 Bei Jiang1
Bei Jiang1 Supeng Yin1Bo You1
Supeng Yin1Bo You1 Guangtao Huang1Zichen Yang1Yulong Zhang1Yu Chen1Jing Chen1
Guangtao Huang1Zichen Yang1Yulong Zhang1Yu Chen1Jing Chen1 Zhiqiang Yuan1
Zhiqiang Yuan1 Xiancai Rao2
Xiancai Rao2 Xiaomei Hu2Yali Gong1*Yizhi Peng1*
Xiaomei Hu2Yali Gong1*Yizhi Peng1*- 1State Key Laboratory of Trauma, Burns and Combined Injury, Institute of Burn Research, Southwest Hospital, Third Military Medical University, Chongqing, China
- 2Department of Microbiology, College of Basic Medical Sciences, Third Military Medical University, Chongqing, China
Methicillin-resistant Staphylococcus aureus (MRSA) infections are prevalent in burn wards, and are especially serious in S. aureus bacteremia (SAB) patients. Glycopeptides and daptomycin are effective against MRSA infections, but MIC creeps can reduce their efficacy. Our object was to perform a molecular epidemiological investigation of S. aureus isolates in our burn center and to evaluate MICs for antimicrobials against SAB-associated MRSA isolates. A total of 259 S. aureus isolates, obtained from August 2011 to July 2016, were used in this study. Multiple molecular typing was used for molecular epidemiological analysis. E-tests were used to determine MICs of vancomycin, teicoplanin, and daptomycin for SAB-associated MRSA isolates. MIC values were stratified by collection date or source and compared. Spearman's test was used to analyze MICs correlations amongst tested antimicrobials. ST239-MRSA-III-t030-agrI clone was found to be dominant in both SAB and non-SAB patients, and significantly more in SAB patients (P < 0.0001). SAB-MRSA isolates exhibited decreased MICs for vancomycin, teicoplanin, and daptomycin during the 5-year period. Compared to those isolated from catheters or wounds, SAB-MRSA isolates from the bloodstream were less susceptible to vancomycin and daptomycin, but more susceptible to teicoplanin. MICs Correlation was found only between vancomycin and daptomycin in MRSA isolates from the bloodstream (rho = 0.250, P = 0.024). In conclusion, our results suggest that MRSA infections are still serious problems in burn centers. In contrast to most other studies, we observed increased susceptibility to glycopeptides and daptomycin against SAB-associated MRSA in our center from 2011 to 2016, suggesting the use of glycopeptides does not lead to MIC creeps. Isolates from different sites of the body may exhibit different levels of susceptibility and change trend over time for different antimicrobials, antimicrobials selection for MRSA infections should be considered comprehensively.
Introduction
Staphylococcus aureus is an important human pathogen that causes infections at diverse sites in the body (Rasigade and Vandenesch, 2014), it is also the most frequently isolated Gram-positive bacterial species from burn patients (Song et al., 2001; Bayram et al., 2013). In recent years, S. aureus has attracted particular attention because of the prevalence of methicillin-resistant S. aureus (MRSA), which poses a serious public health risk (Cheng et al., 2013; Carrel et al., 2015). The concern is even greater in patients suffering burn-associated infections, since the isolation rate for MRSA in burn wards is much higher than in the general hospital population and the resistance to antimicrobials is more dangerous (Bahemia et al., 2015; Motallebi et al., 2016). Multiple molecular typing based on MRSA detection, staphylococcal cassette chromosome mec (SCCmec) typing, multilocus sequence typing (MLST), spa typing, and agr grouping was usually used in molecular epidemiological investigation for S. aureus (Cheng et al., 2013). In China, ST239-MRSA-III-t030-agrI is the most prevalent and persistent MRSA clone, and is a major challenge to clinical anti-infection therapy (Cheng et al., 2013; Li et al., 2013). Several factors contribute to its successful adaptation and survival. The clone often carries the portable SCCmec III, which can transfer drug resistance genes (Cheng et al., 2013). In addition, the ST239 clone may have adaptations that confer enhanced antimicrobial resistance (Cha et al., 2005; Chen et al., 2014), and ST239-MRSA is more likely to be classified as a heterogeneous vancomycin-intermediate S. aureus (hVISA) (Hu et al., 2015).
S. aureus bacteremia (SAB) is a common and severe infection (Naber, 2009). It is associated with high mortality and represents a major burden to both the patient and the health care system, especially when life-threatening complications such as infective endocarditis and metastatic infections occur (Naber, 2009). Due to susceptible factors such as loss of the skin barrier, immune deficiency, and the use of invasive catheters and monitoring devices, SAB in burn patients occurs more frequently, and is extremely serious in cases involving MRSA-associated SAB (Gang et al., 2000; Bahemia et al., 2015).
Vancomycin, a glycopeptide antimicrobial, has been in clinical use globally for over 50 years, and still serves as a first-line drug for treatment of SAB caused by MRSA (Choo and Chambers, 2016). However, many recent studies have documented an increase in the minimum inhibitory concentration (MIC) for vancomycin over time (“MIC creep”) (Steinkraus et al., 2007; Chang et al., 2015). Because vancomycin MIC creep is thought to be a potential contributor to increased treatment failure and mortality, new agents for effective therapy against MRSA are urgently needed (Chang et al., 2015; Choo and Chambers, 2016). In the USA, daptomycin, a lipopeptide class antimicrobial, is available as an effective alternative for invasive MRSA infection (Humphries et al., 2013). Daptomycin is seldom used in China primarily because its high cost is not reimbursed by medical insurance. Although the drug may have a promising market and widespread application in China, several studies have reported a correlation between vancomycin and daptomycin MICs, suggesting that decreased vancomycin susceptibility is linked to decreased susceptibility to daptomycin (Hsieh et al., 2016; San-Juan et al., 2016). If this is indeed the case, it will restrict the utility of daptomycin in China in the future. Teicoplanin is another glycopeptide antimicrobial used for serious infections caused by MRSA (Choo and Chambers, 2016). While having not been approved for use in the USA, it is used as commonly as vancomycin in Europe and many hospitals in China, and exhibits an efficacy comparable to vancomycin (Chang et al., 2012; Choo and Chambers, 2016). Decreased teicoplanin susceptibility has also been suggested as a contributor to treatment failure of MRSA infections (Chang et al., 2012). Because MIC creeps may affect the prognosis of MRSA-associated SAB (Chang et al., 2012, 2015), for clinical MRSA isolates, the evaluation of MICs for glycopeptides and daptomycin over time is a high priority.
In this study, we first analyzed the molecular epidemiological characteristics of clinical S. aureus isolates from SAB and non-SAB patients in our center. Since our result suggested that SAB patients presented significantly more ST239-MRSA-III-t030-agrI infections, we determined MICs for all the MRSA isolates from SAB patients using E-tests, and evaluated antimicrobial MICs of these isolates according to their collection dates and sources. The tested antimicrobials included vancomycin and teicoplanin, the two most commonly used glycopeptides in our center. Daptomycin, which is never used in our hospital, was also tested to analyze the correlation of MICs amongst the three antimicrobials.
Patients and Methods
Ethics Statement
The study was approved by the Committee of the First Affiliated Hospital of Third Military Medical University, China. No written informed consent was required because all the patients were anonymous and any other personal information was not used in this study.
Study Design and Bacterial Isolates
This study was conducted in the 150-bed burn center of Southwest Hospital in China. From August 2011 to July 2016, 259 clinical isolates derived from SAB and non-SAB patients were enrolled for analysis. Strains from SAB patients were isolated from the bloodstream (group BB), catheters (group CB), or wounds (group WB), the three sites where S. aureus was most commonly isolated from SAB patients in our center. All patients in groups CB and WB were included in group BB. Strains from non-SAB patients were isolated from wounds (group WN), the most common infection site in burn patients. The numbers of isolates in each group and collection dates are summarized in Table 1. All isolates were identified as S. aureus by phenotypic methods (API staphy system, Biomerieux) and confirmed by PCR amplification of the femB gene. SAB was defined as an episode of fever with at least one peripherally-drawn blood culture that was positive for S. aureus (Ponce-De-Leon et al., 2010). Only the first positive culture in the course of infection was enrolled for analysis.
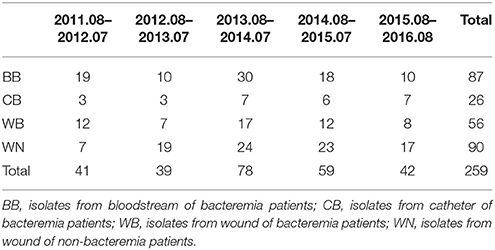
Table 1. Distribution of isolates based on source and sampling time.
Molecular Typing
MRSA was identified by duplex PCR using femB and mecA as reference genes (Kobayashi et al., 1994). SCCmec typing of MRSA was performed using four unique and specific pairs of primers as described previously (Kondo et al., 2007). For MLST, ST239 strains were first screened using two sets of primers designed by Feil et al. (2008). Other sequence types (STs) were determined by PCR amplification of seven housekeeping genes (arcC, aroE, glpF, gmk, pta, tpi, and yqil), the reaction products were sequenced and aligned to sequences available at the Multi Locus Sequence Typing website (http://saureus.mlst.net/) (Cheng et al., 2013). The spa type was identified by amplifying and sequencing the polymorphic X-region of the spa gene (Harmsen et al., 2003). The agr group was identified by PCR using one common and four specific primers, followed by electrophoresis, as previously described (Bardiau et al., 2016).
Antimicrobial Susceptibility Tests
All MRSA isolates from SAB patients were tested for susceptibility to vancomycin, teicoplanin, and daptomycin by standard E-test according to the manufacturer's guidelines (bioMérieux, France). All E-test results were visually read by two independent observers, who were blinded to each other and to the grouping situations. Interpretive standards for antimicrobial susceptibility followed criteria established by the Clinical and Laboratory Standards Institute (CLSI). S. aureus ATCC 29213 was used as the control strain.
Statistical Analysis
IBM SPSS Statistics 19.0 (IBM, Chicago, IL, USA) and GraphPad Prism 6.0 software (San Diego, CA, USA) were used for statistical analysis. We used Student's t-test to compare continuous variables, and χ2 test to compare categorical variations. Correlations between E-test MICs were calculated using Spearman's rho (ρ) test. All statistical tests were two-sided and the threshold for statistical significance was P < 0.05.
Results
Molecular Epidemiological Characteristics of S. aureus Isolates in the Burn Center
A total of 239 MRSA isolates (239/259, 92.28%) were identified from patients in our burn center. As shown in Table 2, MRSA was significantly more frequently isolated from SAB patients than from non-SAB patients (95.86 vs. 85.56%, respectively; P = 0.0031). Overwhelming majority of MRSA isolates were classified as SCCmec III (230/239, 96.23%). ST239 was the predominant MLST type (238/259, 91.89%), and was more likely to be isolated from SAB patients (95.86 vs. 84.44%, respectively; P = 0.0014). The spa type t030 (93.49 vs. 77.78%, respectively; P = 0.0002) and agr group I (99.41 vs. 94.44%, respectively; P = 0.0362) were also significantly more abundant in SAB patients. For isolates from wounds, the most common isolation site for S. aureus in burn wards, SAB patients were more likely to be infected by the ST239-MRSA-t030 clone compared to non-SAB patients. The ST239-MRSA-III-t030-agrI clone, the most prevalent MRSA clone in China and closely related to antimicrobial resistance (Cheng et al., 2013; Li et al., 2013), was significantly more frequent in SAB patients (92.90 vs. 70.00%, respectively; P < 0.0001).
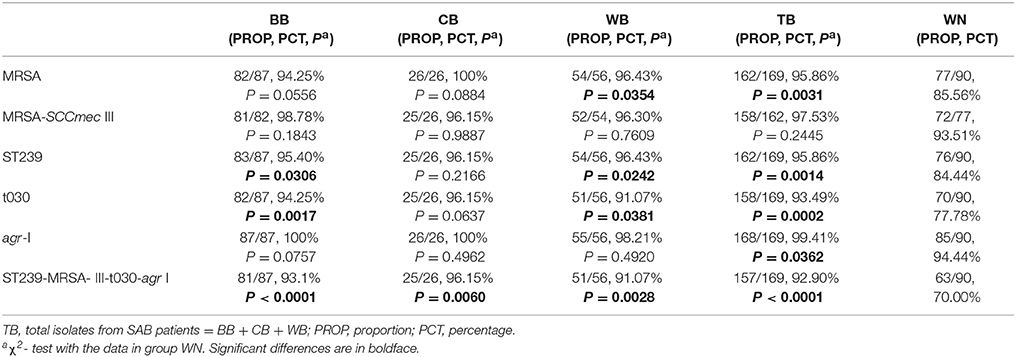
Table 2. Molecular epidemiological characteristics of enrolled isolates.
Susceptibility of SAB-Associated MRSA Isolates to Vancomycin, Teicoplanin, and Daptomycin, Stratified by Collection Dates and Sources
Because SAB is a dangerous infection in burn patients, and infections caused by clone ST239-MRSA-III-t030-agrI are significantly more frequent in SAB patients in our center, we sought to evaluate MICs for the three important antimicrobials against MRSA (vancomycin, teicoplanin, and daptomycin) amongst SAB-associated MRSA isolates. No resistant, intermediate-resistant or non-susceptible strain for any of the three antimicrobials was identified. When these MRSA isolates were stratified by collection dates, we were surprised to find that the susceptibility to vancomycin, teicoplanin, and daptomycin all tended to increase during the 5-year period (Table 3). Comparing to the data in the first 3 years, MIC50 values of vancomycin and teicoplanin, MIC50 and MIC90 values of daptomycin all decreased in the last 2 years. MICGM values and percentages of isolates with MIC > median values for the three antimicrobials all significantly decreased, especially for vancomycin (P = 0.0018 and P = 0.0002) and teicoplanin (P < 0.0001 and P < 0.0001), despite their frequent use for MRSA infections in our center.
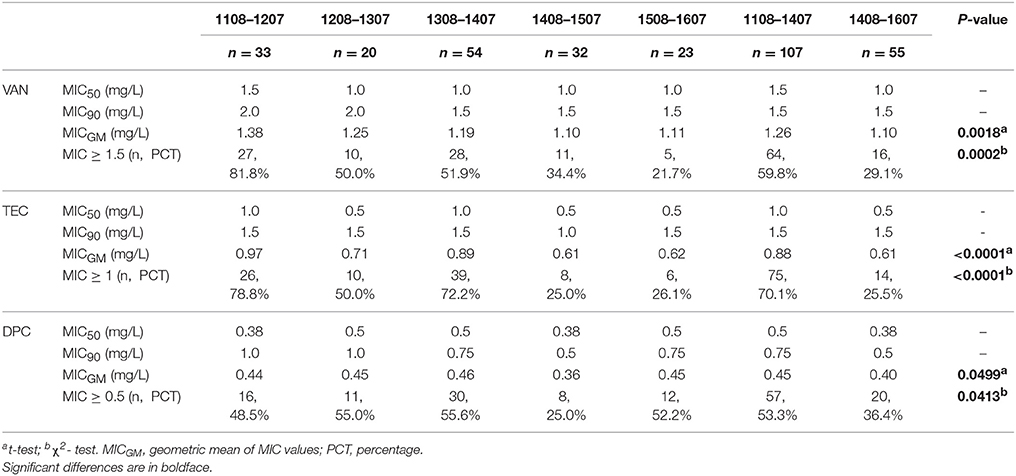
Table 3. Susceptibility of SAB-MRSA to vancomycin, teicoplanin, and daptomycin, stratified by collection date.
SAB-MRSA isolates from different sources presented different susceptibility profiles. As shown in Table 4, although no statistical difference was found, MRSA isolates from the bloodstream were less susceptible to vancomycin, reflected by higher values for MIC50, MICGM, and the percentage of isolates with MIC > 1.5 mg/L (median value). In contrast, MRSA isolates from the bloodstream were more susceptible to teicoplanin. MIC50, MIC90, MICGM, and the proportion of isolates with MIC > 1 mg/L (median value) were all lower in group BB. A t-test showed significantly lower teicoplanin MIC values in group BB compared to group CB (P = 0.0415) or WB (P = 0.0328). Susceptibility patterns of daptomycin and vancomycin were similar. Significant differences were observed between the MIC values (P = 0.0030) and the percentages of isolates with MIC > 0.5 mg/L (P = 0.0295) between group BB and WB.
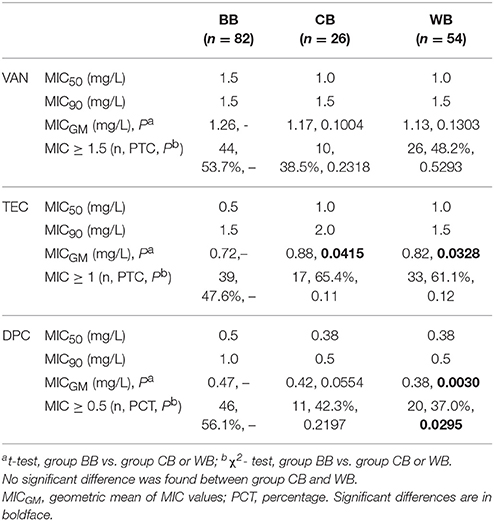
Table 4. Susceptibility of SAB-MRSA to vancomycin, teicoplanin, and daptomycin, stratified by source.
Correlation of MICs amongst Vancomycin, Teicoplanin, and Daptomycin
Vancomycin MIC exhibited a trend of correlation with daptomycin MIC in SAB-MRSA isolates (Spearman's rho = 0.140, P = 0.076). Further analysis revealed that the two MICs were correlated significantly only for isolates from the bloodstream (Spearman's rho = 0.250, P = 0.024). In addition, correlations were not found between teicoplanin and daptomycin MICs, or between vancomycin and teicoplanin MICs (Table 5).
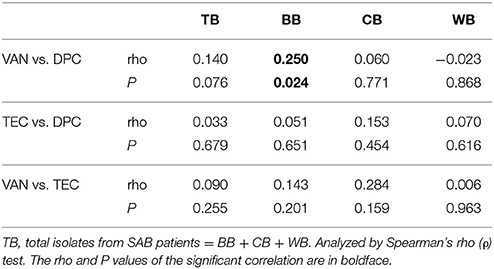
Table 5. Correlation analysis amongst vancomycin, teicoplanin, and daptomycin.
Discussion
Multiple molecular typing of S. aureus is an important tool in epidemiological studies and is useful for the monitoring and control of infection (Cheng et al., 2013). In this work, we first analyzed S. aureus isolates from SAB and non-SAB patients in our burn center over a 5-year period. We found that the overall prevalence rate of MRSA in our center was high (92.28%). This result was similar to burn survey reports by Song et al. (98%) from Korea (Song et al., 2001), Khosravi et al. (87.4%), and Parhizgari et al. (86.4%) from Iran (Khosravi et al., 2012; Parhizgari et al., 2016), but higher than that reported by Chen et al. (55.3%) from southeast China (Chen et al., 2012). In contrast to the molecular typing results of other common bacteria from burn patients, such as Acinetobacter baumannii and Pseudomonas aeruginosa, which often display diverse molecular types (Huang et al., 2016; de Almeida Silva et al., 2017), the molecular types of S. aureus in burn wards were typically simple according to previous studies (Chen et al., 2012; Parhizgari et al., 2016). In our center, almost all the MRSA strains carried SCCmec III (96.23%), which is a characteristic of nosocomial MRSA strains and is associated with the capacity to resist antimicrobials (Cheng et al., 2013). The dominant MLST type was ST239 [91.89%, (162+76)/259], suggesting its strong ability to adapt and persist, as mentioned previously (Table 2) (Cha et al., 2005; Chen et al., 2014). The circulation of limited number of S. aureus clones in burn wards may be due mainly to the compromised skin barrier, poor conditions of burn patients, and the strong adaptability of specific S. aureus clones. This underscores the importance of placing more emphasis on disinfection of burn wards and patients to eradicate or restrict circulating bacteria.
According to our results, SAB patients were significantly more likely to be infected by MRSA (P = 0.0031) and clone ST239-MRSA-III-t030-agrI (P < 0.0001) (Table 2). The latter is considered the most prevalent hospital-acquired MRSA clone in China, and is closely associated with antimicrobial resistance (Cheng et al., 2013; Li et al., 2013). Its presence places burn patients with SAB at greater risk, and makes it more difficult to cure SAB infections. Moreover, if MIC creeps occurs, the situation may get worse (Chang et al., 2015; Choo and Chambers, 2016). MIC creeps to glycopeptides and daptomycin have been widely reported. Chang et al. found that the percentage of isolates with a vancomycin MIC of 1 mg/L increased significantly from 2006 (37.0%) to 2010 (75.7%) in a Chinese hospital, and the high vancomycin MIC was associated with a higher failure rate of anti-infection therapy in these patients (Chang et al., 2015). Increased vancomycin MICs to MRSA were also reported by Steinkraus et al. (2007) and Wang et al. (2006) in their 5-year studies in the USA. Hsieh et al. also observed MIC creeps of MRSA to vancomycin, teicoplanin, and daptomycin in an 11-year period study (Hsieh et al., 2016). However, some studies did not find an upward MIC creep. Sancak et al. demonstrated that the distribution of MICs for vancomycin and daptomycin was stable in an 11-year period (Sancak et al., 2013). Reynolds et al. did not find an upward creep for vancomycin or teicoplanin in the UK and Ireland (Reynolds et al., 2012). To our best knowledge, decreasing MIC trends were rarely reported by now. Steinkraus et al. reported that daptomycin MICs to MRSA significantly decreased from 2001 to 2005 in a medical center (Steinkraus et al., 2007). Lu et al. found that vancomycin MICs among MRSA isolates in a Chinese tertiary hospital decreased in a 12-year period (Lu et al., 2016). However, drug usage information was not mentioned or could not be acquired in the two studies. In this study, vancomycin and teicoplanin were used in almost all the MRSA-SAB patients in our center, while daptomycin was never used. Our results showed that, all the three antimicrobials exhibited significant MICs decreases during the 5-year period, especially teicoplanin (P < 0.0001). These results suggest that long-term use of glycopeptides (vancomycin and teicoplanin) does not necessarily lead to upward MIC creeps for glycopeptides or daptomycin, which are consistent with Lu et al.'s (2016) and Steinkraus et al.'s (2007) studies, but contrast to most other studies. Infection types, enforcement of guidelines for the reasonable use of antimicrobials, time and dosage for antimicrobials administration may contribute to the MIC trends. More detailed and in-depth investigation is needed to explain why different MIC trends were observed in different studies, and this will provide greatly useful guidance for antimicrobials administration.
In burn patients with SAB, wound infection was considered as the major cause of invasive infection into the bloodstream (Pruitt et al., 1998), but previous studies did not evaluate the MICs of SAB isolates from different sites of the body. The present study showed that strains isolated from different sites in SAB patients present different susceptibility profiles to glycopeptides and daptomycin. In our results, MRSA isolates from the bloodstream exhibited decreased susceptibility to both vancomycin and daptomycin, compared to those isolated from catheters or wounds. Intriguingly, teicoplanin MICs showed an opposite trend. MIC values (P < 0.0001), and the number of isolates with MIC ≥ 1 mg/L (P < 0.0001), were both significantly lower in bloodstream isolates (Table 4). Our results suggest that teicoplanin may be a better choice for MRSA infections from the bloodstream. To efficiently defeat MRSA infections, clinicians should select drugs based on the susceptibility tests of bacteria isolated from different sites in the patient.
The correlations amongst MICs for vancomycin, teicoplanin, and daptomycin have been reported previously (Shoji et al., 2015; Hsieh et al., 2016; San-Juan et al., 2016). Hsieh et al. found that the vancomycin MIC was significantly correlated with teicoplanin, daptomycin, and teicoplanin MICs (Hsieh et al., 2016). Shoji et al. also observed that the vancomycin MIC was significantly correlated with MICs for both teicoplanin and daptomycin (Shoji et al., 2015). San-Juan et al. found a correlation between high MICs for vancomycin (>1.5 mg/L) and daptomycin (>0.5 mg/L) (San-Juan et al., 2016). These correlations may restrict the use of related drugs when one drug becomes less susceptible. In our results, although the three antimicrobials presented similar MIC trends over time, no significant correlation was found except between vancomycin and daptomycin in group BB (P = 0.024) (Table 5). Interestingly, consistent with this result, most previously reported correlations amongst these drugs were found in bloodstream isolates (Shoji et al., 2015; San-Juan et al., 2016). Our data suggest that decreased vancomycin susceptibility probably restricts the usage of daptomycin in anti-MRSA therapy, but only for bloodstream-associated infections.
In conclusion, we found that MRSA infections are serious in the center and ST239-MRSA-III-t030-agrI clone is significantly dominated in SAB patients. In contrast with most other reports, although vancomycin and teicoplanin are frequently used in our center, the increasing susceptibility to the two glycopeptides and daptomycin over time was observed, suggesting that the application of glycopeptides does not necessarily lead to MIC creeps. SAB-MRSA isolates from different body sites presented different susceptibility profiles, indicating antimicrobials selection in anti-infection therapy should be considered comprehensively. MICs correlation was found only between vancomycin and daptomycin amongst bloodstream MRSA isolates, suggesting that the usage of daptomycin may be restricted in treating MRSA-associated bloodstream infections if decreased vancomycin susceptibility occurs.
Author Contributions
YP and YG conceived and designed this study. BJ, SY, and BY carried out the experiments, collected and analyzed the data. GH, ZiY, YZ, YC, and JC helped with the data interpretation. ZhY, XR, and XH drafted the manuscript. All authors have read and approved the final manuscript.
Funding
This work was supported by the National Natural Science Foundation of China (grant numbers 81772073, 81571896, and 31570127).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Bahemia, I. A., Muganza, A., Moore, R., Sahid, F., and Menezes, C. N. (2015). Microbiology and antibiotic resistance in severe burns patients: a 5 year review in an adult burns unit. Burns 41, 1536–1542. doi: 10.1016/j.burns.2015.05.007
Bardiau, M., Caplin, J., Detilleux, J., Graber, H., Moroni, P., Taminiau, B., et al. (2016). Existence of two groups of Staphylococcus aureus strains isolated from bovine mastitis based on biofilm formation, intracellular survival, capsular profile and agr-typing. Vet. Microbiol. 185, 1–6. doi: 10.1016/j.vetmic.2016.01.003
Bayram, Y., Parlak, M., Aypak, C., and Bayram, I. (2013). Three-year review of bacteriological profile and antibiogram of burn wound isolates in Van, Turkey. Int. J. Med. Sci. 10, 19–23. doi: 10.7150/ijms.4723
Carrel, M., Perencevich, E. N., and David, M. Z. (2015). USA300 methicillin-resistant Staphylococcus aureus, United States, 2000-2013. Emerg. Infect. Dis. 21, 1973–1980. doi: 10.3201/eid2111.150452
Cha, H. Y., Moon, D. C., Choi, C. H., Oh, J. Y., Jeong, Y. S., Lee, Y. C., et al. (2005). Prevalence of the ST239 clone of methicillin-resistant Staphylococcus aureus and differences in antimicrobial susceptibilities of ST239 and ST5 clones identified in a Korean hospital. J. Clin. Microbiol. 43, 3610–3614. doi: 10.1128/JCM.43.8.3610-3614.2005
Chang, H. J., Hsu, P. C., Yang, C. C., Siu, L. K., Kuo, A. J., Chia, J. H., et al. (2012). Influence of teicoplanin MICs on treatment outcomes among patients with teicoplanin-treated methicillin-resistant Staphylococcus aureus bacteraemia: a hospital-based retrospective study. J. Antimicrob. Chemother. 67, 736–741. doi: 10.1093/jac/dkr531
Chang, W., Ma, X., Gao, P., Lv, X., Lu, H., and Chen, F. (2015). Vancomycin MIC creep in methicillin-resistant Staphylococcus aureus (MRSA) isolates from 2006 to 2010 in a hospital in China. Indian J. Med. Microbiol. 33, 262–266. doi: 10.4103/0255-0857.148837
Chen, C. J., Huang, Y. C., Su, L. H., Wu, T. L., Huang, S. H., Chien, C. C., et al. (2014). Molecular epidemiology and antimicrobial resistance of methicillin-resistant Staphylococcus aureus bloodstream isolates in Taiwan, 2010. PLoS ONE 9:e101184. doi: 10.1371/journal.pone.0101184
Chen, X., Yang, H. H., Huangfu, Y. C., Wang, W. K., Liu, Y., Ni, Y. X., et al. (2012). Molecular epidemiologic analysis of Staphylococcus aureus isolated from four burn centers. Burns 38, 738–742. doi: 10.1016/j.burns.2011.12.023
Cheng, H., Yuan, W., Zeng, F., Hu, Q., Shang, W., Tang, D., et al. (2013). Molecular and phenotypic evidence for the spread of three major methicillin-resistant Staphylococcus aureus clones associated with two characteristic antimicrobial resistance profiles in China. J. Antimicrob. Chemother. 68, 2453–2457. doi: 10.1093/jac/dkt213
Choo, E. J., and Chambers, H. F. (2016). Treatment of methicillin-resistant Staphylococcus aureus bacteremia. Infect. Chemother. 48, 267–273. doi: 10.3947/ic.2016.48.4.267
de Almeida Silva, K. C., Calomino, M. A., Deutsch, G., De Castilho, S. R., De Paula, G. R., Esper, L. M., et al. (2017). Molecular characterization of multidrug-resistant (MDR) Pseudomonas aeruginosa isolated in a burn center. Burns 43, 137–143. doi: 10.1016/j.burns.2016.07.002
Feil, E. J., Nickerson, E. K., Chantratita, N., Wuthiekanun, V., Srisomang, P., Cousins, R., et al. (2008). Rapid detection of the pandemic methicillin-resistant Staphylococcus aureus clone ST 239, a dominant strain in Asian hospitals. J. Clin. Microbiol. 46, 1520–1522. doi: 10.1128/JCM.02238-07
Gang, R. K., Sanyal, S. C., Bang, R. L., Mokaddas, E., and Lari, A. R. (2000). Staphylococcal septicaemia in burns. Burns 26, 359–366. doi: 10.1016/S0305-4179(99)00170-9
Harmsen, D., Claus, H., Witte, W., Rothganger, J., Claus, H., Turnwald, D., et al. (2003). Typing of methicillin-resistant Staphylococcus aureus in a university hospital setting by using novel software for spa repeat determination and database management. J. Clin. Microbiol. 41, 5442–5448. doi: 10.1128/JCM.41.12.5442-5448.2003
Hsieh, Y. C., Lin, Y. C., and Huang, Y. C. (2016). Vancomycin, teicoplanin, daptomycin, and linezolid MIC creep in methicillin-resistant Staphylococcus aureus is associated with clonality. Medicine 95:e5060. doi: 10.1097/MD.0000000000005060
Hu, H. C., Kao, K. C., Chiu, L. C., Chang, C. H., Hung, C. Y., Li, L. F., et al. (2015). Clinical outcomes and molecular typing of heterogenous vancomycin-intermediate Staphylococcus aureus bacteremia in patients in intensive care units. BMC Infect. Dis. 15:444. doi: 10.1186/s12879-015-1215-2
Huang, G., Yin, S., Gong, Y., Zhao, X., Zou, L., Jiang, B., et al. (2016). Multilocus sequence typing analysis of carbapenem-resistant Acinetobacter baumannii in a Chinese burns institute. Front. Microbiol. 7:1717. doi: 10.3389/fmicb.2016.01717
Humphries, R. M., Pollett, S., and Sakoulas, G. (2013). A current perspective on daptomycin for the clinical microbiologist. Clin. Microbiol. Rev. 26, 759–780. doi: 10.1128/CMR.00030-13
Khosravi, A. D., Hoveizavi, H., and Farshadzadeh, Z. (2012). The prevalence of genes encoding leukocidins in Staphylococcus aureus strains resistant and sensitive to methicillin isolated from burn patients in Taleghani Hospital, Ahvaz, Iran. Burns 38, 247–251. doi: 10.1016/j.burns.2011.08.002
Kobayashi, N., Wu, H., Kojima, K., Taniguchi, K., Urasawa, S., Uehara, N., et al. (1994). Detection of mecA, femA, and femB genes in clinical strains of staphylococci using polymerase chain reaction. Epidemiol. Infect. 113, 259–266. doi: 10.1017/S0950268800051682
Kondo, Y., Ito, T., Ma, X. X., Watanabe, S., Kreiswirth, B. N., Etienne, J., et al. (2007). Combination of multiplex PCRs for staphylococcal cassette chromosome mec type assignment: rapid identification system for mec, ccr, and major differences in junkyard regions. Antimicrob. Agents Chemother. 51, 264–274. doi: 10.1128/AAC.00165-06
Li, T., Song, Y., Zhu, Y., Du, X., and Li, M. (2013). Current status of Staphylococcus aureus infection in a central teaching hospital in Shanghai, China. BMC Microbiol. 13:153. doi: 10.1186/1471-2180-13-153
Lu, C., Guo, Y., Wang, S., Wang, Z., Chen, L., Lv, J., et al. (2016). Decreased vancomycin MICs among methicillin-resistant Staphylococcus aureus clinical isolates at a chinese tertiary hospital over a 12-year period. Front. Microbiol. 7:1714. doi: 10.3389/fmicb.2016.01714
Motallebi, M., Jabalameli, F., Asadollahi, K., Taherikalani, M., and Emaneini, M. (2016). Spreading of genes encoding enterotoxins, haemolysins, adhesin and biofilm among methicillin resistant Staphylococcus aureus strains with staphylococcal cassette chromosome mec type IIIA isolated from burn patients. Microb. Pathog. 97, 34–37. doi: 10.1016/j.micpath.2016.05.017
Naber, C. K. (2009). Staphylococcus aureus bacteremia: epidemiology, pathophysiology, and management strategies. Clin. Infect. Dis. 48(Suppl. 4), S231–S237. doi: 10.1086/598189
Parhizgari, N., Khoramrooz, S. S., Malek Hosseini, S. A., Marashifard, M., Yazdanpanah, M., Emaneini, M., et al. (2016). High frequency of multidrug-resistant Staphylococcus aureus with SCCmec type III and Spa types t037 and t631 isolated from burn patients in southwest of Iran. APMIS 124, 221–228. doi: 10.1111/apm.12493
Ponce-De-Leon, A., Camacho-Ortiz, A., Macias, A. E., Landin-Larios, C., Villanueva-Walbey, C., Trinidad-Guerrero, D., et al. (2010). Epidemiology and clinical characteristics of Staphylococcus aureus bloodstream infections in a tertiary-care center in Mexico City: 2003-2007. Rev. Invest. Clin. 62, 553–559.
Pruitt, B. A. Jr., Mcmanus, A. T., Kim, S. H., and Goodwin, C. W. (1998). Burn wound infections: current status. World J. Surg. 22, 135–145. doi: 10.1007/s002689900361
Rasigade, J. P., and Vandenesch, F. (2014). Staphylococcus aureus: a pathogen with still unresolved issues. Infect. Genet. Evol. 21, 510–514. doi: 10.1016/j.meegid.2013.08.018
Reynolds, R., Hope, R., Warner, M., Macgowan, A. P., Livermore, D. M., and Ellington, M. J. (2012). Lack of upward creep of glycopeptide MICs for methicillin-resistant Staphylococcus aureus (MRSA) isolated in the UK and Ireland 2001-07. J. Antimicrob. Chemother. 67, 2912–2918. doi: 10.1093/jac/dks324
Sancak, B., Yagci, S., Mirza, H. C., and Hascelik, G. (2013). Evaluation of vancomycin and daptomycin MIC trends for methicillin-resistant Staphylococcus aureus blood isolates over an 11 year period. J. Antimicrob. Chemother. 68, 2689–2691. doi: 10.1093/jac/dkt247
San-Juan, R., Viedma, E., Chaves, F., Lalueza, A., Fortun, J., Loza, E., et al. (2016). High MICs for vancomycin and daptomycin and complicated catheter-related bloodstream infections with methicillin-sensitive Staphylococcus aureus. Emerg. Infect. Dis. 22, 1057–1066. doi: 10.3201/eid2206.151709
Shoji, H., Maeda, M., Shirakura, T., Takuma, T., Ugajin, K., Fukuchi, K., et al. (2015). More accurate measurement of vancomycin minimum inhibitory concentration indicates poor outcomes in meticillin-resistant Staphylococcus aureus bacteraemia. Int. J. Antimicrob. Agents 46, 532–537. doi: 10.1016/j.ijantimicag.2015.07.013
Song, W., Lee, K. M., Kang, H. J., Shin, D. H., and Kim, D. K. (2001). Microbiologic aspects of predominant bacteria isolated from the burn patients in Korea. Burns 27, 136–139. doi: 10.1016/S0305-4179(00)00086-3
Steinkraus, G., White, R., and Friedrich, L. (2007). Vancomycin MIC creep in non-vancomycin-intermediate Staphylococcus aureus (VISA), vancomycin-susceptible clinical methicillin-resistant S. aureus (MRSA) blood isolates from 2001-05. J. Antimicrob. Chemother. 60, 788–794. doi: 10.1093/jac/dkm258
Keywords: methicillin-resistant Staphylococcus aureus (MRSA), burn, molecular epidemiology, glycopeptides, daptomycin, MIC creep
Citation: Jiang B, Yin S, You B, Huang G, Yang Z, Zhang Y, Chen Y, Chen J, Yuan Z, Rao X, Hu X, Gong Y and Peng Y (2017) A 5-year Survey Reveals Increased Susceptibility to Glycopeptides for Methicillin-Resistant Staphylococcus aureus Isolates from Staphylococcus aureus Bacteremia Patients in a Chinese Burn Center. Front. Microbiol. 8:2531. doi: 10.3389/fmicb.2017.02531
Received: 05 August 2017; Accepted: 05 December 2017;
Published: 14 December 2017.
Edited by:
Tamas Szakmany, Cardiff University, United KingdomReviewed by:
Yan Q. Xiong, University of California, Los Angeles, United StatesZiad Daoud, University of Balamand, Lebanon
Copyright © 2017 Jiang, Yin, You, Huang, Yang, Zhang, Chen, Chen, Yuan, Rao, Hu, Gong and Peng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yali Gong, gyl0804@163.com
Yizhi Peng, yizhipen@sina.com