Patient-Reported Outcomes in Patients with Chronic Kidney Disease and Kidney Transplant—Part 1
 Evan Tang
Evan Tang Aarushi Bansal1,2†
Aarushi Bansal1,2†
 Marta Novak
Marta Novak Istvan Mucsi
Istvan Mucsi- 1Multi-Organ Transplant Program, Division of Nephrology, University Health Network, Toronto, ON, Canada
- 2Institute of Medical Sciences, University of Toronto, Toronto, ON, Canada
- 3Centre for Mental Health, University Health Network, Toronto, ON, Canada
- 4Department of Psychiatry, University of Toronto, Toronto, ON, Canada
Chronic kidney disease (CKD) is a complex medical condition that is associated with several comorbidities and requires comprehensive medical management. Given the chronic nature of the condition, its frequent association with psychosocial distress, and its very significant symptom burden, the subjective patient experience is key toward understanding the true impact of CKD on the patients’ life. Patient-reported outcome measures are important tools that can be used to support patient-centered care and patient engagement during the complex management of patients with CKD. The routine collection and use of patient-reported outcomes (PROs) in clinical practice may improve quality of care and outcomes, and may provide useful data to understand the disease from both an individual and a population perspective. Many tools used to measure PROs focus on assessing health-related quality of life, which is significantly impaired among patients with CKD. Health-related quality of life, in addition to being an important outcome itself, is associated with clinical outcomes such as health care use and mortality. In Part 1 of this review, we provide an overview of PROs and implications of their use in the context of CKD. In Part 2, we will review the selection of appropriate measures and the relevant domains of interest for patients with CKD.
Introduction
In developed countries, there has been a rapid increase in the prevalence of chronic non-communicable diseases, which are responsible for the majority of morbidity and premature deaths in these societies (1, 2). These health conditions require complex long-term professional care and self-management (1, 2). Within the context of the health care system, management of chronic health conditions has been shifting away from the traditional provider-directed care model to a patient-centered care model (3–5). Patient-centered care utilizes the perspective of patients and allows them to play a key role in defining and managing their care (3–5). It promises a more holistic approach, improved patient experience, as well as improved medical outcomes compared with traditional care models (3, 5–12). Incorporating the patient perspective into clinical practice could improve the accuracy and completeness of assessment, provides accountability, and may play a role in outcome prognostication (13–15).
Chronic kidney disease (CKD) represents a major public health problem. Its prevalence has been rapidly increasing, in part, due to the rising prevalence of obesity, diabetes and hypertension (16–21). CKD is associated with substantial disease burden as both the disease and its various treatments—dietary and lifestyle modifications, renal replacement therapies (dialysis and kidney transplant)—are very intrusive. Accordingly, CKD is associated with substantially impaired quality of life (QOL) and a significant increase in the risk of cardiovascular disease and premature death (22–25).
Patient-reported outcome measures (PROMs) are direct responses from patients without alteration or interpretation by a clinician (12, 14). Use of PROMs can improve the assessment of disease burden among patients with CKD (12, 14). As such, incorporation of PROMs in routine clinical care would be an important tool toward facilitating patient-centered care (26–29). Moreover, involving patients in defining clinical and research priorities has the potential to enhance the relevance and acceptability of research from the perspective of all stakeholders, including patients, the public, clinicians, funding and regulating agencies, and policy makers (29, 30) In addition, establishing a shared platform of understanding may improve patient-provider communication, increase adherence, and improve clinical outcomes (31, 32). Perhaps the most crucial component of patient engagement is incorporating the lived patient experience in health care delivery.
There has been an increasing interest in the systematic collection of patient-reported outcomes (PROs) data for monitoring the impact of chronic illness and improving care among patients with chronic medical conditions such as cancer, rheumatoid arthritis, chronic obstructive pulmonary disease, and heart failure (14, 15, 33–35). Patient-reported measures (PRMs) have been shown to be superior to clinician reports both in the detection of symptoms and side effects of treatment, while also, being more sensitive to changes in functional status compared with standard of care (14, 36–39).
Using electronic data capture to assess PROMs may improve the feasibility of assessing PROMs in routine clinical practice (40–42). It eliminates the need for subsequent data entry, storage of the questionnaires, and reduces the risk of privacy breach. It has the potential for immediate scoring and presentation of the results (43–45), offers the potential to link PROMs with clinical data in electronic health records (46, 47), to enhance communication in multidisciplinary care (48, 49), and to facilitate the assessment of PROMs independently from patient-provider encounters (43, 44, 48, 50). Electronic collection of PROs has been linked to improved QOL, reduced rates of hospitalization, and increased adherence and survival among a large cohort of outpatients receiving chemotherapy for advanced cancer (39). These findings support the use and potential implications of using PROs in CKD management (39, 47).
The aim of this review is to explore the use of PROs in the CKD population. In Part 1, we will describe PROs and implications of use. In Part 2, we will review the selection of appropriate PROMs and the relevant domains of interest for patients with CKD.
Chronic Kidney Disease
Defining CKD
Chronic kidney disease is a chronic, frequently progressive condition, defined by structural or functional abnormalities of the kidney and/or a reduced glomerular filtration rate (GFR) of less than 60 mL/min/1.73 m2 for more than 3 months (51–55). It is caused by many different conditions including diabetes mellitus, hypertension, glomerulonephritis, genetic diseases, drug toxicity, urological conditions, infections, and acute kidney injury, among others (55, 56). CKD is a heterogeneous condition due to the varying severity and risk of progression, cause and pathology of disease, and comorbidities experienced by individual patients (57).
The classification of CKD is based on GFR (G category) and abnormal urinary albumin excretion (A category) (10, 54, 55, 58, 59). CKD is divided into five GFR stages, ranging from G1, representing normal to high kidney function with evidence of kidney disease, to G5 (GFR < 15 mL/min/1.73 m2), known as end-stage kidney disease (ESKD). Patients with various stages of CKD can be managed by lifestyle changes and medications with the aim of slowing disease progression (53, 55, 59). ESKD, however, is potentially life threatening without receiving renal replacement therapy (RRT) in the form of dialysis (peritoneal or hemodialysis) or kidney transplantation (10, 52, 60). Classification guidelines recommend the use of a suffix to identify the RRT modality in patients with stage 5 CKD; with “D” representing dialysis and “T” representing a functioning kidney transplant (52, 55). The stages of CKD enable classification of the severity of renal impairment with existing guidelines in place aimed at management of each stage (10, 54, 55).
Epidemiology and Significance of CKD
The latest estimates indicate that the prevalence of CKD is about 14% in Americans, 12.5% in Canadians, and 8–16% globally (61–64). CKD continues to be a growing public health concern for several reasons. Firstly, CKD is frequently caused by diabetes, hypertension, and obesity, with the prevalence of these conditions increasing (16–20, 55, 56, 65). As a result, the incidence of CKD is expected to rise simultaneously (19, 66, 67). Progressive aging of the CKD population is associated with increasing morbidity burden (19, 54, 58, 65, 67, 68), resulting in high rates of mortality (23–25, 69, 70) and severely impaired QOL (22, 71, 72). Often underdiagnosed and undertreated, the psychosocial distress associated with CKD further increase the morbidity and disease burden in this patient population (73–77). Globally, these trends pose dramatic consequences for health care financing and delivery systems (78).
In addition to the human suffering, management of CKD is costly (79, 80). In the United States, the annual cost of each patient undergoing dialysis ranges between 26,000 and 85,000 US dollars, depending on type of dialysis (60, 62, 79, 81). Comparatively, the average annual cost of dialysis per patient in Canada is estimated to be approximately 60,000 Canadian dollars (or approximately 45,000 US dollars) (82). As the prevalence of CKD increases, the associated cost burden will also continue to rise (78, 79).
Kidney transplantation has emerged in the past decade as the gold standard of RRT as it is associated with improved QOL (70, 83–85), decreased morbidity (70, 84), and decreased mortality (20, 70, 86, 87). Furthermore, transplantation is also substantially more cost-effective than maintenance dialysis (78, 79, 88–90). However, a global shortage of available organs prevents kidney transplant from being a universally accessible treatment modality (67, 91).
CKD as a Chronic Condition
Although patients with CKD can be managed with medications and RRT, these treatments will not reinstate normal kidney function. The primary goals of medical treatment during earlier stages of the disease are to prevent or slow disease progression, reduce the consequences of CKD, and to detect and manage subsequent complications (51, 57, 60). Complications and consequences include anemia, fatigue, sleep disorders, mental health conditions (such as depression and anxiety), bone and mineral disorders, and cardiovascular diseases (22, 76, 92, 93). Ultimately, as patients proceed through the stages of CKD, there is a marked increase in symptom burden, impairment of QOL (22, 94), and an increase in morbidity (22, 71, 95). Consequently, management of CKD presents a unique challenge as the needs of patients change as the disease progresses through its various stages (96–98).
Patient-Reported Measures
Traditional clinical tests do not adequately assess the health status, well-being, and functional capacity of patients as patients with similar clinical severity may have vastly different responses to the disease process (99, 100). Likewise, biomedical characteristics and biomarkers are often inadequate for predicting the subsequent illness trajectory (101, 102) or response to a specific treatment. Incorporating the patient experience and patient perspective can improve the accuracy and completeness of assessment and may improve the prediction of outcomes (13, 40–42, 103, 104). These observations led to the rise of health frameworks with patient-centered care as the focus, offering a much more holistic approach to the measurement of outcomes (3, 5–12).
Quality of Life
The first studies focusing on patient-centered care measured QOL: the Almeda County study (105), the RAND Health Insurance study (106), and the Medical Outcomes study (107, 108). These studies represented a major shift in ideology toward one, which took patient’s priorities into consideration. More recently, the World Health Organization defines QOL as “the individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns (109). Recognizing the breadth of this definition, the medical community further refined this concept in the context of health and coined the term health-related quality of life (HRQOL) (108).
Health-Related Quality of Life
There are various definitions of HRQOL in the literature and their detailed comparative assessment is beyond the scope of this review. For the purpose of this review, HRQOL is defined as the “impact of disease and treatment across the physical, psychological, social and somatic domains of functioning and well-being” (108, 110). Measuring HRQOL offers a patient’s subjective perspective on their understanding and experience of the disease and/or its treatment on their overall health and well-being (111, 112). Critics of HRQOL claim that there is a lack of conceptual clarity and measurement feasibility (113). Recent advancement in patient-centered care has striven to address the aforementioned issues and have been broadly classified as PRMs (12, 14).
Patient-Reported Measures
Although QOL, HRQOL, PROMs, and PRMs are often used interchangeably, these terms have important distinctions regarding dimensionality and scope (34, 108). A PRM is any measure that is reported directly by patients without interpretation from a clinician or other health care provider (12, 14). PRMs carry a broader scope in comparison to HRQOL by collecting any information reported by the patient, beyond QOL or HRQOL alone (13, 114, 115).
Patient-reported measures can be classified into two different categories: PROs, referring to one’s perception of health status, and patient-reported experiences (PREs), referring to one’s perception of the care they received (12, 14, 35, 116, 117). Tools designed to measure PROs and PREs are thus labeled as PROMs or patient-reported experience measures (PREMs) (12, 14, 116, 117).
Patient-reported outcome measures can be used to assess a wide variety of health-relevant concepts and are indispensable for gathering comprehensive information about a patient (12, 14). There are four overarching categories of information that PROMs can assess: HRQOL, functional status, symptoms and symptom burden, and health behaviors and perceptions (13, 14). In contrast, PREMs provide an evaluation of quality of health care delivery from the patient’s perspective, such as facility cleanliness, access to information and health care teams, communication, support received, and transportation (12). A core tenant of PROMs and PREMs requires that responses are received without any interpretation as this enables an accurate and unadulterated account about the patient.
Utility of PRMs in Clinical Practice
While the use of PROMs in clinical practice is gaining increasing popularity, the utility of PREMs has been the subject of debate (12, 14, 35, 118, 119). This debate was driven by the inclusion of PREMs as a metric for governmental health care reimbursement in the United States, which resulted in private insurers following suit (12, 119, 120). Subsequently, several studies have suggested that PREMs have limited utility as a marker of quality of care, with PREMs being shown to have little to no association with quality of care or clinical outcomes (35, 118, 120, 121). PROMs, on the other hand, have demonstrated significant association with clinical outcomes (12, 14, 103, 104, 122).
Measuring PROMs during clinical encounters provides an opportunity for patients to reveal physical, psychological, or social concerns that might have an impact on their daily life. These might be concerns not discussed, overlooked, or underestimated by the health care team (36, 112). They also enable the medical team to accurately assess and quantify symptom burden and HRQOL: vital components of the chronic illness experience. Integration of PROMs within the clinical care of patients with CKD has the potential to improve the lives of individual patients and also to understand care needs on the population level (40, 41, 123). Recognition of the importance of PROMs have resulted in the development of guidelines by national organizations to provide guidance on the implementation and reporting of PROMs (117, 124). Since PROMs have shown increased utility and implications for clinical research, the remainder of this paper will focus on PROMs.
Patient-Reported Outcome Measures
Structure of PROMs
Patient-reported outcome measures are composed of individual questions or statements (with standardized response options), also known as items. Items are related to particular domains, which are overarching, measurable themes of interest (e.g., physical functioning, emotional well-being, etc.). Certain PROMs have algorithms in place to aggregate individual items that are similar, into specific composite ratings or domain scores. For instance, one PROM frequently used in CKD is the Kidney Disease Quality of Life Short Form (KDQOL-SF) (88, 125, 126). The general domains include the following: physical functioning, physical role functioning, bodily pain, general health perceptions, vitality, emotional role functioning, social role functioning, and mental health and additional, kidney disease-related domains, such as effects of kidney disease, burden of kidney disease, symptom list, sleep problems—each with scores ranging from 0 to 100 (125, 126). In addition, physical and mental health composite scores are generated, also ranging from 0 to 100, with higher scores representing better overall physical or mental health, respectively (126).
PROMs in CKD
Various PROMs have been developed and validated in the CKD population and can typically be classified as a generic instrument or a CKD-specific instrument (92, 127–130). Generic instruments are PROMs that measure various aspects of patients’ health status and can be administered across the general population or in any patient populations (see Table 1). This is advantageous as it allows for different populations to be more readily compared; however, the variance in burden of disease in certain populations can result in a ceiling or floor effect (127, 131–133). Ceiling or floor effects occur when subjects score at the bottom (floor effect) or at the top (ceiling effect) of the range of a scale, usually because the items are too easy or too difficult. This means that the scale cannot discriminate individuals even with different amounts of the measured trait above or below those points. In addition, because generic tools do not assess disease specific characteristics, they are less sensitive to the severity of disease and may be less responsive to change in the condition in response to treatments or as the condition progresses (134). Some commonly known generic instruments include the Medical Outcomes Study Short Form (SF-36, SF-20, SF-12) (129, 135–139), Quality of Well Being Scale (140), Sickness Impact Profile (SIP) (141, 142), EuroQol (143, 144), Patient-Reported Outcomes Measurement Information System (PROMIS-57, PROMIS-43, PROMIS-29) (33, 115), World Health Organization Quality of Life Scale (WHOQOL-BREF) (145, 146), Illness Intrusiveness Rating Scale (IIRS) (147–149), Patient Health Questionnaire (PHQ) (150, 151), Social Difficulties Inventory (SDI) (152), Generalized Anxiety Disorder 7-item Scale (GAD-7) (153), Edmonton Symptom Assessment System (ESAS) (154–156), Epworth Sleepiness Scale (ESS) (157), Cambridge-Hopkins diagnostic questionnaire for Restless Leg Syndrome (CH-RLSq) (158), and Health Utility Index (88, 127, 129, 133, 135, 136, 159, 160).
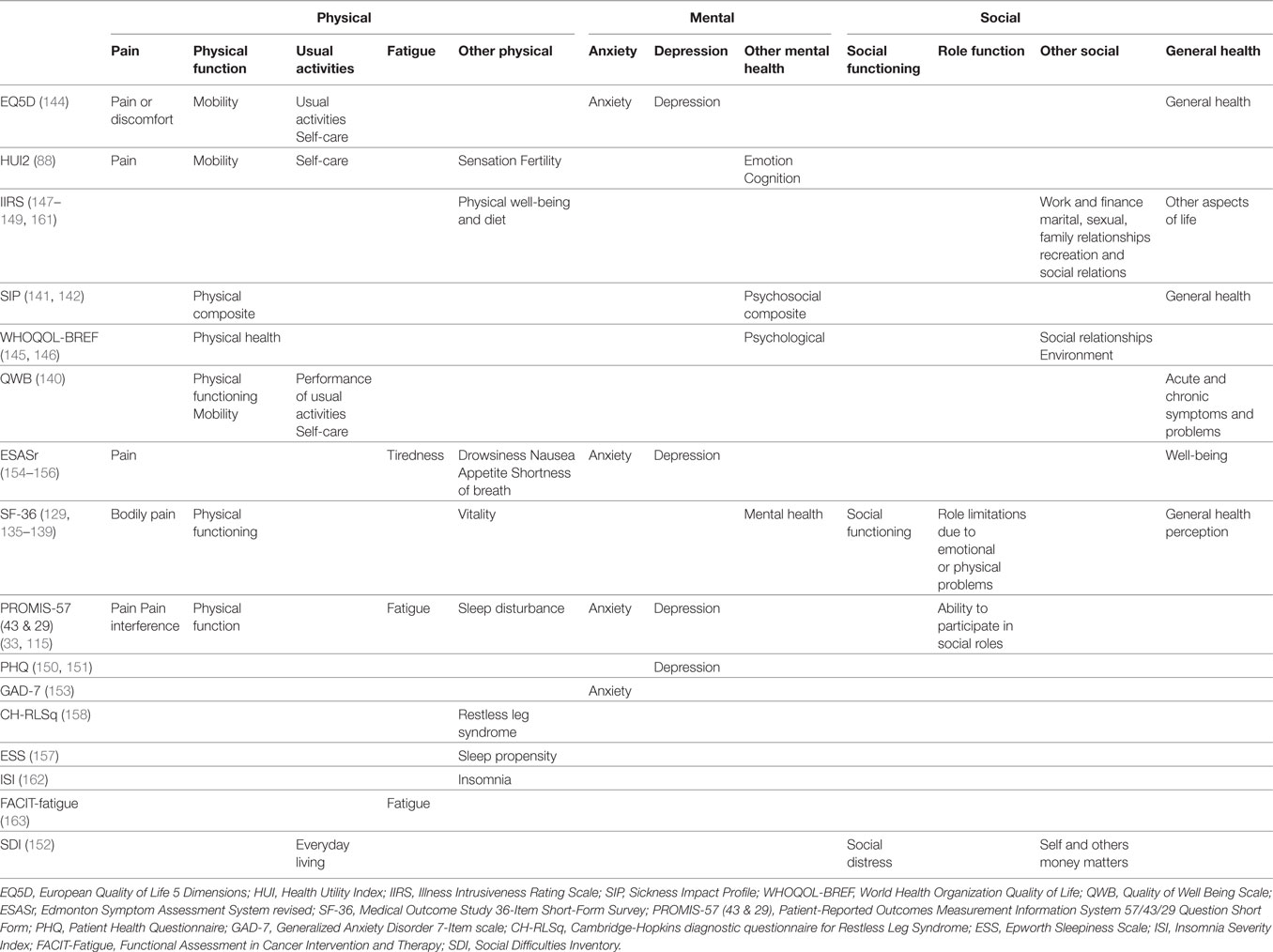
Table 1. Selected generic PROMs and their measured domains.
Chronic-kidney-disease-specific instruments are PROMs that are tailored to the specific symptom burden and disease experience by patients with CKD (see Table 2) (22, 116, 127, 159). These instruments are often very specific, thus avoiding the ceiling or floor effects observed when using generic instruments (127, 132). The specificity of the questions, however, usually precludes its use in other populations thus limiting generalizability of results (127, 133). Some commonly known CKD-specific instruments include the following: Kidney Disease Quality of Life (KDQOL) (136, 164), Quality of Life Index Dialysis version (QLI-D) (165, 166), Kidney Disease Questionnaire (KDQ) (167), Kidney Transplant Questionnaire (KTQ) (168), Renal Quality of Life Profile (RQLP) (169), CHOICE Health Experience Questionnaire (CHEQ) (170), End-Stage Renal Disease Symptom Checklist–Transplant Module (ESRD-SCL-TM) (171), and Renal Dependent Individualized Quality of Life Questionnaire (125, 127, 136, 170, 172–174). By no means exhaustive, a more comprehensive list of PROMs will be explored in Part 2 of our review. Despite the wide selection of available PROMs, we are not aware of routine PROM use in nephrology clinical settings currently.
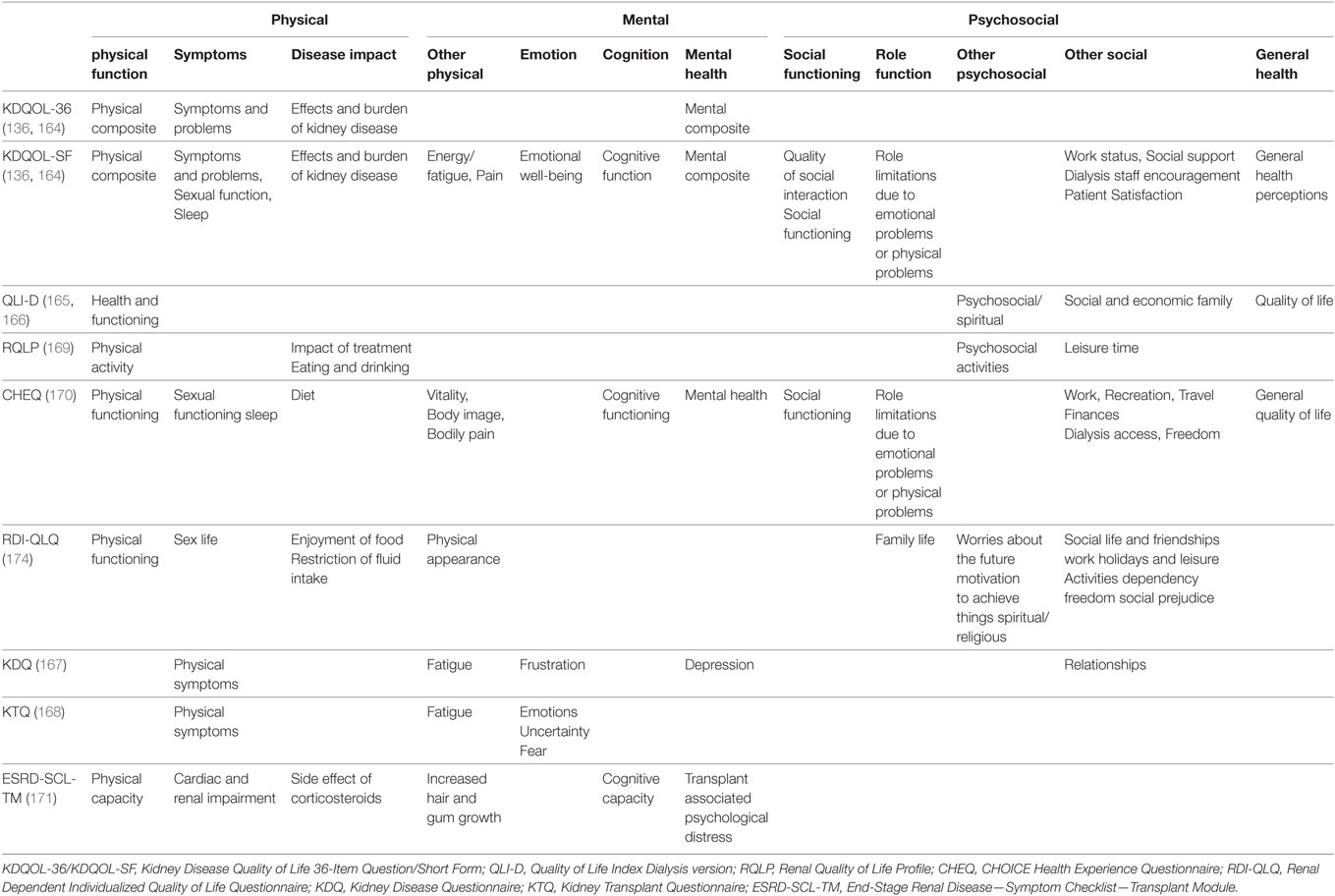
Table 2. Selected CKD-specific PROMs and their measured domains.
Implications of PROMs in Clinical Care
Measurement of PROs provides information about patient health and well-being which cannot be obtained by traditional medical/biological assessments (11, 12, 14). Responses through a subjective lens, without clinician interpretation, facilitate a holistic approach by gaining insight into patients’ values and preferences while also obtaining reports on outcomes of care (11, 12, 31, 32). An important goal of the extensive research in PROMs would be the eventual integration of tools into the standard of care of patients with CKD. There are many implications for clinical practice based on the results drawn from PROMs. Integration of PROMs can enhance patient-centered care, facilitate communication between patients and health care providers as well as between health care team members, and provide information for evaluating clinical outcomes (3, 6, 9, 40, 41, 119).
Enhanced Patient-Centered Care
Patient-reported outcome measures can be used to guide treatment options by elucidating domains that require intervention, especially those that are frequently under-assessed or neglected by the managing health care teams (9, 175). For instance, the identification of psychological distress, sleep problems, fatigue, social difficulties, and/or pain interference scores or low physical function scores can assist the health care team in tailoring treatment to target these areas (7, 11). Beyond merely identifying domains, PROMs can assist to determine the level of severity within each domain. Periodic collection of PROMs allows the health care team to track the progression of symptoms and subjective health status, as well the impact of different treatment modalities (176). Longitudinal assessment of PROMs can further be utilized in a “treat to target” approach, where treatment and referrals are prescribed with the aim of achieving a specific score (177, 178). Major deviations from baseline scores can also serve as an indicator for interventions.
Patient-reported outcome measures can also be utilized to identify which symptoms are personally relevant and important to patients, which is an essential component of assessing the impact of disease and their QOL (179). Considering the recent finding that 80% of current clinical research does not include the top 10 research priorities as identified by patients on or nearing dialysis, understanding patients’ needs, values, and opinions are crucial to improving outcomes (9, 27, 31, 32). As such, PROMs can be used to address this disparity in current research, by utilizing information from PROMs to align research priorities with patient priorities (26, 31–33).
Enhanced Communication
The use of PROMs can facilitate better communication between the patient and provider. This is possibly due to PROMs providing an avenue to broach on topics related to specific domains, such as adverse events, anxiety, or depression, which may otherwise not be communicated openly by patients or overlooked by the health care team (83, 180–182). Other findings suggest that use of PROMs improves patient engagement by engaging patients in treatment planning and evaluation (182, 183). In addition, Schorn et al. demonstrated that use of PROM in primary care improved self-management behavior (183). Ultimately, this has the potential to improve patient outcomes as seen in the study conducted by Basch et al., where patients randomized to the group using PROMs expressed a greater number of symptoms and had better overall survival and less hospitalization compared with the group receiving standard care (39).
Clinical Outcomes
Paramount to the discussion of implication is that of “hard” clinical outcomes, such as mortality, hospitalization, and symptom burden. Many studies have suggested that PROs have the potential to be used for prognostication (103, 104, 184–187). While links between clinical outcomes and PROs have been identified, only a few studies have explored the impact of interventions on these outcomes (188). Further studies are required to elucidate the impact of PRO modification on clinical outcomes.
Conclusion
In this paper, we have reviewed the relevance and importance of using PROMs in the context of CKD, largely supported by the need to address currently unexplored aspects of the illness experience of patients suffering from the multifaceted and chronic nature of this disease, which contribute to a high symptom burden and clinical outcomes. This includes both physical and psychosocial concerns, which are often overlooked in this patient population. As such, the value of patient involvement in care delivery and research is increasingly recognized. PROMs are the latest frontier as a means of collecting and utilizing patient-reported information without clinician interpretation. This not only provides a means to identify and address the patient concerns but also has benefits including the facilitation of patient-centered care, enhancing communication, and elucidating research priorities. PROMs, however, are still a growing field with implications for clinical practice that is still being uncovered in the context of CKD. In Part 2, we will explore the domains of interest for patients with CKD and the selection of appropriate PROMs.
Author Contributions
ET and AB were involved in the conception of the review, including a critical review of the literature accompanied by the drafting of the manuscript. MN and IM provided support in the form of professional appraisal and the provision of supporting literature. Critical revisions were performed and the final version was reviewed and approved by both IM and MN.
Conflict of Interest Statement
The authors declare that this review was conducted without any commercial or financial conflict of interest.
References
1. McGrail K, Bryan S, Davis J. Let’s all go to the PROM: the case for routine patient-reported outcome measurement in Canadian healthcare. Healthc Pap (2011) 11(4):8–18. doi:10.12927/hcpap.2012.22697
2. Nugent R. Chronic diseases in developing countries. Ann N Y Acad Sci (2008) 1136(1):70–9. doi:10.1196/annals.1425.027
3. Epstein RM, Street RL. The values and value of patient-centered care. Ann Fam Med (2011) 9(2):100–3. doi:10.1370/afm.1239
4. Snyder CF, Jensen RE, Segal JB, Wu AW. Patient-reported outcomes (PROs): putting the patient perspective in patient-centered outcomes research. Med Care (2013) 51:S73–9. doi:10.1097/MLR.0b013e31829b1d84
5. Wasson JH, Godfrey MM, Nelson EC, Mohr JJ, Batalden PB. Microsystems in health care: part 4. Planning patient-centered care. Jt Comm J Qual Saf (2003) 29(5):227–37. doi:10.1016/S1549-3741(03)29027-4
6. Greene SM, Tuzzio L, Cherkin D. A framework for making patient-centered care front and center. Perm J (2012) 16(3):49–53.
8. Havas K, Douglas C, Bonner A. Person-centred care in chronic kidney disease: a cross-sectional study of patients’ desires for self-management support. BMC Nephrol (2017) 18:17. doi:10.1186/s12882-016-0416-2
9. Bear RA, Stockie S. Patient engagement and patient-centred care in the management of advanced chronic kidney disease and chronic kidney failure. Can J Kidney Health Dis (2014) 1:24. doi:10.1186/s40697-014-0024-7
10. Kidney disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012. Clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl (2013) 3:1–150.
11. Black N. Patient reported outcome measures could help transform healthcare. Br Med J (2013) 346:f167. doi:10.1136/bmj.f167
12. Weldring T, Smith SMS. Patient-reported outcomes (PROs) and patient-reported outcome measures (PROMs). Health Serv Insights (2013) 6:61–8. doi:10.4137/HSI.S11093
13. Cella D, Hahn EA, Jensen SE, Butt Z, Nowinski CJ, Rothrock N, et al. Patient-Reported Outcomes in Performance Measurement. Research Triangle Park, NC: RTI Press Publication (2015).
14. Deshpande PR, Rajan S, Sudeepthi BL, Abdul Nazir CP. Patient-reported outcomes: a new era in clinical research. Perspect Clin Res (2011) 2(4):137–44. doi:10.4103/2229-3485.86879
15. Kojima M, Kojima T, Suzuki S, Takahashi N, Funahashi K, Asai S, et al. Patient-reported outcomes as assessment tools and predictors of long-term prognosis: a 7-year follow-up study of patients with rheumatoid arthritis. Int J Rheum Dis (2015) 20(9):1193–200. doi:10.1111/1756-185X.12789
16. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes. Estimates for the year 2000 and projections for 2030. Diabetes Care (2004) 27(5):1047–53. doi:10.2337/diacare.27.5.1047
17. Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, et al. Global disparities of hypertension prevalence and control. a systematic analysis of population-based studies from 90 countries. Circulation (2016) 134(6):441–50. doi:10.1161/CIRCULATIONAHA.115.018912
18. Padwal RS, Bienek A, McAlister FA, Campbell NR. Epidemiology of hypertension in Canada: an update. Can J Cardiol (2016) 32(5):687–94. doi:10.1016/j.cjca.2015.07.734
20. Novak M, Mucsi I, Rhee CM, Streja E, Lu JL, Kalantar-Zadeh K, et al. Increased risk of incident chronic kidney disease, cardiovascular disease, and mortality in patients with diabetes with comorbid depression. Diabetes Care (2016) 39(11):1940–7. doi:10.2337/dc16-0048
21. Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet (2012) 380(9859):2095–128. doi:10.1016/S0140-6736(12)61728-0
22. Abdel-Kader K, Unruh ML, Weisbord SD. Symptom burden, depression, and quality of life in chronic and end-stage kidney disease. Clin J Am Soc Nephrol (2009) 4(6):1057–64. doi:10.2215/CJN.00430109
23. Culleton BF, Larson MG, Wilson PW, Evans JC, Parfrey PS, Levy D. Cardiovascular disease and mortality in a community-based cohort with mild renal insufficiency. Kidney Int (1999) 56(6):2214–9. doi:10.1046/j.1523-1755.1999.00773.x
24. Garg AX, Clark WF, Haynes RB, House AA. Moderate renal insufficiency and the risk of cardiovascular mortality: results from the NHANES I. Kidney Int (2002) 61(4):1486–94. doi:10.1046/j.1523-1755.2002.00270.x
25. Muntner P, He J, Hamm L, Loria C, Whelton PK. Renal insufficiency and subsequent death resulting from cardiovascular disease in the United States. J Am Soc Nephrol (2002) 13(3):745–53.
26. Demian MN, Lam NN, Mac-Way F, Sapir-Pichhadze R, Fernandez N. Opportunities for engaging patients in kidney research. Can J Kidney Health Dis (2017) 4:2054358117703070. doi:10.1177/2054358117703070
27. Jun M, Manns B, Laupacis A, Manns L, Rehal B, Crowe S, et al. Assessing the extent to which current clinical research is consistent with patient priorities: a scoping review using a case study in patients on or nearing dialysis. Can J Kidney Health Dis (2015) 2:35. doi:10.1186/s40697-015-0070-9
28. Basch E, Abernethy AP. Supporting Clinical Practice Decisions With Real-Time Patient-Reported Outcomes. J Clin Oncol (2011) 29(8):994–1024. doi:10.1200/JCO.2010.33.2668
29. Haywood K, Brett J, Salek S, Marlett N, Penman C, Svetlana S, et al. Patient and public engagement in health-related quality of life and patient-reported outcomes research: what is important and why should we care? Findings from the first ISOQOL patient engagement symposium. Qual Life Res (2014) 24(5):1069–76. doi:10.1007/s11136-014-0796-3
30. Staniszewska S, Denegri S. Patient and public involvement in research: future challenges. Evid Based Nurs (2013) 16(3):69. doi:10.1136/eb-2013-101406
31. Tong A, Sainsbury P, Carter SM, Hall B, Harris DC, Walker RG, et al. Patients’ priorities for health research: focus group study of patients with chronic kidney disease. Nephrol Dial Transplant (2008) 23(10):3206–14. doi:10.1093/ndt/gfn207
32. Hemmelgarn BR, Pannu N, Ahmed SB, Elliott MJ, Tam-Tham H, Lillie E, et al. Determining the research priorities for patients with chronic kidney disease not on dialysis. Nephrol Dial Transplant (2017) 32(5):847–54. doi:10.1093/ndt/gfw065
33. Bartlett SJ, Witter J, Cella D, Ahmed S. Montreal accord on patient-reported outcomes use series—paper 6: creating national initiatives to support patient reported outcomes (PRO) development and use-the PROMIS example. J Clin Epidemiol (2017) 89:148–53. doi:10.1016/j.jclinepi.2017.04.015
34. Chen H, Taichman DB, Doyle RL. Health-related quality of life and patient-reported outcomes in pulmonary arterial hypertension. Proc Am Thorac Soc (2008) 5(5):623–30. doi:10.1513/pats.200802-020SK
35. Hodson M, Andrew S, Michael Roberts C. Towards an understanding of PREMS and PROMS in COPD. Breathe (2013) 9(5):358. doi:10.1183/20734735.006813
36. Basch E. The missing voice of patients in drug-safety reporting. N Engl J Med (2010) 362(10):865–9. doi:10.1056/NEJMp0911494
37. Pakhomov SV, Jacobsen SJ, Chute CG, Roger VL. Agreement between patient-reported symptoms and their documentation in the medical record. Am J Manag Care (2008) 14(8):530–9.
38. Weingart SN, Gandhi TK, Seger AC, Seger DL, Borus J, Burdick E, et al. Patient-reported medication symptoms in primary care. Arch Intern Med (2005) 165(2):234–40. doi:10.1001/archinte.165.2.234
39. Basch E, Deal AM, Kris MG, Scher HI, Hudis CA, Sabbatini P, et al. Symptom monitoring with patient-reported outcomes during routine cancer treatment: a randomized controlled trial. J Clin Oncol (2016) 34(6):557–65. doi:10.1200/JCO.2015.63.0830
40. Baumhauer JF. Patient-reported outcomes—are they living up to their potential? N Engl J Med (2017) 377(1):6–9. doi:10.1056/NEJMp1702978
41. Baumhauer JF, Bozic KJ. Value-based healthcare: patient-reported outcomes in clinical decision making. Clin Orthop Relat Res (2016) 474(6):1375–8. doi:10.1007/s11999-016-4813-4
42. Ho B, Houck JR, Flemister AS, Ketz J, Oh I, DiGiovanni BF, et al. Preoperative PROMIS Scores Predict Postoperative Success in Foot and Ankle Patients. Foot Ankle Int (2016) 37(9):911–8. doi:10.1177/1071100716665113
43. Abernethy AP, Ahmad A, Zafar SY, Wheeler JL, Reese JB, Lyerly HK. Electronic patient-reported data capture as a foundation of rapid learning cancer care. Med Care (2010) 48(6 Suppl):S32–8. doi:10.1097/MLR.0b013e3181db53a4
44. Chang Y-J, Chang C-H, Peng C-L, Wu H-C, Lin H-C, Wang J-Y, et al. Measurement equivalence and feasibility of the EORTC QLQ-PR25: paper-and-pencil versus touch-screen administration. Health Qual Life Outcomes (2014) 12:23. doi:10.1186/1477-7525-12-23
45. Holzner B, Giesinger JM, Pinggera J, Zugal S, Schöpf F, Oberguggenberger AS, et al. The Computer-based Health Evaluation Software (CHES): a software for electronic patient-reported outcome monitoring. BMC Med Inform Decis Mak (2012) 12:126. doi:10.1186/1472-6947-12-126
46. Bennett AV, Jensen RE, Basch E. Electronic patient-reported outcome systems in oncology clinical practice. CA Cancer J Clin (2012) 62(5):337–47. doi:10.3322/caac.21150
47. Snyder CF, Aaronson NK, Choucair AK, Elliott TE, Greenhalgh J, Halyard MY, et al. Implementing patient-reported outcomes assessment in clinical practice: a review of the options and considerations. Qual Life Res (2012) 21(8):1305–14. doi:10.1007/s11136-011-0054-x
48. Smith SK, Rowe K, Abernethy AP. Use of an electronic patient-reported outcome measurement system to improve distress management in oncology. Palliative Support Care (2014) 12(01):69–73. doi:10.1017/S1478951513000345
49. Dupont A, Wheeler J, Herndon JE, Coan A, Zafar SY, Hood L, et al. Use of tablet personal computers for sensitive patient-reported information. J Support Oncol (2009) 7(3):91–7.
50. Espallargues M, Valderas JM, Alonso J. Provision of feedback on perceived health status to health care professionals: a systematic review of its impact. Med Care (2000) 38(2):175–86. doi:10.1097/00005650-200002000-00007
51. Stevens PE, Levin A. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med (2013) 115(11):825–30. doi:10.7326/0003-4819-158-11-201306040-00007
52. National Kidney Foundation. KDOQI clinical practice guideline for diabetes and CKD: 2012 update. Am J Kidney Dis (2012) 60(5):850–86. doi:10.1053/j.ajkd.2012.07.005
53. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis (2002) 39(2 Suppl 1):S1–266.
54. Levey AS, Coresh J. Chronic kidney disease. Lancet (2012) 379(9811):165–80. doi:10.1016/S0140-6736(11)60178-5
55. Levey AS, Eckardt KU, Tsukamoto Y, Levin A, Coresh J, Rossert J, et al. Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int (2005) 67(6):2089–100. doi:10.1111/j.1523-1755.2005.00365.x
56. Evans PD, Taal MW. Epidemiology and causes of chronic kidney disease. Medicine (2015) 43(8):450–3. doi:10.1016/j.mpmed.2015.05.005
57. Levey AS, Stevens LA, Coresh J. Conceptual model of CKD: applications and implications. Am J Kidney Dis (2009) 53(3 Suppl 3):S4–16. doi:10.1053/j.ajkd.2008.07.048
58. Thomas R, Kanso A, Sedor JR. Chronic kidney disease and its complications. Prim Care (2008) 35(2):329–vii. doi:10.1016/j.pop.2008.01.008
59. Akbari A, Clase CM, Acott P, Battistella M, Bello A, Feltmate P, et al. Canadian Society of Nephrology commentary on the KDIGO clinical practice guideline for CKD evaluation and management. Am J Kidney Dis (2015) 65(2):177–205. doi:10.1053/j.ajkd.2014.10.013
60. Levin A, Hemmelgarn B, Culleton B, Tobe S, McFarlane P, Ruzicka M, et al. Guidelines for the management of chronic kidney disease. CMAJ (2008) 179(11):1154–62. doi:10.1503/cmaj.080351
61. CDC. National Chronic Kidney Disease Fact Sheet: General Information and National Estimates on Chronic Kidney Disease in the United States, 2014. Atlanta, GA: CDC (2014).
62. Arora P, Vasa P, Brenner D, Iglar K, McFarlane P, Morrison H, et al. Prevalence estimates of chronic kidney disease in Canada: results of a nationally representative survey. CMAJ (2013) 185(9):E417–23. doi:10.1503/cmaj.120833
63. Hill NR, Fatoba ST, Oke JL, Hirst JA, O’Callaghan CA, Lasserson DS, et al. Global prevalence of chronic kidney disease—a systematic review and meta-analysis. PLoS One (2016) 11(7):e0158765. doi:10.1371/journal.pone.0158765
64. Mandayam S, Winkelmayer WC. Worldwide preparedness for kidney health care. JAMA (2017) 317(18):1838–9. doi:10.1001/jama.2017.2825
65. Jha C, Garcia-Garcia G, Iseki K, Li Z, Naicker S, Plattner B, et al. Chronic kidney disease: global dimension and perspectives. Lancet (2013) 382(9888):12. doi:10.1016/S0140-6736(13)60687-X
66. Stevens LA, Viswanathan G, Weiner DE. Chronic kidney disease and end-stage renal disease in the elderly population: current prevalence, future projections, and clinical significance. Adv Chronic Kidney Dis (2010) 17(4):293–301. doi:10.1053/j.ackd.2010.03.010
67. Webster G, Wu J, Terner M, Ivis F, de Sa E, Hall N. Canadian Organ Replacement Register Annual Report: Treatment of End-Stage Organ Failure in Canada, 2004 to 2013. Canadian Institute for Health Information (2015).
68. Schoolwerth AC, Engelgau MM, Rufo KH, Vinicor F, Hostetter TH, Chianchiano D, et al. Chronic kidney disease: a public health problem that needs a public health action plan. Prev Chronic Dis (2006) 3(2):A57.
69. Wannamethee SG, Shaper AG, Perry IJ. Serum creatinine concentration and risk of cardiovascular disease: a possible marker for increased risk of stroke. Stroke (1997) 28(3):557–63. doi:10.1161/01.STR.28.3.557
70. Tonelli M, Wiebe N, Knoll G, Bello A, Browne S, Jadhav D, et al. Systematic review: kidney transplantation compared with dialysis in clinically relevant outcomes. Am J Transplant (2011) 11(10):2093–109. doi:10.1111/j.1600-6143.2011.03686.x
71. Cruz MC, Andrade C, Urrutia M, Draibe S, Nogueira-Martins LA, de Castro Cintra Sesso R. Quality of life in patients with chronic kidney disease. Clinics (2011) 66(6):991–5. doi:10.1590/S1807-59322011000600012
72. Finkelstein FO, Wuerth D, Finkelstein SH. Health related quality of life and the CKD patient: challenges for the nephrology community. Kidney Int (2009) 76(9):946–52. doi:10.1038/ki.2009.307
73. Moreira JM, Matta SM, Kummer AM, Barbosa IG, Teixeira AL, Silva ACS. Transtornos neuropsiquiátricos e doenças renais: uma atualização. Jornal Brasileiro de Nefrologia (2014) 36:396–400. doi:10.5935/0101-2800.20140056
74. Kellerman QD, Christensen AJ, Baldwin AS, Lawton WJ. Association between depressive symptoms and mortality risk in chronic kidney disease. Health Psychol (2010) 29(6):594–600. doi:10.1037/a0021235
75. Cukor D, Cohen SD, Peterson RA, Kimmel PL. Psychosocial aspects of chronic disease: ESRD as a paradigmatic illness. J Am Soc Nephrol (2007) 18(12):3042–55. doi:10.1681/ASN.2007030345
76. Kimmel PL. Depression in patients with chronic renal disease: what we know and what we need to know. J Psychosom Res (2002) 53(4):951–6. doi:10.1016/S0022-3999(02)00310-0
77. Cukor D, Peterson RA, Cohen SD, Kimmel PL. Depression in end-stage renal disease hemodialysis patients. Nat Clin Pract Neph (2006) 2(12):678–87. doi:10.1038/ncpneph0359
78. Wang V, Vilme H, Maciejewski ML, Boulware LE. The economic burden of chronic kidney disease and end-stage renal disease. Semin Nephrol (2016) 36(4):319–30. doi:10.1016/j.semnephrol.2016.05.008
79. Klarenbach SW, Tonelli M, Chui B, Manns BJ. Economic evaluation of dialysis therapies. Nat Rev Nephrol (2014) 10(11):644–52. doi:10.1038/nrneph.2014.145
80. Terner M, Redding N, Wu J. Increasing rates of kidney failure care in Canada strains demand for kidney donors. Healthcare Q (2016) 19(3):10–2. doi:10.12927/hcq.2016.24864
81. Saran R, Robinson B, Abbott K. US Renal Data System 2016 Annual Data Report: Epidemiology of Kidney Disease in the United States. United States Renal Data System (2017).
82. Canadian Institute for Health Information. Canadian Organ Replacement Register Annual Report: Treatment of End-Stage Organ Failure in Canada, 2001 to 2010. (2010).
83. Valderrábano F, Jofre R, López-Gómez JM. Quality of life in end-stage renal disease patients. Am J Kidney Dis (2001) 38(3):443–64. doi:10.1053/ajkd.2001.26824
84. Molnar-Varga M, Molnar MZ, Szeifert L, Kovacs AZ, Kelemen A, Becze A, et al. Health-related quality of life and clinical outcomes in kidney transplant recipients. Am J Kidney Dis (2011) 58(3):444–52. doi:10.1053/j.ajkd.2011.03.028
85. Kovacs AZ, Molnar MZ, Szeifert L, Ambrus C, Molnar-Varga M, Szentkiralyi A, et al. Sleep disorders, depressive symptoms and health-related quality of life—a cross-sectional comparison between kidney transplant recipients and waitlisted patients on maintenance dialysis. Nephrol Dial Transplant (2011) 26(3):1058–65. doi:10.1093/ndt/gfq476
86. Port FK, Wolfe RA, Mauger EA, Berling DP, Jiang K. Comparison of survival probabilities for dialysis patients vs cadaveric renal transplant recipients. JAMA (1993) 270(11):1339–43. doi:10.1001/jama.270.11.1339
87. Rabbat CG, Thorpe KE, Russell JD, Churchill DN. Comparison of mortality risk for dialysis patients and cadaveric first renal transplant recipients in Ontario, Canada. J Am Soc Nephrol (2000) 11(5):917–22.
88. Gorodetskaya I, Zenios S, McCulloch CE, Bostrom A, Hsu CY, Bindman AB, et al. Health-related quality of life and estimates of utility in chronic kidney disease. Kidney Int (2005) 68(6):2801–8. doi:10.1111/j.1523-1755.2005.00752.x
89. Pinsky BW, Takemoto SK, Lentine KL, Burroughs TE, Schnitzler MA, Salvalaggio PR. Transplant outcomes and economic costs associated with patient noncompliance to immunosuppression. Am J Transplant (2009) 9(11):2597–606. doi:10.1111/j.1600-6143.2009.02798.x
90. Barnieh L, Yilmaz S, McLaughlin K, Hemmelgarn BR, Klarenbach S, Manns BJ, et al. The cost of kidney transplant over time. Prog Trans (2014) 24(3):257–62. doi:10.7182/pit2014710
91. Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt KU, et al. Chronic kidney disease as a global public health problem: approaches and initiatives—a position statement from Kidney Disease Improving Global Outcomes. Kidney Int (2007) 72(3):247–59. doi:10.1038/sj.ki.5002343
92. Aiyegbusi OL, Kyte D, Cockwell P, Marshall T, Keeley T, Gheorghe A, et al. Measurement properties of patient-reported outcome measures (PROMs) used in adult patients with chronic kidney disease: a systematic review protocol. BMJ Open (2016) 6(10):e012014. doi:10.1136/bmjopen-2016-012014
93. Walters BA, Hays RD, Spritzer KL, Fridman M, Carter WB. Health-related quality of life, depressive symptoms, anemia, and malnutrition at hemodialysis initiation. Am J Kidney Dis (2002) 40(6):1185–94. doi:10.1053/ajkd.2002.36879
94. Almutary H, Bonner A, Douglas C. Symptom burden in chronic kidney disease: a review of recent literature. J Ren Care (2013) 39(3):140–50. doi:10.1111/j.1755-6686.2013.12022.x
95. Kopyt NP. Slowing progression along the renal disease continuum. J Am Osteopath Assoc (2005) 105(4):207–15.
96. Brand S, Pollock K. How is continuity of care experienced by people living with chronic kidney disease? J Clin Nurs (2018) 27:153–161. doi:10.1111/jocn.13860
97. Drawz PE, Archdeacon P, McDonald CJ, Powe NR, Smith KA, Norton J, et al. CKD as a model for improving chronic disease care through electronic health records. Clin J Am Soc Nephrol (2015) 10(8):1488–99. doi:10.2215/CJN.00940115
98. Fishbane S, Hazzan AD, Halinski C, Mathew AT. Challenges and opportunities in late-stage chronic kidney disease. Clin Kidney J (2015) 8(1):54–60. doi:10.1093/ckj/sfu128
100. Worth A, Hammersley V, Knibb R, Flokstra-de-Blok B, DunnGalvin A, Walker S, et al. Patient-reported outcome measures for asthma: a systematic review. NPJ Prim Care Respir Med (2014) 24:14020. doi:10.1038/npjpcrm.2014.20
101. Burke HB. Predicting clinical outcomes using molecular biomarkers. Biomark Cancer (2016) 8:89–99. doi:10.4137/BIC.S33380
102. Lopez-Giacoman S, Madero M. Biomarkers in chronic kidney disease, from kidney function to kidney damage. World J Nephrol (2015) 4(1):57–73. doi:10.5527/wjn.v4.i1.57
103. Sexton DJ, Lowney AC, O’Seaghdha CM, Murphy M, O’Brien T, Casserly LF, et al. Do patient-reported measures of symptoms and health status predict mortality in hemodialysis? An assessment of POS-S Renal and EQ-5D. Hemodial Int (2016) 20(4):618–30. doi:10.1111/hdi.12415
104. Norekvål TM, Fridlund B, Rokne B, Segadal L, Wentzel-Larsen T, Nordrehaug JE. Patient-reported outcomes as predictors of 10-year survival in women after acute myocardial infarction. Health Qual Life Outcomes (2010) 8(1):140. doi:10.1186/1477-7525-8-140
105. Berkman L, Breslow L. Health and Ways of Living: The Alameda County Study. New York: Oxford University Press (1983).
106. Brook RH, Ware JE Jr, Davies-Avery A, Stewart AL, Donald CA, Rogers WH, et al. Overview of adult health measures fielded in Rand’s health insurance study. Med Care (1979) 17(7 Suppl):iii–x,1–131.
107. Tarlov AR, Ware JE Jr, Greenfield S, Nelson EC, Perrin E, Zubkoff M. The Medical Outcomes Study. An application of methods for monitoring the results of medical care. JAMA (1989) 262(7):925–30. doi:10.1001/jama.1989.03430070073033
108. Pais-Ribeiro JL. Quality of life is a primary end-point in clinical settings. Clin Nutr (2004) 23(1):121–30. doi:10.1016/S0261-5614(03)00109-2
109. Group W. Development of the WHOQOL: rationale and current status. Int J Ment Health (1994) 23(3):24–56. doi:10.1080/00207411.1994.11449286
110. Revicki DA, Osoba D, Fairclough D, Barofsky I, Berzon R, Leidy NK, et al. Recommendations on health-related quality of life research to support labeling and promotional claims in the United States. Qual Life Res (2000) 9(8):887–900. doi:10.1023/A:1008996223999
111. Sprangers MA, Sloan JA, Barsevick A, Chauhan C, Dueck AC, Raat H, et al. Scientific imperatives, clinical implications, and theoretical underpinnings for the investigation of the relationship between genetic variables and patient-reported quality-of-life outcomes. Qual Life Res (2010) 19(10):1395–403. doi:10.1007/s11136-010-9759-5
112. Halyard MY. The use of real-time patient-reported outcomes and quality-of-life data in oncology clinical practice. Expert Rev Pharmacoecon Outcomes Res (2011) 11(5):561–70. doi:10.1586/erp.11.62
113. Leplege A, Hunt S. The problem of quality of life in medicine. JAMA (1997) 278(1):47–50. doi:10.1001/jama.278.1.47
114. Acquadro C, Berzon R, Dubois D, Leidy NK, Marquis P, Revicki D, et al. Incorporating the patient’s perspective into drug development and communication: an Ad Hoc Task Force Report of the patient-reported outcomes (PRO) harmonization group meeting at the Food and Drug Administration, February 16, 2001. Value Health (2003) 6:522–31. doi:10.1046/j.1524-4733.2003.65309.x
115. Cella D, Riley W, Stone A, Rothrock N, Reeve B, Yount S, et al. The patient-reported outcomes measurement information system (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. J Clin Epidemiol (2010) 63(11):1179–94. doi:10.1016/j.jclinepi.2010.04.011
116. Nelson EC, Eftimovska E, Lind C, Hager A, Wasson JH, Lindblad S. Patient reported outcome measures in practice. Br Med J (2015) 350:g7818. doi:10.1136/bmj.g7818
118. Black N, Varaganum M, Hutchings A. Relationship between patient reported experience (PREMs) and patient reported outcomes (PROMs) in elective surgery. BMJ Qual Saf (2014) 23(7):534. doi:10.1136/bmjqs-2013-002707
119. Miller D, Steele Gray C, Kuluski K, Cott C. Patient-centered care and patient-reported measures: let’s look before we leap. The Patient (2015) 8(4):293–9. doi:10.1007/s40271-014-0095-7
120. Lyu H, Wick EC, Housman M, Freischlag JA, Makary MA. Patient satisfaction as a possible indicator of quality surgical care. JAMA Surg (2013) 148(4):362–7. doi:10.1001/2013.jamasurg.270
121. Groene O, Arah OA, Klazinga NS, Wagner C, Bartels PD, Kristensen S, et al. Patient experience shows little relationship with hospital quality management strategies. PLoS One (2015) 10(7):e0131805. doi:10.1371/journal.pone.0131805
122. Wennmacker S, Lamberts M, Gerritsen J, Roukema JA, Westert G, Drenth J, et al. Consistency of patient-reported outcomes after cholecystectomy and their implications on current surgical practice: a prospective multicenter cohort study. Surg Endosc (2017) 31(1):215–24. doi:10.1007/s00464-016-4959-x
123. Basch E, Deal AM, Dueck AC, Scher HI, Kris MG, Hudis C, et al. Overall survival results of a trial assessing patient-reported outcomes for symptom monitoring during routine cancer treatment. JAMA (2017) 318(2):197–8. doi:10.1001/jama.2017.7156
124. US Department of Health and Human Services; Food and Drug Administration; Center for Drug evaluation and Research; Center for Biologics Evaluation and Research; Center for Devices and Radiological Health. Guidance for industry—patient reported outcome measures: use in medical product development to support labelling claims. Health Qual Life Outcomes (2009) 4:79.
125. Barotfi S, Molnar MZ, Almasi C, Kovacs AZ, Remport A, Szeifert L, et al. Validation of the Kidney Disease Quality of Life-Short Form questionnaire in kidney transplant patients. J Psychosom Res (2006) 60(5):495–504. doi:10.1016/j.jpsychores.2005.09.009
126. Hays RD. Kidney Disease Quality of Life Short Form (KDQOL-SF™), Version 1.3: A Manual for Use and Scoring. Santa Monica, CA: RAND (1997).
127. Gibbons E, Fitzpatrick R. A Structured Review of Patient Reported Outcome Measures for Adults with Chronic Kidney Disease. Oxford, United Kingdom: University of Oxford (2010).
128. Chen T-H, Li L, Kochen MM. A systematic review: how to choose appropriate health-related quality of life (HRQOL) measures in routine general practice? J Zhejiang Univ Sci B (2005) 6(9):936–40. doi:10.1631/jzus.2005.B0936
129. Coons SJ, Rao S, Keininger DL, Hays RD. A comparative review of generic quality-of-life instruments. Pharmacoeconomics (2000) 17(1):13–35. doi:10.2165/00019053-200017010-00002
130. Dempster M, Donnelly M. Selecting a measure of health related quality of life. Soc Work Health Care (2001) 32(1):45–56. doi:10.1300/J010v32n01_04
131. Lim CR, Harris K, Dawson J, Beard DJ, Fitzpatrick R, Price AJ. Floor and ceiling effects in the OHS: an analysis of the NHS PROMs data set. BMJ Open (2015) 5(7). doi:10.1136/bmjopen-2015-007765
132. Erez G, Selman L, Murtagh FEM. Measuring health-related quality of life in patients with conservatively managed stage 5 chronic kidney disease: limitations of the Medical Outcomes Study Short Form 36: SF-36. Qual Life Res (2016) 25(11):2799–809. doi:10.1007/s11136-016-1313-7
133. Chang TI, Tamura MK. Chapter 35: Methods to Assess Quality of Life and Functional Status and Their Applications in Clinical Care in Elderly Patients with CKD. Palo Alto, California: American Society of Nephrology (2009).
134. Testa MA, Simonson DC. Assessment of quality-of-life outcomes. N Engl J Med (1996) 334(13):835–40. doi:10.1056/NEJM199603283341306
135. Martin ML, Patrick DL, Gandra SR, Bennett AV, Leidy NK, Nissenson AR, et al. Content validation of two SF-36 subscales for use in type 2 diabetes and non-dialysis chronic kidney disease-related anemia. Qual Life Res (2011) 20(6):889–901. doi:10.1007/s11136-010-9812-4
136. Ricardo AC, Hacker E, Lora CM, Ackerson L, DeSalvo KB, Go A, et al. Validation of the kidney disease quality of life short form 36 (KDQOL-36™) US Spanish and English versions in a cohort of hispanics with chronic kidney disease. Ethn Dis (2013) 23(2):202–9.
137. Clifton JC, Finley RJ, Gelfand G, Graham AJ, Inculet R, Malthaner R, et al. Development and validation of a disease-specific quality of life questionnaire (EQOL) for potentially curable patients with carcinoma of the esophagus. Dis Esophagus (2007) 20(3):191–201. doi:10.1111/j.1442-2050.2007.00669.x
138. Carver DJ, Chapman CA, Thomas VS, Stadnyk KJ, Rockwood K. Validity and reliability of the Medical Outcomes Study Short Form-20 questionnaire as a measure of quality of life in elderly people living at home. Age Ageing (1999) 28(2):169–74. doi:10.1093/ageing/28.2.169
139. Gandek B, Ware JE, Aaronson NK, Apolone G, Bjorner JB, Brazier JE, et al. Cross-validation of item selection and scoring for the SF-12 health survey in nine countries. J Clin Epidemiol (1998) 51(11):1171–8. doi:10.1016/S0895-4356(98)00109-7
140. Kaplan RM, Sieber WJ, Ganiats TG. The quality of well-being scale: comparison of the interviewer-administered version with a self-administered questionnaire. Psychol Health (1997) 12(6):783–91. doi:10.1080/08870449708406739
141. Cetingok M, Hathaway DK, Winsett RR. Differences in quality of life before transplantation among transplant recipients with respect to selected socioeconomic variables. Prog Trans (2005) 15(4):338–44. doi:10.7182/prtr.15.4.9721717571731234
142. Bergner M, Bobbitt RA, Pollard WE, Martin DP, Gilson BS. The sickness impact profile: validation of a health status measure. Med Care (1976) 14(1):57–67. doi:10.1097/00005650-197601000-00006
143. Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res (2011) 20(10):1727–36. doi:10.1007/s11136-011-9903-x
144. Johnson JA, Coons SJ, Ergo A, Szava-Kovats G. Valuation of EuroQOL (EQ-5D) health states in an adult US sample. Pharmacoeconomics (1998) 13(4):421–33. doi:10.2165/00019053-199813040-00005
145. Skevington SM, Lotfy M, O’Connell KA. The World Health Organization’s WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res (2004) 13:299–310. doi:10.1023/B:QURE.0000018486.91360.00
146. The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol Med (1998) 28(3):551–8. doi:10.1017/S0033291798006667
147. Fong E, Bargman JM, Chan CT. Cross-sectional comparison of quality of life and illness intrusiveness in patients who are treated with nocturnal home hemodialysis versus peritoneal dialysis. Clin J Am Soc Nephrol (2007) 2(6):1195–200. doi:10.2215/CJN.02260507
148. Devins GM, Binik YM, Hutchinson TA, Hollomby DJ, Barré PE, Guttmann RD. The emotional impact of end-stage renal disease: importance of patients’ perceptions of intrusiveness and control. Int J Psychiatry Med (1984) 13(4):327–43. doi:10.2190/5DCP-25BV-U1G9-9G7C
149. Devins GM, Dion R, Pelletier LG, Shapiro CM, Abbey S, Raiz LR, et al. Structure of lifestyle disruptions in chronic disease: a confirmatory factor analysis of the Illness Intrusiveness Ratings Scale. Med Care (2001) 39(10):1097–104. doi:10.1097/00005650-200110000-00007
150. Watnick S, Wang PL, Demadura T, Ganzini L. Validation of 2 depression screening tools in dialysis patients. Am J Kidney Dis (2005) 46(5):919–24. doi:10.1053/j.ajkd.2005.08.006
151. Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA (1999) 282(18):1737–44. doi:10.1001/jama.282.18.1737
152. Wright P, Smith AB, Keding A, Velikova G. The Social Difficulties Inventory (SDI): development of subscales and scoring guidance for staff. Psychooncology (2011) 20(1):36–43. doi:10.1002/pon.1705
153. Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med (2006) 166(10):1092–7. doi:10.1001/archinte.166.10.1092
154. Davison SN, Jhangri GS, Johnson JA. Cross-sectional validity of a modified Edmonton symptom assessment system in dialysis patients: a simple assessment of symptom burden. Kidney Int (2006) 69(9):1621–5. doi:10.1038/sj.ki.5000184
155. Bruera E, Kuehn N, Miller MJ, Selmser P, Macmillan K. The Edmonton Symptom Assessment System (ESAS): a simple method for the assessment of palliative care patients. J Palliat Care (1991) 7(2):6–9.
156. Watanabe SM, Nekolaichuk C, Beaumont C, Johnson L, Myers J, Strasser F. A multicenter study comparing two numerical versions of the Edmonton Symptom Assessment System in palliative care patients. J Pain Symptom Manage (2011) 41(2):456–68. doi:10.1016/j.jpainsymman.2010.04.020
157. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep (1991) 14(6):540–5. doi:10.1093/sleep/14.6.540
158. Allen RP, Burchell BJ, MacDonald B, Hening WA, Earley CJ. Validation of the self-completed Cambridge-Hopkins questionnaire (CH-RLSq) for ascertainment of restless legs syndrome (RLS) in a population survey. Sleep Med (2009) 10(10):1097–100. doi:10.1016/j.sleep.2008.10.007
159. Joshi VD. Quality of life in end stage renal disease patients. World J Nephrol (2014) 3(4):308–16. doi:10.5527/wjn.v3.i4.308
160. Davison SN, Jhangri GS, Feeny DH. Comparing the health utilities index mark 3 (HUI3) with the short form-36 preference-based SF-6D in chronic kidney disease. Value Health (2009) 12(2):340–5. doi:10.1111/j.1524-4733.2008.00433.x
161. Devins GM. Using the illness intrusiveness ratings scale to understand health-related quality of life in chronic disease. J Psychosom Res (2010) 68(6):591–602. doi:10.1016/j.jpsychores.2009.05.006
162. Bastien CH, Vallieres A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med (2001) 2(4):297–307. doi:10.1016/S1389-9457(00)00065-4
163. Yellen SB, Cella DF, Webster K, Blendowski C, Kaplan E. Measuring fatigue and other anemia-related symptoms with the functional assessment of cancer therapy (FACT) measurement system. J Pain Symptom Manage (1997) 13(2):63–74. doi:10.1016/S0885-3924(96)00274-6
164. Hays RD. The Medical Outcomes Study (MOS) Measures of Patient Adherence. Santa Monica, California: The RAND Corporation (Vol. 19). (1994). 2004 p.
165. Ferrans CE, Powers MJ. Quality of life index: development and psychometric properties. Adv Nurs Sci (1985) 8(1):15–24. doi:10.1097/00012272-198510000-00005
166. Ferrans CE, Powers MJ. Psychometric assessment of the quality of life index. Res Nurs Health (1992) 15(1):29–38. doi:10.1002/nur.4770150106
167. Laupacis A, Muirhead N, Keown P, Wong C. A disease-specific questionnaire for assessing quality of life in patients on hemodialysis. Nephron (1992) 60(3):302–6. doi:10.1159/000186769
168. Laupacis A, Pus N, Muirhead N, Wong C, Ferguson B, Keown P. Disease-specific questionnaire for patients with a renal transplant. Nephron (1993) 64(2):226–31. doi:10.1159/000187318
169. Salek S. Quality of life in patients with end-stage renal disease. J Appl Therap (1999) 2:163–70.
170. Wu AW, Fink NE, Cagney KA, Bass EB, Rubin HR, Meyer KB, et al. Developing a health-related quality-of-life measure for end-stage renal disease: the CHOICE Health Experience Questionnaire. Am J Kidney Dis (2001) 37(1):11–21. doi:10.1053/ajkd.2001.20631
171. Franke GH, Reimer J, Kohnle M, Luetkes P, Maehner N, Heemann U. Quality of life in end-stage renal disease patients after successful kidney transplantation: development of the ESRD symptom checklist—transplantation module. Nephron (1999) 83(1):31–9. doi:10.1159/000045470
172. Devins GM, Binik YM, Mandin H, Letourneau PK, Hollomby DJ, Barre PE, et al. The Kidney Disease Questionnaire: a test for measuring patient knowledge about end-stage renal disease. J Clin Epidemiol (1990) 43(3):297–307. doi:10.1016/0895-4356(90)90010-M
173. Chisholm-Burns MA, Erickson SR, Spivey CA, Gruessner RWG, Kaplan B. Concurrent validity of kidney transplant questionnaire in US renal transplant recipients. Patient Prefer Adherence (2011) 5:517–22. doi:10.2147/PPA.S24261
174. Bradley C. Design of a renal-dependent individualized quality of life questionnaire. Adv Perit Dial (1997) 13:116–20.
175. Weisbord SD, Fried LF, Arnold RM, Fine MJ, Levenson DJ, Peterson RA, et al. Prevalence, severity, and importance of physical and emotional symptoms in chronic hemodialysis patients. J Am Soc Nephrol (2005) 16(8):2487–94. doi:10.1681/ASN.2005020157
176. Antunes B, Harding R, Higginson IJ. Implementing patient-reported outcome measures in palliative care clinical practice: a systematic review of facilitators and barriers. Palliat Med (2013) 28(2):158–75. doi:10.1177/0269216313491619
177. Wangnoo SK, Sethi B, Sahay RK, John M, Ghosal S, Sharma SK. Treat-to-target trials in diabetes. Indian J Endocrinol Metab (2014) 18(2):166–74. doi:10.4103/2230-8210.129106
178. Solomon DH, Bitton A, Katz JN, Radner H, Brown E, Fraenkel L. Treat to target in rheumatoid arthritis: fact, fiction or hypothesis? Arthritis Rheumatol (2014) 66(4):775–82. doi:10.1002/art.38323
179. Gill TM, Feinsten AR. A critical appraisal of the quality of quality-of-life measurements. JAMA (1994) 272(8):619–26. doi:10.1001/jama.272.8.619
180. Kimmel PL. Just whose quality of life is it anyway? Controversies and consistencies in measurements of quality of life. Kidney Int (2000) 57:S113–20. doi:10.1046/j.1523-1755.2000.07419.x
181. Karimi M, Brazier J. Health, health-related quality of life, and quality of life: what is the difference? Pharmacoeconomics (2016) 34(7):645–9. doi:10.1007/s40273-016-0389-9
182. Hvitfeldt H, Carli C, Nelson EC, Mortenson DM, Ruppert BA, Lindblad S. Feed forward systems for patient participation and provider support: adoption results from the original US context to Sweden and beyond. Qual Manag Health Care (2009) 18(4):247–56. doi:10.1097/QMH.0b013e3181bee32e
183. Schorn MM, Doorenbos AZ, Gordon D, Read-Williams P. Survey of primary-care providers on perceived benefits of and barriers to pain tracker. J Nurse Pract (2014) 10(10):781–6. doi:10.1016/j.nurpra.2014.08.003
184. Gerber Y, Benyamini Y, Goldbourt U, Drory Y. Prognostic importance and long-term determinants of self-rated health after initial acute myocardial infarction. Med Care (2009) 47:342–9. doi:10.1097/MLR.0b013e3181894270
185. Narita I, Alchi B, Omori K, Sato F, Ajiro J, Saga D, et al. Etiology and prognostic significance of severe uremic pruritus in chronic hemodialysis patients. Kidney Int (2006) 69(9):1626–32. doi:10.1038/sj.ki.5000251
186. van Melle JP, de Jonge P, Spijkerman TA, Tijssen JG, Ormel J, van Veldhuisen DJ, et al. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: a meta-analysis. Psychosom Med (2004) 66:814–22. doi:10.1097/01.psy.0000146294.82810.9c
187. Kluetz PG, Chingos DT, Basch EM, Mitchell SA. Patient-reported outcomes in cancer clinical trials: measuring symptomatic adverse events with the National Cancer Institute’s patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). Am Soc Clin Oncol Educ Book (2016) 35:67–73. doi:10.14694/EDBK_159514
Keywords: patient-reported outcomes, chronic kidney disease, kidney transplantation, renal transplantation, patient-reported outcome measures, quality of life measurement, quality of life
Citation: Tang E, Bansal A, Novak M and Mucsi I (2018) Patient-Reported Outcomes in Patients with Chronic Kidney Disease and Kidney Transplant—Part 1. Front. Med. 4:254. doi: 10.3389/fmed.2017.00254
Received: 29 September 2017; Accepted: 21 December 2017;
Published: 15 January 2018
Edited by:
Howard Trachtman, New York University, United StatesReviewed by:
Maria-Eleni Roumelioti, University of New Mexico, United StatesKirk Campbell, Icahn School of Medicine at Mount Sinai, United States
Copyright: © 2018 Tang, Bansal, Novak and Mucsi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Istvan Mucsi, istvan.mucsi@utoronto.ca
†These authors have contributed equally to this work.