 Robson Luis Oliveira de Amorim1*
Robson Luis Oliveira de Amorim1* André Russowsky Brunoni2
André Russowsky Brunoni2 Mirian Akiko Furutani de Oliveira3
Mirian Akiko Furutani de Oliveira3 Ana Luiza Costa Zaninotto3
Ana Luiza Costa Zaninotto3 Marcia Mitie Nagumo1
Marcia Mitie Nagumo1 Vinícius Monteiro de Paula Guirado1
Vinícius Monteiro de Paula Guirado1 Iuri Santana Neville1
Iuri Santana Neville1 Gláucia Rosana Guerra Benute3
Gláucia Rosana Guerra Benute3 Mara Cristina Souza de Lucia3
Mara Cristina Souza de Lucia3 Wellingson Silva Paiva1
Wellingson Silva Paiva1 Almir Ferreira de Andrade1
Almir Ferreira de Andrade1 Manoel Jacobsen Teixeira1
Manoel Jacobsen Teixeira1
- 1Division of Neurosurgery, University of São Paulo Medical School, São Paulo, Brazil
- 2Division of Psychiatry and Psychology, University Hospital of São Paulo University, São Paulo, Brazil
- 3Division of Psychology, University of São Paulo Medical School, São Paulo, Brazil
Background: Mild traumatic brain injury (MTBI) represents 70–80% of all treated brain injuries. A considerable proportion of MTBI patients experience post-concussion symptoms for a prolonged period after MTBI, and these symptoms are diagnosed as persistent post-concussion syndrome (PPCS). PPCS is defined as a range of physical, cognitive, and emotional symptoms. However, memory and executive dysfunction seems to be one of the most debilitating symptoms. Recently, non-invasive brain stimulation has been studied as a potential treatment method for traumatic brain injury (TBI) patients. Therefore, our primary goal is to verify the effects of transcranial direct current stimulation (tDCS) in patients with PPCS who demonstrate cognitive deficits in long-term episodic memory, working memory, and executive function following MTBI.
Methods/design: This is a randomized crossover trial of patients with a history of MTBI with cognitive deficits in memory and executive function. Thirty adult patients will be randomized in a crossover manner to receive three weekly sessions of anodal tDCS (2 mA) at left dorsolateral prefrontal cortex, left temporal cortex, and sham stimulation that will be performed at 7-day intervals (washout period). The clinical diagnosis of PPCS will be determined using the Rivermead Post-Concussion Symptoms Questionnaire. Patients who meet the inclusion criteria will be assessed with a neuropsychological evaluation. A new battery of computerized neuropsychological tests will be performed before and immediately after each stimulation. Statistical analysis will be performed to determine trends of cognitive improvement.
Discussion: There is paucity of studies regarding the use of tDCS in TBI patients, and although recent results showed controversial data regarding the effects of tDCS in such patients, we will address specifically patients with PPCS and MTBI and no brain abnormalities on CT scan other than subarachnoid hemorrhage. Moreover, due to the missing information on literature regarding the best brain region to be studied, we will evaluate two different regions to find immediate effects of tDCS on memory and executive dysfunction.
Clinical Trial Registration: www.ClinicalTrials.gov, identifier NCT02292589 (https://register.clinicaltrials.gov).
Introduction
Traumatic brain injury (TBI) is the leading cause of death and disability among children and young adults. Approximately 90% of more than two million annual traumatic brain injuries in the United States are classified as mild traumatic brain injury (MTBI) (1). The criteria for clinical identification of MTBI consists of one or more of the following: a Glasgow Coma Scale (GCS) score of 13–15, confusion and disorientation, loss of consciousness for 30 min or less, posttraumatic amnesia for less than 24 h, and/or other transient neurologic abnormalities (2).
Mild traumatic brain injury has been referred to as a “silent epidemic” because the problems experienced by patients after injury are often unnoticed but can have profound consequences, such as long-term physical, mental, social, or occupational sequelae (3–5). For the majority of patients, MTBI follows a natural course in which the symptoms rapidly resolve within 3 months. However, a considerable proportion of patients with MTBI experience post-concussion symptoms (PCS) for a prolonged period after injury (6). The range of these symptoms can include headache, dizziness, fatigue, irritability, sleep disturbance, difficulties with concentration, memory loss, stress intolerance, light and sound sensitivity, balance problems, anxiety, and a depressed mood. Such prolonged post-injury effects are referred to as persistent post-concussion syndrome (PPCS).
The consequences of PPCS are overwhelming and include a broad spectrum of cognitive, behavioral, and sensorimotor disabilities that dramatically reduce the quality of life; therefore, PPCS is a worldwide public health problem that requires long-term care (7). Given the magnitude of the problem and the lack of specificity of PPCS symptoms, there is an obvious need for studies to examine whether early intervention might reduce the duration of PPCS symptoms.
Neurological and Neuropsychological Findings concerning PPCS
Along with changes in emotional regulation, impairments in attention, memory, and executive function dominate the clinical profile of PPCS (8). However, a variety of symptoms can exist following concussion. The most common symptoms are a disruption of consciousness and a brief period of posttraumatic amnesia. The individual may also report feeling as though he or she is “in a fog.” Somatic symptoms, such as headache, fatigue, and balance problems, are also very common. During the acute stages following concussion, a patient may demonstrate disturbances in memory and concentration and feel “slowed down” (9).
It has been hypothesized that PPCS is caused by microstructural damage to the brain due to shearing injury, which is not detectable with conventional imaging techniques and may be responsible for functional deficits (10, 11). The brain regions affected by a concussion seem to especially involve the mesial regions and deeper regions including the hippocampus and corpus callosum. This “preference” would justify the deficits found in post-concussion patients who have memory complaints. Another area that is frequently involved is the prefrontal cortex, which would explain the executive function deficits that can persist even 3 months after the trauma (12, 13).
Cognitive dysfunction is characterized by impairments in attention, concentration, memory, and/or executive function. Patients may have difficulties following instructions and performing tasks or jobs that would have been routine before the trauma (14).
The rapid resolution of symptoms after MTBI raises questions of whether patients can directly benefit from neuropsychological interventions. However, PCS can undoubtedly persist in some cases. Addressing such cases through research in neuropsychology and neuroscience would help to improve our understanding of the progression and etiology of PCS, as well as produce new interventions to help patients who do not improve as expected (15).
Neuropsychological assessment provides diagnostic information about the nature and extent of cognitive dysfunction in neurological conditions, including MTBI. The National Institute of Mental Health and Neurosciences suggests that some neuropsychological batteries have adequate sensitivity and ecological validity to assess the cognitive deficits associated with MTBI (16).
Cognitive Rehabilitation—The Role of Non-Invasive Neuromodulation
Recent reports have documented the therapeutic potential of non-invasive neuromodulation techniques for cognitive enhancement (17–23). The main techniques used for this purpose are repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS).
Transcranial direct current stimulation is a non-invasive neuromodulatory technique that is inexpensive, is easy to use, and applicable to the modification of cerebral excitability. This technique delivers weak polarizing direct current to the cortex via two electrodes placed on the scalp. One electrode is an active electrode that is placed over the targeted cortical region, whereas the second electrode is a reference electrode that is typically placed over the contralateral supraorbital area or a non-cephalic region (24). Several studies have demonstrated that a single session of rTMS or tDCS can improve performance on computerized neuropsychological tests that measure cognitive functions, such as working memory, verbal fluency, reaction time, cognitive interference, and sustained attention in patients with TBI (23, 25–28). These stimulation techniques appear to modulate not only “cold” (non-emotional) cognitive functions but also cognitive processes that involve decision-making, attention, and working memory, as shown in studies of patients with depression (29) and eating disorders (30, 31).
Most studies show that anodal instead of cathodal tDCS is better to enhance cognitive function (32–44). Repetitive anodal tDCS (A-tDCS) applied to the dorsolateral prefrontal cortex (DLPFC) was reported to enhance cognition (37–39), reduce depression (40), and suppress food craving (41). Some studies showed short-term facilitation effects on visual recognition memory and memory peformance after prefrontal and temporal A-tDCS applied 30 min at 2 mA, in patients with Alzheimer disease (42–44). Moreover, A-tDCS over the DLPFC may also improve working memory in patients with Alzheimer disease (42). Another recent study showed that applying tDCS to the left temporal lobe effectively improved auditory memory of patients with poststroke cognitive impairment (45). To date, no study evaluated the effects of A-tDCS over left temporal lobe on cognitive function in patients with TBI.
Considering the possible cognitive effects of tDCS and the clinical importance of TBI, the purpose of this study is to investigate the early effects of tDCS in patients diagnosed with PPCS exhibiting cognitive deficits in long-term episodic memory, working memory, and executive function. tDCS was chosen instead of rTMS for several reasons, including that tDCS is more suitable for conducting neuropsychological tests (rTMS causes noise and slight discomfort at the stimulation site, which could interfere with patient performance on the tests), that blinding to tDCS is more reliable considering the study design, and that rTMS is expensive. Furthermore, there is a lower risk of seizures related to tDCS than to rTMS, which is contraindicated for patients with an elevated risk of seizures (46).
Study Purpose and Objectives
The purpose of this study is to determine the early effects of a single session tDCS in patients with MTBI and PPCS with cognitive deficits in long-term episodic memory and executive function (inhibitory control).
Primary Outcome Measures
The primary hypothesis is that there will be evidence of improvement of patient’s episodic memory and executive function measured by neuropsychological test after the stimulation over the left DLPFC (L-DLPFC) in comparison to the other two types of stimulation [sham stimulation and stimulation over the left temporal cortex (L-TC)].
Methods and Analysis
Trial Design
This is a randomized, sham-controlled, crossover trial. All patients will be selected from the outpatient services at the Neurotrauma Clinic of the Hospital das Clínicas of the University of São Paulo Medical School (HCFMUSP). The recruitment period will be from February 2016 to April 2018.
This trial will follow the main Consolidated Standards of Reporting Trials guidelines.
Participants
Thirty patients with a history of MTBI who are least 18 years of age will be recruited through our outpatient services at the Neurotrauma Clinic. In our institution, all patients sustaining MTBI at the emergency department are advised to come to our outpatient clinic if they have persistent symptoms. Participants must be diagnosed with clinically defined PPCS based upon established criteria for the presence and frequency of three or more current PCS-like symptoms. Those symptoms will be assessed using the Rivermead Post-Concussion Symptoms Questionnaire (RPQ) (47). The inclusion criteria are as follows: (1) a history of MTBI on hospital admission, (2) age between 18 and 60 years, (3) current subjective complaints related to memory and executive function, (4) able to sign an informed consent form, and (5) consent to participate in the study. The exclusion criteria are as follows: (1) outside the age limits, (2) no specific complaints related to memory or executive function, (3) severe symptoms of major depression (Beck Inventory >35), (4) drug addiction, (5) uncontrolled epilepsy, (6) presence of a metallic prosthesis implant, (7) presence of a cochlear implant, (8) intracranial hemorrhage other than subarachnoid hemorrhage on admission CT scan, or (9) unable to sign an informed consent form.
All patients will be informed about tDCS and the experimental protocol, which has been approved by the Ethics Committee of our hospital.
Recruitment
First the patients will be evaluated by a senior licensed neurosurgeon in the outpatient clinic. Those who present with PCS for a minimum of 3 months will be diagnosed with PPCS. The diagnosis of PPCS will be established using the RPQ (42). Patients will then be referred for a neuropsychological evaluation. Individuals with cognitive impairment related to episodic memory, working memory, and/or executive function will be eligible for the study.
Procedure
The study will consist of three phases: (1) a baseline neuropsychological assessment before starting the stimulation sessions; (2) a single tDCS session (L-DLPFC, L-TC, or Sham stimulation) once a week for three consecutive weeks. Figure 1 show the fluxogram of the study.
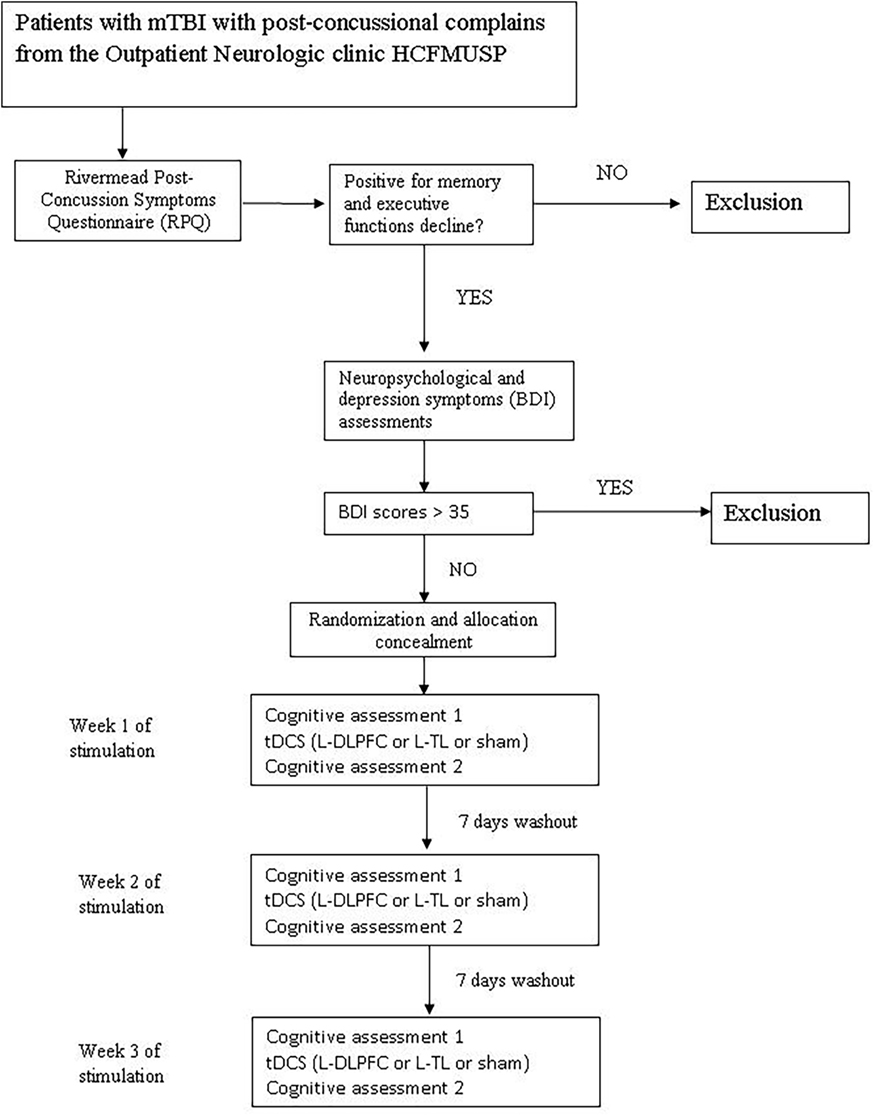
Figure 1. Fluxogram of the study.
All the subjects will receive all types of stimulation (L-DLPFC, L-TC, or Sham). The interval between each session will be 7 days to avoid carry-over effects. Because this is a crossover study, all participants will receive all proposed stimulation sessions. A computerized neuropsychological test will be performed before and immediately after each stimulation session.
(A) Frontal stimulation: patients will receive A-tDCS over the L-DLPFC at an intensity of 1.5 mA for 20 min.
(B) Temporal stimulation: patients will receive A-tDCS over the L-TC at an intensity of 1.5 mA for 20 min.
(C) Sham stimulation: patients will receive sham stimulation over the occipital area for only 30 s, after which the current will be turned off automatically without the patient’s knowledge. To guarantee blinding to the stimulation parameters, the A-tDCS electrode will be placed over the occipital region to simulate a study protocol using three different stimulation positions.
Tolerability and Safety
After each session, patients will be questioned about adverse events. If a major adverse event occurs, the patient will receive medical assistance and further examination and investigation will be provided as needed.
Instruments
To obtain the necessary data to perform this clinical trial and to analyze the results, the following instruments will be used.
Demographic Questionnaire
Information such as age, gender, initial score on the GCS, trauma mechanism, medications in use, and imaging findings will be collected.
Rivermead Post-Concussion Symptoms Questionnaire (47)
The RPQ is used to determine the presence and severity of PPCS according to a set of 16 different symptoms commonly found after MTBI. These symptoms are reported by their severity on a scale from 0 (not experienced) to 4 (severe problem). This instrument will be the screening test to identify patients with PPCS.
Beck Depression Inventory (BDI) (48)
Brazilian version (49) of the BDI will be used. The BDI is a 21-question multiple-choice self-report inventory designed for individuals aged 13 and over to assess depressive symptoms, such as hopelessness, irritability, guilt, and feeling of being punished, as well as physical symptoms, such as fatigue, weight loss, and lack of interest in sex (31). The BDI ranges from 0 to 63 points. The BDI will be assessed only at baseline.
The above neuropsychological tests will be assessed before and after each tDCS session.
Hopkins Verbal Learning Test (50)—Computer Version
This test consists of a list of 12 words. The computer program verbally reproduces the list at a 2-s interstimulus interval. Afterward, the patient is asked to recall as many items as possible in any order. Two additional learning trials are performed, and the delayed recall trial is conducted after a 25-min interval (51).
Forward and Backward Digit Span
The computer version of the Wechsler Intelligence Scale for adults (WAIS III) (52) will be used. The digits forward test assesses attention and short-term memory, whereas the digits backward test measures working memory. A random number sequence is presented to the patient at a rate of approximately one number per second. At the end of each sequence, the patient must repeat the digits in the exact sequence (for the forward sequence) in which they were presented or in the opposite order (for the backward sequence). The test is stopped when the patient has consecutive failure on a sequence with the same digit span.
Stroop Color–Word Test (53)
The Stroop test measures selective attention, cognitive flexibility, and processing speed. It consists of three cards presented by the examiner. The first card (word card) has 24 rectangles painted in brown, pink, blue, or green; the second card (color card) has 24 words (EACH, NEVER, TODAY, ALL) painted in brown, pink, blue, or green; the third card (color–word card) has 24 words (BROWN, PINK, GREEN, and BLUE) painted with mismatched colors. For each card, the subject is asked to say the name of the color as fast as he/she can. The score is calculated based on the time required to respond for each card.
Corsi Block Test (Computerized Version) (53)
This test assesses visual–spatial short-term working memory. This test requires the subject to observe the sequence of blocks “tapped” (illuminated in the computer version) and then repeat the sequence in the same order. The task starts with a short sequence of blocks that gradually increases in number for up to nine blocks. The test measures both the number of correct sequences and the longest sequence remembered.
Inhibitory Control Test (ICT)—Computerized Version (54)
This test assesses attention and inhibitory control of action. In this computerized test, the patient is shown a series of letters and is asked to press the backspace of the keyboard when the letter X is followed by the letter Y or if Y is followed by X. X and Y are the target letters; however, during the presentation of the series, other letters are included and serve as distracters. Patients are instructed not to respond to X following X or Y following Y. The ICT is administered as a practice test followed by a series of six similar 2-min trials separated by breaks to allow the subjects to rest. Performance is evaluated as the number of times the patient misses by clicking following an incorrect letter sequence (55).
Randomization and Blinding
Randomization will be done via a computer-produced randomized controlled table. All the 20 patients will be randomized into the three types of stimulation: frontal stimulation, temporal stimulation, and sham stimulation. The neuropsychologists and the patients will be blinded for the type of stimulation performed in each session.
Electronic Data Collection and Management
Data will be stored in a database developed with the Research Electronic Data Capture system (56), which is hosted on the server of the University of São Paulo. This software developed at Vanderbilt University (TN, USA) is fully web-based and enables electronic data collection, management, and also study process management, while meeting the criteria set by the international policies on data privacy and security in the health sector (57).
Sample Size Calculation
Most studies which aimed to assess the effects of non-invasive neurostimulation on cognitive function in TBI were case reports or small open labels studies. Moreover, there have been no previous studies comparing the cognitive effects of tDCS stimulation in patients with PPCS. Considering that there were no prior data on the effects of A-tDCS on patients with PPCS using our primary outcome measure, a formal sample size calculation was not possible; thus, we estimated that enrolling 30 patients would be a reasonable approach for an exploratory trial.
Statistical Analysis
All analysis will be performed using Statistical Package for Social Sciences software version 23.0 for Windows (Prentice Hall, Chicago, IL, USA). A significance level of p < 0.05 will be considered for all tests. The quantitative variables will be described using the mean and SDs for normally distributed data or median with inter-quartile range for non-parametric data. The qualitative variables will be presented as absolute and relative frequencies. The five neuropsychological assessments will be summed and averaged to create a composite score. Cohen’s d will be calculated to compare the changes in the neuropsychological scores between the groups. An analysis of variance will be used to test whether there is an overall effect of any type of active stimulation on each outcome measure. When appropriate, we will perform post hoc paired comparisons using Bonferroni correction for multiple comparisons.
Ethical Issues
Considering the study’s context and design, there will be minimal risk to patients. Non-invasive neuromodulation techniques follow the ethical criteria for studies involving human participants by respecting the principles of autonomy, beneficence, non-maleficence, and proportionality to ensure that the subject will not be harmed if he/she participates in the study.
Transcranial direct current stimulation can be considered a safe intervention for several reasons: (A) the electric current applied is very low (1–2 mA over an area of 25–35 cm2), (B) there is no direct contact between the electrodes and the brain, and (C) the electrodes are embedded in a saline solution, minimizing tissue resistance and avoiding overheating (58–60).
The most common adverse effects observed in safety studies were tingling sensations, itching, mild transient redness of the skin and discomfort on the site of stimulation, moderate fatigue, difficulty concentrating, nausea, and headache. However, these effects were short-lived and were presented at the same frequency between the experimental and placebo groups (60). Patients will be queried after each tDCS session as to whether they experienced adverse effects and how these effects were related to the tDCS treatment. Stimulation sessions have been established by Dr. André Russowski Brunoni, Assistant Professor in the Division of Psychiatry of HC-FMUSP, who will provide any assistance if necessary.
Several advantages of tDCS have been highlighted in clinical practice. These advantages include few side effects that are usually benign, high tolerability, and good potential for efficacy. Notably, it has been emphasized that this technique “has been used in several clinical trials in the last decade and to date, no serious adverse effect has been reported” (58).
Discussion and Dissemination
This study protocol aims to investigate the neuromodulatory effects of tDCS in patients with a history of MTBI who developed PPCS with a current subjective complaint involving long-term episodic memory, working memory, and executive function. Additionally, the study aims to verify the hypothesis that tDCS exerts pro-cognitive effects in the described population.
Interesting findings have emerged from both clinical trials and neuropsychological studies using tDCS. Knowledge about the cognitive and behavioral functions of brain lesions together with sophisticated neuroimaging techniques have provided major contributions to the fields of neuropsychology and cognitive neuroscience.
The interest in this topic arises from the understanding that neuromodulation techniques can provide causal data that answer questions about the effect of stimulation on cortical structures and specific cognitive functions. The modulatory effect of neuromodulatory stimulation on executive function is of particular interest for understanding the mechanisms underlying the integration of cognition with behavior.
The data that will be obtained in this study may help to provide a step forward for neuropsychology and cognitive neuroscience, as the results will help to reveal brain functioning and the effects derived from interventions. This study also may produce new information regarding the possible pro-cognitive effects of tDCS. Therefore, therapeutic interventions in subsequent studies may be investigated, since the present study will use only a single session of tDCS. We decided to initially study the immediate effects of tDCS in such patients because of the following reasons: (1) we will study a specific population of TBI patients, then, as the first study to evaluate the referred outcomes, we believe that we need to have preliminary data to move forward. (2) We do not know what is the best region to be stimulated, and this trial probably will be able to solve this issue.
This study is expected to initiate a discussion about PPCS thus contributing to the creation of public health policies to treat this underdiagnosed disease. On one hand, PPCS affects a patient’s life in social, work, and cognitive contexts. On the other hand, these patients are poorly supported, and their condition is rarely established based on the findings of imaging exams; this lack of evidence could lead to difficulty in diagnosing and treating PPCS patients.
We believe that tDCS holds great promise. It has been shown in previous studies that tDCS is successful, capable, inexpensive, and safe for use in the treatment of a wide range of neurological conditions. Thus, the application of tDCS might improve the efficiency of different neurorehabilitation techniques and provide further relief to patients suffering from long-term disabilities.
Ethics Statement
Ethics approval has been obtained from the Ethics Committee for Analysis of Research Projects, Hospital das Clínicas, University of São Paulo (CAPPesq 612.643/14). Written informed consent will be obtained from all participants.
Author Contributions
RA participated in conception and design of the study, manuscript writing, and its final approval. AB designed the study and helped with data analysis. MO recruited patients, designed the neuropsychological assessment battery, and performed the neuropsychological assessments. AZ recruited patients and designed the neuropsychological assessment battery. MN performed tDCS applications, collected data, reviewed the literature, recruited patients, and contributed to patient follow-up. VG, IN, GB, ML, WP, and AA participated in the conception and design of the study. MT conceived the study and revised the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to acknowledge “Serviço Interdisciplinar de Neuromodulação—IPQ/HCFMUSP” under the coordination of AB for providing the tDCS equipment and consultation rooms to perform all tDCS sessions. The authors thank Mrs. Sandra Aparecida de Lima Falcon for her assistance in scheduling all patients for tDCS sessions.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sector.
References
1. Naunheim RS, Matero D, Fucetola R. Assessment of patients with mild concussion in the emergency department. J Head Trauma Rehabil (2008) 23:116–22. doi: 10.1097/01.HTR.0000314530.30401.70
2. Stuart B, Mandleco B, Wilshaw R, Beckstrand RL, Heaston S. Mild traumatic brain injury: are ED providers identifying which patients are at risk? J Emerg Nurs (2012) 38:425–42. doi:10.1016/j.jen.2011.04.006
3. McCauley SR, Boake C, Levin HS, Contant CF, Song JX. Postconcussional disorder following mild to moderate traumatic brain injury: anxiety, depression, and social support as risk factors and comorbidities. J Clin Exp Neuropsychol (2001) 23:792–808. doi:10.1076/jcen.23.6.792.1016
4. Ruffolo CF, Friedland JF, Dawson DR, Colantonio A, Lindsay PH. Mild traumatic brain injury from motor vehicle accidents: factors associated with return to work. Arch Phys Med Rehabil (1999) 80:392–8. doi:10.1016/S0003-9993(99)90275-7
5. Lima DP, Simão Filho C, Abib Sde C, de Figueiredo LF. Quality of life and neuropsychological changes in mild head trauma. Late analysis and correlation with S100B protein and cranial CT scan performed at hospital admission. Injury (2008) 39:604–11. doi:10.1016/j.injury.2007.11.008
6. Ahman S, Saveman BI, Styrke J, Björnstig U, Stålnacke BM. Long-term follow-up of patients with mild traumatic brain injury: a mixed-methods study. J Rehabil Med (2013) 45:758–64. doi:10.2340/16501977-1182
7. Willemse-van Son AH, Ribbers GM, Verhagen AP, Stam HJ. Prognostic factors of long-term functioning and productivity after traumatic brain injury: a systematic review of prospective cohort studies. Clin Rehabil (2007) 21:1024–37. doi:10.1177/0269215507077603
8. Lundin A, de Boussard C, Edman G, Borg J. Symptoms and disability until 3 months after mild TBI. Brain Inj (2006) 20:799–806. doi:10.1080/02699050600744327
9. Prigatano GP, Gale SD. The current status of postconcussion syndrome. Curr Opin Psychiatry (2011) 24:243–50. doi:10.1097/YCO.0b013e328344698b
10. Bigler ED. Distinguished neuropsychologist award lecture 1999. The lesion(s) in traumatic brain injury: implications for clinical neuropsychology. Arch Clin Neuropsychol (2001) 16:95–131. doi:10.1016/S0887-6177(00)00095-0
11. King N. Mild head injury: neuropathology, sequelae, measurement and recovery. Br J Clin Psychol (1997) 36:161–84. doi:10.1111/j.2044-8260.1997.tb01405.x
12. Datta SG, Pillai SV, Rao SL, Kovoor JM, Chandramouli BA. Post-concussion syndrome: correlation of neuropsychological deficits, structural lesions on magnetic resonance imaging and symptoms. Neurol India (2009) 57:594–8. doi:10.4103/0028-3886.57810
13. Howell D, Osternig L, Van Donkelaar P, Mayr U, Chou LS. Effects of concussion on attention and executive function in adolescents. Med Sci Sports Exerc (2013) 45(6):1030–7. doi:10.1249/MSS.0b013e3182814595
14. Riggio S, Wong M. Neurobehavioral sequelae of traumatic brain injury. Mt Sinai J Med (2009) 76:163–72. doi:10.1002/msj.20097
15. Bigler ED. Neuropsychology and clinical neuroscience of persistent post-concussive syndrome. J Int Neuropsychol Soc (2008) 14:1–22. doi:10.1017/S135561770808017X
16. Lezak MD, Howieson DB, Bigler ED, Tranel D. Neuropsychological Assessment. 5th ed. Newyork, NY: Oxford Press (2012).
17. Cerruti C, Schlaug G. Anodal transcranial direct current stimulation of the prefrontal cortex enhances complex verbal associative thought. J Cogn Neurosci (2009) 21:1980–7. doi:10.1162/jocn.2008.21143
18. Dockery CA, Hueckel-Weng R, Birbaumer N, Plewnia C. Enhancement of planning ability by transcranial direct current stimulation. J Neurosci (2009) 29:7271–7. doi:10.1523/JNEUROSCI.0065-09.2009
19. Dresler M, Sandberg A, Ohla K, Bublitz C, Trenado C, Mroczko-Wasowicz A, et al. Non-pharmacological cognitive enhancement. Neuropharmacology (2013) 64:529–43. doi:10.1016/j.neuropharm.2012.07.002
20. Koski L, Kolivakis T, Yu C, Chen JK, Delaney S, Ptito A. Noninvasive brain stimulation for persistent postconcussion symptoms in mild traumatic brain injury. J Neurotrauma (2015) 32(1):38–44. doi:10.1089/neu.2014.3449
21. Leśniak M, Polanowska K, Seniów J, Członkowska A. Effects of repeated anodal tDCS coupled with cognitive training for patients with severe traumatic brain injury: a pilot randomized controlled trial. J Head Trauma Rehabil (2014) 29(3):E20–9. doi:10.1097/HTR.0b013e318292a4c2
22. Ulam F, Shelton C, Richards L, Davis L, Hunter B, Fregni F, et al. Cumulative effects of transcranial direct current stimulation on EEG oscillations and attention/working memory during subacute neurorehabilitation of traumatic brain injury. Clin Neurophysiol (2015) 126(3):486–96. doi:10.1016/j.clinph.2014.05.015
23. Kang EK, Kim DY, Paik NJ. Transcranial direct current stimulation of the left prefrontal cortex improves attention in patients with traumatic brain injury: a pilot study. J Rehabil Med (2012) 44(4):346–50. doi:10.2340/16501977-0947
24. Bolognini N, Pascual-Leone A, Fregni F. Using non-invasive brain stimulation to augment motor training-induced plasticity. J Neuroeng Rehabil (2009) 6:8. doi:10.1186/1743-0003-6-8
25. Demirtas-Tatlidede A, Vahabzadeh-Hagh AM, Bernabeu M, Tormos JM, Pascual-Leone A. Noninvasive brain stimulation in traumatic brain injury. J Head Trauma Rehabil (2012) 27:274–92. doi:10.1097/HTR.0b013e318217df55
26. Bonnì S, Mastropasqua C, Bozzali M, Caltagirone C, Koch G. Theta burst stimulation improves visuo-spatial attention in a patient with traumatic brain injury. Neurol Sci (2013) 34(11):2053–6. doi:10.1007/s10072-013-1412-y
27. Louise-Bender Pape T, Rosenow J, Lewis G, Ahmed G, Walker M, Guernon A, et al. Repetitive transcranial magnetic stimulation-associated neurobehavioral gains during coma recovery. Brain Stimul (2009) 2:22–35. doi:10.1016/j.brs.2008.09.004
28. Angelakis E, Liouta E, Andreadis N, Korfias S, Ktonas P, Stranjalis G, et al. Transcranial direct current stimulation effects in disorders of consciousness. Arch Phys Med Rehabil (2014) 95:283–9. doi:10.1016/j.apmr.2013.09.002
29. Boggio PS, Bermpohl F, Vergara AO, Muniz AL, Nahas FH, Leme PB, et al. Go-no-go task performance improvement after anodal transcranial DC stimulation of the left dorsolateral prefrontal cortex in major depression. J Affect Disord (2007) 101:91–8. doi:10.1016/j.jad.2006.10.026
30. Fecteau S, Fregni F, Boggio PS, Camprodon JA, Pascual-Leone A. Neuromodulation of decision-making in the addictive brain. Subst Use Misuse (2010) 45:1766–86. doi:10.3109/10826084.2010.482434
31. Van den Eynde F, Claudino AM, Mogg A, Horrell L, Stahl D, Ribeiro W, et al. Repetitive transcranial magnetic stimulation reduces cue-induced food craving in bulimic disorders. Biol Psychiatry (2010) 67:793–5. doi:10.1016/j.biopsych.2009.11.023
32. Cotelli M, Manenti R, Brambilla M, Petesi M, Rosini S, Ferrari C, et al. Anodal tDCS during face-name associations memory training in Alzheimer’s patients. Front Aging Neurosci (2014) 6:38. doi:10.3389/fnagi.2014.00038
33. Pereira JB, Junqué C, Bartrés-Faz D, Martí MJ, Sala-Llonch R, Compta Y, et al. Modulation of verbal fluency networks by transcranial direct current stimulation (tDCS) in Parkinson’s disease. Brain Stimul (2013) 6(1):16–24. doi:10.1016/j.brs.2012.01.006
34. Kang EK, Baek MJ, Kim S, Paik NJ. Non-invasive cortical stimulation improves post-stroke attention decline. Restor Neurol Neurosci (2009) 27(6):645–50. doi:10.3233/RNN-2009-0514
35. Jo JM, Kim YH, Ko MH, Ohn SH, Joen B, Lee KH. Enhancing the working memory of stroke patients using tDCS. Am J Phys Med Rehabil (2009) 88(5):404–9. doi:10.1097/PHM.0b013e3181a0e4cb
36. Park SH, Koh EJ, Choi HY, Ko MH. A double-blind, sham-controlled, pilot study to assess the effects of the concomitant use of transcranial direct current stimulation with the computer assisted cognitive rehabilitation to the prefrontal cortex on cognitive functions in patients with stroke. J Korean Neurosurg Soc (2013) 54(6):484–8. doi:10.3340/jkns.2013.54.6.484
37. Jones KT, Stephens JA, Alam M, Bikson M, Berryhill ME. Longitudinal neurostimulation in older adults improves working memory. PLoS One (2015) 10:e0121904. doi:10.1371/journal.pone.0121904
38. Vanderhasselt MA, De Raedt R, Brunoni AR, Campanhã C, Baeken C, Remue J, et al. tDCS over the left prefrontal cortex enhances cognitive control for positive affective Stimuli. PLoS One (2013) 8:e62219. doi:10.1371/journal.pone.0062219
39. Wu YJ, Tseng P, Chang CF, Pai MC, Hsu KS, Lin CC, et al. Modulating the interference effect on spatial working memory by applying transcranial direct current stimulation over the right dorsolateral prefrontal cortex. Brain Cogn (2014) 91:87–94. doi:10.1016/j.bandc.2014.09.002
40. Bueno VF, Brunoni AR, Boggio PS, Bensenor IM, Fregni F. Mood and cognitive effects of transcranial direct current stimulation in post-stroke depression. Neurocase (2011) 17:318–22. doi:10.1080/13554794.2010.509319
41. Goldman RL, Borckardt JJ, Frohman HA, O’Neil PM, Madan A, Campbell LK, et al. Prefrontal cortex transcranial direct current stimulation (tDCS) temporarily reduces food cravings and increases the self-reported ability to resist food in adults with frequent food craving. Appetite (2011) 56:741–6. doi:10.1016/j.appet.2011.02.013
42. Boggio PS, Ferrucci R, Rigonatti SP, Covre P, Nitsche M, Pascual-Leone A, et al. Effects of transcranial direct current stimulation on working memory in patients with Parkinson’s disease. J Neurol Sci (2006) 249(1):31–8. doi:10.1016/j.jns.2006.05.062
43. Boggio PS, Khoury LP, Martins DC, Martins OE, de Macedo EC, Fregni F. Temporal cortex direct current stimulation enhances performance on a visual recognition memory task in Alzheimer disease. J Neurol Neurosurg Psychiatry (2009) 80:444–7. doi:10.1136/jnnp.2007.141853
44. Boggio PS, Fregni F, Valasek C, Ellwood S, Chi R, Gallate J, et al. Temporal lobe cortical electrical stimulation during the encoding and retrieval phase reduces false memories. PLoS One (2009) 4:e4959. doi:10.1371/journal.pone.0004959
45. Yun GJ, Chun MH, Kim BR. The effects of transcranial direct-current stimulation on cognition in stroke patients. J Stroke (2015) 17(3):354–8. doi:10.5853/jos.2015.17.3.354
46. Rossi S, Hallett M, Rossini PM, Pascual-Leone A; Safety of TMS Consensus Group. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin Neurophysiol (2009) 120:2008–39. doi:10.1016/j.clinph.2009.08.016
47. King NS, Crawford S, Wenden FJ, Moss NE, Wade DT. The Rivermead Post Concussion Symptoms Questionnaire: a measure of symptoms commonly experienced after head injury and its reliability. J Neurol (1995) 242:587–92. doi:10.1007/BF00868811
48. Beck AT. An inventory for measuring depression. Arch Gen Psychiatry (1961) 4:561–71. doi:10.1001/archpsyc.1961.01710120031004
49. Gorenstein C, Andrade L. Validation of a Portuguese version of the Beck Depression Inventory and the State-Trait Anxiety Inventory in Brazilian subjects. Braz J Med Biol Res (1996) 29:453–7.
50. Benedict RHB, Schretlen D, Groninger L. Hopkins verbal learning test – revised: normative data and analysis of inter-form and test-retest reliability. Clin Neuropsychol (1998) 12:43–55. doi:10.1076/clin.12.1.43.1726
51. Brandt J, Benedict RHB. The Hopkins Verbal Learning Test Revised: Professional Manual. Odessa, FL: Psychological Assessment Resources, Inc (2001).
52. Weschler D. Weschler Adult Intelligence Scale. San Antonio, TX: The Psychological Corporation (1997).
53. Spreen O, Strauss E. A Compendium of Neuropsychological Tests Administration Norms and Commentary. New York, NY: Oxford University Press (1998).
54. Garavan H, Ross TJ, Stein EA. Right hemispheric dominance of inhibitory control: an event-related functional MRI study. Proc Natl Acad Sci U S A (1999) 96:8301–6. doi:10.1073/pnas.96.14.8301
55. Bajaj JS, Hafeezullah M, Franco J, Varma RR, Hoffmann RG, Knox JF, et al. Inhibitory control test for the diagnosis of minimal hepatic encephalopathy. Gastroenterology (2008) 135:1591–600. doi:10.1053/j.gastro.2008.07.021
56. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform (2009) 42(2):377–81. doi:10.1016/j.jbi.2008.08.010
57. U.S. Department of Health and Human Services. Health Insurance Portability and Accountability Act of 1996 (HIPAA) Privacy, Security and Breach Notification Rules. USA Public law (1996) (Vol 104), 191 p.
58. Brunoni AR, Nitsche MA, Bolognini N, Bikson M, Wagner T, Merabet L, et al. Clinical research with transcranial direct current stimulation (tDCS): challenges and future directions. Brain Stimul (2012) 5:175–95. doi:10.1016/j.brs.2011.03.002
59. Nitsche MA, Cohen LG, Wassermann EM, Priori A, Lang N, Antal A, et al. Transcranial direct current stimulation: state of the art 2008. Brain Stimul (2008) 1:206–23. doi:10.1016/j.brs.2008.06.004
Keywords: brain injuries, post-concussion syndrome, transcranial direct current stimulation, non-invasive brain stimulation, crossover studies
Citation: de Amorim RLO, Brunoni AR, Oliveira MAF, Zaninotto ALC, Nagumo MM, Guirado VMP, Neville IS, Benute GRG, de Lucia MCS, Paiva WS, Andrade AF and Teixeira MJ (2017) Transcranial Direct Current Stimulation for Post-Concussion Syndrome: Study Protocol for a Randomized Crossover Trial. Front. Neurol. 8:164. doi: 10.3389/fneur.2017.00164
Received: 31 October 2016; Accepted: 07 April 2017;
Published: 02 May 2017
Edited by:
Mattias K. Sköld, Uppsala University, SwedenReviewed by:
Eric Peter Thelin, University of Cambridge, UKLynda Mainwaring, University of Toronto, Canada
Copyright: © 2017 Amorim, Brunoni, Oliveira, Zaninotto, Nagumo, Guirado, Neville, Benute, de Lucia, Paiva, Andrade and Teixeira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robson Luis Oliveira de Amorim, amorim.robson@gmail.com