
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Aging Neurosci., 27 May 2016
Sec. Parkinson’s Disease and Aging-related Movement Disorders
Volume 8 - 2016 | https://doi.org/10.3389/fnagi.2016.00121
 Stefanie Lerche1,2*†Sebastian Heinzel1,2†Guido W. Alves3Paolo Barone4Stefanie Behnke5Yoav Ben-Shlomo6Henk Berendse7Bastiaan R. Bloem8David Burn9Richard Dodel10Donald G. Grosset11Geraldine Hipp12,13Michele T. Hu14Meike Kasten15Rejko Krüger12,13Inga Liepelt-Scarfone1,2Walter Maetzler1,2Marcello Moccia4Brit Mollenhauer16,17Wolfgang Oertel10Benjamin Roeben1,2Uwe Walter18Karin Wirdefeldt19,20Daniela Berg1,2,21
Stefanie Lerche1,2*†Sebastian Heinzel1,2†Guido W. Alves3Paolo Barone4Stefanie Behnke5Yoav Ben-Shlomo6Henk Berendse7Bastiaan R. Bloem8David Burn9Richard Dodel10Donald G. Grosset11Geraldine Hipp12,13Michele T. Hu14Meike Kasten15Rejko Krüger12,13Inga Liepelt-Scarfone1,2Walter Maetzler1,2Marcello Moccia4Brit Mollenhauer16,17Wolfgang Oertel10Benjamin Roeben1,2Uwe Walter18Karin Wirdefeldt19,20Daniela Berg1,2,21Parkinson's disease (PD) is an example for a complex field of research, which is driven by the multifactorial etiology, the heterogeneity in phenotype and the variability in disease progression, as well as the presence of a long pre-diagnostic period, called prodromal PD, lasting up to decades (Postuma et al., 2010). The very slow, so far inevitably progressive, neurodegenerative process and the multidimensional heterogeneity of symptoms in kind (motor and non-motor), time of onset and speed of progression call for prediction markers and progression markers to understand the onset of neurodegeneration and its course. These markers would also help to establish endpoints for neuroprotective treatment strategies aiming to modify disease progression. Because of the complexity, heterogeneity, and the progressive nature of PD, such predictive and progression markers can only be identified in large cohorts and in studies with a longitudinal design. A considerable number of longitudinal cohort studies in PD patients, as well as in individuals at risk, are currently being performed, and extensive effort has gone into the characterization of the individuals assessed. Although each study has its own value and merits, many important research questions cannot be answered as the numbers of participants are too small (e.g., when studying conversion to PD in at-risk populations). Moreover, the pivotal combination of data and findings across studies is hampered by the lack of comparability of symptoms/factors that are being assessed and the specific assessments that are being applied. Therefore, a common approach is needed to enable harmonization and combination of data across studies to define and validate predictive and progression markers.
Based on the need for harmonized assessments of symptoms/markers in PD, the working group: Harmonization of biomarker assessment in longitudinal cohort studies in Parkinson's Disease (BioLoC-PD) of the Joint Programme for Neurodegenerative Diseases (JPND), set out to develop an assessment battery that includes the most useful clinical, laboratory, and brain imaging assessments for (longitudinal) studies in PD.
We here describe the result of the process to find a way to harmonize assessments across studies and propose a modular set of biomarker assessments agreed upon by the group of experts who were included in the working group (all authors of this manuscript).
As a first step, information about the design, markers, and assessments of 21 ongoing cohort studies in various phases of PD represented by members of the JPND working group were collected using a detailed questionnaire. These data served as a basis for the project. Detailed results have been reported previously in Lerche et al. (2015). In a second step, a systematic literature search on assessments and markers in the prodromal and clinical phases of PD was conducted to determine the most useful predictive and progression markers in PD. The outcome of this literature search was combined with the study information derived from the BioLoC-PD studies and the expert clinical knowledge of the principal investigators in their clinical routine. This information were used to establish the proposed assessment battery. A common modular set of biomarker assessments was defined that includes a basic module and different modules for extension, in order to account for the differences in research focus between studies.
Based on the analyses, the JPND BioLoC-PD working group suggests the following three-level modular assessment battery to be implemented in new and whenever possible ongoing longitudinal studies for PD (Figure 1). The set comprises a basic module (demographics, diagnosis, etc.), a minimum function and assessment module and several optional extension modules.
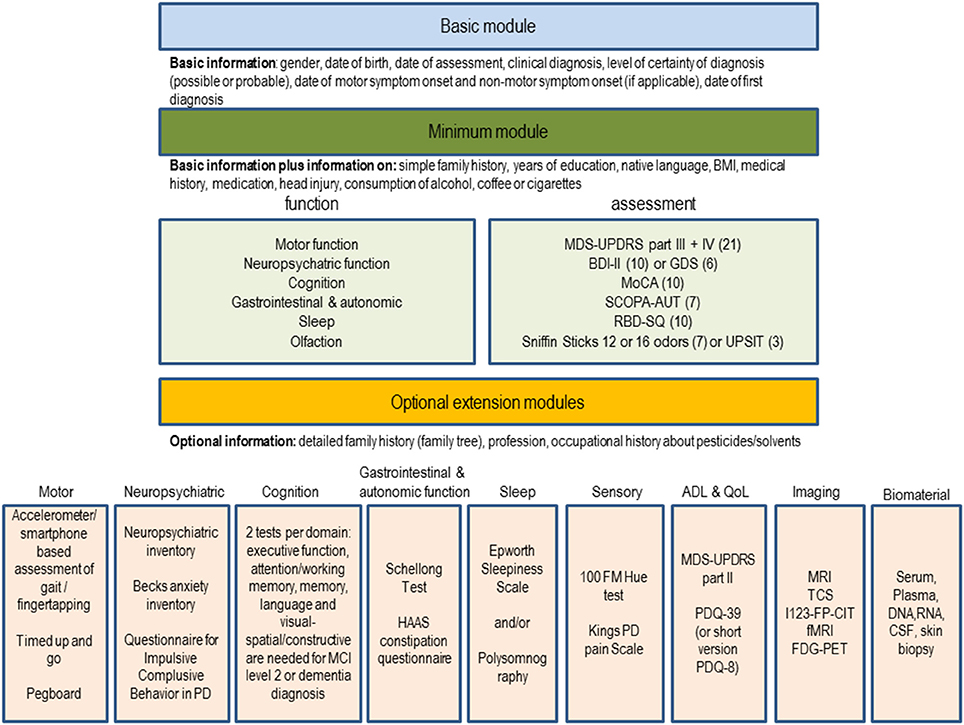
Figure 1. Suggestion for a modular set of biomarker assessments to be used in longitudinal studies in PD. The number of studies using the assessment in the BioLoC-PD consortium are given in brackets.
The basic module is meant to be applied to all participants in longitudinal studies in PD. It may also be applied to existing registers and patients seen routinely in outpatient clinics irrespective of whether they are currently recruited for a longitudinal study. It may also be used for retrospective analyses or identification of potential eligible participants for future randomized controlled trials.
The minimum module is suitable for all individuals participating in at risk, prodromal, and clinical longitudinal studies of PD. The functions of the minimum module are in a descending order (sorted by their use within the BioLoC-PD working group). Functions used in all (risk, prodromal, and clinical) PD studies are at the beginning of each of the lists (in the minimum and extension modules). Modes of assessment of these symptoms are based on the frequency and applicability within studies (easy to apply assessments, which still provide sufficient information were preferred). Each of the assessments suggested for the minimum module (Figure 1) takes no more than 10 min, depending on the cognitive capacity of the study participant. For some functions (neuropsychiatric and olfactory), two optional assessments are suggested from which one can be chosen. This is because they are used in almost equal proportion in ongoing studies and are similarly tolerable for the participants. For the neuropsychiatric function we recommend to use the BDI in prodromal studies and in early stage PD studies and the GDS in late stage PD studies. For olfaction two assessments are given because they are used in almost equal proportion in ongoing studies are similarly tolerable for the participants. However, the first mentioned suggestion, is slightly preferred by the BioLoC-PD consortium (used more often). Regarding the use of the MMSE or MoCA, we found that the MMSE is more often applied in existing studies but for new studies we clearly recommend to use the MoCA.
The optional extension module can be applied to evaluate study participants in more detail. The selection of the additional function modules depends on the main research focus of the study, on the number of study participants and on the available staff and finance. Optional modules can be applied to interesting sub-groups of participants, if financial or pragmatic/practical factors hinder administration to the whole cohort. The assessments included in the extension modules were chosen based on their implementation in the ongoing BioLoC-PD studies. For each subdomain within the extension modules, the most commonly used assessment is suggested in addition to the minimum module (e.g., motor → gait and balance → accelerometer). In case of the imaging module the methods are in a descending order with the one on the top preferred by the BioLoC-PD consortium.
We propose, that each study should as a minimum requirement collect the data specified in the basic module. The basic module is valuable also for genetic or other non-clinical analyses. Once individuals are clinically examined, several motor and non-motor domains should be covered, as suggested in the minimum module which also comprises additional data about medical history. Finally, according to the main research aim of the study, different extension modules can be added.
In general, we provide researchers with suggestions for specific assessment tools/scales to allow comparison across studies. For the cognition module, however, it is less important which assessments are used rather, it is important to take a minimum of two tests per domain for a sensitive and specific diagnosis of dementia and Mild Cognitive Impairment (MCI) level II (Goldman et al., 2015). For cognitive analyses, a comparison of studies with different assessments will then be possible by comparing the domain z-scores (Aarsland et al., 2010), equipercentile or item response theory modeling or by using existing conversion algorithms (e.g., conversion between the MMSE and MOCA tests (Lawton et al., 2016)). A list of neuropsychological tests suitable for the optional cognitive extension module can be found in Goldman et al. (2015) and Litvan et al. (2012).
The inventory of assessments used in ongoing longitudinal studies within the working group revealed that there is a consensus about the functions/domains that should be assessed in PD cohort studies, but not about the nature of specific assessments used. The variability in the choice of the assessments may be explained by a number of different factors: (i) Not all scales/questionnaires are available and validated in all languages. (ii) Study designs vary with regard to outcome variables which influences the choice of assessments. (iii) Some assessments require more resources than others (more time-consuming, more costly or requiring trained staff members), which also influenced the selection and composition of the selected assessment battery. (iv) Advances in knowledge about assessments and biomarkers have led to revision or expansion of assessments after the respective study was initiated. (v) Preference for a specific assessment based on previous experience of the individual researchers involved.
With our proposed modular set of biomarker assessments, we propose a concept by which we hope to overcome the problem of data comparison due to lack of harmonization and set the stage for broad data sharing, joint data analyses and acceleration of biomarker research.
SL, SH, GA, PB, SB, YBS, HB, BRB, DBu, RD, DG, GH, MH, MK, RK, ILS, WM, MM, BM, WO, BR, UW, KW, DBe substantial contributed to the conception and design of the work; SL, SH, DBe drafted the work; GA, PB, SB, YBS, HB, BRB, DBu, RD, DG, GH, MH, MK, RK, ILS, WM, MM, BM, WO, BR, UW, KW revised the work critically for important intellectual content; SL, SH, GA, PB, SB, YBS, HB, BRB, DBu, RD, DG, GH, MH, MK, RK, ILS, WM, MM, BM, WO, BR, UW, KW, DBe gave their final approval to the version to be published; SL, SH, GA, PB, SB, YBS, HB, BRB, DBu, RD, DG, GH, MH, MK, RK, ILS, WM, MM, BM, WO, BR, UW, KW, DBe agreed to be accountable for all aspects of the work.
The work was funded by the EU Joint Programme—Neurodegenerative Disease Research (JPND) program (BMBF No:01ED1410).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We acknowledge support of publication by Deutsche Forschungsgemeinschaft and Open Access Publishing Fund of Tuebingen University, Tuebingen, Germany.
ADL, Activities of daily living; BDI-II, Beck depression inventory version II; CSF, Cerebrospinal fluid; I123-FP-CIT, 123I-N-ω-fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl)nortropane); DNA, Deoxyribonucleic acid; FDG-PET, fluorodeoxyglucose positron emission tomography; fMRI, functional magnetic resonance imaging; GDS, Geriatric depression scale; HAAS, Honolulu Asia Aging study, MDS-UPDRS, Movement Disorder Society—Unified Parkinson's Disease Rating Scale; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; MRI magnetic resonance imaging; PD, Parkinson's Disease; PDQ-39, Parkinson's Disease Questionnaire-39 items; QoL, Quality of Life; RBD-SQ, Rapid eye movement sleep behavior disorder screening questionnaire; RNA, Ribonucleic acid; SCOPA, Scales for Outcome in Parkinson's Disease; TCS, transcranial sonography.
Aarsland, D., Bronnick, K., Williams-Gray, C., Weintraub, D., Marder, K., Kulisevsky, J., et al. (2010). Mild cognitive impairment in Parkinson disease: a multicenter pooled analysis. Neurology 75, 1062–1069. doi: 10.1212/WNL.0b013e3181f39d0
Goldman, J. G., Holden, S., Ouyang, B., Bernard, B., Goetz, C. G., and Stebbins, G. T. (2015). Diagnosing PD-MCI by MDS Task Force criteria: how many and which neuropsychological tests? Mov. Disord. 30, 402–406. doi: 10.1002/mds.26084
Lawton, M., Kasten, M., May, M. T., Mollenhauer, B., Schaumburg, M., Liepelt-Scarfone, I., et al. (2016). Validation of conversion between mini-mental state examination and montreal cognitive assessment. Mov. Disord. 31, 593–596. doi: 10.1002/mds.26498
Lerche, S., Liepelt-Scarfone, I., Alves, G., Barone, P., Behnke, S., Ben-Shlomo, Y., et al. (2015). Methods in neuroepidemiology characterization of European Longitudinal Cohort Studies in Parkinson's Disease - Report of the JPND Working Group BioLoC-PD. Neuroepidemiology 45, 282–297. doi: 10.1159/00043922
Litvan, I., Goldman, J. G., Tröster, A. I., Schmand, B. A., Weintraub, D., Petersen, R. C., et al. (2012). Diagnostic criteria for mild cognitive impairment in Parkinson's disease: Movement Disorder Society Task Force guidelines. Mov. Disord. 27, 349–356. doi: 10.1002/mds.24893
Keywords: Parkinson's disease, marker, harmonization, cohort studies
Citation: Lerche S, Heinzel S, Alves GW, Barone P, Behnke S, Ben-Shlomo Y, Berendse H, Bloem BR, Burn D, Dodel R, Grosset DG, Hipp G, Hu MT, Kasten M, Krüger R, Liepelt-Scarfone I, Maetzler W, Moccia M, Mollenhauer B, Oertel W, Roeben B, Walter U, Wirdefeldt K and Berg D (2016) Aiming for Study Comparability in Parkinson's Disease: Proposal for a Modular Set of Biomarker Assessments to be Used in Longitudinal Studies. Front. Aging Neurosci. 8:121. doi: 10.3389/fnagi.2016.00121
Received: 21 March 2016; Accepted: 12 May 2016;
Published: 27 May 2016.
Edited by:
J. Arturo García-Horsman, University of Helsinki, FinlandReviewed by:
Claire O'Callaghan, University of Cambridge, UKCopyright © 2016 Lerche, Heinzel, Alves, Barone, Behnke, Ben-Shlomo, Berendse, Bloem, Burn, Dodel, Grosset, Hipp, Hu, Kasten, Krüger, Liepelt-Scarfone, Maetzler, Moccia, Mollenhauer, Oertel, Roeben, Walter, Wirdefeldt and Berg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stefanie Lerche, c3RlZmFuaWUubGVyY2hlQHVuaS10dWViaW5nZW4uZGU=
†These authors have contributed equally to this work.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.