 Alexandra S. Simões1*
Alexandra S. Simões1* Isabel Couto1
Isabel Couto1 Cristina Toscano2,3
Cristina Toscano2,3 Elsa Gonçalves2,3
Elsa Gonçalves2,3 Pedro Póvoa3,4
Pedro Póvoa3,4 Miguel Viveiros1
Miguel Viveiros1 Luís V. Lapão1,5
Luís V. Lapão1,5- 1Global Health and Tropical Medicine, Instituto de Higiene e Medicina Tropical, Universidade Nova de Lisboa, Lisbon, Portugal
- 2Laboratório de Microbiologia Clínica e Biologia Molecular, Serviço de Patologia Clínica, Hospital de Egas Moniz, Centro Hospitalar de Lisboa Ocidental, Lisbon, Portugal
- 3Centro de Estudos de Doenças Crónicas, NOVA Medical School/Faculdade de Ciências Médicas, Universidade Nova de Lisboa, Lisbon, Portugal
- 4Unidade de Cuidados Intensivos Polivalente, Hospital de São Francisco Xavier, Centro Hospitalar de Lisboa Ocidental, Lisbon, Portugal
- 5WHO Collaborating Center for Health Workforce Policy and Planning, Instituto de Higiene e Medicina Tropical, Universidade Nova de Lisboa, Lisbon, Portugal
In Europe, each year, more than four milion patients acquire a healthcare-associated infection (HAI) and almost 40 thousand die as a direct consequence of it. Regardless of many stategies to prevent and control HAIs, they remain an important cause of morbidity and mortality worldwide with a significant economic impact: a recent estimate places it at the ten billion dollars/year. The control of HAIs requires a prompt and efficient identification of the etiological agent and a rapid communication with the clinician. The Microbiology Laboratory has a significant role in the prevention and control of these infections and is a key element of any Infection Control Program. The work of the Microbiology Laboratory covers microbial isolation and identification, determination of antimicrobial susceptibility patterns, epidemiological surveillance and outbreak detection, education, and report of quality assured results. In this paper we address the role and importance of the Microbiology Laboratory in the prevention and control of HAI and in Antibiotic Stewardship Programs and how it can be leveraged when combined with the use of information systems. Additionally, we critically review some challenges that the Microbiology Laboratory has to deal with, including the selection of analytic methods and the proper use of communication channels with other healthcare services.
Introdution
Healthcare-associated infections (HAIs) are a significant cause of morbidity and mortality leading to 37,000 deaths/year in Europe1 and 75,000 deaths in USA in 2011 (Magill et al., 2014). The HAIs economic impact is also significant: about 9.8 billion dollars/year/USA for the five major infections (Zimlichman et al., 2013). Antibiotic resistance is one of the major problems associated with HAIs (Cosgrove, 2006; Neidell et al., 2012): the Centers for Disease Prevention and Control (CDC) estimates that over two million people/year acquire antibiotic resistant infections, and 23,000 die as a result of it (CDC, 2013). In Europe, 25,000 people/year die with drug-resistant infections (ECDC, 2009).
Prevention through education is the most used strategy for HAIs control: the benefits from prevention can be as high as 5.5 billion dollars (Zimlichman et al., 2013). Reinforcing hand washing, staff education, environmental cleaning practices, Antibiotic Stewardship Programs (ASPs) and improved communication systems are measures implemented worldwide to control HAIs. However, to efficiently control HAIs, clinicians need to act quickly, which implies gathering all relevant information about the infection as soon as possible. That is why the Microbiology Laboratory is so important in HAIs prevention and control since it is in the front line for the early identification of infection, characterization of antibiotic resistance patterns and recognition of outbreaks (Diekema and Saubolle, 2011; Davey et al., 2013).
Traditionally, the tasks of the Microbiology Laboratory are to isolate, identify and determine antibiotic susceptibility patterns of pathogens (Wilson and Spencer, 1999). However, its scope covers other areas that are critical for Infection Control Programs as well as to ASPs, which should ideally include a member of the Microbiology Laboratory staff (Kolmos, 1999; Benbachir, 2008; CDC, 2014). The success of these kind of programs depends largely on the active involvement of the Microbiology Laboratory in activities beyond the regular microbiology exams, namely in results report, surveillance, communication, and other daily routine tasks of Infection Control Teams (Kalenić and Budimir, 2009).
In this paper, we describe the multiple chores of the Microbiology Laboratory highlighting its importance in HAIs prevention and control, and in ASPs, especially when combined with properly designed information systems. We also review some of the problems that the Microbiology Laboratory has to deal with when assisting Infection Control Teams, including the selection of the most appropriate analytic methods to provide fast and accurate results.
Tasks of the Microbiology Laboratory
Microbial Isolation and Identification
The Microbiology Laboratory main task is to isolate and identify the infection etiological agent (Benbachir, 2008), using the most appropriate, rapid and accurate diagnostic method. To ensure this, the Microbiology Laboratory needs to keep up-to-date materials, culture media, reagents, equipment, identification methods and trained personnel (CDC, 2003). The staff needs continuous on-the-job training in microbiological techniques and to be updated on the internationally endorsed methods for isolation and characterization of pathogens (Pfaller and Herwaldt, 1997; Benbachir, 2008). In addition, external and internal quality control and assurance programs must be implemented to guarantee the quality of the results (Benbachir, 2008).
Determination of Antimicrobial Susceptibility Patterns
The Microbiology Laboratory should provide frequently updated information on antimicrobial resistance patterns, essential to design appropriate hospital prescription guidelines, help clinicians to choose the most appropriate empiric therapy and to create a culture of patient safety (Pfaller and Herwaldt, 1997; Benbachir, 2008). This data can be analyzed in different perspectives, including infectious agent, specimen, ward, clinical specialty, antibiotics prescribed, or anatomic site of infection, among others (Pfaller and Herwaldt, 1997; Benbachir, 2008).
The availability of periodic reports on local antimicrobial resistance patterns is also relevant in ASPs, since it can be used to evaluate trends of antimicrobial resistance rates, to educate clinicians on optimal antimicrobial use and to assess the impact of prevention measures (Diekema and Saubolle, 2011).
Report of the Results
The laboratory work is completed only when it is effectively reported (Newton and Novak-Weekley, 2011). All laboratory results (preliminary and final) should be reported as soon as possible to clinicians and Infection Control Teams (Kalenić and Budimir, 2009). Daily reports on significant microbiology results and periodic reports with frequency of isolated pathogens and prevalence of resistant microorganisms provide clinicians and Infection Control Teams with accurate and timely information, essential to follow trends of hospital infections and control urgent situations (Pfaller and Herwaldt, 1997; Benbachir, 2008).
These reports can be delivered through meetings, phone, information systems alerts, paper, or e-mail. However, making results accessible through an information system is an advantage by ensuring that all results are available in an organized, easily accessible, and timely manner, and also permits links to other surveillance data systems (Cantón, 2005). Information systems that incorporate information about the patient, disease, infectious agent and antimicrobial susceptibility are fundamental because they promote timely exchange of information between healthcare workers (Schreckenberger and Binnicker, 2011). For instance, ARTEMIS (Teodoro et al., 2012) and HAITool (Pinto et al., 2016) are good examples of this kind of systems. They analyze heterogeneous data sources and can be used to build antimicrobial resistance surveillance networks participating in the management and prevention of antibiotic resistant HAIs, and by doing so, optimizing human and economic resources2 (Teodoro et al., 2012). Some of these systems alert the clinician (or the pharmacist) when laboratory results reveal that the antibiotic(s) in use may not be optimal or when de-escalation treatment is indicated (Schreckenberger and Binnicker, 2011; Pinto et al., 2016). The “processed information” generated by these systems are very useful for surveillance purposes and in supporting and leveraging ASPs (Davey et al., 2013).
Surveillance and Outbreak Detection
Surveillance enables the identification of infected patients, the origin of HAIs and to understand their paths of spread. Since most of this data comes from microbiological isolates and other laboratory identification tests (Emori and Gaynes, 1993; Peterson and Brossette, 2002), the Microbiology Laboratory has a central role not only on the surveillance and early detection of outbreaks but also on monitoring and reporting unusual laboratory results (e.g., clusters of pathogens, emergence of multidrug-resistant organisms, isolation of unusual pathogens).
To detect outbreaks early enough to mitigate their impact on morbidity and mortality is one of the major challenges of an efficient surveillance program (Diekema and Saubolle, 2011). The Microbiology Laboratory, in association with the Infections Control Team, is the first to detect an outbreak because unusual clusters of pathogens or resistance patterns are easily noticed (Arias, 2010). During an outbreak, these two entities have to work side by side to: (i) provide information on the epidemiology of the etiologic agent; (ii) identify and store the isolates involved for further testing; (iii) define/select appropriate selective isolation media and drug susceptibility testing (if needed/when applicable); (iv) perform the appropriate tests for strain typing (or provide its dispatch to a reference laboratory); (v) and perform supplemental microbiological surveillance of patients, personnel, or environmental sources of infection (Emori and Gaynes, 1993; Pfaller and Herwaldt, 1997; Arias, 2010).
As described above, the use of surveillance systems can enhance surveillance programs by aggregating all the information related with patient, disease, infectious agent and antimicrobial susceptibility, making easier outbreaks detection.
Education
To maximize the efficacy of Infection Control programs, the Microbiology Laboratory should provide training and information on basic microbiology and biosafety for healthcare workers in areas such as: specimen collection, handling and transport, epidemiologically important pathogens vs. normal flora, colonization vs. infection, interpretation of microbiological results (Kalenić and Budimir, 2009). Written guidelines about sampling, handling and transport should be available in every ward, which can also include details on the tests available for proper isolation, identification, and typing of microorganisms (Grosek, 1999).
Antibiotic Stewardship Programs
Antibiotic Stewardship Programss should be included in all HAIs prevention and control programs and are essential for gathering information about epidemiological and molecular markers of resistance, and changes in resistance patterns. They not only contribute to the optimization of antimicrobial therapy, by ensuring proper use (indication, dose, route of administration, and duration) and minimizing side effects, but also promote education on it (Davey et al., 2013). The adoption of these programs leads to a reduction in the prevalence of antimicrobial resistance and costs (Malani et al., 2012). These programs have been implemented throughout the world and there are guidelines and recommendations for their use in the USA (CDC, 2014; Fridkin et al., 2014) and Europe (Pina, 2002; Department of Health Advisory Committee on Antimicrobial Resistance and Healthcare Associated Infection, 2011; Lower et al., 2013; Simões et al., 2015).
Also here, computerized surveillance and decision support systems are a good support for ASPs, since have proven to be effective in the prescription errors reduction, medical care improvement and compliance with recommendations (Evans et al., 1998; Pestotnik, 2005).
A schematic representation of the network of interactions in ASPs is shown in Figure 1. The laboratory imparts an important function in ASPs, generating most of the relevant information needed to characterize the biology of the pathogen (and the hosts), namely its identification, antimicrobial susceptibility patterns and epidemiological connections. Therefore, it is recommended that all ASPs include a microbiologist (CDC, 2014). A good example of the role of Microbiology Laboratory in ASPs is described by MacKenzie et al. (2007) who demonstrated that hospitals with routine reports on antimicrobial susceptibility patterns for restricted antibiotics had lower usage (and misusage) of these antibiotics.
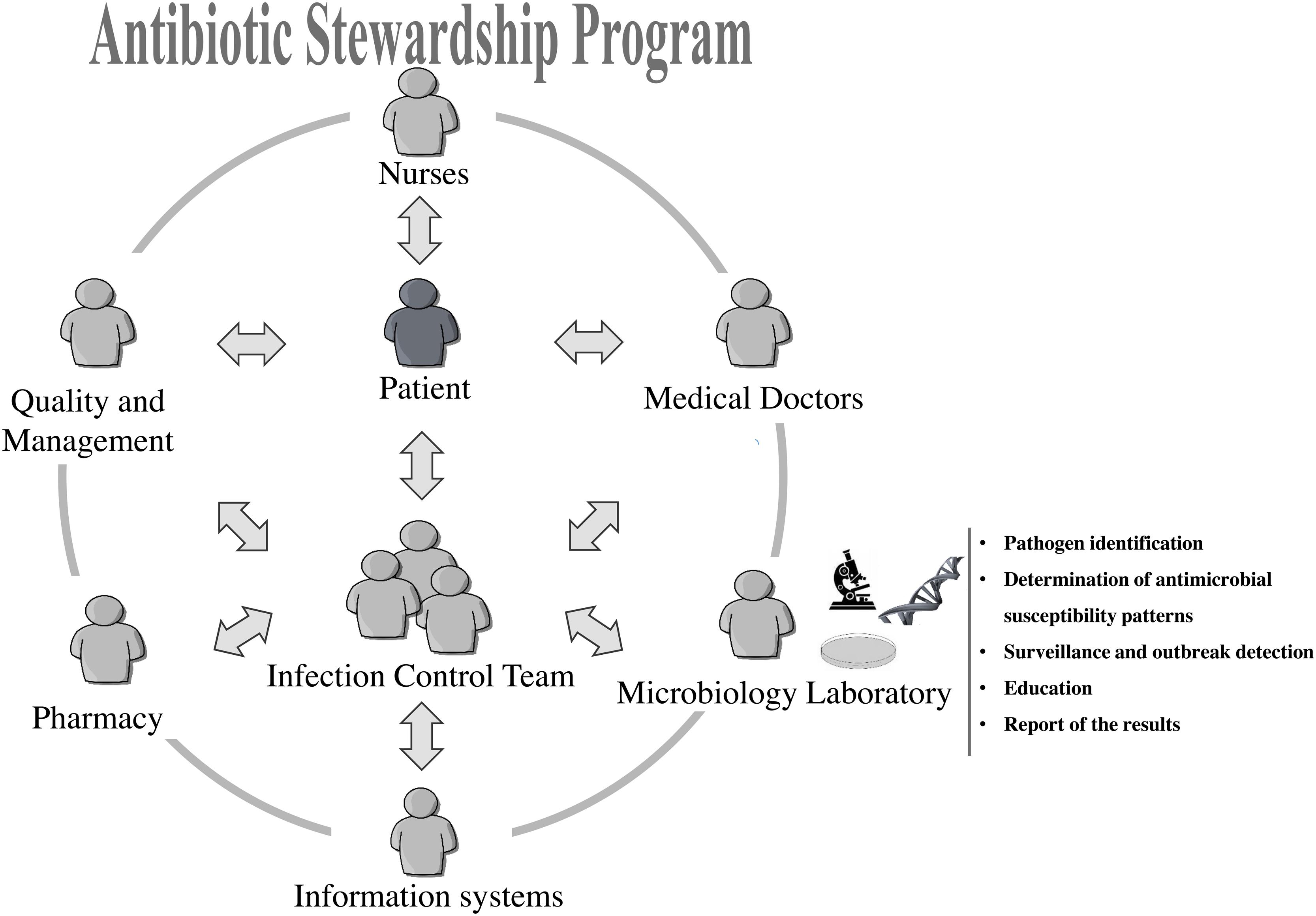
FIGURE 1. Network of interactions in an Antibiotic Stewardship Program.
Issues on the Laboratory Efficacy
Sample’s Quality and Access to Clinical Data
The quality of the laboratory diagnosis is closely related with the quality of the collected samples (Benbachir, 2008). Samples should be taken on the correct time and from appropriate sites, using proper techniques and in amounts that makes possible to perform all the tests necessary for the isolation and identification (and other testing) of the pathogen (Department of Health Advisory Committee on Antimicrobial Resistance and Healthcare Associated Infection, 2011). Samples that are not properly collected and transported may lead to false results (Benbachir, 2008).
Relevant epidemiological and clinical information data are also important for accurate laboratory diagnosis. Every request for exam should include: name of the patient, name of the clinician in charge, location of the patient, date and time of specimen collection, short anamnesis including suspected diagnosis and underlying patient conditions and comorbidities (Benbachir, 2008; Kalenić and Budimir, 2009). The access to this pre-analytic data facilitates significantly the guidance toward pathogen detection and identification. These kind of information should be easily accessed throughout an information system.
Isolation in Culture or Molecular Identification Methods, Which One to Choose?
The use of laboratory culture methods for isolation of pathogens followed by identification procedures (biochemical, molecular, serologic, or other) has been the gold standard in Medical Microbiology and continues to play a vital role in the overall management of infectious diseases. As an example, blood culture is still mandatory for isolation and identification of blood pathogens and guiding therapy (Book et al., 2013). However, isolation in culture has limitations, namely being time consuming (Singh et al., 2006). Results provided 48 to 72 h after the onset of the infection often have limited impact on therapy (Tenover, 2010) and the ability of the laboratory to provide results in a timely manner is essential.
Conversely, the major benefit of direct molecular methods is related to time saving. Using Polymerase Chain Reaction (PCR) based methods, results can be obtained within 6 to 8 h, reducing greatly the time-to-result and implementation of appropriate therapy (Book et al., 2013). Molecular methods have been described as a powerful tool against the spread of microorganisms in hospital environment, in particular during outbreaks (Singh et al., 2006), and many have been used to rapidly identify microorganisms (e.g., multiplex PCR, Real-time PCR, MALDI-TOF MS), to find resistance patterns (e.g., PCR/hybridization screening of resistance determinants) and to estimate epidemiological links between bacteria (e.g., pulsed-field gel electrophoresis, multi-locus sequence typing), enabling rapid and appropriate therapeutic responses (Cantón, 2005; Simões et al., 2011; Sabat et al., 2013; Patel, 2015; Srinivasan et al., 2015). More recently whole-genome sequencing (WGS) promises to transform Infection Control. WGS provides almost all the genetic information needed for epidemiological studies (Köser et al., 2012) and has been widely used to identify and control outbreaks of antibiotic resistant HAIs (Reuter et al., 2013; Price et al., 2013). WGS can be used to quickly identify pathogenic agents from specimens and unravel many genomic single nucleotide polymorphisms and markers for drug resistance, allowing the implementation of immediate and appropriate control measures (Coll et al., 2014). However, the translation of the large amount of data generated by WGS to the clinical utility is still under development (Burke and Korngiebel, 2015).
Molecular methods have been associated with global cost reduction, due to their high specificity, sensitivity and rapid turnaround (Cantón, 2005; Tenover, 2010; Currie, 2011). Combining molecular typing with surveillance programs was shown to be cost effective and result in significant reduction of HAIs rates (Hacek et al., 1999). More recently, the integration of rapid identifications methods with stewardship interventions has been described as a way to improve time to optimal antibiotic therapy, decrease length of hospital stay and reduce mortality and healthcare costs (Huang et al., 2013; Bauer et al., 2014; Perez et al., 2014).
However, molecular methods do not solve all the problems. Several authors have described drawbacks associated with molecular methods: limited number of detectable pathogens, possibility of false positives and complex sample preparation procedures (Laxminarayan et al., 2013). In addition, molecular methods are more expensive, require specialized equipment, and training (Morshed et al., 2007) and their value in diagnosis of some infections has not been fully proven. For instance, in a recent study testing the accuracy of SeptiFast multi-pathogens real-time PCR, authors concluded that, despite providing faster results, this method has limited utility in bloodstream infections, when compared with conventional blood culture (Warhurst et al., 2015). Additionally, there are several microorganisms for which isolation by culture methods is the most effective and recommend procedure especially when dealing with drug-resistant inducible geno/phenotypes.
The dispute on isolation in culture followed by identification versus direct identification from specimen by molecular methods seems endless and unnecessary since both methods can be used in concert. Several authors suggested a combination of culture and molecular methods in order to increase the rate, efficacy and accuracy of pathogen detection. (Dolinger and Jacobs, 2011; Brown-Elliott and Wallace, 2012; Huttunen et al., 2013). Table 1 summarizes some pros and cons of both strategies.
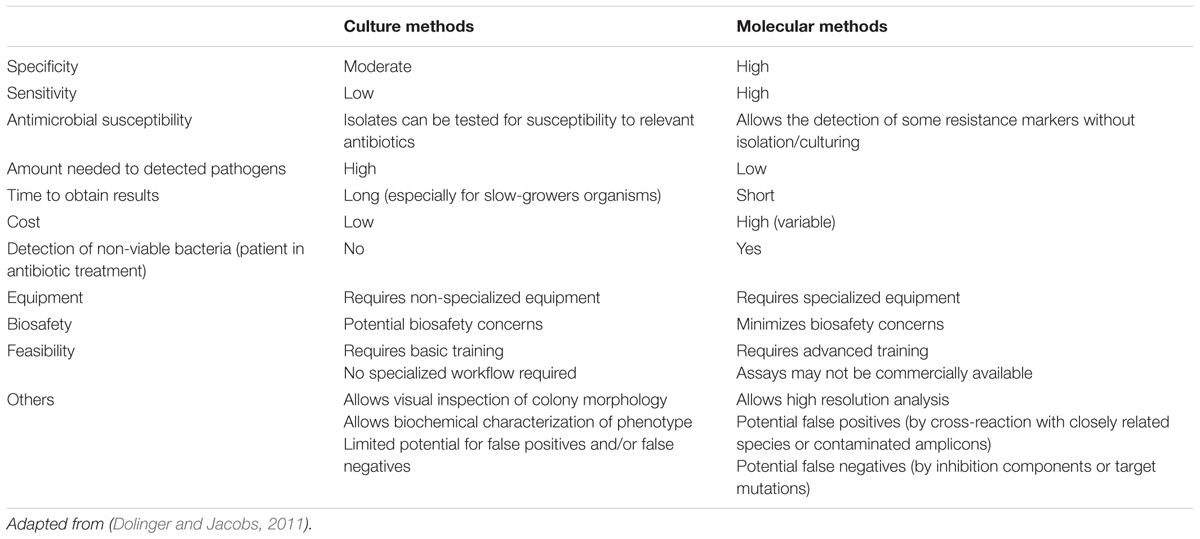
TABLE 1. Comparison of culture and molecular identification methods.
Antimicrobial Resistance Surveillance
With the emergence and spread of antimicrobial resistant pathogens, antimicrobial resistance surveillance is becoming an important task of the Microbiology Laboratory. Antimicrobial resistance surveillance is an ongoing (and organized) data collection that after being analyzed and reported provides useful information for empirical antimicrobial therapy (Cornaglia et al., 2004).
Nevertheless, a good surveillance program is time consuming and involve dedicated human resources. In addition there are several challenges on data collection, management, analysis, interpretation and reporting. For instance, promoting the use of new and low-cost technologies to improve laboratory work and to prioritize which bacteria are most important to track are issues that should be addressed (Solomon and Ijaz, 2015). Regarding interpretation, uniformization is needed: currently, different guidelines and breakpoints for evaluation of antimicrobials susceptibility patterns values are adopted in the United States of America and within several European countries (Vernet et al., 2014). Finally, the results should be presented in formats easily understandable by the clinicians (Grundmann et al., 2011).
Information systems are a good way to keep-it working smoothly (Lapão, 2007). As stated above, surveillance information systems ensure that antimicrobial resistance related data are available and organized, making easy to report it retrospectively. In addition, surveillance information systems allow better antibiotic resistance management and help to provide evidence based results that can be used for the development of control policies (Evans et al., 1998; Pestotnik, 2005).
Communication
Effective communication is critical for the Microbiology Laboratory procedures. Nevertheless, it can also be one of its major issues. Effective communication is the base of a healthy collaboration between laboratory, healthcare workers and Infection Control Teams (Kalenić and Budimir, 2009). The dialog between healthcare workers and laboratory staff must be easy and effective (Peterson et al., 2001). The existence of a dedicated laboratory staff element (privileged interlocutor) and the participation of microbiologists in regular clinician’s meetings is recommended. Efficient communication between clinicians and microbiologists about the presumptive diagnosis, accelerates the diagnosis and avoids problems with inappropriate specimens (Baron et al., 2013).
In order to facilitate communication, it is recommended that the director of the Microbiology Laboratory be a clinician or a laboratory scientist with expertise in infectious diseases and microbiology (Thomson et al., 2010) since their background on disease pathologic process facilitates the discussion of clinical cases. Additionally, information systems have an important role in communication within the hospitals by facilitating the exchange of clinical and microbiological relevant data between clinicians and laboratories (Lapão, 2007). However, it is important that information systems are defined and designed together with the healthcare workers in order to really improve communication, data quality, be useful on decision-making and be easy to use (Pinto et al., 2016).
Another reality that can affect the communication is the location of the Microbiology Laboratory. There are an increasing number of off-site laboratories providing services to hospitals and in the cases of in-house laboratories, they usually are in the basement or in an annex outside the hospital main building. It has been described that off-site laboratories delay and decrease communication, could jeopardizes infection diagnosis and treatment and weaken infection prevention and antibiotic stewardship infrastructures (Peterson et al., 2001; Dancer et al., 2015).
Conclusion
The Microbiology Laboratory plays a key role in HAIs prevention and control. From ensuring appropriate specimen collection and transport, to the wise selection of isolation and identification methods and finally on the antibiotic therapy guidance plus effective report and communication of the results, the laboratory covers all important aspects of infection control process. The microbiologist is a fundamental and enriching member of ASPs and Infection Control Teams. The new identifications methods (including WGS) combined with the emergence of innovative and centralized information systems that integrate the microbiology results with clinical data will revolutionize HAIs prevention and control strategies, help decision-making and resolve some of the difficulties felt by the microbiologists.
Author Contributions
ASS, IC, CT, EG, PP, MV, and LVL contributed to the draft and revision of the paper and approved the final version to be published.
Funding
This work was supported by project “HAITool – A Toolkit to Prevent, Manage and Control Healthcare-Associated Infections in Portugal” EEA Grants, 000182DT3; and by FCT for funds to GHTM – UID/Multi/04413/2013.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
- ^http://ecdc.europa.eu/en/healthtopics/Healthcare-associated_infections
- ^http://haitool.ihmt.unl.pt/
References
Arias, K. M. (2010). “The role of the laboratory in outbreak detection, prevention and investigation,” in Outbreak Investigation, Prevention, and Control in Health Care Settings, Critical Issues in Patient Safety, 2nd Edn, ed. K. M. Arias (Burlington, MA: Jones & Bartlett Learning).
Baron, E. J., Miller, J. M., Weinstein, M. P., Richter, S. S., Gilligan, P. H., Thomson, R. B., et al. (2013). A guide to utilization of the microbiology laboratory for diagnosis of infectious diseases: 2013 recommendations by the infectious diseases society of america (IDSA) and the american society for microbiology (ASM). Clin. Infect. Dis. 57:e22–e121. doi: 10.1093/cid/cit278
Bauer, K. A., Perez, K. K., Forrest, G. N., and Goff, D. A. (2014). Review of rapid diagnostic tests used by antimicrobial stewardship programs. Clin. Infect. Dis. 59(Suppl. 3), S134–S145. doi: 10.1093/cid/ciu547
Benbachir, M. (2008). “Role of the microbiology laboratory in infection control,” in Guide to Infection Control in Hospitals, IV Edn, eds R. Wenzel, G. Bearman, T. Brewer, and J.-P. Butzler (Boston: International Society for Infectious Diseases).
Book, M., Lehmann, L. E., Zhang, X. H., and Stüber, F. (2013). Monitoring infection: from blood culture to polymerase chain reaction (PCR). Best Practice & Research. Clin. Anaesthesiol. 27, 279–288. doi: 10.1016/j.bpa.2013.06.010
Brown-Elliott, B. A., and Wallace, R. J. (2012). Enhancement of conventional phenotypic methods with molecular-based methods for the more definitive identification of nontuberculous Mycobacteria. Clin. Microbiol. Newslett. 34, 109–115. doi: 10.1016/j.clinmicnews.2012.06.004
Burke, W., and Korngiebel, D. M. (2015). Closing the gap between knowledge and clinical application: challenges for genomic translation. Edited by Mildred Cho. PLoS Genet. 11:e1004978. doi: 10.1371/journal.pgen.1004978
Cantón, R. (2005). Role of the microbiology laboratory in infectious disease surveillance, alert and response. Clin. Microbiol. Infect. 11(Suppl. 1), 3–8. doi: 10.1111/j.1469-0691.2005.01081.x
CDC (2003). Manual for the Laboratory Identification and Antimicrobial Susceptibility Testing of Bacterial Pathogens of Public Health Importance in the Developing World. Geneva: World Health Organization.
CDC (2013). Antibiotic Resistance Threats in the United States, 2013 Edn. Atlanta, GA: Centers for Disease Control.
CDC (2014). Core Elements of Hospital Antibiotic Stewardship Programs. Atlanta, GA: Centers for Disease Control. Available at: http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html
Coll, F., McNerney, R., Guerra-Assunção, J. A., Glynn, J. R., Perdigão, J., Viveiros, M., et al. (2014). A Robust SNP barcode for typing Mycobacterium tuberculosis complex strains. Nat. Commun. 5:4812. doi: 10.1038/ncomms5812
Cornaglia, G., Hryniewicz, W., Jarlier, V., Kahlmeter, G., Mittermayer, H., Stratchounski, L., et al. (2004). European recommendations for antimicrobial resistance surveillance. Clin. Microbiol. Infect. 10, 349–383. doi: 10.1111/j.1198-743X.2004.00887.x
Cosgrove, S. E. (2006). The relationship between antimicrobial resistance and patient outcomes: mortality, length of hospital stay, and health care costs. Clin. Infect. Dis. 42(Suppl. 2), S82–S89. doi: 10.1086/499406
Currie, B. (2011). Impact of molecular diagnostics on infection control. Infect. Dis. Special Ed. 9, 11–15.
Dancer, S. J., Varon-Lopez, C., Moncayo, O., Elston, A., and Humphreys, H. (2015). Microbiology service centralization: a step too far. J. Hosp. Infect. 91, 292–298. doi: 10.1016/j.jhin.2015.08.017
Davey, P., Brown, E., Charani, E., Fenelon, L. I, Gould, M., Holmes, A., et al. (2013). Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 4:CD003543. doi: 10.1002/14651858.CD003543.pub3
Department of Health Advisory Committee on Antimicrobial Resistance and Healthcare Associated Infection (ARHAI) (2011). Antimicrobial Stewardship: “Start Smart–Then Focus”: Guidance for Antimicrobial Stewardship in Hospitals. London: Public Health England.
Diekema, D. J., and Saubolle, M. A. (2011). Clinical microbiology and infection prevention. J. Clin. Microbiol. 49, S57–S60. doi: 10.1128/JCM.00690-11
Dolinger, D. L., and Jacobs, A. A. (2011). “Molecular diagnostics and active screening for health care-associated infections: stepping-up the game,” in Laboratory Medicine ed. R. L. Bertholf (Oxford: Oxford University Press).
ECDC (2009). The Bacterial Challenge?: Time to React. Stockholm: European Centre for Disease Prevention and Control.
Emori, T. G., and Gaynes, R. P. (1993). An overview of nosocomial infections, including the role of the microbiology laboratory. Clin. Microbiol. Rev. 6, 428–442. doi: 10.1128/CMR.6.4.428
Evans, R. S., Pestotnik, S. L., Classen, D. C., Clemmer, T. P., Weaver, L. K., Orme, J. F., et al. (1998). A computer-assisted management program for antibiotics and other antiinfective agents. New Engl. J. Med. 338, 232–238. doi: 10.1056/NEJM199801223380406
Fridkin, S., Baggs, J., Fagan, R., Magill, S., Pollack, L. A., Malpiedi, P., et al. (2014). Vital signs: improving antibiotic use among hospitalized patients. Morb Mortal Wkly Rep. 63, 194–200.
Grosek, S. (1999). What does a clinician expect from a microbiologist? Towards an effective joint policy. J. Hosp. Infect. 43. (Suppl.), S293–S296. doi: 10.1016/S0195-6701(99)90102-0
Grundmann, H., Klugman, K. P., Walsh, T., Ramon-Pardo, P., Sigauque, B., Khan, W., et al. (2011). A framework for global surveillance of antibiotic resistance. Drug Resist. Updat. 14, 79–87. doi: 10.1016/j.drup.2011.02.007
Hacek, D. M., Suriano, T., Noskin, G. A., Kruszynski, J., Reisberg, B., and Peterson, L. R. (1999). Medical and economic benefit of a comprehensive infection control program that includes routine determination of microbial clonality. Am. J. Clin. Pathol. 111, 647–654. doi: 10.1093/ajcp/111.5.647
Huang, A. M., Newton, D., Kunapuli, A., Gandhi, T. N., Washer, L. L., Isip, J., et al. (2013). Impact of rapid organism identification via matrix-assisted laser desorption/ionization time-of-flight combined with antimicrobial stewardship team intervention in adult patients with bacteremia and candidemia. Clin. Infect. Dis. 57, 1237–1245. doi: 10.1093/cid/cit498
Huttunen, R., Syrjänen, J., Vuento, R., and Aittoniemi, J. (2013). Current concepts in the diagnosis of blood stream infections. are novel molecular methods useful in clinical practice? Int. J. Infect. Dis. 17, e934–e938. doi: 10.1016/j.ijid.2013.04.018
Kalenić, S., and Budimir, A. (2009). The role of the microbiology laboratory in healthcare-associated infection prevention. Int. J. Infect. Control 60, (Suppl.), S57–S60. doi: 10.3396/ijic.V5i2.014.09
Kolmos, H. J. (1999). Interaction between the microbiology laboratory and clinician: what the microbiologist can provide. J. Hosp. Infect. 43(Suppl. 1), doi: 10.1016/S0195-6701(99)90101-9
Köser, C. U., Ellington, M. J., Cartwright, E. J., Gillespie, S. H., Brown, N. M., Farrington, M., et al. (2012). Routine use of microbial whole genome sequencing in diagnostic and public health microbiology. PLoS Pathog. 8:e1002824. doi: 10.1371/journal.ppat.1002824
Lapão, L. V. (2007). Survey on the status of the hospital information systems in portugal. Methods Informat. Med. 46, 493–499. doi: 10.1160/ME9055
Laxminarayan, R., Duse, A., Wattal, C., Zaidi, A. K. M., Wertheim, H. F. L., Sumpradit, N., et al. (2013). Antibiotic resistance—the need for global solutions. Lancet Infect. Dis. 13, 1057–1098. doi: 10.1016/S1473-3099(13)70318-9
Lower, H. L., Eriksen, H. M., Aavitsland, P., and Skjeldestad, F. E. (2013). Methodology of the norwegian surveillance system for healthcare-associated infections: the value of a mandatory system, automated data collection, and active postdischarge surveillance. Am. J. Infect. Control 41, 591–596. doi: 10.1016/j.ajic.2012.09.005
MacKenzie, F. M. I., Gould, M., Bruce, J., Mollison, J., Monnet, D. L., Krcmery, V., et al. (2007). The role of microbiology and pharmacy departments in the stewardship of antibiotic prescribing in european hospitals. J. Hosp. Infect. 65, 73–81. doi: 10.1016/S0195-6701(07)60019-X
Magill, S. S., Edwards, J. R., Bamberg, W., Beldavs, Z. G., Dumyati, G., Kainer, M. A., et al. (2014). Multistate point-prevalence survey of health care–associated infections. New Engl. J. Med. 370, 1198–1208. doi: 10.1056/NEJMoa1306801
Malani, A. N., Richards, P. G., Kapila, S., Otto, M. H., Czerwinski, J., and Singal, B. (2012). Clinical and economic outcomes from a community hospital’s antimicrobial stewardship program. Am. J. Infect. Control 41, 145–148. doi: 10.1016/j.ajic.2012.02.021
Morshed, M. G., Lee, M., Jorgensen, D., and Isaac-Renton, J. L. (2007). Molecular methods used in clinical laboratory: prospects and pitfalls. FEMS Immunol. Med. Microbiol. 49, 184–191. doi: 10.1111/j.1574-695X.2006.00191.x
Neidell, M. J., Cohen, B., Furuya, Y., Hill, J., Jeon, C. Y., Glied, S., et al. (2012). Costs of healthcare- and community-associated infections with antimicrobial-resistant versus antimicrobial-susceptible organisms. Clin. Infect. Dis. 55, 807–815. doi: 10.1093/cid/cis552
Newton, D. W., and Novak-Weekley, S. (2011). Enhancing the function of clinical microbiology laboratories: can we navigate the road less traveled? J. Clin. Microbiol. 49 9(Suppl.), S72–S76. doi: 10.1128/JCM.00691-11
Patel, R. (2015). MALDI-TOF MS for the diagnosis of infectious diseases. Clin. Chem. 61, 100–111. doi: 10.1373/clinchem.2014.221770
Perez, K. K., Olsen, R. J., Musick, W. L., Cernoch, P. L., Davis, J. R., Peterson, L. E., et al. (2014). Integrating rapid diagnostics and antimicrobial stewardship improves outcomes in patients with antibiotic-resistant gram-negative bacteremia. J. Infect. 69, 216–225. doi: 10.1016/j.jinf.2014.05.005
Pestotnik, S. L. (2005). Expert clinical decision support systems to enhance antimicrobial stewardship programs: insights from the society of infectious diseases pharmacists. Pharmacotherapy 25, 1116–1125. doi: 10.1592/phco.2005.25.8.1116
Peterson, L. R., and Brossette, S. E. (2002). Hunting health care-associated infections from the clinical microbiology laboratory: passive, active, and virtual surveillance. J. Clin. Microbiol. 40, 1–4. doi: 10.1128/JCM.40.1.1-4.2002
Peterson, L. R., Hamilton, J. D., Baron, E. J., Tompkins, L. S., Miller, J. M., Wilfert, C. M., et al. (2001). Role of clinical microbiology laboratories in the management and control of infectious diseases and the delivery of Health Care. Clin. Infect. Dis. 32, 605–611. doi: 10.1086/318725
Pfaller, M. A., and Herwaldt, L. A. (1997). The clinical microbiology laboratory and infection control: emerging pathogens, antimicrobial resistance, and new technology. Clin. Infect. Dis. 25, 858–870. doi: 10.1086/515557
Pina, E. (2002). Prevenção de Infecções Adquiridas No Hospital - Um Guia Prático, 2a Edição. Lisboa: Instituto Nacional de Saúde Dr. Ricardo Jorge.
Pinto, P., Gil, M., Simões, A. S., da Silva, M. M., and Lapão, L. V. (2016). “Using design science research methodology to implement a surveillance and decision-support information system to manage healthcare associated infections and antibiotic use in hospitals,” in Conference Proceedings of European, Mediterranean & Middle Eastern Conference on Information Systems, Krakow.
Price, J., Gordon, N. C., Crook, D., Llewelyn, M., and Paul, J. (2013). The usefulness of whole genome sequencing in the management of Staphylococcus aureus infections. Clin. Microbiol. Infect. 19, 784–789. doi: 10.1111/1469-0691.12109
Reuter, S., Harrison, T. G., Koser, C. U., Ellington, M. J., Smith, G. P., Parkhill, J., et al. (2013). A pilot study of rapid whole-genome sequencing for the investigation of a legionella outbreak. BMJ Open 3:e002175. doi: 10.1136/bmjopen-2012-002175
Sabat, A. J., Budimir, A., Nashev, D., Sá-Leão, R., van Dijl, J. M., Laurent, F., et al. (2013). Overview of molecular typing methods for outbreak detection and epidemiological surveillance. Euro Surveill 18:20380.
Schreckenberger, P. C., and Binnicker, M. J. (2011). Optimizing antimicrobial susceptibility test reporting. J. Clin. Microbiol. 49(Suppl.), S15–S19. doi: 10.1128/JCM.00712-11
Simões, A. S., Valente, C., de Lencastre, H., and Sá-Leão, R. (2011). Rapid Identification of Noncapsulated Streptococcus pneumoniae in nasopharyngeal samples allowing detection of co-colonization and reevaluation of prevalence. Diagn. Microbiol. Infect. Dis. 71, 208–216. doi: 10.1016/j.diagmicrobio.2011.07.009
Simões, A. S., Gregório, J., Póvoa, P., and Lapão, L V. (2015). Practical Guide for the Implementation of Antibiotic Stewardship Programs. Lisboa: Instituto de Higiene e Medicina Tropical.
Singh, A., Goering, R. V., Simjee, S., Foley, S. L., and Zervos, M. J. (2006). Application of molecular techniques to the study of hospital infection. Clin. Microbiol. Rev. 19, 512–530. doi: 10.1128/CMR.00025-05
Solomon, S., and Ijaz, K. (2015). Surveillance and Monitoring of Antimicrobial Resistance (AMR). Geneva: World Health Organization.
Srinivasan, R., Karaoz, U., Volegova, M., MacKichan, J., Kato-Maeda, M., Miller, S., et al. (2015). Use of 16S rRNA gene for identification of a broad range of clinically relevant bacterial pathogens. PLoS ONE 10:e0117617. doi: 10.1371/journal.pone.0117617
Tenover, F. C. (2010). Potential impact of rapid diagnostic tests on improving antimicrobial use. Ann. N. Y. Acad. Sci. 1213, 70–80. doi: 10.1111/j.1749-6632.2010.05827.x
Teodoro, D., Pasche, E., Gobeill, J., Emonet, S., Ruch, P., and Lovis, C. (2012). Building a transnational biosurveillance network using semantic web technologies: requirements, design, and preliminary evaluation. J. Med. Internet. Res. 14:e73. doi: 10.2196/jmir.2043
Thomson, R. B., Wilson, M. L., and Weinstein, M. P. (2010). The clinical microbiology laboratory director in the united states hospital setting. J. Clin. Microbiol. 48, 3465–3469. doi: 10.1128/JCM.01575-10
Vernet, G., Mary, C., Altmann, D. M., Doumbo, O., Morpeth, S., Bhutta, Z. A., et al. (2014). Surveillance for antimicrobial drug resistance in under-resourced countries. Emerg. Infect. Dis. 20, 434–441. doi: 10.3201/EID2003.121157
Warhurst, G., Maddi, S., Dunn, G., Ghrew, M., Chadwick, P., Alexander, P., et al. (2015). Diagnostic accuracy of septifast multi-pathogen real-time pcr in the setting of suspected healthcare-associated bloodstream infection. Intensive Care Med. 41, 86–93. doi: 10.1007/s00134-014-3551-x
Wilson, M. P., and Spencer, R. C. (1999). Laboratory role in the management of hospital acquired infections. J. Hosp. Infect. 42, 1–6. doi: 10.1053/jhin.1998.0545
Keywords: microbiology, healthcare-associated infections, antibiotics, antibiotic stewardship, information systems, prevention, control, communication
Citation: Simões AS, Couto I, Toscano C, Gonçalves E, Póvoa P, Viveiros M and Lapão LV (2016) Prevention and Control of Antimicrobial Resistant Healthcare-Associated Infections: The Microbiology Laboratory Rocks! Front. Microbiol. 7:855. doi: 10.3389/fmicb.2016.00855
Received: 22 December 2015; Accepted: 23 May 2016;
Published: 07 June 2016.
Edited by:
Gilberto Igrejas, University of Trás-os-Montes and Alto Douro, PortugalReviewed by:
Santi M. Mandal, Vidyasagar University, IndiaGuyue Cheng, Huazhong Agricultural University, China
Copyright © 2016 Simões, Couto, Toscano, Gonçalves, Póvoa, Viveiros and Lapão. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandra S. Simões, assimoes@ihmt.unl.pt