 Ana L. G. Terças1Sirlei G. Marques2
Ana L. G. Terças1Sirlei G. Marques2 Eduardo B. Moffa3,4*Márcia B. Alves4Conceição M. P. S. de Azevedo5
Eduardo B. Moffa3,4*Márcia B. Alves4Conceição M. P. S. de Azevedo5 Walter L. Siqueira6Cristina A. Monteiro4*
Walter L. Siqueira6Cristina A. Monteiro4*- 1Department Federal Technological Teaching Center of Maranhão, São Luis, Brazil
- 2Nucleus of Tropical Pathology and Social Medicine, Department of Pathology, Federal University of Maranhão, São Luis, Brazil
- 3Department of Post-Graduate Program in Dentistry, CEUMA University, São Luis, Brazil
- 4Department of Post-Graduate Program in Parasite Biology, CEUMA University, São Luis, Brazil
- 5Department of Medicine, Federal University of Maranhão, São Luis, Brazil
- 6Schulich Dentistry and Department of Biochemistry, Schulich School of Medicine and Dentistry, The University of Western Ontario, London, ON, Canada
Oropharyngeal candidiasis is the most common fungal infection in hospitalized patients with acquired immune deficiency syndrome (AIDS). Its progression results in invasive infections, which are a significant cause of morbidity and mortality. This study aimed to quickly and accurately identify Candida spp. from oral mucosa of AIDS patients recruited at Presidente Vargas Hospital, in São Luís city, Brazil and to evaluate the sensitivity profile of these fungi to antifungals by using an automated system. Isolates were collected from oropharyngeal mucosa of 52 hospitalized AIDS patients, under anti-viral and antifungal therapies. Patients were included in research if they were HIV-positive, above 18 years of age and after obtaining their written consent. CHROMagar®Candida and the automated ViteK-2®system were used to isolate and identify Candida spp., respectively. Antifungal susceptibility testing was performed using the ViteK-2®system, complemented with the Etest®, using the drugs amphotericin B, fluconazole, flucytosine, and voriconazole. Oropharyngeal candidiasis had a high prevalence in these hospitalized AIDS patients (83%), and the most prevalent species was Candida albicans (56%). Antifungal susceptibility test showed that 64.7% of the Candida spp. were susceptible, 11.8% were dose-dependent sensitive, and 23.5% were resistant. All the Candida krusei and Candida famata isolates and two of Candida glabrata were resistant to fluconazole. Most of AIDS patients presented oropharyngeal candidiasis and C. albicans was the most frequently isolated species. The results showed high variability in resistance among isolated species and indicates the need to identify the Candida spp. involved in the infection and the need to test antifungal susceptibility as a guide in drug therapy in patients hospitalized with AIDS. This is the first relate about AIDS patients monitoring in a public hospital in São Luís concerning the precise identification and establishing of antifungal profile of Candida spp..
Introduction
In recent decades, the increasing incidence of fungal infections has been linked to patients with congenital or acquired immunodeficiency (Ortega et al., 2010; Junqueira et al., 2012; Li et al., 2013). Candida albicans is the most frequently isolated species in humans (Delgado et al., 2009; Hise et al., 2009; Junqueira et al., 2012; Li et al., 2013). However, there has been a significant increase in the prevalence of infections caused by species of Candida other than C. albicans such as C. krusei, C. tropicalis, C. glabrata, C. guilliermondii, and C. parapsilosis (Sant’Ana et al., 2002; Li et al., 2013; Kaur et al., 2016).
Despite the high effectiveness of the current antiretroviral therapies, HIV+ subjects have a higher prevalence of oropharyngeal candidiasis (OPC) than individuals without this disease, and its expression is a predictive marker for increased immunosuppression (Erkose and Erturan, 2007). The advancement of HIV infection can result in more frequent and severe OPC episodes (Sharma et al., 2009). The severity of the disease, associated with debilitating conditions of patients, causes prolonged hospital stays and higher hospital costs, generating a major public health problem (Back-Brito et al., 2009).
The progression of oral candidiasis is often faster and more severe in patients with AIDS due to immunodeficiency and the emergency of antifungal resistance among Candida species isolates. Also, in fungal infection, the identification of Candida spp. is essential since the pathogenicity profile and sensitivity to a particular antifungal agent vary between different species (Costa et al., 2009; Negri et al., 2009). Some authors also argue that exposure to antifungal agents during candidiasis treatment provided a positive selection pressure for non-albicans yeasts, such as C. glabrata and C. krusei (Hunter et al., 1998; Martinez et al., 2002), that are considered intrinsically less sensitive than others species (Pfaller, 2012).
Therefore, this variability in the behavior of different Candida spp. and the increasing number of clinical isolates resistant to current antifungal therapies highlight the need for antifungal susceptibility testing to monitor the antifungal resistance of these microorganisms. This could guide the therapeutic choice and the clinical treatment. In addition, an accurate identification of strains isolated from infections in patients with AIDS is important because these patients are more likely to carry species other than C. albicans that may be less sensitive to antifungal agents (Belazi et al., 2005; Li et al., 2013; Idelevich et al., 2014).
Antifungal agents available for the treatment of candidiasis are as follows: the polyenes [nystatin and amphotericin B (AMB)]; the ergosterol biosynthesis inhibitors – the azoles (miconazole, clotrimazole, ketoconazole, itraconazole, and FCZ), allylaminesthiocarbamates, and morpholines; and DNA analog 5-fluorocytosine, and newer agents such as caspofungins (Pappas et al., 2009). The antifungal agents target three cellular components of fungi. Azoles inhibit the synthesis of ergosterol in the endoplasmic reticulum of the fungal cell. Polyenes such as AMB bind to ergosterol in the fungal membrane causing disruption of membrane structure and function. Flucytosine (5-FC) is converted within the fungal cell to 5-fluorouracil, which inhibits DNA synthesis (Patil et al., 2015). All can be used with varying efficacy depending on the type and site of infection and the sensitivity of the Candida species (Pfaller et al., 2010). For most Candida infections, FCZ is the drug of choice (Pfaller et al., 2010; Patil et al., 2015).
Like many others cities in developing countries such as São Luís in Brazil, antifungal testing is not performed routinely (Hamza et al., 2008; Costa et al., 2009). Also, to the best of our knowledge, there are no studies that have established the prevalence or evaluated the profile of antifungal sensitivity of clinical isolates obtained from AIDS patients in São Luís city, Northeast Brazil. Importantly, the mortality rate for AIDS cases in Maranhão in 2013 is the highest in the Northeast: 6.6 cases per 100,000 inhabitants. In addition, a total of 249 new cases of AIDS has been confirmed in São Luís in 2013 (Brazil, Ministério da Saúde, 2014).
Thus, this study was conducted with the objective of identifying Candida spp. from oropharynx in hospitalized AIDS patients using the automated ViteK-2system. We also aimed to evaluate and compare the sensitivity profile of these yeasts to four antifungal drugs, FCZ, AMB, 5-FC, and voriconazole (VCZ), using the ViteK-2 and Etest systems in order to guide the therapeutic choice and the clinical treatment of these patients.
Materials and Methods
Patients and Oral Isolates
The Candida spp. were obtained by swabbing the oropharyngeal mucosa of 52 AIDS patients hospitalized in Getúlio Vargas Hospital in São Luis, Brazil. Patients were included in research if they were HIV-positive, above 18 years of age and submitted their written consent (Ethics Committee of Federal University of Maranhão process No. 23115006540/2009-40). Some patients were under anti-viral and antifungal therapies. Among the patients, there were 22 females and 30 males in the age range of 19–61 years.
The patients in this study presented CD4+ cell counts ranging from 10 to 552 cells/mm3 and viral loads of 2,567 to 256,860 copies/mL. Sterile swabs were used for the collection of samples and were inoculated into tubes containing saline solution P.A 0.85% (ISOFAR, Paraná, Brazil). They were then sent to the Medical Mycology Laboratory of Ceuma University and were incubated in BHI (Broth Heart Infusion – Acumedia Manufactures) at 37°C for 48 h.
Candida spp. Identification and Preparation of Inoculums
The primary isolation of yeasts was performed using the CHROMagar®Candida (Difco) Chromogenic differential medium in Petri dishes and incubated at 37°C for 48 h. This medium is based on the use of β-glucosaminidase substrate and differentiates yeast according to the morphology and the color of the colonies. This method provides a presumptive diagnosis of Candida spp. (Hospenthal et al., 2004). Green colored colonies were identified as C. albicans, blue-cobalt as C. tropicalis, pink or lilac as C. krusei, and other species were whitish-pink in color. The isolated yeasts from chromogenic medium were picked and incubated at 35°C for 48 h in tubes with SDA (Sabouraud Dextrose Agar with chloramphenicol – Acumedia) medium and then stored at -20°C for use in the study.
The biochemical identification of the yeasts was performed using an automated method (Vitek-2 Compact bioMérieux, Marcy-l’Étoile, France).
The Biomerieux Vitek-2 system includes the Vitek-2 cards that allow species identification by comparison of the biochemical profile with an extensive database http://www.jgid.org/article.asp?issn=0974-174777X;year=2016;volume=8;issue=4;spage=139;epage=146;aulast=Kaur-ref9 (Cuenca-Estrella et al., 2010). Biomerieux Vitek-2 expanded its role in this area with a yeast susceptibility test that determines Candida growth spectrophotometrically using Vitek-2 microbiology systems, performing fully automated testing of susceptibility to 5-FC, AMB, FCZ, and VCZ (Borghi et al., 2010).
For the preparation of the fungal inoculum (3 mL 0.45% saline + yeast colony), a McFarland scale 2 from DensiChek-bioMerieuxVitek® system was used. This standardized suspension was aspirated into the identification cards, and then the cards were sealed and subjected to biochemical tests by an optical sensor reading. We used the YST card (Yeast identification, bioMérieux) to determine the genus and species of yeast. The test was considered complete when the percentage of probability was ≥85% and there was no request for further testing.
In vitro Antifungals Susceptibility Tests
Thereafter, antifungal susceptibility tests (AFST) were conducted using the ViteK-2® automated system and Etest® (Biodisk AB, Solna, Sweden) according to the manufacturer’s recommendations. These methods have been chosen because they are easy to perform and offer results in a short period of time (Kaur et al., 2016).
For this, 180 μL of inoculum was standardized to the McFarland scale 2.0 using the DensiChek densitometer of the ViteK-2® system, placed in a tube containing 3 mL of 0.45% saline, and aspirated into the AST-YSO1 card (bioMérieux). The following antifungal drugs were tested: AMB (0.03–16 μg/mL), FCZ (1–64 μg/mL), 5-FC (0.125–64 μg/mL), and VCZ (0.125–16 μg/ml). The analysis and interpretation of data were performed according to M27-A3 and M27-S3 CLSI standards. For quality control, we used standard strains of C. krusei (ATCC 6258) and C. parapsilosis (ATCC 22019). For fungal strains that did not respond to the AST cards, an Etest® (Biodisk AB, Solna, Sweden) was performed, which consisted of a gradient method with predefined concentrations of FCZ and AMB in μg/mL. In this method, the colonies were seeded at a concentration of 0.5 McFarland on dishes with RPMI (Probac®, Sao Paulo, Brazil) supplemented with 2% glucose agar and then incubated at 35°C for 48 h. The reading was performed by assessing the point of intersection between the halo formed and the Etest strip. The FCZ MIC was determined as the lowest concentration that inhibited 80% of fungal strains, and the AMB MIC was calculated as the lowest concentration with no observed fungal growth. The profile of the antifungal drug sensitivity was classified as sensitive (S), dose-dependent sensitivity (S-DD), and/or intermediate (I), and resistant (R).
The breakpoints used to define sensitivity, intermediate, and resistant for each species were those defined by Clinical and Laboratory Standards Institute [CLSI] (2008). The MIC values ≤ 8 μg/mL for FCZ were considered susceptible (S), 16–32 μg/mL was considered as susceptible dose-dependent (SDD), and ≥64 μg/mL as resistant (R). For AMB, MICs ≤ 1 μg/mL were considered to be S and ≥1 μg/mL was R. For 5-FC, CIMs ≤ 4 μg/mL were considered to be S, 8–16 μg/mL was I, and ≥32 μg/mL was R. For VCZ, MICs ≤ 0,125 μg/mL were S and ≥16 μg/mL were considered R.
Fluconazole and amphotericin were chosen for the tests because they have different mechanisms of action and are the main drugs chosen for the treatment of Candida infections (Patil et al., 2015). VCZ and 5-FC were chosen because they could be an alternative for species resistant to FCZ and amphotericin.
Ethics Statement
The study protocol was established according to the Guidelines and Standards for Research Involving Humans (Resolution of the National Council No. 196/96 of October 10, 1996) and was approved by the Ethics Committee of UFMA (Federal University of Maranhão) under decision No. 23115006540/2009-40. All the participants signed a free and informed consent form.
Statistical Analysis
The data collected were expressed as mean and standard deviation for numeric variables, and absolute and relative frequencies for categorical variables. We used the chi-squared (χ2) test to analyze categorical variables, and analysis of variance (ANOVA) followed by the Tukey’s post-test was used for numeric variables when p < 0.05. A significance level of p < 0.05 was adopted.
Results
Patient Data and Prevalence of Isolates
From 52 AIDS patients participating in the study, 43 were positive for Candida. Fifty-four fungal isolates were recovered from these patients, and thus, in some cases, more than one species was isolated from a single clinical sample. Eighty-three percent of patients participating in the study had oropharyngeal candidiasis, and 52.2% had used antifungals. Of these, 75% were using both FCZ and nystatin and 8.3% used FCZ, nystatin, and AMB.
Among the yeast samples, 43 (83%) grew in CHROMagar Candida medium and 9 (17%) were negative. Using the automated Vitek-2® Compact bioMérieux system, 51 isolates were identified as Candida spp., including 29 C. albicans (56%), 6 C. tropicalis (12%), 6 C. krusei (12%), 4 C. glabrata (8%), 2 C. famata (4%), 2 C. parapsilosis (4%), and 2 C. guilliermondii (4%) (Table 1). One isolate of Kodamaeaohmeri (Pichia ohmeri), one of Rhodotorula spp., and one of Trichosporon spp. were also identified.
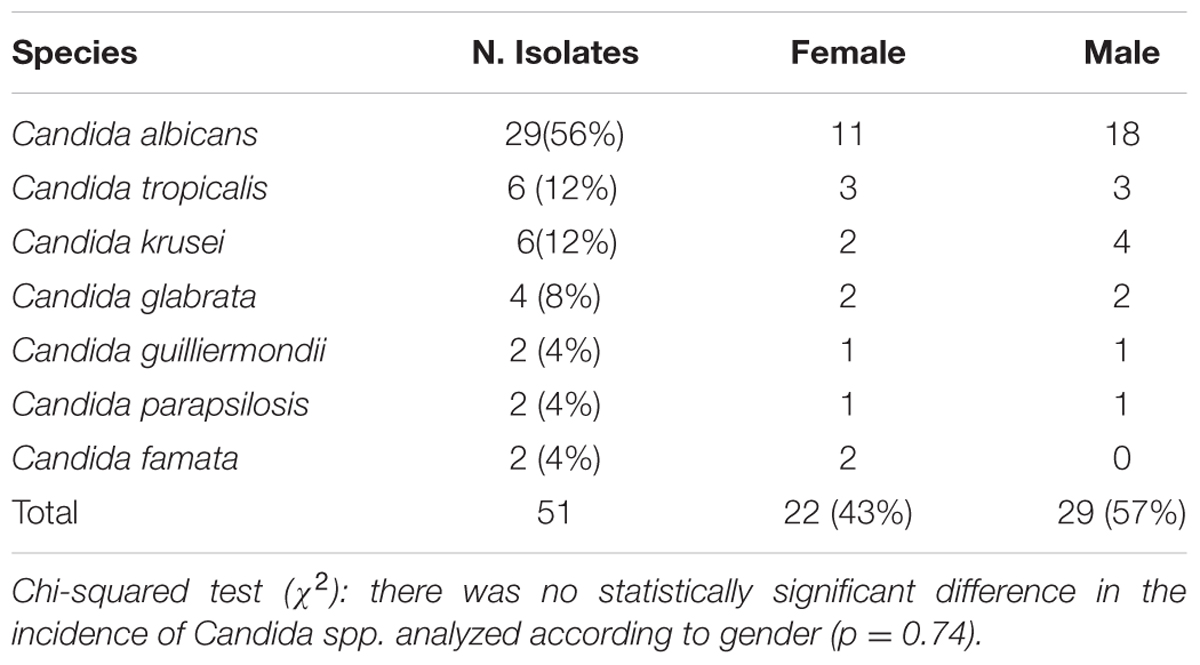
TABLE 1. Number and prevalence (%) of the Candida strains identified by the Vitek-2® system, and their distribution according to patient gender.
When looking at the distribution of isolates of Candida spp. by patients’ gender, we observed that the number of isolates coming from the men patients (n = 29/57%) was higher than that from the women (n = 22/43%; Table 1). The age group with the highest frequency of Candida spp. isolates was 30–40 years (50.98%), followed by the 20–29 years age group (27.45%; Figure 1).
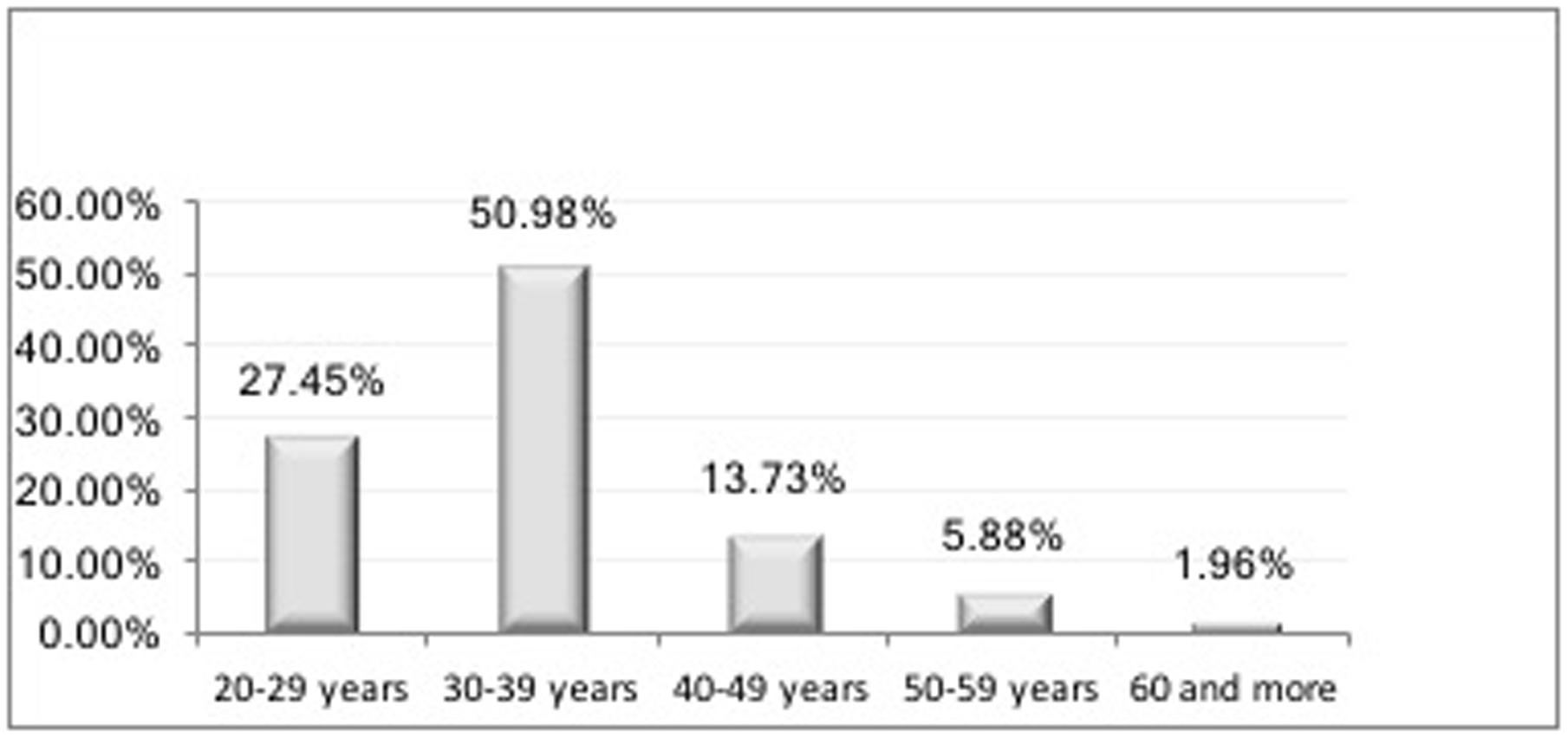
FIGURE 1. Distribution (%) of hospitalized patients with acquired immune deficiency syndrome (AIDS) by age group (years).
In vitro Susceptibility of Isolates
The antifungal susceptibility testing performed by the automated ViteK-2® system showed that 58% of tests were completed in a period of 12–15 h, and most of them did not exceed 19 h. However, for four slow-growing or nutritionally fastidious and demanding microorganisms, 36 h was not sufficient to obtain the results. These cases included the following isolates: 2 C. famata, 1 Rhodotorulaglutinis, 1 Trichosporon spp., and 1 Kodamaeaohmeri (Pichia ohmeri). For these isolates, the MIC was determined using the Etest® system. The results showed that all strains of C. albicans (n = 29), C. tropicalis (n = 6), C. parapsilosis (n = 2), and C. guilliermondii (n = 2) showed sensitivity to all antifungals drugs tested. All six isolates of C. krusei were resistant to FCZ, four of them showed intermediate susceptibility to 5-FC, and all were sensitive to AMB and VCZ (Table 2). Two C. glabrata isolates were resistant to FCZ, one was resistant to AMB, and another one was resistant to VCZ. The sensitivity profile of the antifungals tested was virtually the same for all of the Candida spp. used in the survey, except for C. krusei and C. famata, which were resistant to FCZ. C. glabrata isolates showed resistance to three different antifungals. However, this small difference in sensitivity toward the antifungals in these three species did not translate to a statistically significant difference. The ANOVA test showed no difference in the sensitivity profile (p = 0.99), S-DD (p = 0.51), and resistance (p = 0.18) of the antifungals.
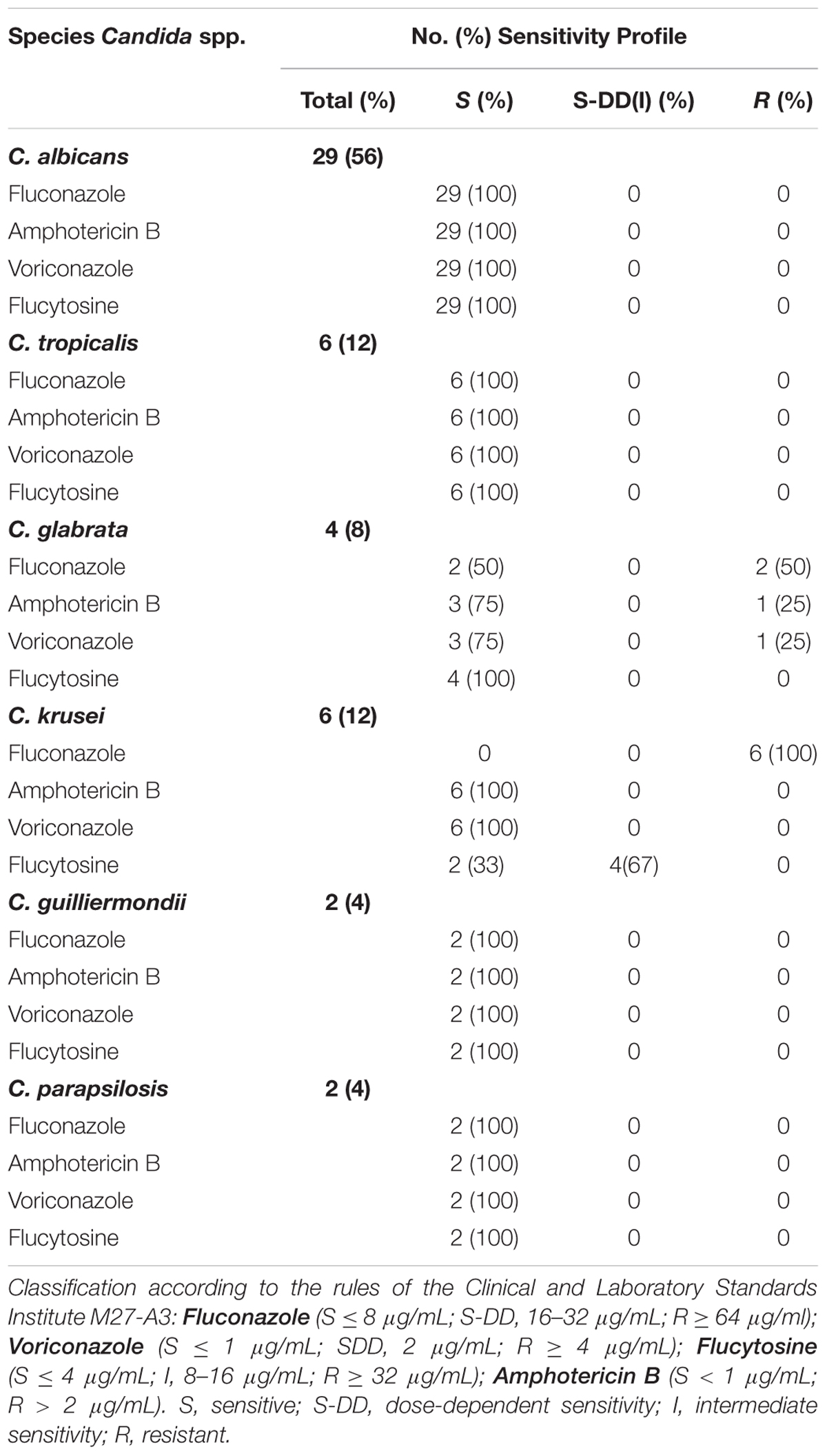
TABLE 2. Distribution of isolates of Candida spp. according to the minimum inhibitory concentration (MIC) against four antifungal drugs as evaluated by the Vitek 2® system.
In the susceptibility test performed using the Etest® method, two isolates of C. famata were resistant to FCZ but were susceptible to AMB. Rhodotorulaglutinis isolates were resistant to FCZ and AMB. Trichosporon spp. isolates were susceptible to FCZ and resistant to AMB. Kodamaeaohmeri (Pichia ohmeri) was resistant to FCZ but it displayed sensitivity to AMB (Table 3).
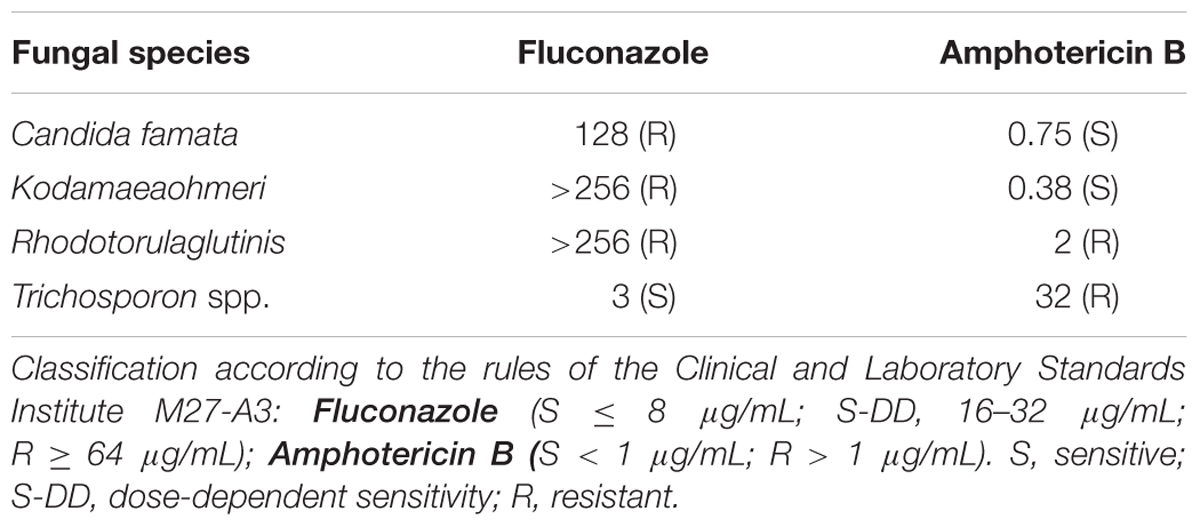
TABLE 3. Minimum inhibitory concentrations (MIC) as evaluated by the Etest®system of four different fungals.
Discussion
Oropharyngeal candidiasis is the most common opportunistic infection among HIV-seropositive patients and in those with AIDS, and it represents a major treatment challenge. Hence, it is recommended to determine the species involved in the infection and its antifungal susceptibility.
Among 52 patients involved in this study, 30 were men and 22 were women, resulting in the ratio of 1.4 cases in men for every 1 case in women. These findings lead us to reflect on whether the incidence of AIDS in women is increasing and equating with the incidence in males. Data from the last epidemiological study in Brazil, published in the AIDS and STDs Bulletin in 2011, showed that in 2011, the ratio of 1.7 cases in men for every 1 case in women was greatly diminished when compared to data from 1989, when there were about six cases of AIDS in men for every case in women (Hinrichsen et al., 2008). In the present study, we also found that the most prevalent age group was 30–39 years, followed by the 40–49 years age group. These data are similar to those published in Brazil (Hinrichsen et al., 2008) and other countries (Hamza et al., 2008).
The patients hospitalized with AIDS in this study presented a low CD4+ lymphocyte count (90% of patients had less than 200 cells/mm3) and a high viral load (80% of patients had above 50,000 copies/mL). Although 90% of patients had CD4+ lymphocyte counts below 200 cells/mm3, studies have not shown any correlation between oral candidiasis and low CD4+ lymphocyte counts, but they have shown correlation with a high viral load (Morgan, 2005; Erkose and Erturan, 2007; Back-Brito et al., 2009). This study also showed a high frequency of OPC in these patients (83%), and most of them had exposure to more than one antifungal agent, including FCZ, nystatin, and AMB. These data are alarming and support the relevance of our research since we isolated a very high frequency of resistant yeasts. As far as we know, this is the first study with AIDS patients from the city of São Luís concerning the distribution of oral yeasts, species prevalence, and antifungal susceptibility profile.
The isolation of Candida species in this study was performed by the CHROMagar Candida culture medium, and consequently, it presumptively identified some species involved. Thereafter, we used the ViteK-2system, a system with excellent reproducibility and accuracy when compared with the CLSI method (Clinical and Laboratory Standards Institute [CLSI], 2008; Bourgeois et al., 2010; Cuenca-Estrella et al., 2010; Kaur et al., 2016) for identification of all isolates. Among the 52 patients admitted with AIDS who submitted to buccal smears, 43 (83%) were positive for Candida ssp. culture. This result is similar to that found in other studies, which showed that 80–95% of these patients develop one or more fungal infections during their illness (Rex et al., 2000; Campisi et al., 2002, Junqueira et al., 2012). In this study, we observed that C. albicans was the most prevalent species (56%) against all non-albicans Candida species (NAC; 44%), which is in accordance with other studies (Viudes et al., 2002; Colombo et al., 2006; Kaur et al., 2016). Among the NAC species, the most prevalent species were C. tropicalis, C. krusei, and C. glabrata, which is in agreement with other studies (Colombo et al., 2006; Hamza et al., 2008). In this study, we identified a case of a patient with four Candida spp. that were identified in a single clinical sample; one of the species was C. glabrata, which is resistant to both FCZ and AMB, and the other was C. krusei, which is resistant to FCZ. This finding is relevant because FCZ is the drug of choice for candidiasis treatment in AIDS patients although it has a fungistatic action (Siikala et al., 2010; Rautemaa and Ramage, 2011), and both FCZ and AMB were being used by some of the patients who participated in the research. Seven patients had double colonization, and one of them had colonization by C. krusei resistant to FCZ. The coexistence of various species in the same clinical specimen has also been reported in other studies (Swinne et al., 2004; Junqueira et al., 2012).
We used the automated ViteK-2® and Etest® systems to screen for AFST because they present good reproducibility and rapid diagnostic tests with Candida spp. (Pfaller et al., 2007; Borghi et al., 2010; Bourgeois et al., 2010; Cuenca-Estrella et al., 2010; Kaur et al., 2016). Both methods have advantages over the Clinical and Laboratory Standards Institute (CLSI) standardized broth microdilution method, which is considered as a reference for antifungal susceptibility testing although it is complex and laborious to use as a routine method (Bourgeois et al., 2010; Kaur et al., 2016). The VK2 method demonstrated excellent reproducibility, which underscores its excellent level of standardization. Spectrophotometric readings remove subjectivity from the MIC determination. Furthermore, Candida species identification and in vitro antifungal susceptibility are obtained in less than 26.5 h (mean, 15.2 h), thus, reducing the time necessary for optimizing antifungal treatment decisions. ViteK-2® system results are on average available within 15 h 13 min, with a range of 12 h 15 min (C. albicans) to 26 h 30 min (C. glabrata; Bourgeois et al., 2010). The Etest® method is an alternative, standardized, and reliable method adapted to hospital laboratories. This method provides an accurate MIC value, and this critical information helps the clinician to ensure that the appropriate treatment of the patient will be achieved (Pfaller et al., 1998; Bourgeois et al., 2010).
Nevertheless, in this study, some fastidious species failed to grow sufficiently when we used the automated ViteK-2® system, but for the Etest® method, all of the isolates grew enough to be read at 24 and 48 h. Thus, we note that, when used in conjunction with the ViteK-2® method, these two AST methods have the potential to satisfy all the requirements for susceptibility testing in routine clinical microbiology analysis. Generally, many authors use one or another method, mainly the classical, laborious, and time consuming microdilution method described in the CLSI M27-A3 standard (Bremenkamp et al., 2011; Melo et al., 2011; Li et al., 2013; Sanitá et al., 2013), which is still considered the gold standard for susceptibility tests.
In this study, all isolates of C. albicans (n = 29), C. tropicalis (n = 6), C. parapsilosis (n = 2), and C. guilliermondii (n = 2) showed sensitivity to all of the antifungal drugs tested, which is consistent with the general pattern of susceptibility of the NCLS M-27 method and with the results of other studies (Pfaller et al., 2007, 2008). Eighty percent of the Candida spp. studied were sensitive to FCZ, 18% were resistant, and 2% presented a S-DD. These results are similar to those observed by other researchers (Hospenthal et al., 2004; Pfaller et al., 2007; Hamza et al., 2008). Resistance to FCZ was observed in this study in all six samples of C. krusei (100%), two of C. glabrata (50%), and all of C. famata (100%). In fact, C. krusei has an innate resistance to FCZ, and C. glabrata possesses the capacity to develop resistance after the first contact with this antifungal agent. The results of this study are in agreement with several studies that demonstrated the innate resistance of C. krusei to FCZ and the increased resistance of C. glabrata and C. famata species to this antifungal drug (Campisi et al., 2002; Hamza et al., 2008; Pfaller et al., 2008; Junqueira et al., 2012; Patil et al., 2015).
Regarding VCZ, almost all Candida spp. isolates in this study were sensitive to this drug, and only C. glabrata demonstrated resistance. Based on these data, VCZ could be an effective drug for the treatment of patients involved in the study. In fact, studies have shown that VCZ is effective against Candida spp. that were resistant to FCZ and/or AMB (Swinne et al., 2004; Pfaller et al., 2007).
For AMB, the cutoff point (breakpoints) had not been determined by CLSI. Researchers have determined that a value of <1 μg/mL for an isolated strain would show sensitivity to AMB, and a value of >1 μg/mL would demonstrate resistance (Hepburn et al., 2003; Kaur et al., 2016). According to these cutoffs, this study showed that 94% of the Candida isolates were sensitive, 2% presented S-DD, and 4% were resistant. These results were similar to those from other studies, where upon examination of 100 HIV-infected patients revealed 58 with positive cultures for Candida spp., and of these, 96% were susceptible to AMB and 4% were resistant (Alves et al., 2006). Despite 50 years of polyene use, resistance to AMB is rare because it binds to ergosterol in the fungal membrane causing disruption of membrane structure and function, having, thus, a fungicide action (Patil et al., 2015). However, it is worth noting that among the non-Candida yeasts isolated in this study, two were resistant to AMB and two were resistant to FCZ. One of them was resistant to both antifungals, which draws our attention to the danger of treatment without the precise identification and establishment of the antifungal profile.
With regard to 5-FC, a high sensitivity of Candida isolates (92%) was observed in this study probably because this antifungal inhibits DNA synthesis (Patil et al., 2015). Only four (8%) C. krusei samples showed S-DD. Flucytosine has a high activity against C. albicans, although it has been reported that 40% of C. krusei strains are resistant to this drug. Flucytosine should be used as a treatment option only when the Candida spp. is resistant to the azole antifungal family (Alves et al., 2006).
Many public hospitals that treat patients with HIV/AIDS do not have the laboratory facilities that allow a rapid and accurate diagnosis for treatment planning. Our results showed that OPC infection has a high prevalence in hospitalized AIDS patients (83%), and although all C. albicans were sensitive to the drugs tested, most of the NAC species showed high resistance to more than one antifungal agents (30%). Most of the observed resistance was to FCZ, and the species that highlights as resistant were C. krusei (100%), C. famata (100%), and C. glabrata (50%). Also, 25% of C. glabrata were resistant to AMB and 40% of C. krusei were intermediate to 5-FC. These findings are important because they show the variable resistance profile among different strains and the need to identify the Candida spp. involved in the infection, mainly because the patients involved were or had been on antifungal treatment. This also demonstrates the use of antifungal susceptibility testing as a guide to drug therapy in hospitalized AIDS patients.
Determining the MIC of a drug does not guarantee the success of the treatment because, in an infection, the role of the host is critical to obtain a satisfactory clinical response. However, it is known that when the profile of a Candida spp. is resistant at a tested drug concentration, this concentration often leads to a failed clinical treatment (Rex et al., 2000).
We found a high prevalence of OPC and high frequency of resistant Candida spp. in AIDS patients in a public hospital in Sao Luis. São Luís is a city in the northeast of Brazil with the highest number of cases of AIDS, and like other cities in developing countries, in vitro antifungal testing is not performed routinely. Monitoring clinical samples is extremely important for the selection of the appropriate drug and dose, which helps predict those patients who are likely to respond to therapy and ensure prevention of excessive dosing and selection of resistant microorganisms. The data obtained here allowed the most effective monitoring of these patients, providing them with the possibility of more adequate therapy. It is noteworthy that the Vitek-2® automated system used in conjunction with the Etest® meets all the requirements for the susceptibility testing of fungi in routine clinical microbiology laboratories.
Author Contributions
Conceived and designed the experiments: AT, SM, CdA, MA, and CM. Performed the experiments: AT, SM, CdA, and CM. Analyzed the data: AT, SM, EM, MA, WS, and CM. Contributed reagents/materials/analysis tools: AT, SM, EM, MA; CdA, WS, and CM. Wrote the manuscript: AT, SM, EM, MA, CdA, WS, and CAM.
Funding
The authors would like to thank Foundation for Research and Scientific 441 Development of Maranhão (FAPEMA) for the financial support (UNIVERSAL #01444/16).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Alves, S. H., Da Matta, D. A., Azevedo, A. C., Loreto, E. S., Boff, E., Santurio, J. M., et al. (2006). In vitro activities of new and conventional antimycotics against fluconazole-susceptible and non-susceptible Brazilian Candida spp. isolates. Mycoses 49, 220–225. doi: 10.1111/j.1439-0507.2006.01226.x
Back-Brito, G. N., Mota, A. J., Vasconcellos, T. C., Querido, S. M., Jorge, A. O., Reis, A. S., et al. (2009). Frequency of Candida spp. in the oral cavity of Brazilian HIV-positive patients and correlation with CD4 cell counts and viral load. Mycopathologia 167, 81–87. doi: 10.1007/s11046-008-9153-9
Belazi, M., Velegraki, A., Fleva, A., Gidarakou, I., Papanaum, L., Baka, D., et al. (2005). Candidal overgrowth in diabetic patients: potential predisposing factors. Mycoses 48, 192–196. doi: 10.1111/j.1439-0507.2005.01124.x
Borghi, E., Iatta, R., Sciota, R., Biassoni, C., Cuna, T., Montagna, M. T., et al. (2010). Comparative evaluation of the Vitek 2 yeast susceptibility test and CLSI broth microdilution reference method for testing antifungal susceptibility of invasive fungal isolates in Italy: the GISIA 3 study. J. Clin. Microbiol. 48, 3153–3157. doi: 10.1128/JCM.00952-10
Bourgeois, N., Dehandschoewercker, L., Bertout, S., Bousquet, P. J., Rispail, P., and Lachaud, L. (2010). Antifungal susceptibility of 205 Candida spp. isolated primarily during invasive Candidiasis and comparison of the Vitek 2 system with the CLSI broth microdilution and Etest methods. J. Clin. Microbiol. 48, 154–161. doi: 10.1128/JCM.01096-09
Bremenkamp, R. M., Caris, A. R., Jorge, A. O., Back-Brito, G. N., Mota, A. J., Balducci, I., et al. (2011). Prevalence and antifungal resistance profile of Candida spp. oral isolates from patients with type 1 and 2 diabetes mellitus. Arch. Oral Biol. 56, 549–555. doi: 10.1016/j.archoralbio.2010.11.018
Campisi, G., Pizzo, G., Milici, M. E., Mancuso, S., and Margiotta, V. (2002). Candidal carriage in the oral cavity of human immunodeficiency virus-infected subjects. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 93, 281–286. doi: 10.1067/moe.2002.120804
Clinical and Laboratory Standards Institute [CLSI] (2008). M27-A3 Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeast; Approved Standard, 3rd Edn, Vol. 28. Wayne, PA: CLSI, 6–12.
Colombo, A. L., Nucci, M., Park, B. J., Nouér, S. A., Arthington-Skaggs, B., da Matta, D. A., et al. (2006). Epidemiology of candidemia in Brazil: a nationwide sentinel surveillance of candidemia in eleven medical centers. J. Clin. Microbiol. 44, 2816–2823. doi: 10.1128/JCM.00773-06
Costa, A. R., Rodrigues, M. E., Silva, F., Henriques, M., Azeredo, J., Faustino, A., et al. (2009). MIC evaluation of Candida reference strains and clinical isolates by E-test. J. Chemother. 21, 351–355. doi: 10.1179/joc.2009.21.3.351
Cuenca-Estrella, M., Gomez-Lopez, A., Alastruey-Izquierdo, A., Martinez, L. B., Cuesta, I., Buitrago, M. J., et al. (2010). Comparison of the Vitek 2 antifungal system with the clinical and laboratory standards institute (CLSI) and european committee on antimicrobial susceptibility testing (EUCAST) broth microdilution reference methods and with the sensititre yeast one and etest techniques for in vitro detection of antifungal resistance in yeast isolates. J. Clin. Microbiol. 48, 1782–1786. doi: 10.1128/JCM.02316-09
Delgado, A. C., de Jesus Pedro, R., Aoki, F. H., Resende, M. R., Trabasso, P., Colombo, A. L., et al. (2009). Clinical and microbiological assessment of patients with a long-term diagnosis of human immunodeficiency virus infection and Candida oral colonization. Clin. Microbiol. Infect. 15, 364–371. doi: 10.1111/j.1469-0691.2009.02707.x
Erkose, G., and Erturan, Z. (2007). Oral Candida colonization of human immunodeficiency virus infected subjects in Turkey and its relation with viral load and CD4+ T-lymphocyte count. Mycoses 50, 485–490. doi: 10.1111/j.1439-0507.2007.01393.x
Hamza, O. J., Matee, M. I., Moshi, M. J., Simon, E. N., Mugusi, F., Mikx, F. H., et al. (2008). Species distribution and in vitro antifungal susceptibility of oral yeast isolates from Tanzanian HIV-infected patients with primary and recurrent oropharyngeal candidiasis. BMC Microbiol. 8:135. doi: 10.1186/1471-2180-8-135
Hepburn, M. J., Pennick, G. J., Sutton, D. A., Crawford, G. E., and Jorgensen, J. H. (2003). Candida krusei renal cyst infection and measurement of amphotericin B levels in cystic fluid in a patient receiving AmBisome. Med. Mycol. 41, 163–165.
Hinrichsen, S. L., Falcao, E., Vilella, T. A., Colombo, A. L., Nucci, M., Moura, L., et al. (2008). Candidemia in a tertiary hospital in northeastern Brazil. Rev. Soc. Bras. Med. Trop. 41, 394–398. doi: 10.1590/S0037-86822008000400014
Hise, A. G., Tomalka, J., Ganesan, S., Patel, K., Hall, B. A., Brown, G. D., et al. (2009). An essential role for the NLRP3 inflammasome in host defense against the human fungal pathogen Candida albicans. Cell Host Microbe 5, 487–497. doi: 10.1016/j.chom.2009.05.002
Hospenthal, D. R., Murray, C. K., and Rinaldi, M. G. (2004). The role of antifungal susceptibility testing in the therapy of candidiasis. Diagn. Microbiol. Infect. Dis. 48, 153–160. doi: 10.1016/j.diagmicrobio.2003.10.003
Hunter, K. D., Gibson, J., Lockhart, P., Pithie, A., and Bagg, J. (1998). Fluconazole resistant Candida species in the oral flora of fluconazole-exposed HIV-positive patients. Oral Surg. Oral Med. Oral Pathol. 85, 558–564.
Idelevich, E. A., Grunewald, C. M., Wullenweber, J., and Becker, K. (2014). Rapid identification and susceptibility testing of Candida spp. from positive blood cultures by combination of direct MALDI-TOF mass spectrometry and direct inoculation of Vitek 2. PLoS ONE 9:e114834. doi: 10.1371/journal.pone.0114834
Junqueira, J. C., Vilela, S. F., Rossoni, R. D., Barbosa, J. O., Costa, A. C. B. P., Rasteiro, V. M. C., et al. (2012). Oral colonization by yeasts in HIV-positive patients in Brazil. Rev. Inst. Med. Trop. Sao Paulo 54, 17–24. doi: 10.1590/S0036-46652012000100004
Kaur, R., Dhakad, M. S., Goyal, R., Haque, A., and Mukhopadhyay, G. (2016). Identification and Antifungal susceptibility testing of Candida species: a comparison of Vitek-2 system with conventional and molecular methods. J. Glob. Infect. Dis. 8, 139–146. doi: 10.4103/0974-777X.192969
Li, Y. Y., Chen, W. Y., Li, X., Li, H. B., Li, H. Q., Wang, L., et al. (2013). Asymptomatic oral yeast carriage and antifungal susceptibility profile of HIV-infected patients in Kunming, Yunnan Province of China. BMC Infect. Dis. 13:46–53. doi: 10.1186/1471-2334-13-46
Martinez, M., López-Ribot, J. L., Kirkpatrick, W. R., Coco, B. J., Bachmann, S. P., and Patterson, T. F. (2002). Replacement of Candida albicans with Candida dubliniensis in human immunodeficiency virus infected patients with oropharyngeal candidiasis treated with fluconazole. J. Clin. Microbiol. 40, 3135–3139. doi: 10.1128/JCM.40.9.3135-3139.2002
Melo, A. S., Bizerra, F. C., Freymüller, E., Arthington-Skaggs, B. A., and Colombo, A. L. (2011). Biofilm production and evaluation of antifungal susceptibility amongst clinical Candida spp. isolates, including strains of the Candida parapsilosis complex. Med Mycol. 49, 253–262. doi: 10.3109/13693786.2010.530032
Morgan, J. (2005). Global trends in candidemia: review of reports from 1995-2005. Curr. Infect. Dis. Rep. 7, 429–439.
Negri, M., Henriques, M., Svidzinski, T. I., Paula, C. R., and Oliveira, R. (2009). Correlation between Etest, disk diffusion, and microdilution methods for antifungal susceptibility testing of Candida species from infection and colonization. J. Clin. Lab. Anal. 23, 324–330. doi: 10.1002/jcla.20337
Ortega, M., Marco, F., Soriano, A., Almela, M., Martínez, J. A., Pitart, C., et al. (2010). Candida spp. bloodstream infection: influence of antifungal treatment on outcome. J. Antimicrob. Chemother. 65, 562–568. doi: 10.1093/jac/dkp495
Pappas, P. G., Kauffman, C. A., Andes, D., Benjamin, D. K. Jr., Calandra, T. F., Edwards, J. E. Jr., et al. (2009). Clinical practice guidelines for the management of candidiasis. Clin. Infect. Dis. 48, 503–535. doi: 10.1086/596757
Patil, S., Rao, R. S., Majumdar, B., and Anil, S. (2015). Clinical appearance of oral Candida infection and therapeutic strategies. Front. Microbiol. 6:1391. doi: 10.3389/fmicb.2015.01
Pfaller, M. A. (2012). Antifungal drug resistance: mechanisms, epidemiology, and consequences for treatment. Am. J. Med. 125(Suppl. 1), S3–S13. doi: 10.1016/j.amjmed.2011.11.001
Pfaller, M. A., Diekema, D. J., Gibbs, D. L., Newell, V. A., Ellis, D., Tullio, V., et al. (2010). Results from the ARTEMIS DISK global antifungal surveillance study, 1997 to 2007: a 10.5-year analysis of susceptibilities of Candida species to fluconazole and voriconazole as determined by CLSI standardized disk diffusion. J. Clin. Microbiol. 48, 1366–1377. doi: 10.1128/JCM.02117-09
Pfaller, M. A., Diekema, D. J., Gibbs, D. L., Newell, V. A., Nagy, E., Dobiasova, S., et al. (2008). Candida krusei, a multidrug-resistant opportunistic fungal pathogen: geographic and temporal trends from the ARTEMIS DISK antifungal surveillance program, 2001 to 2005. J. Clin. Microbiol. 46, 515–521. doi: 10.1128/JCM.01915-07
Pfaller, M. A., Diekema, D. J., Procop, G. W., and Rinaldi, M. G. (2007). Multicenter comparison of the VITEK 2 antifungal susceptibility test with the CLSI broth microdilution reference method for testing amphotericin B, flucytosine, and voriconazole against Candida spp. J. Clin. Microbiol. 45, 3522–3528. doi: 10.1128/JCM.00403-07
Pfaller, M. A., Messer, S. A., Houston, A., Rangel-Frausto, M. S., Wiblin, T., Blumberg, H. M., et al. (1998). National epidemiology of mycoses survey: a multicenter study of strain variation and antifungal susceptibility among isolates of Candida species. Diagn. Microbiol. Infect. Dis. 31, 289–296.
Rautemaa, R., and Ramage, G. (2011). Oral candidosis – clinical challenges of a biofilm disease. Crit. Rev. Microbiol. 37, 328–336. doi: 10.3109/1040841X.2011.585606
Rex, J. H., Walsh, T. J., Sobel, J. D., Filler, S. G., Pappas, P. G., Dismukes, W. E., et al. (2000). Practice guidelines for the treatment of candidiasis. Clin. Infect. Dis. 30, 662–678. doi: 10.1086/313749
Sanitá, P. V., Mima, E. G. O., Pavarina, A. C., Jorge, J. H., Machado, A. L., and Vergani, C. E. (2013). Susceptibility profile of a Brazilian yeast stock collection of Candida species isolated from subjects with Candida-associated denture stomatitis with or without diabetes. Oral Med. 116, 562–569. doi: 10.1016/j.oooo.2013.07.002
Sant’Ana, P. L., Milan, E. P., Martinez, R., Telles, F. Q., Ferreira, M. S., Alcântara, A. P., et al. (2002). Multicenter Brazilian study of oral Candida species isolated from AIDS patients. Mem. Inst. Oswaldo Cruz 97, 253–257. doi: 10.1590/S0074-02762002000200019
Sharma, G., Pai, K. M., Setty, S., Ramapuram, J. T., and Nagpal, A. (2009). Oral manifestations as predictors of immune suppression in a HIV-/AIDS-infected population in south India. Clin. Oral Investig. 13, 141–148. doi: 10.1007/s00784-008-0210-z
Siikala, E., Rautemaa, R., Richardson, M., Saxen, H., Bowyer, P., and Sanglard, D. (2010). Persistent Candida albicans colonization and molecular mechanisms of azole resistance in autoimmunepolyendocrinopathy-candidiasis-ectodermal dystrophy (APECED) patients. J. Antimicrob. Chemother. 65, 2505–2513. doi: 10.1093/jac/dkq354
Swinne, D., Watelle, M., Van der Flaes, M., and Nolard, N. (2004). In vitro activities of voriconazole (UK-109, 496), fluconazole, itraconazole and amphotericin B against 132 non-albicans bloodstream yeast isolates (CANARI study). Mycoses 47, 177–183. doi: 10.1111/j.1439-0507.2004.00971.x
Keywords: HIV, AIDS, antifungals, Candida, oropharyngeal candidiasis
Citation: Terças ALG, Marques SG, Moffa EB, Alves MB, de Azevedo CMPS, Siqueira WL and Monteiro CA (2017) Antifungal Drug Susceptibility of Candida Species Isolated from HIV-Positive Patients Recruited at a Public Hospital in São Luís, Maranhão, Brazil. Front. Microbiol. 8:298. doi: 10.3389/fmicb.2017.00298
Received: 04 October 2016; Accepted: 14 February 2017;
Published: 02 March 2017.
Edited by:
Octavio Luiz Franco, Universidade Católica de Brasília, BrazilReviewed by:
Nádia Skorupa Parachin, University of Brasília, BrazilSonia Rozental, Federal University of Rio de Janeiro, Brazil
Copyright © 2017 Terças, Marques, Moffa, Alves, de Azevedo, Siqueira and Monteiro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina A. Monteiro, cristina.monteiro@ceuma.br Eduardo B. Moffa, du_moffa@yahoo.com.br