 Aníbal García-Sempere1,2*
Aníbal García-Sempere1,2* Daniel Bejarano-Quisoboni1
Daniel Bejarano-Quisoboni1 Julián Librero2,3
Julián Librero2,3 Clara L. Rodríguez-Bernal1,2Salvador Peiró1,2
Clara L. Rodríguez-Bernal1,2Salvador Peiró1,2 Gabriel Sanfélix-Gimeno1,2
Gabriel Sanfélix-Gimeno1,2- 1Center for Public Health Research (CSISP-FISABIO), Valencia, Spain
- 2Spanish Network of Chronic Care and Health Services Research (REDISSEC), Valencia, Spain
- 3Navarrabiomed Biomedical Research Centre, Pamplona, Spain
Introduction: Beyond clinical trials, clinical practice guidelines, and administrative regulation, treatment decision-making can be influenced by individual and contextual factors. Our goal was to describe variations in the patterns of initiation of anticoagulation therapy in patients with atrial fibrillation by Health Areas (HA) in the region of Valencia in Spain and to quantify the influence of the HAs on variations in treatment choice.
Methods: We conducted a population-based retrospective cohort study of all atrial fibrillation patients who started treatment with oral anticoagulants between November 2011 and February 2014 in each of the region's 24 HAs. We described patient and utilization characteristics per HA and initiation patterns over time, and we identified contextual and individual factors associated with differences in initiation patterns.
Results: 21,879 patients initiated treatment with an oral anticoagulant in the 24 HAs. Initiation with direct oral anticoagulants (DOAC) in the first year was 14.6%. In November 2013 the ratio was 25.4%, with HA ratios ranging from 3.8 to 57.1%. DOAC-initiating patients had less comorbidity but were more likely to present episodes of previous ischemic stroke, hemorrhagic stroke, or TIA when compared with patients initiating with VKA treatment. Variability among HAs was statistically significant, with the majority of HAs ranking above or below the regional initiation average (ICC ≈ 8%).
Conclusion: There was high variability in the percentage of DOAC initiation and in the choice of DOAC among HAs. Interventions aimed to improve DOAC initiation decision-making and to reduce variations should take into account the Health Area component.
Introduction
Atrial fibrillation (AF) increases the risk of stroke, which in turn, leads to cerebrovascular morbidity, neurological disability, loss of quality of life, and death (Jørgensen et al., 1996; Lin et al., 1996). Population-based studies in developed countries have shown a strong age gradient, with a prevalence of 6.6 men and 3.9 women for every 1,000 people of the respective gender (Chugh et al., 2014). Vitamin K antagonists (VKA) such as warfarin are highly effective in the prevention of stroke in AF patients, with several randomized clinical trials showing decreases in its incidence of more than 50% (1991; 1994; Petersen et al., 1989; The Boston Area Anticoagulation Trial for Atrial Fibrillation Investigators et al., 1990; Lancaster et al., 1991). Consequently, the use of VKA has been the standard therapy for AF patients at the highest risk of a stroke (Fuster et al., 2012; January et al., 2014). However, the treatment withVKA is subject to many limitations such as a higher risk of bleeding, the requirement of regular monitoring, and the presence of several drug–drug and drug–food interactions.
In recent years, novel direct oral anticoagulants (DOACs) such as dabigatran, rivaroxaban, apixaban, and edoxaban, have entered the market following the pivotal phase-III trials reporting efficacy and safety features and rates comparable to those of warfarin (Connolly et al., 2009; Granger et al., 2011; Patel et al., 2011; Giugliano et al., 2013). DOACs are considered a more convenient therapy, as they have lesser interactions than VKA treatments, simpler dosing regimes and the absence of need for INR monitoring. However, they also have important limitations, such as the low availability of antidotes to reverse their effect, their renal implications, the current lack of tests for monitoring their anticoagulant effectiveness, and the fact that the cost per day of treatment with DOACs is much higher than that of VKAs, including monitoring costs. Recently, real-world studies are shedding some light on whether or not the advantages of DOACs demonstrated in pivotal trials are being reflected in routine clinical practice (Potpara and Lip, 2017). Closely linked to safety and effectiveness outcomes in daily practice, the study of local patterns of use can provide relevant information for improving the management of patients with atrial fibrillation, and is essential to adequately interpret local real-world evidence.
To the best of our knowledge, patterns of real-world use of VKA and DOAC have barely been studied in other contexts (Brais et al., 2015; Olesen et al., 2015; Patel et al., 2015). In Spain, only one recently published study tackles this issue (Rodríguez-Bernal et al., 2017). DOAC prescription is subject to prior authorization in the Spanish National Health System, compelling the prescriber to get its prescription validated—by a so-called “medical inspector”—before it is accepted for public funding and dispensing. This validation relies on criteria fixed by the Ministry of Health. These criteria place DOAC as a second line therapy, and initiation of treatment with a DOAC is restricted to VKA contraindication, impossibility of accessing INR control facilities, or being at high risk of intracranial hemorrhage (ACOD, 2016). According to these formal strict regulatory rules, little variations in patterns of use, and initiation with DOAC among territories and neighboring populations with very similar demographic and epidemiological characteristics should be expected.
However, beyond the evidence provided by clinical trials, the recommendations of clinical practice guidelines, and the rules of administrative regulation, treatment decisions and the choice of a particular drug can be influenced by patient characteristics, physician, and organizational factors, pharmaceutical promotion, and healthcare system characteristics (Eisenberg, 2002). While a significant amount of literature about small area variations analysis (SAVA) in surgical and medical hospitalizations and healthcare spending has been an essential element for interpreting the behavior of healthcare providers and defining public policies (Wennberg et al., 2002; Fisher et al., 2003a,b; National Research Council., 2013), studies examining geographical variations in pharmaceutical prescribing have been scarce (Anis et al., 1996; Dubois et al., 2002) until recent years (Zhang et al., 2010a,b, 2012; Donohue et al., 2012) and, to our knowledge, none have addressed the contextual variability in VKA and DOAC drug utilization. Furthermore, because stroke prevention in atrial fibrillation treatment can be managed by several medical specialists (hematologists, cardiologists, and neurologists, among others) and primary care physicians, the role of the different levels of care explaining the geographical variations seems of special interest. This study aims to describe variations in the patterns of initiation of anticoagulation therapy in patients with atrial fibrillation in the region of Valencia in Spain, and to quantify the influence of the geographical healthcare administrative boundaries (Health Areas) on variations in treatment choice.
Methods
Design and Setting
This population-based retrospective cohort study was conducted in the Valencia Health Agency (VHA), the public health system of the region of Valencia in Spain, covering about 97% of the region's population (5 million inhabitants). We created a cohort with all naïve patients with diagnosed AF [diagnosis code of International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) 427.31] who started treatment with oral anticoagulants (warfarin, acenocoumarol, dabigatran, rivaroxaban, apixaban) between November 2011 (date of the market launch of dabigatran) and February 2014, in each of the 24 Health Areas (HAs, the administrative and territorial management units) that make up the public health care provision network in the region. We defined the naïve population as those patients without anticoagulant treatment prescribed in the 12 months preceding the first prescription in our analysis time window. People without pharmaceutical/health coverage by VHA, mainly some government employees whose prescriptions are reimbursed by civil service insurers, and thus not included in the pharmacy databases of the VHA, and patients not registered in the municipal census (non-residents or temporary residents), or who left the region or who were disenrolled from VHA coverage for other causes, were excluded because of limitations on follow-up. A patient flowchart has already been published elsewhere in Frontiers (Rodríguez-Bernal et al., 2017).
Source
Information was obtained from the electronic information systems of the VHA. The Population Information System (SIP) provides information on the population under VHA coverage and registers some demographic characteristics, including the geographical/contextual situation of each person and dates and causes of VHA discharge, including death. The Minimum Basic Dataset (MBDS) at hospital discharge is a synopsis of clinical and administrative information on all hospital discharges, including diagnoses and procedures. The electronic medical record for ambulatory care (EMR), available in all primary healthcare centers and ambulatory facilities, has information about diagnoses, personal, and family medical history, laboratory results, lifestyle, etc. as well as information about both physician prescriptions and dispensations from pharmacy claims. All the information in these systems is linked at an individual level through a unique identifier.
Covariates
Variables potentially related to the risk of atrial fibrillation and the use of oral anticoagulants in the study population over the study period were considered. These included demographic characteristics, comorbidities, use of DOAC and healthcare resource utilization in the preceding 12 months. Based on comorbidity information, we calculated and added relevant patient-level risk predictor scores—CHADS2, CHA2DS2-VASC, and HAS-BLED scores– to the dataset.
Analysis
We first described sociodemographic and clinical patient and healthcare utilization measures per Health Area. Second, to describe HA initiation patterns over time, we calculated monthly percentages of treatment initiation with either a VKA or a DOAC. Third, we examined the variability in the percentage of initiation with VKA and with each different DOAC per HA, based on data from the last trimester of the study window (Nov 2013 to Feb 2014). Fourth, to identify contextual and individual factors associated with differences in initiation patterns, we used multilevel regression analyses with random effects with patients (first level) nested within HAs (second level) and we compared the output of the empty model (a model considering only the HA component) with models adding individual variables (Model I) and risk scores (Models II and III). Finally, we ranked HAs with respect to the regional average of the percentage of initiation to visualize inter-area differences by means of a caterpillar plot. All analyses were performed using R 3.2.3 (R Foundation) statistical software.
Ethics
The study protocol was approved by the regional Ethics Committee for Clinical Research of the General Directorate of Public Health and the Centre for Public Health Research. Patient informed consent was not required because datasets were extracted with anonymized identifiers according to Spanish laws on privacy (Act 15/1999) and patients' rights (Act 41/2002).
Results
Patient Characteristics and Healthcare Utilization
During the study period a total of 21,879 patients initiated treatment with an oral anticoagulant in the 24 Health Areas. For the annual period from November 2011 to November 2012, the total ratio of initiation with a DOAC was 14.6%. For the whole period, initiation with a DOAC was 18%, with HA rates ranging from 4.7 to 27.8%, thus implying a six-fold difference among HAs. In the month of November 2013, 2 years after the first prescription of a DOAC, the regional initiation share was 25.4%, ranging from 3.8 to 57.1%. Mean patient age was 75 years old and 48% of patients were females, with hypertension being by far the most frequent comorbidity (79%) followed by diabetes (31%) and history of bleeding or predisposition to bleeding (23%). The average number of medications per patient was 9.89, ranging from 8.70 to 10.99. The average ambulatory cardiology visits was 0.47, with HAs ranging from 0.13 to 0.85—again showing a six-fold difference among HAs (Table 1).
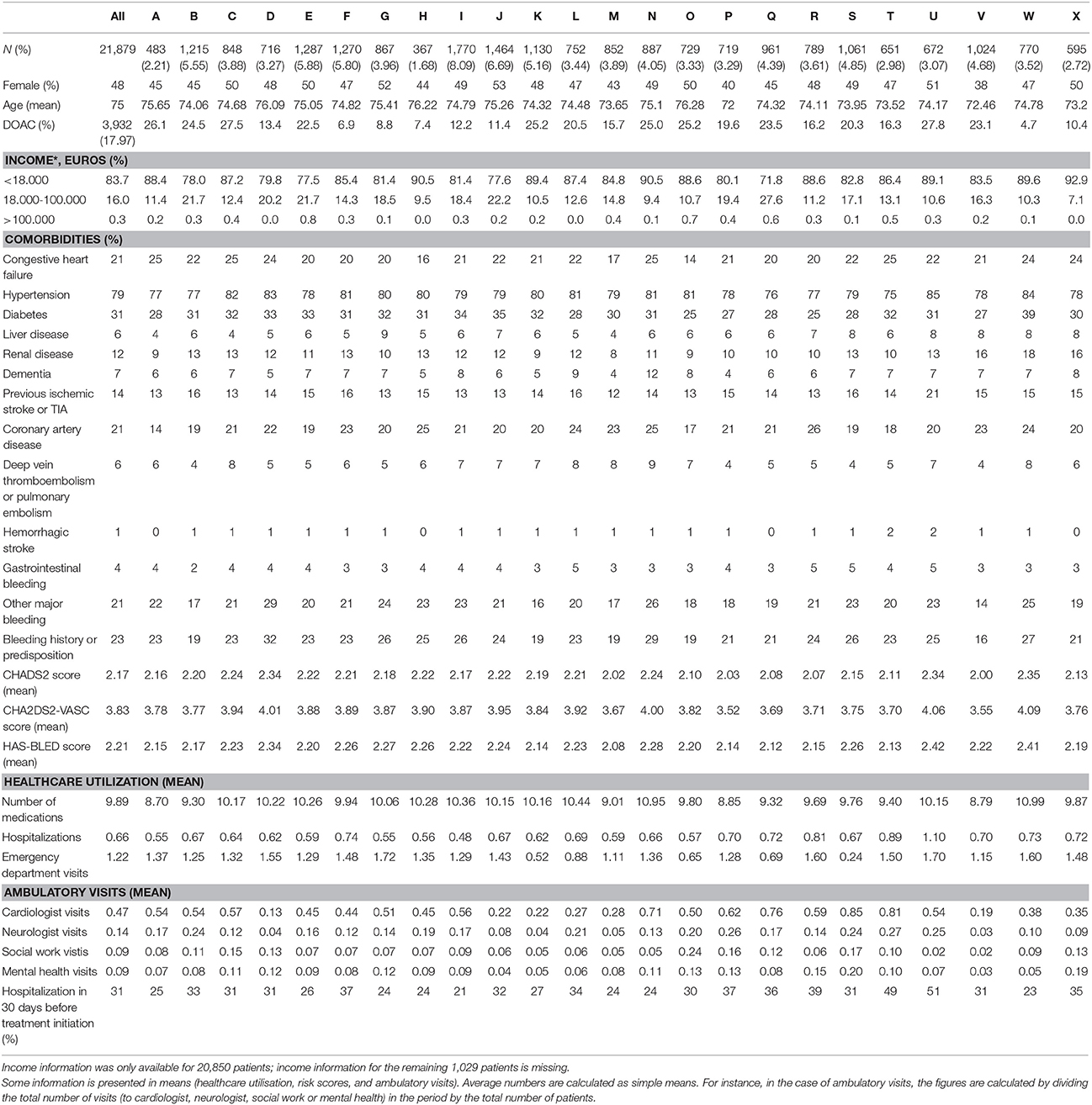
Table 1. Demographics, clinical characteristics, and healthcare utilization of the cohort per Health Areas.
Initiation Time Trends
Descriptive time trends of relative–VKA vs. DOAC–treatment initiation in the 24 HAs are presented in Figure 1. Trends in DOAC uptake differ among HAs, with some areas maintaining a modest introduction of DOAC as an initial therapy throughout the study period (for instance, areas F, G, I, J, or W show a monthly DOAC initiation share of below 25% for the whole period), while others show increasing levels of DOAC penetration over time (see areas B, K, N, P, or Q, where DOAC initiation rises from 25 to 50% at the end of the study window). Still, in some HAs the pace of DOAC initiation is sharp enough to overtake the ratio of VKA initial prescription at specific moments of time (areas A, C, and U where % of DOAC initiation surpasses 50% in certain months).
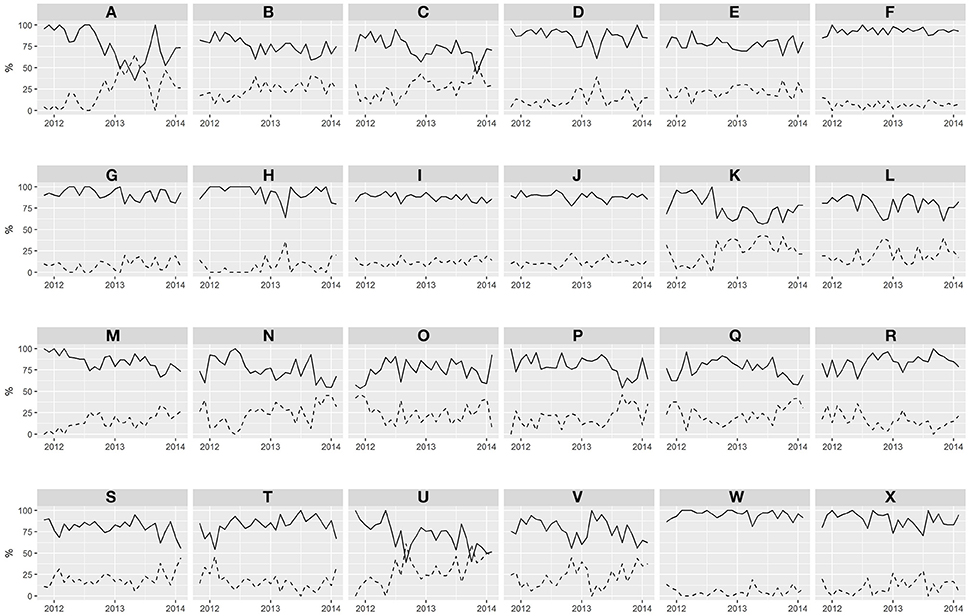
Figure 1. Time trends of the percentage of initiation with VKA or DOAC per Health Areas over time. Letters A to X represents the 24 HAs. Solid line: % of initiation with VKA. Dotted line: % of initiation with DOAC.
With regard to the choice of DOAC per HA, Figure 2 shows that the relative percentage of initiation with apixaban, dabigatran, or rivaroxaban in the last trimester of the study period (Dec 2013 to Feb 2014) is highly variable. For instance, in areas D and F apixaban is not prescribed while it leads area T with 1.7% of the initiation share. Rivaroxaban is not prescribed in Area T but is the leading DOAC of choice for initiation in 15 HAs, with a share of up to 25% of initiations in one area. The first comer, dabigatran, 2 years after its launch, still leads initiation in seven territories but with more modest shares, always below 15%. Also worth noting is the variation in the relative penetration of total DOAC initiation, with HAs ranging from 7.1% of initiation with DOAC for the considered trimester to 47.6%, thus entailing once again a more-than six-fold difference among areas.
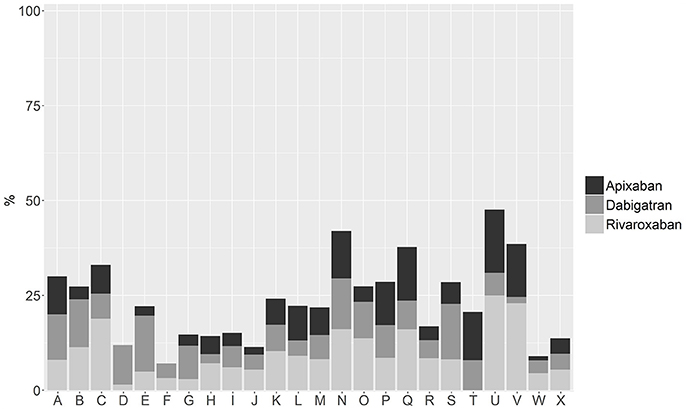
Figure 2. Choice of DOAC as initiation therapy per Health Area, expressed as a percentage of total initiation, for the period December 2013 to February 2014.
Analysis of Associations
Table 2 presents a multilevel analysis showing the specific associations between individual and contextual (Health Area) characteristics and DOAC initiation in the study period as well as the analysis of variance and the values of the Intra-Class Correlation statistic (ICC) for the different models. Regarding the influence of the HA on initiation patterns, variability among HAs was statistically significant. ICC was 8.51% in the empty model, 8.07, 8.04, and 8.12% in models I, II, and III, respectively. Median Odds Ratio of the effect of HA heterogeneity on initiation variability was 1.70 for the empty model and 1.67 for models I, II, and III.
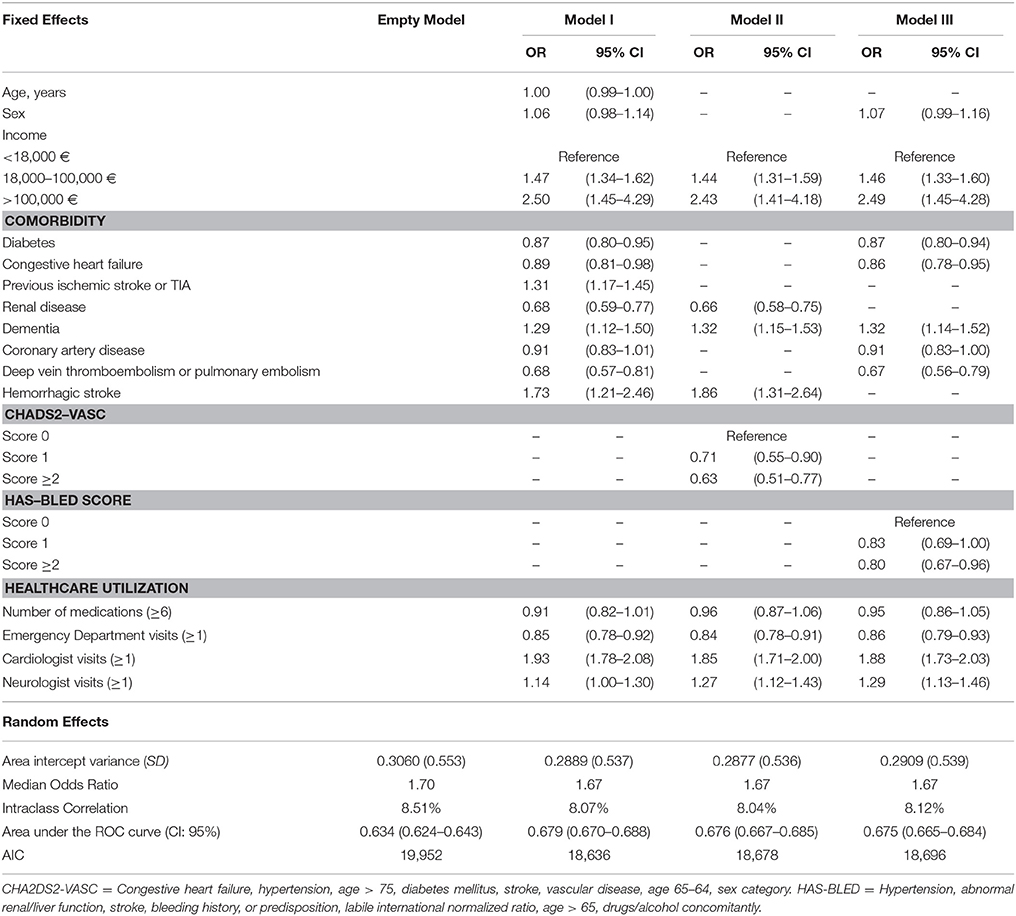
Table 2. Predicting factors of DOAC initiation. Multilevel analysis results.
In Model I, where individual characteristics are added to the empty model, DOAC-initiating patients were less likely to have comorbidities such as diabetes (OR:0.87), renal disease (OR:0.68), deep vein thromboembolism or pulmonary embolism (OR:0.68), but were more likely to present episodes of previous stroke or TIA (OR:1.31) and hemorrhagic stroke (OR:1.73) when compared with patients initiating with VKA treatment. Patients initiating with DOAC showed fewer ED (OR:0.85) visits but more visits to a cardiologist in the 12 months preceding the index prescription (OR:1.93). In Models II and III, in which we incorporate risk prediction scores, we found that an increased risk of stroke and bleeding as captured by CHADS2 and HAS BLED scores was significantly associated with lower odds of DOAC initiation. Also, higher income was associated with a significant increase in the likelihood of initiating with a DOAC instead of VKA (OR: 2.50, 2.43, and 2.49 in Models I, II, and III).
With regard to discriminatory accuracy, AUC in the empty model was 0.634. Information provided by individual variables in model I resulted in an increase of AUC over the empty model of 0.045 units. Inclusion of risk scores in models II and III did not further increase discriminatory ability.
Finally, we ranked HAs according to their mean likelihood of DOAC initiation with regard to the regional average—see Figure 3. In seven HAs the propensity for DOAC prescription was significantly below the regional average, in 11 the propensity for DOAC prescription was significantly higher than average, and six areas showed no difference with the regional average.
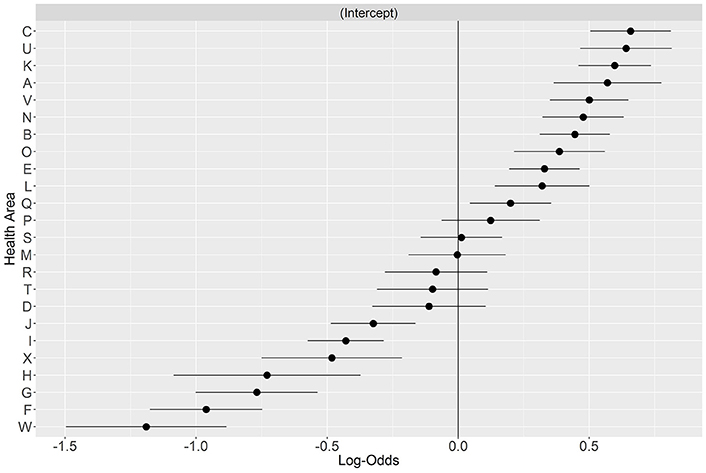
Figure 3. Variation in initiation with a DOAC per Health Area. HAs are ranked with respect to the regional average.
Discussion
We found that HAs are contextual level factors that significantly influence patterns of oral anticoagulation initiation in patients with atrial fibrillation in the region of Valencia, regardless of individual characteristics. The HA of residence was, together with some individual variables, one of the most important factors of variation in the choice of anticoagulant treatment initiation. At patient level, initiation with DOAC was associated with fewer concomitant comorbidities, lower risk of bleeding and stroke according to prediction indexes scores, presence of previous ischemic or hemorrhagic stroke, wealthier status, and with more visits to the cardiologist. To our knowledge, this is the first study to evaluate contextual and individual level factors associated with the initiation of oral anticoagulant therapy in a real world setting.
We observed a marked heterogeneity in the initiation trends among Health Areas, with a high variability in the percentage of DOAC prescription and in the choice of DOAC. Many factors, mainly supply side elements, may be associated with such different trends: inter medical-inspector variability in prior-authorization decision-making, level of ability of the HA pharmacy managers to influence specialist and primary care prescription, or different prescriber risk aversion in the face of uncertainties when prescribing. In some HAs DOAC initiation peaks coinciding in time with DOAC launches can be observed, suggesting that a variation gradient may come from differential promotion intensity and sensitivity. The variations observed in the patterns of oral anticoagulant initiation among patients with atrial fibrillation, and the ascertainment that the contextual factor “Health Area” exerts a noticeable influence on initiation patterns, may have important implications for patients, payers and the health care system.
The relatively low uptake of DOAC observed in our study when compared to other healthcare systems (Desai et al., 2014; Olesen et al., 2015) is consistent with the formal restriction of DOAC as a second line therapy for stroke prevention in atrial fibrillation patients. Also, renal failure patients were less likely to be initiated with DOAC, which is reasonable as renal precautions are stated on every DOAC Summary of Product Characteristics. Similarly, patients with a previous stroke (ischemic or hemorrhagic) were more likely to initiate on DOACs, which seems logical as those conditions are part of the prior authorization criteria for initiating treatment with a DOAC. On the other hand, some of our results are less foreseeable. Patients that initiate with a DOAC seem to be at lower risk, and this should be taken into account when considering real-life effectiveness. Exploring whether health outcomes are affected by anticoagulant choice (and by DOAC choice when a DOAC is prescribed) and at what cost, should be a research priority to gain a better understanding of the implications of initiation variability and ultimately to be able to provide policy guidance on the matter. Finally, we found that higher income is strongly associated with more than a two-fold odds of being initiated with a DOAC. This could be explained by cost-sharing considerations (González López-Valcárcel et al., 2017), as DOAC entails a higher cost burden to patients than VKA, and doctors may be acting as financial (in addition to clinical) agents to patients (González López-Valcárcel et al., 2011) nevertheless it is a disturbing result that causes concern with regard to the universal and equal access to healthcare resources in the Spanish National Health System.
Limitations
Our study is subject to some limitations. We considered the simplest possible multilevel structure of individuals nested within Health Areas, but we acknowledge that other contexts and/or care levels may influence prescription—such as primary care areas or physicians. However, this is the most common design in neighborhood and health studies (Merlo et al., 2006), and the variables we included in our analyses are appropriate to evaluate differences in the initiation of oral anticoagulation. Despite including many relevant individual variables in our analysis, we cannot rule out the existence of omitted confounding factors; the relatively low values of AUC evidence that the factors considered had a modest discriminatory capacity to distinguish between VKA and DOAC initiators. For instance, we could not include information on the impossibility of accessing INR control facilities or regarding the presence of a contraindication to VKA, as these data are not routinely recorded in linkable clinical databases. These factors could explain some contextual and individual heterogeneity and further research should examine their influence on initiation variation, but their absence does not affect the relevance of our results. Still, in multilevel analyses it is always critical to distinguish between confounder and mediator factors given that place of residence, as well as clinical outcomes, may act as mediators of the Health Area effect (Merlo et al., 2006). Furthermore, cautiousness is needed when establishing causal relationships with observational designs, and neighborhood and health studies are not an exception (Diez Roux, 2004; Merlo et al., 2016). Some contextual effects may be determined by the individual composition of the Health Area while others may be due to independent factors (e.g., better access to a specialist cardiology unit). All in all, our results should be interpreted with caution, and transferability to other contexts may be limited to the Spanish territory.
Conclusions
The main finding of this study is that initiation with oral anticoagulants was influenced by factors both at the patient and the HA level, with the HA level having a greater impact on initiation behavior than many individual variables. The fact that factors not directly related to clinical appropriateness are influencing treatment initiation choice exposes important management issues. Among those, and according to our results, interventions aimed at improving DOAC initiation decision making and at reducing variability should take into account the Health Area component.
In Spain, prior authorization criteria relegate DOAC to a second line therapy. Based on this assumption, low rates of DOAC initiation throughout the country would be expected. However, in our study we showed that in some Health Areas roughly 50% of patients initiate with a DOAC in the region of Valencia, and visiting a cardiologist is associated with a relatively higher initiation with a DOAC. Within Health Areas, the choice of DOAC was also very variable, raising the need to generate more evidence about the factors affecting anticoagulant initiation decision making. Also, the linkage of utilization studies with real-world comparative safety and effectiveness analyses is needed to better seize the pros and cons—and the why's—of new oral anticoagulant use in daily clinical practice as a way to take full advantage of their potential benefits.
Author Contributions
GS, SP, and AG had full access to all the data in the study and take responsibility for its integrity and the accuracy of its analysis. The study was designed by SP and GS and carried out by AG, DB, JL, CR, SP, and GS. JL and DB carried out the data preparation and the statistical analysis. AG drafted the manuscript. All authors participated in the analysis and interpretation of data and critical revision of the manuscript for important intellectual content. All approved the final version submitted for publication and agree to be accountable for all aspects of the work by ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
This work was partially supported by the 2013 Collaboration Agreement between the Fundación para el Fomento de la Investigación Sanitaria y Biomédica (FISABIO) from the Valencia Ministry of Health and Boehringer Ingelheim, a non-conditioned program to conduct independent research in chronic healthcare, pharmacoepidemiology, and medical practice variation. It was also partially supported by the FISABIO grant for Emerging Researchers UGP-15-226. CRB was funded by the grant RD12/0001/0005 from the Carlos III Institute of Health of the Spanish Ministry of Health (co-financed by the European Regional Development Fund). None of the sponsors played any role in the study design, the collection, analysis, or interpretation of data, the writing of the manuscript or in the decision to submit it for publication.
Conflict of Interest Statement
AG is a former employee of Boehringer-Ingelheim. GS has participated in an advisory board meeting for Boehringer-Ingelheim, and SP has participated in scientific meetings for Novartis and Ferrer International.
The other authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The Valencia Regional Health Department (Conselleria de Sanitat Universal i Salut Pública, Generalitat Valenciana) facilitated the primary data used in this study. The views presented here are those of the authors and not necessarily those of the FISABIO Foundation, the Valencia Ministry of Health or the study sponsors.
References
(1991). Stroke prevention in atrial fibrillation study. Final Results. Circulation 84, 527–539. doi: 10.1161/01.CIR.84.2.527
(1994). Warfarin versus aspirin for prevention of thromboembolism in atrial fibrillation: stroke prevention in atrial fibrillation ii study. Lancet 343, 687–691
ACOD (2016). INFORME DE POSICIONAMIENTO TERAPÉUTICO UT_ACOD/V5/21112016. Criterios Y Recomendaciones Generales Para El Uso De Los Anticoagulantes Orales Directos (ACOD) En La Prevención Del Ictus Y La Embolia Sistémica En Pacientes Con Fibrilación Auricular No Valvular. Ministerio de Sanidad, Servicios Sociales e Igualdad. Madrid. Available online at: https://www.aemps.gob.es/medicamentosUsoHumano/informesPublicos/docs/criterios-anticoagulantes-orales.pdf).
Anis, A. H., Carruthers, G., Carter, A. O., and Kierulf, J. (1996). Variability in prescription drug utilization: issues for research. Can. Med. Assoc. J. 154, 635–640
Brais, C., Larochelle, J., Turgeon, M., Tousignant, A., Blais, L., Perreault, S., et al. (2015). Patterns of oral anticoagulants use in atrial fibrillation. J. Popul. Ther. Clin. Pharmacol. 22:e90–e95.
Chugh, S. S., Havmoeller, R., Narayanan, K., Singh, D., Rienstra, M., Benjamin, E. J., et al. (2014). Worldwide epidemiology of atrial fibrillation: a global burden of disease 2010 study. Circulation 129, 837–847. doi: 10.1161/CIRCULATIONAHA.113.005119
Connolly, S. J., Ezekowitz, M. D., Yusuf, S., Eikelboom, J., Oldgren, J., Parekh, A., et al. (2009). Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 361, 1139–1151. doi: 10.1056/NEJMoa0905561
Desai, N. R., Krumme, A. A., Schneeweiss, S., Shrank, W. H., Brill, G., Pezalla, E. J., et al. (2014). Patterns of initiation of oral anticoagulants in patients with atrial fibrillation- quality and cost implications. Am. J. Med. 127, 1075–1082. doi: 10.1016/j.amjmed.2014.05.013
Diez Roux, A. V. (2004). The study of group-level factors in epidemiology: rethinking variables, study designs, and analytical approaches. Epidemiol. Rev. 26, 104–111. doi: 10.1093/epirev/mxh006
Donohue, J. M., Morden, N. E., Gellad, W. F., Bynum, J. P., Zhou, W., Hanlon, J. T., et al. (2012). Sources of regional variation in medicare part D drug spending. N. Engl. J. Med. 366, 530–538. doi: 10.1056/NEJMsa1104816
Dubois, R. W., Batchlor, E., and Wade, S. (2002). Geographic variation in the use of medications: is uniformity good news or bad? Health Aff. 21, 240–250. doi: 10.1377/hlthaff.21.1.240
Eisenberg, J. M. (2002). Physician utilization: the state of research about physicians' practice patterns. Med. Care 40, 1016–1035 doi: 10.1097/00005650-200211000-00004
Fisher, E. S., Wennberg, D. E., Stukel, T. A., Gottlieb, D. J., Lucas, F. L., and Pinder, E. L. (2003a). The implications of regional variations in medicare spending. Part 1: the content, quality, and accessibility of care. Ann. Intern. Med. 138, 273–287. doi: 10.7326/0003-4819-138-4-200302180-00006
Fisher, E. S., Wennberg, D. E., Stukel, T. A., Gottlieb, D. J., Lucas, F. L., and Pinder, E. L. (2003b). The implications of regional variations in Medicare spending. Part 2: health outcomes and satisfaction with care. Ann. Intern. Med. 138, 288–298. doi: 10.7326/0003-4819-138-4-200302180-00007
Fuster, V., Bhatt, D. L., Califf, R. M., Michelson, A. D., Sabatine, M. S., Angiolillo, D. J., et al. (2012). Guided antithrombotic therapy: current status and future research direction: report on a national heart, lung and blood institute working group. Circulation 126, 1645–1662. doi: 10.1161/CIRCULATIONAHA.112.105908
Giugliano, R. P., Ruff, C. T., Braunwald, E., Murphy, S. A., Wiviott, S. D., Halperin, J. L., et al. (2013). Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 369, 2093–2104. doi: 10.1056/NEJMoa1310907
González López-Valcárcel, B., Librero, J., García-Sempere, A., Peña, L. M., Bauer, S., Puig-Junoy, J., Peiró, S., et al. (2017). Effect of cost sharing on adherence to evidence-based medications in patients with acute coronary syndrome. Heart 103, 1082–1088. doi: 10.1136/heartjnl-2016-310610
González López-Valcárcel, B., Librero, J., Sanfélix-Gimeno, G., Peiró, S., and Group for Drug Utilization Research in the Spanish National Health System (IUM-SNS Group) (2011). Are prescribing doctors sensitive to the price that their patients have to pay in the Spanish National Health System? BMC Health Serv. Res. 11:333. doi: 10.1186/1472-6963-11-333
Granger, C. B., Alexander, J. H., McMurray, J. J., Lopes, R. D., Hylek, E. M., Hanna, M., et al. (2011). Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 365, 981–992. doi: 10.1056/NEJMoa1107039
January, C. T., Wann, L. S., Alpert, J. S., Calkins, H., Cigarroa, J. E., Cleveland, J. C. Jr., et al. (2014). AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the heart rhythm society. Circulation 130, 2071–2104. doi: 10.1161/CIR.0000000000000040
Jørgensen, H. S., Nakayama, H., Reith, J., Raaschou, H. O., and Olsen, T. S. (1996). Acute stroke with atrial fibrillation. The copenhagen stroke study. Stroke 27, 1765–1769. doi: 10.1161/01.STR.27.10.1765
Lancaster, T. R., Singer, D. E., Sheehan, M. A., Oertel, L. B., Maraventano, S. W., Hughes, R. A., et al. (1991). The impact of long-term warfarin therapy on quality of life. Evidence from a randomized trial. Boston area anticoagulation trial for atrial fibrillation investigators. Arch. Intern. Med. 151, 1944–1949. doi: 10.1001/archinte.1991.00400100032005
Lin, H. J., Wolf, P. A., Kelly-Hayes, M., Beiser, A. S., Kase, C. S., Benjamin, E. J., et al. (1996). Stroke severity in atrial fibrillation. The framingham study. Stroke 27, 1760–1764. doi: 10.1161/01.STR.27.10.1760
Merlo, J., Chaix, B., Ohlsson, H., Beckman, A., Johnell, K., Hjerpe, P., et al. (2006). A brief conceptual tutorial of multilevel analysis in social epidemiology: using measures of clustering in multilevel logistic regression to investigate contextual phenomena. J. Epidemiol. Community Health 60, 290–297. doi: 10.1136/jech.2004.029454
Merlo, J., Wagner, P., Ghith, N., and Leckie, G. (2016). An original stepwise multilevel logistic regression analysis of discriminatory accuracy: the case of neighbourhoods and health. PLoS ONE 11:e0153778. doi: 10.1371/journal.pone.0153778
National Research Council. (2013). Variation in Health Care Spending: Target Decision Making, Not Geography. (Washington, DC: The National Academies Press).
Olesen, J. B., Sørensen, R., Hansen, M. L., Lamberts, M., Weeke, P., Mikkelsen, A. P., et al. (2015). Non-vitamin K antagonist oral anticoagulation agents in anticoagulant naïve atrial fibrillation patients: Danish nationwide descriptive data 2011-2013. Europace 17, 187–193. doi: 10.1093/europace/euu225
Patel, M. R., Mahaffey, K. W., Garg, J., Pan, G., Singer, D. E., Hacke, W., et al. (2011). Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 365, 883–891. doi: 10.1056/NEJMoa1009638
Patel, P. A., Zhao, X., Fonarow, G. C., Lytle, B. L., Smith, E. E., Xian, Y., et al. (2015). Novel oral anticoagulant use among patients with atrial fibrillation hospitalized with ischemic stroke or transient ischemic attack. Circ. Cardiovasc. Qual. Outcomes 8, 383–392. doi: 10.1161/CIRCOUTCOMES.114.000907
Petersen, P., Boysen, G., Godtfredsen, J., Andersen, E. D., and Andersen, B. (1989). Placebo-controlled, randomised trial of warfarin and aspirin for prevention of thromboembolic complications in chronic atrial fibrillation. The copenhagen AFASAK study. Lancet 1, 175–179. doi: 10.1016/S0140-6736(89)91200-2
Potpara, T. S., and Lip, G. (2017). Postapproval observational studies of non–vitamin k antagonist oral anticoagulants in atrial fibrillation. JAMA 317, 1115–1116. doi: 10.1001/jama.2017.1152
Rodríguez-Bernal, C. L., Hurtado, I., García-Sempere, A., Peiró, S., and Sanfélix-Gimeno, G. (2017). Oral anticoagulants initiation in patients with atrial fibrillation: real-world data from a population-based cohort. Front. Pharmacol. 8:63. doi: 10.3389/fphar.2017.00063
The Boston Area Anticoagulation Trial for Atrial Fibrillation Investigators Singer, D. E., Hughes, R. A., Gress, D. R., Sheehan, M. A., Oertel, L. B., et al. (1990). The effect of low-dose warfarin on the risk of stroke in patients with nonrheumatic atrial fibrillation. N. Engl. J. Med. 323, 1505–1511. doi: 10.1056/NEJM199011293232201
Wennberg, J. E., Fisher, E. S., and Skinner, J. S. (2002). Geography and the debate over medicare reform. Health Aff. 21, W96–W114. doi: 10.1377/hlthaff.w2.96
Zhang, Y., Baicker, K., and Newhouse, J. P. (2010a). Geographic variation in medicare drug spending. N. Engl. J. Med. 363, 405–409. doi: 10.1056/NEJMp1004872
Zhang, Y., Baicker, K., and Newhouse, J. P. (2010b). Geographic variation in the quality of prescribing. N. Engl. J. Med. 363, 1985–1988. doi: 10.1056/NEJMp1010220
Keywords: analysis of variance, anticoagulants, atrial fibrillation, drug utilization, multilevel analysis
Citation: García-Sempere A, Bejarano-Quisoboni D, Librero J, Rodríguez-Bernal CL, Peiró S and Sanfélix-Gimeno G (2017) A Multilevel Analysis of Real-World Variations in Oral Anticoagulation Initiation for Atrial Fibrillation in Valencia, a European Region. Front. Pharmacol. 8:576. doi: 10.3389/fphar.2017.00576
Received: 28 June 2017; Accepted: 10 August 2017;
Published: 24 August 2017.
Edited by:
Jean-Paul Deslypere, Proclin Therapeutic Research Pte Ltd., SingaporeReviewed by:
Robert L. Lins, Retired, Antwerpen, BelgiumSandor Kerpel-Fronius, Semmelweis University, Hungary
Copyright © 2017 García-Sempere, Bejarano-Quisoboni, Librero, Rodríguez-Bernal, Peiró and Sanfélix-Gimeno. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aníbal García-Sempere, garcia_ani@gva.es