 Claire Marcroft
Claire Marcroft Aftab Khan
Aftab Khan Nicholas D. Embleton
Nicholas D. Embleton Michael Trenell2
Michael Trenell2 Thomas Plötz
Thomas Plötz- 1Neonatal Service, Royal Victoria Infirmary (RVI), Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK
- 2MoveLab, The Medical School, Newcastle University, Newcastle upon Tyne, UK
- 3Culture Lab, School of Computing Science, Newcastle University, Newcastle upon Tyne, UK
Preterm birth is associated with increased risks of neurological and motor impairments such as cerebral palsy. The risks are highest in those born at the lowest gestations. Early identification of those most at risk is challenging meaning that a critical window of opportunity to improve outcomes through therapy-based interventions may be missed. Clinically, the assessment of spontaneous general movements is an important tool, which can be used for the prediction of movement impairments in high risk infants. Movement recognition aims to capture and analyze relevant limb movements through computerized approaches focusing on continuous, objective, and quantitative assessment. Different methods of recording and analyzing infant movements have recently been explored in high risk infants. These range from camera-based solutions to body-worn miniaturized movement sensors used to record continuous time-series data that represent the dynamics of limb movements. Various machine learning methods have been developed and applied to the analysis of the recorded movement data. This analysis has focused on the detection and classification of atypical spontaneous general movements. This article aims to identify recent translational studies using movement recognition technology as a method of assessing movement in high risk infants. The application of this technology within pediatric practice represents a growing area of inter-disciplinary collaboration, which may lead to a greater understanding of the development of the nervous system in infants at high risk of motor impairment.
Introduction
Each year more than 15 million babies worldwide are born preterm (before 37 weeks gestational age) and the number of cases continues to rise (1). Infants born preterm are at higher risk of developing motor impairment than infants born at term (2). Morbidity is inversely correlated to gestational age meaning that those born extremely preterm (<28 weeks gestation) are most at risk (3). Cerebral palsy (CP) is a common motor impairment (3) for high risk infants (such as those born preterm) and these infants are also at high risk of developmental delay and other motor coordination disorders (4).
There are currently no standardized clinical guidelines for the prediction of motor impairment in high risk infants and the identification of those at highest risk typically involves the integration of clinical history, neuroimaging results, different clinical assessments, and experience of health care professionals. The assessment of spontaneous general movements is an important tool, which can be used for the prediction of movement impairments in high risk infants (5).
Movement recognition aims to capture and analyze relevant limb movements through computerized approaches focusing on continuous, objective, and quantitative assessment. Different methods of recording and analyzing infant movements have recently been explored. Camera-based solutions (6–10) and body-worn miniaturized movement sensors (11–14) have been applied in order to record continuous time-series data that represent the dynamics of limb movements. Various machine learning methods have been developed to analyze the recorded movement data. This has specifically focused on the detection and classification of atypical spontaneous general movements.
The aim of this article is to briefly summarize the current most evidence based clinical approach to observational movement assessment in high risk infants (Prechtl’s General Movements Assessment) and identify the current studies, which have applied a variety of automated movement recognition technologies to assess infant movement.
Clinical Prediction of Cerebral Palsy Using Prechtl’s General Movements Assessment
Infants learn how their bodies move and interact with the environment in early infancy (15). This is achieved through the development of spontaneous movements into goal directed movements through exploration and problem solving (15). Consequently, the development of spontaneous movements in early infancy is a high predictor for later movement (and also cognitive) performance (4, 16).
The development of spontaneous movements in infants has been studied and described in detail by Heinze Prechtl and colleagues (17). Prechtl’s general movements assessment is currently the clinical assessment that can most reliably predict CP in high risk infants with a reported sensitivity of 98% (95% confidence interval, CI 74–100%) and specificity of 91% (95% CI 83–93%) (5).
The application of this assessment clinically involves the evaluation of the qualities of the spontaneous general movements through Gestalt perception of the observer (18). A video recording is taken of the infant’s spontaneous general movements, which is then assessed during playback of the video recording at normal speed and in addition, a higher speed may be used to identify the presence of movement stereotypies (18).
In typically developing infants, spontaneous movements are characterized by large variation (18, 19). Writhing movements (observed between 36 weeks and 2 months post term) are performed with moderate amplitude and speed and are characterized by high complexity and large variation in relation to amplitude, velocity, and acceleration (18). Between 2 and 5 months of age, fidgety movements become apparent: these show smaller amplitudes of circular shape, lower speed, and a higher variability in acceleration (18).
Atypical motor development is characterized by limited variation and limited variability in generalized movements (18). In particular, the presence of cramped synchronized general movements (CSGMs) during preterm and term age and the absence of fidgety movements at 3–5 months are strong predictors for later CP diagnosis (20, 21). CSGM’s are atypical and lack fluency, variation, and complexity and are also stereotyped in nature (limb and trunk muscles contract and relax nearly simultaneously) (18, 21).
The challenges of applying the GM assessment in practice relate to the availability of appropriately trained and skilled clinicians. Considerable training is required for an assessor to become reliable enough to make an accurate evaluation. The assessment is susceptible to observer fatigue (21) and is dependent on the behavioral state of the infant during recording (ideally an infant should be in an alert, awake state). By the time, a single GM assessment is most accurate in predicting CP (3–5 months) (5) an opportunity to influence the nervous system at an earlier stage of development may have been missed.
Despite good levels of inter-observer reliability with the GM assessment (22), there will always remain a degree of subjectivity in interpretation. In common with all techniques involving interpretation by a skilled and experienced observer (including for example, ultrasound scan interpretation), experience of interpretation will improve with time. Despite this, it is not possible to determine the nature and extent of any subjectivity; however, the lack of widespread adoption among clinical teams may suggest there is a concern.
These challenges in the early detection of motor impairments in high risk infants have led to an increasing interest in the use of automated movement recognition technologies being applied in this clinical area.
Automated Movement Recognition for Clinical Movement Assessment
The use of automated movement recognition technology has been explored in many different clinical conditions such as dementia (23), Parkinson’s disease (24), and Autism (25, 26). Many of these applications have produced promising results regarding the overall potential for continuous and longitudinal assessments in both clinical and home environments (27).
Movement recognition in clinical applications aims at the automated detection, classification, and assessment of the quality of limb movements focusing on indications for abnormalities. Capturing limb movements can be based on either indirect or direct sensing (28). Indirect sensing utilizes devices that are integrated into the assessment environment, such as video cameras or 3D motion capture facilities (29) and direct sensing records movement data through sensors that are worn by the patient, i.e., miniaturized devices attached to the limbs (11, 30, 31). Both methods capture movement as time-series data, i.e., sequences of sensor readings. Depending on the sensing modality applied, this data exhibit differences in temporal and spatial resolution, which requires adaptations of the analysis methods. Typical methods for automated data analysis include sequential probabilistic modeling, e.g., using Markovian approaches (32), statistical methods (11, 14) to model specific gestures of interest (12) or holistic monitoring of general movements (27).
There are considerable challenges in utilizing this technology in the neonatal environment, in particular, the size, fragility, and vulnerability of infants needs to be taken into account. Furthermore, the automated movement assessment must be sensitive and reliable enough to detect subtle changes in movements, which are the basis for clinical diagnosis.
Table 1 summarizes some of the advantages and disadvantages associated with the two sensing modalities, i.e., direct sensing, where movements are captured using hardware directly attached to the subject; and indirect sensing, where hardware is placed in the assessment environment.
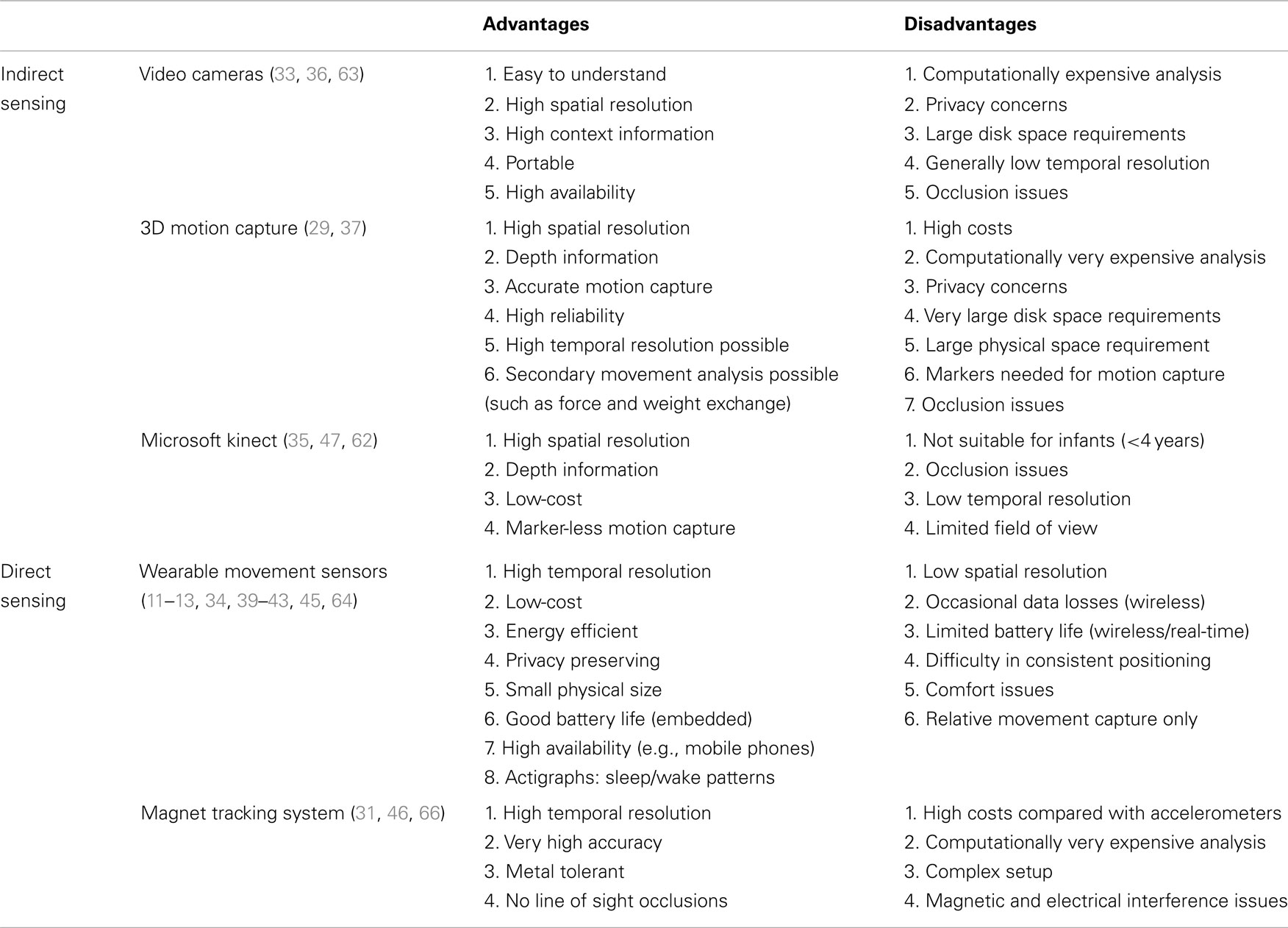
Table 1. Brief overview of some of the advantages and disadvantages associated with various sensing modalities in the context of recording general movements in preterm infants.
Figure S1 in Supplementary Material gives an overview of the general approach to automated gesture recognition for clinical movement assessment. Sensory data for capturing movements using one or more of the sensing techniques (summarized in Table 1) are usually pre-processed [see in Ref. (40, 48, 49)] for wearable sensors and (50, 51) for vision-based systems followed by movement segmentation, i.e., parts from the recorded data are partitioned that might contain important movement information [see in Ref. (26) for automatic segmentation]. This is usually followed by feature extraction used to represent large amounts of sensing data in a reduced fashion [e.g., (52); see also Ref. (53) for a generic feature learning approach]. Finally, classification is performed to identify (or predict) different types of movements. Various classification frameworks have been reported in the context of wearable/environmental sensors such as (54–56) and vision-based systems for activity recognition (57–59). A supervised classification framework also requires some form of ground truth labeling. These labels are used for training a machine learning classifier [some issues related to ground truth annotation have been addressed in Ref. (48, 60); automated vision-based annotation systems have also been explored in Ref. (59, 61)].
In the following sections, we identify and classify existing systems for gesture recognition based automated movement assessment in preterm infants.
Automated Movement Recognition for Clinical Movement Assessment in High Risk Infants
Video-Based Assessment
Existing video-based movement assessment systems for infants can be categorized into: (i) using three dimensional (3D) motion capture systems; and (ii) using traditional color cameras. Motion capture based systems require special markers to be attached to the limbs being tracked. High-end cameras typically provide very high 3D tracking accuracy and resolution (both spatially and temporally; Figure S1 in Supplementary Material), but at a considerable price and setup effort. These systems are most commonly seen in the research setting and due to practical limitations are not easily adaptable to the clinical environment.
Meinecke and colleagues applied a motion capture system to objectively measure the spontaneous movements of infants during the first months of life (29). Fifty-three movement-based parameters were automatically extracted from motion tracks followed by cluster analysis based on Euclidian distances that selected eight of the parameters. These were able to delineate between healthy and at risk infants. Classification was performed using quadratic discriminant analysis (sensitivity 1, specificity 0.7) (see Table 2). With a similar setup Kanemaru and co-workers analyzed spontaneous movements in infants aiming to investigate the relationship between spontaneous movements and the development of CP at 3 years of age. The authors found that the jerkiness in spontaneous movements at term age (defined as the time integral of the square of the magnitude of jerks per unit movement distance) was higher in infants who developed CP (8–10).
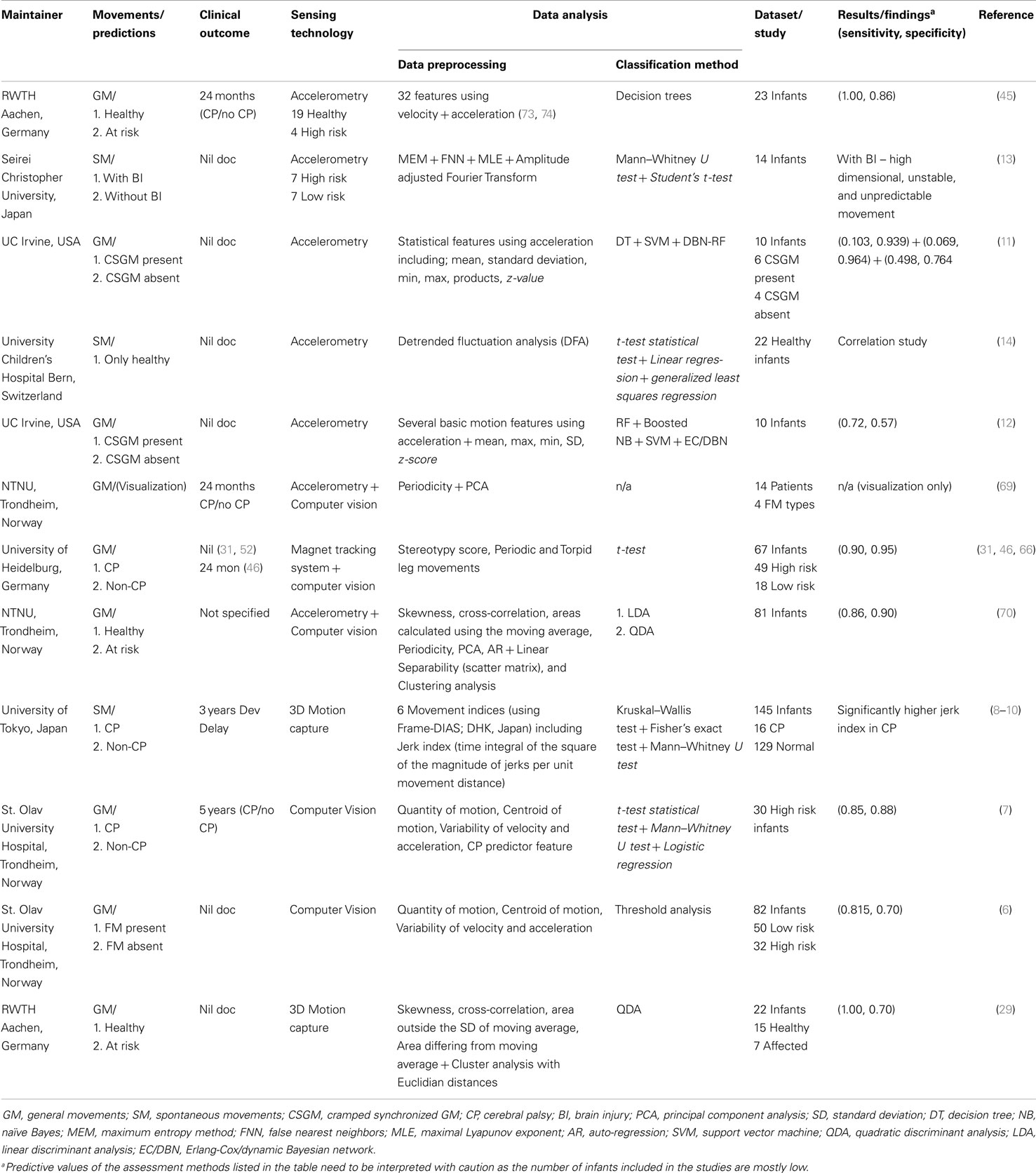
Table 2. Identification of different automated gesture recognition systems applied to objectively measure movement in infants.
Despite the popularity of consumer 3D cameras such as Microsoft’s Kinect (47), these have not yet been used extensively for movement analysis in infants. This is in stark contrast to other clinical applications (35, 62). Although having great potential for general movement analysis, Kinect’s capabilities are not largely explored with regards to assessments of preterm infants. This could be because the provided human tracking system in Kinect, necessary for detailed analysis, is recommended for tracking humans who are at least 4 years old and therefore considered unsuitable for use with infants.
Standard video cameras such as regular web-cams, RGB cameras on tripods, and even video-enabled baby monitors (36) have also been used for marker-less capturing of infants’ body movements. These systems offer a more reasonable priced alternative to 3D motion capture system and in addition come with substantially less set up effort, which enables applications beyond research and clinical settings, allowing for continuous and more detailed analysis in natural (home) environments. Typically, these recording setups come with lower spatial and temporal resolution, which limits the level of detail of the analysis. Additionally, marker-less tracking is less accurate than professional motion capture (37), which may be problematic when attempting to identify more subtle differences in movement patterns. An example would be in identification of the differences between CSGMs and poor repertoire general movements. CSGMs are described as monotonous and rigid with the limb and trunk muscles contracting and relaxing simultaneously (33) and poor repertoire general movements are monotonous, with the amplitude, speed, and intensity lacking normal variability (33). While both of these movement patterns are identified as being atypical (18, 33), CSGMs can also be most easily recognized by human gestalt perception and also have a much higher predictive value for motor impairment (33). Therefore, identification of any difference between the two atypical patterns is clinically highly relevant.
Adde and colleagues have developed an advanced video-based analysis system for quantitative and qualitative assessments of infants general movements (63). Utilizing standard RGB video cameras and an analysis method that uses so-called “motion-grams” for quantifying changes in the infant’s movements, the general movements toolbox (GMT) is able to detect fidgety movements as described in the GM assessment (18). This clinical toolbox may be useful in the early diagnosis and/or risk stratification of infants at high risk of developing CP. The first studies using GMT on a small number of high risk infants (n = 30) report promising results (sensitivity 85% and specificity 88%) with respectable follow-up data past 4 years of age (7). This suggests that the application of the GMT as a method for prediction of neurological impairment may be straightforward, cost-effective, and feasible for use in clinical practice but will require further systematic validation.
Assessment through Direct Movement Sensing
While indirect sensing settings require external tracking equipment, body-worn accelerometers have recently been successfully applied and remain popular in clinical studies. In particular, the proliferation of affordable, reliable, and miniaturized sensing facilities in combination with sophisticated data analysis techniques has allowed for automation of movement assessment in small infants. Accelerometers are sensors, which measure inertial forces in one or three spatial axes, resulting in high-resolution time-series data that represent the dynamics of the acceleration of the sensor during movements (34). Specifically, they have been used to measure physical activity levels in children (34), sleep/wake cycles, and the physiology of swallowing in infants (38, 64). These applications are in line with a large body of research that focuses on objective assessments of movement related parameters in a multitude of health-related scenarios, including gait analysis (39) sport activity (40), rehabilitation monitoring (41, 42), quantification of disease progression, and investigation of effectiveness of therapy interventions (43).
Even though reduced frequency and quantity of limb movements in infants have recently been identified as early predictors for developmental delay (9), it is widely accepted that in infants with a suspected diagnosis of CP, the general movements change in quality rather than quantity (44, 65). An automated analysis therefore needs to capture fine details of limb movements, for which video-based assessments are often limited.
Karch et al. developed an electromagnetic tracking system to undertake movement analysis (66). Small lightweight sensors (1.3 mm diameter) were attached to the infant’s limbs, which were then sensed using a commercial (external) tracking system that provided high accuracy and allowed for detailed analysis of joint flexion. Serving as proof of concept this tracking system has successfully been used for detecting anomalous, spontaneous limb movements in infants (31, 66). Phillippi et al. conducted a recent study using this work where it was found that the stereotypy score of arm movements could be used as a predictor for CP and stereotyped periodic leg movements predicted neurodevelopmental impairments (46).
A limited number of more recent studies have successfully applied accelerometers to preterm infants to measure spontaneous movements (13, 31, 45, 46) and also to create models for atypical movement patterns such as CSGMs (11, 12). While this is an evolving area of translational use of technology in the healthcare setting, there is limited data quantifying limb movements and also comparing the results to longer-term neurodevelopmental outcomes. Ohgi et al. used tri-axial accelerometry for a cross-sectional study that measured upper limb acceleration in a small number of preterm infants with and without brain injuries at 1 month corrected age (13). This was the first application of accelerometers in preterm infants in a clinical environment but the recording time was limited to 200 s due to the variability of the infant’s states. Statistical analysis confirmed that infants with brain injuries exhibited unstable and unpredictable spontaneous movements with larger dimensionality (details of the analysis techniques and statistical tests are provided in Table 2).
A group from University of California, Irvine have tested the use of wireless accelerometers in the neonatal unit and compared accelerometer data to the general movements assessment (11, 12). CSGMs are highly predictive of CP (21, 67) and the group investigated whether accelerometry, combined with machine learning techniques for automated data analysis, could accurately identify the components of these atypical movements. By means of this automated assessment, limb acceleration and correlation have been characterized successfully. Gravem et al. used various statistical classification techniques to correctly identify the presence of CSGM in 6 out of 10 infants (11). Reported accuracy varied between 70 and 90% (see Table 2 for details).
Heinze et al. used miniature accelerometers with the aim of developing a methodology to allow objective diagnosis of the development of movement disorders in preterm infants (45). The overall detection rate was >90% over three measurements and the timing of the data collection correlated with the characteristics of spontaneous movements as described in the general movements assessment (18). Nineteen healthy term infants and four “at risk” preterm infants were included in the study. Clinical and neurological examinations were undertaken and “at risk” infants were identified through abnormalities on computer tomography and/or follow-up to 2 years.
These direct sensing studies represent promising applications of technology to contribute to the identification of atypical movement patterns in preterm infants. However, it is important to take into consideration that only small numbers of preterm infants with atypical movements were included which do not allow for the calculation of sensitivity and specificity. Furthermore, the feasibility of applying these techniques to larger numbers of high risk infants in a clinical environment is difficult to establish and in comparison to applying video-based methods of assessment (including Prechtl’s GM assessment) may be more difficult to achieve due to the logistics of attaching direct sensors to small infants.
Hybrid systems
The main advantage of video-based movement analysis lies in the recording of spatial data in addition to temporal measurements, which gives direct access to, for example, posture-related information. In contrast, direct sensing approaches typically have a much higher temporal resolution allowing for more detailed assessments, which is beneficial for in-depth analysis of subtle changes that may precede the development of CP.
Some approaches have been developed that aim at combining both sensing methods in order to benefit from both spatial and high temporal resolution – at reasonable costs and minimum setup efforts for practical applications – for high-fidelity movement analysis (68). Berge and colleagues have proposed a software tool for GM representation and modeling called ENIGMA – enhanced interactive general movement assessment. ENIGMA provides a useful support tool for visualizing features of motion data in conjunction with video data for GM experts (69). Similarly, Rahmanpour et al. employ a hybrid sensing approach for the prediction of CP using an extensive analysis of movement-based features. The authors found that dynamic features are more indicative than the standard statistical features (70). Results from their analysis are shown in Table 2 with a detailed description of the employed features.
Summary
Prediction of motor impairment (such as CP) in preterm infants is challenging, and ideally requires techniques that are both sensitive and specific. Due to the large number of complex factors affecting neurodevelopment, and the difficulty in assessing brain plasticity, predicting which children will develop CP on the basis of a single assessment will always be challenging (71). A multi-modal longitudinal approach including a combination of methods, e.g., neurological assessment, general movements’ assessment, and neuroimaging is likely to improve both positive and negative prediction. Early risk stratification and prediction has many benefits. It allows for early identification of those most likely to benefit from early intervention and targeting of resources and support for parents. Furthermore, access to health, social, and educational services is often dependent on a diagnosis (72).
Accurate, non-invasive assessments of sufficient sensitivity to identify longitudinal changes in movement patterns could hold considerable hope for the future. This mini-review has identified recent studies employing video-based assessment, assessment through direct movement sensing and hybrid systems. Specifically, the use of accelerometry and computer vision may offer clinically feasible and promising methods of objectively measuring quality and quantity of infant movement. The application of these technologies may prove to be useful not only in the prediction of infants at highest risk of motor impairment but also in the evaluation of therapies aiming to influence the developing brain.
Conflict of Interest Statement
The Guest Associate Editor Gavin John Clowry declares that, despite being affiliated to the same institution as authors Claire Marcroft, Aftab Khan, Michael Trenell, and Thomas Plötz, the review process was handled objectively and no conflict of interest exists. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The first author (Ms. Claire Marcroft) received funding from UK National Institute of Health Research Clinical Academic Training Program as part of training for Masters in Clinical Research. Dr. Aftab Khan is funded by the RCUK Research Hub on Social Inclusion through the Digital Economy (SiDE) project.
Supplementary Material
The Supplementary Material for this article can be found online at http://www.frontiersin.org/Journal/10.3389/fneur.2014.00284/abstract
References
1. World Health Organisation. Born Too Soon: The Global Action Report on Preterm Birth. Geneva: WHO Press (2012).
2. Odd DE, Lingam R, Emond A, Whitelaw A. Movement outcomes of infants born moderate and late preterm. Acta Paediatr (2013) 102(9):876–82. doi:10.1111/apa.12320
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
3. Moore T, Hennessy EM, Myles J, Johnson SJ, Draper ES, Costeloe KL, et al. Neurological and developmental outcome in extremely preterm children born in England in 1995 and 2006: the EPICure studies. BMJ (2012) 345:e7961. doi:10.1136/bmj.e7961
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
4. Fjørtoft T, Grunewaldt KH, Løhaugen GCC, Mørkved S, Skranes J, Evensen KAI. Assessment of motor behaviour in high-risk-infants at 3 months predicts motor and cognitive outcomes in 10 years old children. Early Hum Dev (2013) 89(10):787–93. doi:10.1016/j.earlhumdev.2013.06.007
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
5. Bosanquet M, Copeland L, Ware R, Boyd R. A systematic review of tests to predict cerebral palsy in young children. Dev Med Child Neurol (2013) 55(5):418–26. doi:10.1111/dmcn.12140
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
6. Adde L, Helbostad JL, Jensenius AR, Taraldsen G, Stoen R. Using computer-based video analysis in the study of fidgety movements. Early Hum Dev (2009) 85(9):541–7. doi:10.1016/j.earlhumdev.2009.05.003
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
7. Adde L, Helbostad JL, Jensenius AR, Taraldsen G, Grunewaldt KH, Støen R. Early prediction of cerebral palsy by computer-based video analysis of general movements: a feasibility study. Dev Med Child Neurol (2010) 52(8):773–8. doi:10.1111/j.1469-8749.2010.03629.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
8. Kanemaru N, Watanabe H, Taga G. Increasing selectivity of interlimb coordination during spontaneous movements in 2- to 4-month-old infants. Exp Brain Res (2012) 218(1):49–61. doi:10.1007/s00221-012-3001-3
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
9. Kanemaru N, Watanabe H, Kihara H, Nakano H, Takaya R, Nakamura T, et al. Specific characteristics of spontaneous movements in preterm infants at term age are associated with developmental delays at age 3 years. Dev Med Child Neurol (2013) 55(8):713–21. doi:10.1111/dmcn.12156
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
10. Kanemaru N, Watanabe H, Kihara H, Nakano H, Nakamura T, Nakano J, et al. Jerky spontaneous movements at term age in preterm infants who later developed cerebral palsy. Early Hum Dev (2014) 90(8):387–92. doi:10.1016/j.earlhumdev.2014.05.004
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
11. Gravem D, Singh M, Chen C, Rich J, Vaughan J, Goldberg K, et al. Assessment of infant movement with a compact wireless accelerometer system. J Med Device (2012) 6(2):021013. doi:10.1115/1.4006129
12. Mingming F, Dana G, Dan MC, Donald JP. Augmenting gesture recognition with erlang-cox models to identify neurological disorders in premature babies. International Joint Conference on Pervasive and Ubiquitous Computing (Ubicomp). Pittsburg: ACM (2012).
13. Ohgi S, Morita S, Loo KK, Mizuike C. Time series analysis of spontaneous upper-extremity movements of premature infants with brain injuries. Phys Ther (2008) 88(9):1022–33. doi:10.2522/ptj.20070171
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
14. Waldmeier S, Grunt S, Delgado-Eckert E, Latzin P, Steinlin M, Fuhrer K, et al. Correlation properties of spontaneous motor activity in healthy infants: a new computer-assisted method to evaluate neurological maturation. Exp Brain Res (2013) 227(4):433–46. doi:10.1007/s00221-013-3504-6
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
15. Thelen E. Origins of origins of motor control. Behav Brain Sci (1995) 18(04):780–3. doi:10.1017/S0140525X00041030
16. Disselhorst-Klug C, Heinze F, Breitbach-Faller N, Schmitz-Rode T, Rau G. Introduction of a method for quantitative evaluation of spontaneous motor activity development with age in infants. Exp Brain Res (2012) 218(2):305–13. doi:10.1007/s00221-012-3015-x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
17. Prechtl HFR. Qualitative changes of spontaneous movements in fetus and preterm infant are a marker of neurological dysfunction. Early Hum Dev (1990) 23(3):151–8. doi:10.1016/0378-3782(90)90011-7
18. Prechtl HFR. State of the art of a new functional assessment of the young nervous system. An early predictor of cerebral palsy. Early Hum Dev (1997) 50(1):1–11. doi:10.1016/S0378-3782(97)00088-1
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
19. Hadders-Algra M. Variation and variability: key words in human motor development. Phys Ther (2010) 90(12):1823–37. doi:10.2522/ptj.20100006
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
20. Spittle AJ, Orton J. Cerebral palsy and developmental coordination disorder in children born preterm. Semin Fetal Neonatal Med (2013) 19(2):84–9. doi:10.1016/j.siny.2013.11.005
21. Einspieler C, Marschik PB, Bos AF, Ferrari F, Cioni G, Prechtl HFR. Early markers for cerebral palsy: insights from the assessment of general movements. Future Neurol (2012) 7(6):709–17. doi:10.2217/fnl.12.60
22. Fjørtoft T, Einspieler C, Adde L, Strand LI. Inter-observer reliability of the “assessment of motor repertoire – 3 to 5 months” based on video recordings of infants. Early Hum Dev (2009) 85(5):297–302. doi:10.1016/j.earlhumdev.2008.12.001
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
23. Ourique de Morais W, Sant Anna A, Wickström N. A wearable accelerometer based platform to encourage physical activity for the elderly. Gerontechnology (2008) 7(2):181. doi:10.4017/gt.2008.07.02.118.00
24. Maetzler W, Domingos J, Srulijes K, Ferreira JJ, Bloem BR. Quantitative wearable sensors for objective assessment of Parkinson’s disease. Mov Disord (2013) 28(12):1628–37. doi:10.1002/mds.25628
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
25. Goodwin M, Intille S, Albinali F, Velicer W. Automated detection of stereotypical motor movements. J Autism Dev Disord (2011) 41(6):770–82. doi:10.1007/s10803-010-1102-z
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
26. Ploetz T, Hammerla N, Rozga A, Reavis A, Call N, Abowd GD. Automatic assessment of problem behavior in individuals with developmental disabilities. International Joint Conference on Pervasive and Ubiquitous Computing (Ubicomp). Newcastle: ACM (2012).
27. Godfrey A, Conway R, Meagher D, ÓLaighin G. Direct measurement of human movement by accelerometry. Med Eng Phys (2008) 30(10):1364–86. doi:10.1016/j.medengphy.2008.09.005
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
28. Chen C, Hoey J, Nugent CD, Cook DJ, Zhiwen Y. Sensor-based activity recognition. Syst Man Cybern (2012) 42(6):790–808. doi:10.1109/TSMCC.2012.2198883
29. Meinecke L, Breitbach-Faller N, Bartz C, Damen R, Rau G, Disselhorst-Klug C. Movement analysis in the early detection of newborns at risk for developing spasticity due to infantile cerebral palsy. Hum Mov Sci (2006) 25(2):125–44. doi:10.1016/j.humov.2005.09.012
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
30. Ohgi S, Morita S, Kek KL, Mizuike C. A dynamical systems analysis of spontaneous movements in newborn infants. J Mot Behav (2007) 39(3):203–14. doi:10.3200/JMBR.39.3.203-214
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
31. Karch D, Kang K-S, Wochner K, Philippi H, Hadders-Algra M, Pietz J, et al. Kinematic assessment of stereotypy in spontaneous movements in infants. Gait Posture (2012) 36(2):307–11. doi:10.1016/j.gaitpost.2012.03.017
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
32. Moeslund TB, Granum E. A survey of computer vision-based human motion capture. Comput Vis Image Underst (2001) 81(3):231–68. doi:10.2165/00007256-200838120-00006
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
33. Einspieler C, Prechtl HFR. Prechtl’s assessment of general movements: a diagnostic tool for the functional assessment of the young nervous system. Ment Retard Dev Disabil Res Rev (2005) 11(1):61–7. doi:10.1002/mrdd.20051
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
34. Cliff DP, Reilly JJ, Okely AD. Methodological considerations in using accelerometers to assess habitual physical activity in children aged 0-5 years. J Sci Med Sport (2009) 12(5):557–67. doi:10.1016/j.jsams.2008.10.008
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
35. Luna-Oliva L, Ortiz-Gutierrez RM, Cano-de la Cuerda R, Piedrola RM, Alguacil-Diego IM, Sanchez-Camarero C, et al. Kinect Xbox 360 as a therapeutic modality for children with cerebral palsy in a school environment: a preliminary study. NeuroRehabilitation (2013) 33(4):513–21. doi:10.3233/NRE-131001
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
36. Koninklijke P. (2014). Available from: http://www.philips.co.uk/c-p/SCD600_00
37. Vicon Motion Systems Ltd. (2014). Available from: http://www.vicon.com
38. So K, Michael Adamson T, Horne RSC. The use of actigraphy for assessment of the development of sleep/wake patterns in infants during the first 12 months of life. J Sleep Res (2007) 16(2):181–7. doi:10.1111/j.1365-2869.2007.00582.x
39. Tao W, Liu T, Zheng R, Feng H. Gait analysis using wearable sensors. Sensors Basel Sensors (2012) 12(2):2255–83. doi:10.3390/s120202255
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
40. Ladha C, Hammerla N, Olivier P, Ploetz T. ClimbAX: skill assessment for climbing enthusiasts. International Joint Conference on Pervasive and Ubiquitous Computing (Ubicomp). Zurich: ACM (2013).
41. Patel S, Park H, Bonato P, Chan L, Rodgers M. A review of wearable sensors and systems with application in rehabilitation. J Neuroeng Rehabil (2012) 9:21. doi:10.1186/1743-0003-9-21
42. Moeller ARL, Diewald S, Kranz M, Hammerla N, Olivier P, Ploetz T. GymSkill: a personal trainer for physical exercises. International Conference on Pervasive Computing. Newcastle: IPCP (2012).
43. Choquette S, Hamel M, Boissy P. Accelerometer-based wireless body area network to estimate intensity of therapy in post-acute rehabilitation. J Neuroeng Rehabil (2008) 5:20. doi:10.1186/1743-0003-5-20
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
44. Burger M, Louw QA. The predictive validity of general movements – a systematic review. Eur J Paediatr Neurol (2009) 13(5):408–20. doi:10.1016/j.ejpn.2008.09.004
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
45. Heinze F, Hesels K, Breitbach-Faller N, Schmitz-Rode T, Disselhorst-Klug C. Movement analysis by accelerometry of newborns and infants for the early detection of movement disorders due to infantile cerebral palsy. Med Biol Eng Comput (2010) 48(8):765–72. doi:10.1007/s11517-010-0624-z
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
46. Philippi H, Karch D, Kang K-S, Wochner K, Pietz J, Dickhaus H, et al. Computer-based analysis of general movements reveals stereotypies predicting cerebral palsy. Dev Med Child Neurol (2014) 56(10):922–3. doi:10.1111/dmcn.12477
47. MicrosoftCorp. (2014). Available from: http://www.xbox.com/en-gb/kinect
48. Ploetz T, Chen C, Hammerla NY, Abowd GD. Automatic synchronization of wearable sensors and video-cameras for ground truth annotation – a practical approach. International Symposium on Wearable Computers (ISWC). Zurich: ISWC (2012).
49. Ladha C, Hammerla N, Hughs E, Olivier P, Ploetz T. Dog’s life: wearable activity recognition for dogs. International Joint Conference on Pervasive and Ubiquitous Computing (Ubicomp). Zurich: ACM (2013).
50. Almajai I, Kittler J, De Campos T, Christmas W, Yan F, Windridge D, et al. Ball event recognition using hmm for automatic tennis annotation. International Conference on Image Processing (ICIP). Hong Kong: IEEE (2010).
51. Khan A, Windridge D, Kittler J. Multilevel Chinese takeaway process and label-based processes for rule induction in the context of automated sports video annotation. IEEE Trans Cybern (2014) 44(10):1910–23. doi:10.1109/TCYB.2014.2299955
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
52. Hammerla NY, Kirkham R, Andras P, Ploetz T. On preserving statistical characteristics of accelerometry data using their empirical cumulative distribution. International Symposium on Wearable Computers (ISWC). Zurich: ISWC (2013).
53. Ploetz T, Hammerla NY, Olivier P. Feature learning for activity recognition in ubiquitous computing. International Joint Conference on Artificial Intelligence. Barcelona: IJCAI (2011).
54. Khan A, Nicholson J, Mellor S, Jackson D, Ladha K, Ladha C, et al. Occupancy monitoring using environmental & context sensors and a hierarchical analysis framework. Embedded Systems for Energy-Efficient Buildings (BuildSys). ACM (2014). p. 90–9. doi:10.1145/2674061.2674080
55. Bhattacharya S, Nurmi P, Hammerla N, Ploetz T. Using unlabeled data in a sparse-coding framework for human activity recognition. Pervasive Mob Comput (2014) 15:242–62. doi:10.1016/j.pmcj.2014.05.006
56. Kranz M, Moeller A, Hammerla N, Diewald S, Ploetz T, Olivier P, et al. The mobile fitness coach: towards individualized skill assessment using personalized mobile devices. Pervasive Mob Comput (2013) 9(2):203–15. doi:10.1016/j.pmcj.2012.06.002
57. Bettadapura V, Schindler G, Ploetz T, Irfan E. Augmenting bag-of-words: data-driven discovery of temporal and structural information for activity recognition. IEEE Conference on Computer Vision and Pattern Recognition (CVPR). Portland: IEEE (2013).
58. Almajai I, Yan F, de Campos TE, Khan A, Christmas W, Windridge D, et al. Anomaly detection and knowledge transfer in automatic sports video annotation. In: Weinshall D, Anemüller J, van Gool L, editors. Detection and Identification of Rare Audiovisual Cues. Berlin: Springer (2012). p. 109–17. doi:10.1007/978-3-642-24034-8_9
59. de Campos T, Khan A, Yan F, Faraji Davar N, Windridge D, Kittler J, et al. A framework for automatic sports video annotation with anomaly detection and transfer learning. Proceedings of Machine Learning and Cognitive Science, Palma de Mallorca: 3rd EUCogIII Members Conference. (2013).
60. Kirkham R, Khan A, Bhattacharya S, Hammerla N, Mellor S, Roggen D, et al. Automatic correction of annotation boundaries in activity datasets by class separation maximization. International Joint Conference on, Adjunct Publication Pervasive and Ubiquitous Computing (Ubicomp). Zurich: ACM (2013).
61. Khan A, Windridge D, de Campos T, Kittler J, Christmas W. Lattice-based anomaly rectification for sport video annotation. International Conference on Pattern Recognition (ICPR). Istanbul: IEEE (2010). p. 4372–5.
62. Chang Y-J, Han W-Y, Tsai Y-C. A kinect-based upper limb rehabilitation system to assist people with cerebral palsy. Res Dev Disabil (2013) 34(11):3654–9. doi:10.1016/j.ridd.2013.08.021
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
63. Adde L, Helbostad JL, Jensenius AR, Taraldsen G, Støen R. Using computer-based video analysis in the study of fidgety movements. Early Hum Dev (2009) 85(9):541–7. doi:10.1016/j.earlhumdev.2009.05.003
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
64. Reynolds EW, Vice FL, Bosma JF, Gewolb IH. Cervical accelerometry in preterm infants. Dev Med Child Neurol (2002) 44(9):587–92. doi:10.1017/S0012162201002626
65. Darsaklis V, Snider LM, Majnemer A, Mazer B. Predictive validity of Prechtl’s method on the qualitative assessment of general movements: a systematic review of the evidence. Dev Med Child Neurol (2011) 53(10):896–906. doi:10.1111/j.1469-8749.2011.04017.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
66. Karch D, Kim K-S, Wochner K, Pietz J, Dickhaus H, Philippi H. Quantification of the segmental kinematics of spontaneous infant movements. J Biomech (2008) 41(13):2860–7. doi:10.1016/j.jbiomech.2008.06.033
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
67. Spittle AJ, Spencer-Smith MM, Cheong JLY, Eeles AL, Lee KJ, Anderson PJ, et al. General movements in very preterm children and neurodevelopment at 2 and 4 years. Pediatrics (2013) 132(2):e452–8. doi:10.1542/peds.2013-0177
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
68. Huang EW, Fu LC. Gesture stroke recognition using computer vision and linear accelerometer. International Conference on Automatic Face and Gesture Recognition. Amsterdam: IEEE (2008).
69. Berge PR, Adde L, Espinosa G, Stavdahl Ø. ENIGMA – enhanced interactive general movement assessment. Expert Syst Appl (2008) 34(4):2664–72. doi:10.1016/j.eswa.2007.05.024
70. Rahmanpour P. Features for Movement based Prediction of Cerebral Palsy [MSc Thesis]. Trondheim: Norwegian University of Science and Technology (2009).
71. Spittle A. How do we use the assessment of general movements in clinical practice? Dev Med Child Neurol (2011) 53(8):681–2. doi:10.1111/j.1469-8749.2011.04034.x
72. Shevell AH, Shevell M. Doing the “talk”: disclosure of a diagnosis of cerebral palsy. J Child Neurol (2013) 28(2):230–5. doi:10.1177/0883073812471430
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
73. Lanzi PL. Fast feature selection with genetic algorithms: a filter approach. International Conference on Evolutionary Computation. Indianapolis: IEEE (1997). p. 537–40.
Keywords: preterm birth, cerebral palsy, neuro-motor assessment, general movement assessment, movement recognition
Citation: Marcroft C, Khan A, Embleton ND, Trenell M and Plötz T (2015) Movement recognition technology as a method of assessing spontaneous general movements in high risk infants. Front. Neurol. 5:284. doi: 10.3389/fneur.2014.00284
Received: 24 July 2014; Accepted: 15 December 2014;
Published online: 09 January 2015.
Edited by:
Gavin John Clowry, Newcastle University, UKReviewed by:
Catherine Disselhorst-Klug, RWTH Aachen University, GermanyMijna Hadders-Algra, University Medical Center Groningen, Netherlands
Copyright: © 2015 Marcroft, Khan, Embleton, Trenell and Plötz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Claire Marcroft, Newcastle Neonatal Service, Special Care Baby Unit (Ward 35), Royal Victoria Infirmary (RVI), Newcastle upon Tyne NE1 4LP, UK e-mail: c.marcroft@newcastle.ac.uk