation correction artifacts. With the most recent hybrid SPECT imaging technology, the situation changed, leading to an improved specificity of 99mTc/SPECT. Currently, the main advantage of 82Rb/PET is its capacity to accurately measure the MBF and flow reserve. Even if such measurement is technologically feasible with 99mTc/SPECT, it will take some years before potential validation. Finally, given the very short physical half-life of rubidium-82, the radiation exposure rate with this radionuclide is significantly lower than with technetium-99m. Using 3D hybrid PET system, it is possible to inject low activities of rubidium-82 while maintaining a good image quality. The radiation exposure rate is then acceptable and inferior to natural exposure.
It can be anticipated that in the future 82Rb/PET and 99mTc/SPECT will continue to be used according availability of hybrid cameras and radionuclides.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This work has been supported in part by grants from the French National Agency for Research called “Investissements d’Avenir” Equipex ArronaxPlus no. ANR-11-EQPX-0004.
References
1. Love WD, Romney RB, Burch GE. A comparison of the distribution of potassium and exchangeable rubidium in the organs of the dog, using rubidium. Circ Res (1954) 2:112–22. doi: 10.1161/01.RES.2.2.112
2. Selwyn AP, Allan RM, L’Abbate A, Horlock P, Camici P, Clark J, et al. Relation between regional myocardial uptake of rubidium-82 and perfusion: absolute reduction of cation uptake in ischemia. Am J Cardiol (1982) 50:112–21. doi:10.1016/0002-9149(82)90016-9
3. Gould KL, Goldstein RA, Mullani NA, Kirkeeide RL, Wong WH, Tewson TJ, et al. Noninvasive assessment of coronary stenoses by myocardial perfusion imaging during pharmacologic coronary vasodilation. VIII. Clinical feasibility of positron cardiac imaging without a cyclotron using generator-produced rubidium-82. J Am Coll Cardiol (1986) 7:775–89. doi:10.1016/S0735-1097(86)80336-9
4. ACNP/SNM Task Force on Clinical PET. Positron emission tomography: clinical status in the United States in 1987. J Nucl Med (1988) 29:1136–43.
5. Garcia EV. Are SPECT measurements of myocardial blood flow and flow reserve ready for clinical use? Eur J Nucl Med Mol Imaging (2014) 41:2291–3. doi:10.1007/s00259-014-2924-2
6. Dorbala S, Blankstein R, Skali H, Park M-A, Fantony J, Mauceri C, et al. Approaches to reducing radiation dose from radionuclide myocardial perfusion imaging. J Nucl Med (2015) 56:592–9. doi:10.2967/jnumed.112.115097
7. Love WD, Burch GE. Influence of the rate of coronary plasma flow on the extraction of Rb86 from coronary blood. Circ Res (1959) 7:24–30. doi:10.1161/01.RES.7.1.24
8. Levy MN, Martins De Oliveira J. Regional distribution of myocardial blood flow in the dog as determined by Rb86. Circ Res (1961) 9:96–8. doi:10.1161/01.RES.9.1.96
9. Nishiyama H, Sodd VJ, Adolph RJ, Saenger EL, Lewis JT, Gabel M. Intercomparison of myocardial imaging agents: 201Ti, 129Cs, 43K, and 81Rb. J Nucl Med (1976) 17:880–9.
10. Yano Y, Budinger TF, Chiang G, O’Brien HA, Grant PM. Evaluation and application of alumina-based Rb-82 generators charged with high levels of Sr-82/85. J Nucl Med (1979) 20:961–6.
11. Nandalur KR, Dwamena BA, Choudhri AF, Nandalur SR, Reddy P, Carlos RC. Diagnostic performance of positron emission tomography in the detection of coronary artery disease: a meta-analysis. Acad Radiol (2008) 15:444–51. doi:10.1016/j.acra.2007.08.012
12. Jaarsma C, Leiner T, Bekkers SC, Crijns HJ, Wildberger JE, Nagel E, et al. Diagnostic performance of noninvasive myocardial perfusion imaging using single-photon emission computed tomography, cardiac magnetic resonance, and positron emission tomography imaging for the detection of obstructive coronary artery disease: a meta-analysis. J Am Coll Cardiol (2012) 59:1719–28. doi:10.1016/j.jacc.2011.12.040
13. Mc Ardle BA, Dowsley TF, deKemp RA, Wells GA, Beanlands RS. Does rubidium-82 PET have superior accuracy to SPECT perfusion imaging for the diagnosis of obstructive coronary disease?: a systematic review and meta-analysis. J Am Coll Cardiol (2012) 60:1828–37. doi:10.1016/j.jacc.2012.07.038
14. Renaud JM, Mylonas I, McArdle B, Dowsley T, Yip K, Turcotte E, et al. Clinical interpretation standards and quality assurance for the multicenter PET/CT trial rubidium-ARMI. J Nucl Med (2014) 55:58–64. doi:10.2967/jnumed.112.117515
15. O’Keefe JH, Barnhart CS, Bateman TM. Comparison of stress echocardiography and stress myocardial perfusion scintigraphy for diagnosing coronary artery disease and assessing its severity. Am J Cardiol (1995) 75:25D–34D. doi:10.1016/S0002-9149(99)80399-3
16. Fleischmann KE, Hunink MG, Kuntz KM, Douglas PS. Exercise echocardiography or exercise SPECT imaging? A meta-analysis of diagnostic test performance. JAMA (1998) 280:913–20. doi:10.1001/jama.280.10.913
17. Kim C, Kwok YS, Heagerty P, Redberg R. Pharmacologic stress testing for coronary disease diagnosis: a meta-analysis. Am Heart J (2001) 142:934–44. doi:10.1067/mhj.2001.119761
18. Imran MB, Pálinkás A, Picano E. Head-to-head comparison of dipyridamole echocardiography and stress perfusion scintigraphy for the detection of coronary artery disease: a meta-analysis. Comparison between stress echo and scintigraphy. Int J Cardiovasc Imaging (2003) 19:23–8. doi:10.1023/A:1021746515555
19. Mowatt G, Vale L, Brazzelli M, Hernandez R, Murray A, Scott N, et al. Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of myocardial perfusion scintigraphy for the diagnosis and management of angina and myocardial infarction. Health Technol Assess (2004) 8:iii–iv, 1–207. doi:10.3310/hta8300
20. Bateman TM, Heller GV, McGhie AI, Friedman JD, Case JA, Bryngelson JR, et al. Diagnostic accuracy of rest/stress ECG-gated Rb-82 myocardial perfusion PET: comparison with ECG-gated Tc-99m sestamibi SPECT. J Nucl Cardiol (2006) 13:24–33. doi:10.1016/j.nuclcard.2005.12.004
21. Chow BJW, Dorbala S, Di Carli MF, Merhige ME, Williams BA, Veledar E, et al. Prognostic value of PET myocardial perfusion imaging in obese patients. JACC Cardiovasc Imaging (2014) 7:278–87. doi:10.1016/j.jcmg.2013.12.008
22. Stewart RE, Schwaiger M, Molina E, Popma J, Gacioch GM, Kalus M, et al. Comparison of rubidium-82 positron emission tomography and thallium-201 SPECT imaging for detection of coronary artery disease. Am J Cardiol (1991) 67:1303–10. doi:10.1016/0002-9149(91)90456-U
23. Go RT, Marwick TH, MacIntyre WJ, Saha GB, Neumann DR, Underwood DA, et al. A prospective comparison of rubidium-82 PET and thallium-201 SPECT myocardial perfusion imaging utilizing a single dipyridamole stress in the diagnosis of coronary artery disease. J Nucl Med (1990) 31:1899–905.
24. Marwick TH, Go RT, MacIntyre WJ, Saha GB, Underwood DA. Myocardial perfusion imaging with positron emission tomography and single photon emission computed tomography: frequency and causes of disparate results. Eur Heart J (1991) 12:1064–9.
25. Flotats A, Bravo PE, Fukushima K, Chaudhry MA, Merrill J, Bengel FM. 82Rb PET myocardial perfusion imaging is superior to 99mTc-labelled agent SPECT in patients with known or suspected coronary artery disease. Eur J Nucl Med Mol Imaging (2012) 39:1233–9. doi:10.1007/s00259-012-2140-x
26. Senthamizhchelvan S, Bravo PE, Esaias C, Lodge MA, Merrill J, Hobbs RF, et al. Human biodistribution and radiation dosimetry of 82Rb. J Nucl Med (2010) 51:1592–9. doi:10.2967/jnumed.110.077669
27. El Fakhri G, Kardan A, Sitek A, Dorbala S, Abi-Hatem N, Lahoud Y, et al. Reproducibility and accuracy of quantitative myocardial blood flow assessment with (82)Rb PET: comparison with (13)N-ammonia PET. J Nucl Med (2009) 50:1062–71. doi:10.2967/jnumed.104.007831
28. Ziadi MC, Dekemp RA, Williams KA, Guo A, Chow BJW, Renaud JM, et al. Impaired myocardial flow reserve on rubidium-82 positron emission tomography imaging predicts adverse outcomes in patients assessed for myocardial ischemia. J Am Coll Cardiol (2011) 58:740–8. doi:10.1016/j.jacc.2011.01.065
29. Farhad H, Dunet V, Bachelard K, Allenbach G, Kaufmann PA, Prior JO. Added prognostic value of myocardial blood flow quantitation in rubidium-82 positron emission tomography imaging. Eur Heart J Cardiovasc Imaging (2013) 14:1203–10. doi:10.1093/ehjci/jet068
30. Nesterov SV, Deshayes E, Sciagrà R, Settimo L, Declerck JM, Pan X-B, et al. Quantification of myocardial blood flow in absolute terms using (82)Rb PET imaging: the RUBY-10 Study. JACC Cardiovasc Imaging (2014) 7:1119–27. doi:10.1016/j.jcmg.2014.08.003
31. Mc Ardle BA, Davies RA, Chen L, Small GR, Ruddy TD, Dwivedi G, et al. Prognostic value of rubidium-82 positron emission tomography in patients after heart transplant. Circ Cardiovasc Imaging (2014) 7:930–7. doi:10.1161/CIRCIMAGING.114.002184
32. Murthy VL, Naya M, Foster CR, Gaber M, Hainer J, Klein J, et al. Association between coronary vascular dysfunction and cardiac mortality in patients with and without diabetes mellitus. Circulation (2012) 126:1858–68. doi:10.1161/CIRCULATIONAHA.112.120402
33. Taqueti VR, Hachamovitch R, Murthy VL, Naya M, Foster CR, Hainer J, et al. Global coronary flow reserve is associated with adverse cardiovascular events independently of luminal angiographic severity and modifies the effect of early revascularization. Circulation (2015) 131:19–27. doi:10.1161/CIRCULATIONAHA.114.011939
34. Maddahi J, Packard RRS. Cardiac PET perfusion tracers: current status and future directions. Semin Nucl Med (2014) 44:333–43. doi:10.1053/j.semnuclmed.2014.06.011
35. Valenta I, Schindler TH. 82Rb PET/CT: entering a new area of myocardial perfusion imaging? Eur J Nucl Med Mol Imaging (2012) 39:1231–2. doi:10.1007/s00259-012-2154-4
36. Ben-Haim S, Murthy VL, Breault C, Allie R, Sitek A, Roth N, et al. Quantification of myocardial perfusion reserve using dynamic SPECT imaging in humans: a feasibility study. J Nucl Med (2013) 54:873–9. doi:10.2967/jnumed.112.109652
37. Hsu B, Chen F-C, Wu T-C, Huang W-S, Hou P-N, Chen C-C, et al. Quantitation of myocardial blood flow and myocardial flow reserve with 99mTc-sestamibi dynamic SPECT/CT to enhance detection of coronary artery disease. Eur J Nucl Med Mol Imaging (2014) 41:2294–306. doi:10.1007/s00259-014-2881-9
Keywords: rubidium-82, myocardial perfusion, PET imaging
Citation: Chatal J-F, Rouzet F, Haddad F, Bourdeau C, Mathieu C and Le Guludec D (2015) Story of rubidium-82 and advantages for myocardial perfusion PET imaging. Front. Med. 2:65. doi: 10.3389/fmed.2015.00065
Received: 16 June 2015; Accepted: 26 August 2015;
Published: 11 September 2015
Edited by:
Denis Guilloteau, Université de Tours and CHRU Tours, FranceReviewed by:
Flavia Groppi, Università degli Studi di Milano, ItalyUlli Köster, Institut Laue-Langevin, France
Copyright: © 2015 Chatal, Rouzet, Haddad, Bourdeau, Mathieu and Le Guludec. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jean-François Chatal, GIP Arronax, 1, rue Aronnax, BP 10112, 44817 Saint-Herblain Cedex, France, chatal@arronax-nantes.fr