
- Department of Sport Science, Institute of Sport Science and Institute of Psychology, University of Regensburg, Regensburg, Germany
The present study investigated the influence of cognitive, motor, and Karate (accordingly the guidelines of the German-Karate-Federation, DKV) training on the cognitive functioning and mental state of older people between 67 and 93 years of age. The three training groups each consisted of 12 elderly participants; the waiting control group included 9 participants. Before the training, participants were evaluated with cognitive measurements (cognitive speed: number-connection test, number–symbol test; memory performance: digit-span test, blocking-tapping test, figure test) and a measurement of emotional well-being. After this pre-testing they participated the specific training in on average sixteen 1-h training sessions. The cognitive training exercised inductive thinking ability, the motor training worked on easy stretching and mobilization techniques, and the Karate training taught tasks of self-defense, partner training, and Katas. After completion of the training sessions, all tests were applied again. The results show no significant difference in cognitive improvement dependent on group between the three training conditions. However a significant improvement was found in the emotional mental state measurement for the Karate group compared to the waiting control group. This result suggests that the integrated involvement in Karate leads to a feeling of self-worth and that, even in elderly people, integration of new sports helps to improve quality of life.
Introduction
Increasing life expectancy and demographic changes are causing the absolute number of elderly people to increase as well as their proportion of the total population. Because of this, maintaining cognitive function and emotional well-being in the last decades of life becomes an important topic for our society. It is well known that some cognitive functions decline in older age, mainly fluid intelligence components such as perceptual speed and working memory capacity; other cognitive functions stay stable over a long period in life, such as verbal fluency and knowledge representations (Smith and Baltes, 2010). Today it is well accepted that there are domain-general as well as function specific-mechanisms which explain the cognitive and sensory decline that occurs in old age (Lindenberger and Ghisletta, 2009).
Much research has been done to investigate how cognitive functions remain stable over long periods of time. Correlation studies suggest that older people who are physically, emotionally, and socially engaged are at less risk to suffer from dementia than older adults who do not engage in such activities (Karp et al., 2006). Larson et al. (2006) conducted an investigation with 1,750 older adults, performing tests every 2 years over a period of 6 years. They showed that people who are physically active at least three times a week had a minor probability for suffering from dementia. But if other factors were included in the analysis, for example smoking and education level, this advantage was reduced.
In addition, experimental studies with younger participants have been performed which demonstrate that cognitive training as well as physical exercise is associated with improved cognitive functioning (Colcombe and Kramer, 2003) and emotional well-being (Lee and Russel, 2003). In a study by Strawbridge et al. (2002) it was shown that physical activity in older people (mean age 63 years) reduces the risk of depression. In their study they constructed a physical activity scale, which was based on the frequency of four activities: physical exercise, sports participation, long walks, and swimming.
Furthermore, it was shown that an active and socially integrated lifestyle in late life could even protect against dementia (Fratiglioni et al., 2004). This suggests that emotional well-being and cognitive functioning may be related to each other. This connection is further supported by Royall et al. (2012), whose results show that depressive symptoms may predict longitudinal change in some forms of executive functioning but not in memory tasks for seniors older than 70 years.
The Influence of Cognitive Training on Cognitive Performance and Emotional Well-Being in the Elderly
Baltes and Lindenberger (1988) summarized the effect of cognitive training on cognitive performance regarding fluid intelligence measurements done in former studies. Twenty-five years ago, Schaie and Willis (1986) had already demonstrated that existing cognitive performance impairments in inductive, visual, and spatial thinking could be improved with cognitive training. Yang and Krampe (2009) showed that learning effects of elderly people over 80 years old remained stable for 8 months by just repeating the learning tests. In Tranter’s and Koutsall’s (2008) study a group of older people who were cognitively active (solving cognitive problems and performing creative tasks) were better in fluid intelligence measurements after 8–12 weeks of training than a group of older people who did not do any specific cognitive task. Stine-Morrow et al. (2008) showed that a group of people who participated in 20 problem solving training sessions exhibited an increase in fluid intelligence components compared to a group which did not receive any training. In the Active Study, 705 elderly people aged between 65 and 94 years old took part in 10 training sessions of inductive thinking (EG 1) or cognitive speed (EG 2). It was found that 87% of the people in EG 1 and 74% of the people in the EG 2 improved their fluid intelligence components (Willis et al., 2006).
Concerning emotional well-being, it is proposed that well-being remains largely stable across adulthood and old age (Diener et al., 2006) until around 3–5 years before death. During this time, mechanisms which are related to mortality cause changes in the emotional well-being of the elderly (Gerstorf et al., 2010). Brum et al. (2009) investigated the effect of cognitive training on cognitive performance and emotional well-being in 16 older adults diagnosed with mild dementia. People with mild dementia were defined as those adults whose activities of daily living were preserved but were beginning to demonstrate a decline in cognitive performance. Each training session lasted 2 h and was held twice a week over a period of 1 month. The training included tasks of orientation in time and space (paper–pencil tests), remembering names, visual and auditory attention exercises, memory exercises, and transfer tasks. A waiting control group did not take part in any form of training. Before and after the training, different cognitive tests (direct assessment of functional scale revised, clock drawing test) and a measurement of depression were conducted. The results show an improvement in attention, in daily activity tasks, and in the depression scale.
While no studies were conducted which focused explicitly on the influence of cognitive training on mental state, Yaffe et al. (1999) demonstrated an influence of cognitive training on emotional well-being. In this study, depressive symptoms in older women without dementia were found to be associated with both poor cognitive performance and cognitive decline (Yaffe et al., 1999). All of these studies demonstrate that cognitive training can improve intelligence, especially fluid intelligence, in older people. Furthermore, an association between depressive symptoms and cognitive decline is suggested.
The Influence of Physical Activity Training on Cognitive Performance and Emotional Well-Being in the Elderly
A considerable number of studies have provided evidence for the beneficial effects of physical training in older adults for physiological processes (e.g., Karavirta et al., 2011) as well as for cognitive performance (Colcombe and Kramer, 2003). For middle-aged adults (40–56 years) both cardiovascular and coordination training improved episodic memory performance but not other cognitive performances compared to a control group (Hötting et al., 2011). Colcombe et al. (2006) provided further evidence that older participants show a greater activation in certain brain regions, which are associated with effective control of attention, after a cardiovascular intervention. So far, more research has been done on the effect of endurance training than on the effect of strength training (compare Völcker-Rehage et al., 2011). Because of this, Völcker-Rehage et al. (2011) investigated the effect of cardiovascular and coordination training on cognitive performance (perceptual speed and executive functions) of elderly people (62–79 years old) over a longitudinal period of 3 months, three times a week. Using fMRI, brain activity was recorded before and after the training. Both experimental groups improved in executive functioning and mental speed, demonstrated by reaction time and accuracy measurements. One of the neurophysiological results showed a decreased activation in the prefrontal cortex while solving an executive task for both experimental groups compared to the control group. Furthermore, both training tasks induced different kind of activation: cardiovascular training was associated with the activation of sensorimotor regions in the brain, whereas after the coordination training visual–spatial regions were activated. This indicates both cardiovascular and coordination training is of particular importance for improving the cognitive functions of older people. This is in line with a study of Boyke et al. (2008) which showed that healthy senior citizens who learned three-ball cascade juggling demonstrated gray-matter changes in the brain.
There are only a few studies investigating the effects of physical activity on emotional well-being or on the prevention of depression in older people. In a study with young adults, Hassmann et al. (2000) showed that physically fit individuals experienced fewer symptoms of depression and anxiety. Netz et al. (2005) demonstrated that the effect of physical activity on emotional well-being depends on age. The largest effect was seen in the late middle-age adults, whereas very old people did not show an improvement. The review of Forsman et al. (2011) suggests that social activities but not physical activity alone were effective in reducing depressive symptoms.
These studies show that physical activity can have an effect on cognitive performance. However it is still unclear which physical activity is linked to each aspect of cognition. While results suggest that physical activity has a high impact on emotional well-being in middle-aged adults, studies with older people are rare. Moreover, in many studies physical activity was performed in groups, therefore social interaction might play a crucial role in the demonstrated emotional improvement.
Karate Training as a Combination of Cognitive, Physical, and Emotional Activity
Karate-Do is a form of martial arts focusing on self-protection and health improvement. It might be interpreted as sport and therapy at once (Burke et al., 2007). In contrast to Tai-Chi (Hong et al., 2000; Li et al., 2001), the effectiveness of Karate as therapy is not well investigated. One goal of Karate is to improve self-control and self-awareness. Richmann and Rehberg (1986) showed that self-esteem was higher for those people who trained in Karate for a longer time. The training of Karate consists of three parts: “Kihon,” basic exercise, which is mainly characterized by the attention to and repetition of specific movements or a combination of movements; “Kumite,” exercises with the partner, the main goal is to train “together with” and not “against” the partner; and “Katas,” where sequences of different moves are combined (Pflüger, 2003). Accordingly the guidelines of the German-Karate-Federation (DKV), it is important not to injure the trainings-partner. In contrast to boxing, injuries of the antagonist will not lead to victory but to disqualification. Participants have to learn the “katas,” a series of prescribed movements. Katas are formal exercises, sometimes thought of as representing a battle against an unspecified number of imaginary opponents. To learn and to retain these movements in the memory is a very demanding cognitive task. This suggests that the learning of the Katas includes a cognitive as well as a physical component. Karate also includes a philosophical or spiritual component. In the beginning and in the end of the training a short meditation is done to clear the mind, for only with a clear mind and conscience can the practitioner understand the knowledge which he receives. This meditation increases calmness and improves psychological balance. Karate is meant to improve personal development. Respecting others as well as endeavor is considered of prime importance. You may be slow in your training progress, but you are supposed to always try to improve your techniques. In one pilot study on the effects of karate training, 15 men (50 years old) showed an improvement in depression scores, physical health, and reaction time. The improvement in reaction time was found for non-dominant hand and postural control tasks, but not for most of the finger-tapping tasks. Since this was a pilot study a control group was not included (Chateau-Degat et al., 2010).
Main Goal of this Paper
Former studies have shown that under some circumstances cognitive training and physical training can improve cognitive performance. The literature is not that clear concerning the effects of cognitive and physical training on emotional well-being.
The main goal of this paper is to investigate the influence of Karate training on cognitive performance and emotional well-being. It is hypothesized that the influence of Karate on the cognitive and emotional measurement is higher than either cognitive or physical training alone, because Karate includes both cognitive and physical components. To determine the effects of Karate we included two additional experimental groups which only received cognitive or physical training. Furthermore, a control group was included which did not receive any training.
Materials and Methods
Study Design
An experimental pilot study with four different groups was conducted to evaluate the behavioral effects of four different kinds of training:
(a) motor training, (b) cognitive training, (c) DKV-Karate training, and (d) a control group which did not receive any experimental training. The study was conducted in accordance to the guidelines regarding human experimentation in the declaration of Helsinki. All participants gave their written informed consent.
Participants
Sixty older adults agreed to participate in this study. Six people had to be excluded because four of them suffered from Parkinson’s disease and two from dementia. In addition, four participants dropped out because they had to stay in the hospital, four participants quit for personal reasons, and one person died. This resulted in a total of 45 older adults participating throughout the training phase. The participants differed significantly by age [F(3,41) = 10.19, p < 0.05]. A post hoc Bonferroni correction shows that the participants of the motor training and control group were significantly older than the participants of the cognitive training and Karate group. Participants lived in two different nursing homes or in their own houses. All participants were recruited through one physician. The number of couples in each group was: karate training (1), motor training (1), cognitive training (4), and control group (0). The number of participants and mean age are given in Table 1.

Table 1. Number of participants, gender distribution, and mean age for the four different training groups.
All participants received a medical check-up and those with chronic illnesses were excluded before the experiment began. All remaining participants were informed about possible risks and signed a written informed consent.
Materials
The following tests were used to measure the cognitive performance as well as the emotional mental state.
Test procedures
Cognitive performance. Cognitive Performance was measured regarding (a) cognitive speed and (b) memory performance.
Cognitive speed was measured by the number-connection Test (ZVT) and the Number–Symbol Test (ZS) from the NAI (Nürnberger-Alters Inventar; Oswald and Fleischmann, 1997).
The Number-Connection Test (ZVT) consists of five sheets of paper, two exercise sheets and three test sheets. On each sheet, the numbers 1–30 are printed in a scrambled order. The participant has to connect the numbers with a pen as fast as possible. The mean time of both test trials is calculated. The test lasts around 7–10 min. The test–retest reliability is r = 0.95.
The Number–Symbol Test (ZS) consists of one test sheet with 75 boxes, which are ordered in three rows. In each of these 75 boxes the numbers from 1 to 9 are presented in a scrambled order. Beneath each of the 75 boxes, an empty box is presented. The task of the participant is to draw a simple specific symbol which corresponds to the numbers in each of the empty boxes. The relationship between the symbols and the numbers are presented at the top of the paper. The time for this task is 90 s. The number of correctly assigned symbols is counted. The test lasts around 5 min. Test–retest reliability is given between r = 0.89 and r = 0.97 (Oswald and Fleischmann, 1997).
Memory Performance. Memory performance was measured by the digit-span test, the figure test (Oswald and Fleischmann, 1997), and the block-tapping test (Schelling, 1997).
The Digit-span Test measures working memory capacities. Participants have to recall digits which are presented to them in ascending order, up to nine digits forward and eight digits backward. In the first time they have to recall the numbers forward, in the second test backward. If participants are not able to recall the digits in two successive sessions the test is stopped. The mean number of the longest span of numbers which is reproduced backward and forward is registered. The test lasts around 5 min. The test–retest reliability is r = 0.64.
The Figure Test is comprised of 12 single tasks with different figures. The figures are presented on a black sheet of paper in descending difficulty (one, two, or three single figures) for 10 s at a time. Immediately after the presentation, the participant has to recognize the presented figure out of four figures. No feedback is given. The test lasts around 5 min. Test–retest reliability is r = 0.60.
The Block-tapping Test (Schelling, 1997) measures the visual–spatial sketchpad according to Baddeley’s working memory model. On a black wooden board, blocks (4.5 cm × 4.5 cm) are marked in a scrambled order. All wooden blocks are numbered on the side which is visible to the experimenter but not to the participant. The board is set between the experimenter and the participant. The experimenter taps a series of blocks and the participant has to repeat this sequence immediately. The numbers of blocks within a sequence determines the level of difficulty. The test is aborted when a participant cannot recall three attempts of a sequence. The longest length of the block sequences that can be repeated two times is the maximum score of each participant. The test lasts around 10–15 min. The reliability varies between r = 0.81 and r = 0.089.
Emotional mental state. Emotional mental state and depressive pathology was measured with the Center of Epidemiological Studies Depressions Scale [CES-D-scala, long version (German version: ADS, Hautzinger and Bailer, 1993)] which measures the different stages of depressive symptoms. Through questioning the depressive symptoms of uncertainty, fatigue, hopelessness, demotion of oneself, dejection, loneliness, sadness, listlessness, fear, etc., are analyzed. The questionnaire lasts around 10 min. Split-half reliability is r = 0.81.
Training sessions
Physical exercise training. The training included simple exercises for strength, mobilization, stretching, and relaxation. Everyday objects such as towels, chairs, etc., were used as exercise equipment. Tasks differed from simple tasks, such as moving the legs one at time to more difficult tasks, such as moving legs and arms in a specific rhythm. The intensity of the movements was regulated by each participant. Each session was preceded by warming-up and ended with cooling-down.
Cognitive training. The training of cognitive performance was taught according to Klauer’s book “Sport for thinking for the elderly” (2008). The main goal of this program is to improve inductive thinking and to train fluid intelligence and memory performance. The program consists of 121 tasks, 104 inductive thinking tasks (13 generalization, 15 discrimination, 17 cross-classification, 32 relation, 14 relation differentiation, and 13 system-building tasks) and 17 deductive thinking and concentration tasks. Tasks appear in a specific order to allow the participants to become familiarized with the task. The test was administered in small groups and the participants had to solve the problem by themselves. Each training session lasted around 60 min.
Training of DKV-Karate. Shotokan-Karate (Karate-Do) Training was performed accordingly the guidelines of the German-Karate-Federation (DKV). Karate-Do involves powerful movements of the legs or arms (or both of them at the same time). Long sequences of arm and leg movements were taught. Every training session lasted around 60 min and was conducted by a professional karate teacher.
Procedure
In each of the 4 groups 20 training sessions were provided in a period of 3–6 months. It was not possible to clearly randomize participants to one of four groups because inhabitants of the nursing homes wanted to stay together as well as married couples.
Prior to training the tests mentioned above were applied in single sessions. Standardized instructions were given. For each group, post-testing was done immediately after the last training session. Testing of all groups was conducted in rooms of one of the nursing homes.
Statistical Analysis
A univariate analysis of variance was done with the “number of training sessions” as the dependent variable and “training group” (motor training, cognitive training, and Karate) as the independent variable.
Moreover, for each of the cognitive measurements and for the emotional mental state a co-variance of analysis was conducted with “time of testing” (pre- and post-test) and “training group” as independent variables. Because the four groups differ by age, age was considered as a co-variate.
Results
Number of Training Lessons
The univariate analysis of variance showed a significant influence of the factor “training group,” F(1,33) = 3.45, p < 0.055, η2 = 0.17). Bonferroni corrections shows that participants of the cognitive training group (M = 17.75; SE = 0.85) had more training sessions than the participants of the physical exercise group (M = 14.67, SE = 0.81). The number of training sessions of the Karate group (M = 15.67, SE = 0.85) did not differ significantly from the other two groups.
Cognitive Speed Measurements
Concerning cognitive speed measurements, all training groups performed better than controls (see Table 2).

Table 2. Main effect in the cognitive measurements (cognitive speed and memory performance).
Number-connection test
The control group (M = 45.51 s; SE = 3.8) needed more time to solve the test compared to the physical exercise group (M = 29.72 s; SE = 3.45), the cognitive training group (M = 23.83 s; SE = 3.28), and the Karate group (M = 29.31 s; SE = 3.41).
Number–symbol test
The control group (M = 26.34; SE = 2.95) answered less items compared to the cognitive training group (M = 41.11; SE = 2.41) and the Karate group (M = 35.82; SE = 2.51). Furthermore, the participants of the cognitive training group answered more items than the participants of the physical exercise group (M = 30.71; SE = 2.57).
Memory Performance
None of the factors in the different memory tests showed an effect.
Measurements of Emotional Mental State
First of all, there was no statistical significant difference in the baseline depression measurement, F(3, 40) = 2.48, n.s. The Co-variance analysis did not show a significant main effect of “time of testing” (before or after training), F(1,37) = 0.84, n.s., or of “training group,” F(3,37) = 0.81, n.s., but did show a significant interaction between both factors, F(3,37) = 4.12, p < 0.05, η2 = 0.25. Figure 1 shows that the ADS-score did not differ from pre- to post-test for the physical exercise and cognitive group but increases for the control group and decreases for the Karate group.
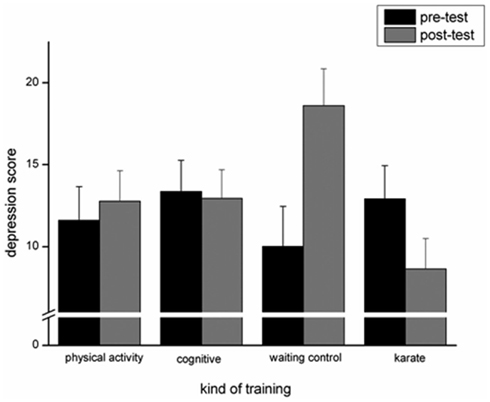
Figure 1. Depression score in the pre- and post-test dependent for each of the trainings groups.
Discussion
In this study with elderly people the effect of cognitive training, physical exercise training, and Karate training was investigated with regard to cognitive performance and emotional well-being. While the results did not show a significant improvement in the cognitive performance measurements, an improvement was shown in the emotional well-being measurement for those in the karate group.
Karate Improves Emotional Well-Being
In this study we found an improvement in emotional well-being only in the Karate group. This reduction of the depression score in the Karate group was also found in the pilot study of Chateau-Degat et al. (2010); however, this study is limited by the fact that no control group was included and that the participants consisted of only one gender and age group (50-year-old men). As far as we know, this is the first study under controlled experimental conditions which showed an improvement in emotional well-being due to Karate in men and women with a mean age of more than 70 years. Because Karate training combines cognitive and physical training with the goal to actively improve performance, the older people may have been more engaged in this kind of activity than in the physical or cognitive training alone. This increased engagement seems to have improved the emotional well-being of the participants and is in line with studies which found reduced depression rates for physically active older people (i.e., Strawbridge et al., 2002). At this point we do not know exactly why the depression score was reduced in the Karate group. One reason might be that the completion of the difficult cognitive and physical activity tasks enhanced the self-esteem of the older people. A second reason might be that the Karate lessons have inspired some spiritual insight, which led to a reduction of depression symptoms. Furthermore, the beneficial effect of Karate training might be caused by the play fight situation. Because Katas can be exercises, which sometimes thought of as representing a battle against an imaginary opponent, imaginary and maybe creative thinking might be improved. Our study presented here showed that the influence of Karate might not have been due to the social support of the trainer, because both the trainer of the cognitive training group as well as the trainer of the physical activity group exhibited the same dedication. In addition, the number of training sessions did not differ significantly between the Karate group and the cognitive and physical exercise group. Furthermore, there were no more couples in the Karate group than in the other groups. This excludes the possibility that there was more engagement and receptivity in the Karate group than in the other two groups due to the interaction of couples. In future studies, the influence of Karate training might also be contrasted with a group of older people who receive only a Meditation or Attentiveness intervention to investigate the importance of the emotional training component in Karate.
This study also showed that the depression score of the control group increased whereas the scores remained the same in the cognitive and exercise groups and decreased in the Karate group. Due to this trend in depression scores, any activity which is performed in a group seems to have a benefit on the emotional parameters of older people, an assumption which is in line with the findings of the importance of social activity (Forsman et al., 2011).
No Significant Improvement on Cognitive Performance Measurements
This study shows no significant improvement in cognitive abilities after cognitive, physical, or Karate training, despite finding positive trends in cognitive speed for the cognitive training group (number–symbol test and number-connection test), the physical exercise group (number-connection test), and in memory performance for the karate group (digit-span test and form-identification test). At the first glance this is astonishing that there are no significant results when compared with the literature, which has found an improvement after cognitive (Stine-Morrow et al., 2008) as well as physical training (Colcombe and Kramer, 2003). This difference might be due to different cognitive measurements, different intervention programs, different duration of the training, and different ages of the elderly people. The differences in these factors make it difficult to compare the results across studies. In this study the mean ages of the older participants varied between 73 and 83 years, which is older compared to the mean ages in other studies (see for example Dorbath et al., 2011; Karavirta et al., 2011). Furthermore, in this study, inductive tasks were used in the cognitive training to improve fluid intelligence measurements; this might differ from other cognitive training programs. The physical exercise program did not have any endurance component and did not include walking and jogging but was concentrated on more coordinative and strength training exercises, which were adapted to the age of the older people in this training group.
Limitations
One limitation in this study might be the fact that after the exclusion of some older people due to illness only 12 older people completed each of the trainings. Also, the duration of the training could be increased in further studies. Furthermore, the cognitive as well as the physical training might be better adapted to the cognitive measurements. We have chosen to model the inductive training on the training program of Klauer (2008) because: (1) it is specifically created for the elderly and (2) it is supposed to train fluid intelligence which we can measure with cognitive speed and working memory. A specific working memory training as well as training of cognitive speed might be more applicable to the measurements applied in this study. The physical training was conceptualized in relation to the very old age of the participants. In further studies endurance might be an important component to investigate as well as strength training. Both have to be adapted to the individual’s physical fitness. The improvement of the training as mentioned above in further studies with adults of high age might lead to cognitive improvement as described by others (see for example Völcker-Rehage et al., 2011). Furthermore, the group compositions as well as the basic test rate have to be regarded carefully in the next study on this topic.
Conclusion
Even though this study did not find a significant improvement in cognitive performance or emotional well-being after cognitive or physical training, a significant improvement in emotional well-being was found in the participants who received Karate training. It shows that “unusual” sports can enhance the quality of life and that the “impossible” might be “possible,” even in old age.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Baltes, P. B., and Lindenberger, U. (1988). On the range of cognitive plasticity in old age as a function of experience: 15 years of intervention research. Behav. Ther. 19, 283–300.
Boyke, J., Driemeyer, J., Gaser, C., Büchel, C., and May, A. (2008). Training-induced brain structure changes in the elderly. J. Neurosci. 28, 7031–7035.
Brum, P. S., Forlenza, O. V., and Yassuda, M. S. (2009). Cognitive training in older adults with mild cognitive impairment. Neuropsychologia 3, 124–131.
Burke, D. T., Al-Adawi, S., Lee, Y. T., and Audette, J. (2007). Martial arts as sport and therapy. J. Sports Med. Phys. Fitness 47, 96–102.
Chateau-Degat, M.-L., Papouin, G., Saint-Val, P., and Lopez, A. (2010). Effect of adapted karate training on quality of life and body balance in 50-year-old men. J. Sports Med. 1, 143–150.
Colcombe, S. J., Erickson, K. I., Scalf, P. E., Kim, J. S., Prakash, R., McAuley, E., Elavsky, S., Marquez, D. X., Hu, L., and Kramer, A. F. (2006). Aerobic exercise training increases brain volume in aging humans. J. Gerontol. A 61, 1166–1170.
Colcombe, S. J., and Kramer, A. F. (2003). Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol. Sci. 14, 125–130.
Diener, E., Lucas, R. E., and Scollon, C. N. (2006). Beyond the hedonic treadmill: revising the adaptation theory of well-being. Am. Psychol. 61, 305–314.
Dorbath, L., Hasselhorn, M., and Titz, C. (2011). Aging and executive functioning: a training study on focus-switching. Front. Psychol. 2:257. doi:10.3389/fpsyg.2011.00257
Forsman, A. K., Schierenbeck, I., and Wahlbeck, K. (2011). Psychosocial interventions of the prevention of depression in older adults: systematic review and meta-analysis. J. Aging Health 23, 387–416.
Fratiglioni, L., Paillard-Borg, S., and Winblad, B. (2004). An active and socially integrated lifestyle in late life might protect against dementia. Lancet Neurol. 3, 343–353.
Gerstorf, D., Ram, N., Röcke, C., Lindenberger, U., and Smith, J. (2010). Decline in life satisfaction in older age: longitudinal evidence for links to distance-to-death. Psychol. Aging 23, 154–168.
Hassmann, P., Koivula, N., and Uutela, A. (2000). Physical exercise and psychological well-being: a population study in Finland. Prev. Med. 30, 17–25.
Hautzinger, M., and Bailer, M. (1993). Allgemeine Depressions Skala, German Version of G-ADS. Göttingen: Beltz Test Verlag.
Hong, Y., Li, J. X., and Robinson, P. (2000). Balance control, flexibility and cardiorespiratory fitness among older Tai Chi practitioners. Br. J. Sports Med. 34, 29–34.
Hötting, K., Reich, B., Holzschneider, K., Kauschke, K., Schmidt, T., Reer, R., Braumann, K.-M., and Röder, B. (2011). Differential cognitive effects of cycling versus stretching/coordination training in middle-aged adults. J. Hist. Philos. [advance online].
Karavirta, L., Häkkinnen, K., Kauhanen, A., Arija-Blazquez, A., Sillanpää, E., Rinkinen, N., and Häkkinen, A. (2011). Individual responses to combined endurance and strength training in older adults. Med. Sci. Sports Exerc. 43, 484–490.
Karp, A., Paillard-Borg, S., Wang, H.-X., Silverstein, M., Winblad, B., and Fratiglioni, L. (2006). Mental, physical and social components in leisure activities equally contribute to decrease dementia risk. Dement. Geriatr. Cogn. Disord. 21, 65–73.
Klauer, K. J. (2008). Denksport für Ältere – Geistig fit bleiben (2. Auflage) [Thinking Sports for the Elderly – Staying mentally fit]. Bern: Hans Huber.
Larson, E. B., Wang, L., Bowen, J. D., McCormick, W. C., Teri, L., Crane, P., and Kukull, W. (2006). Exercise is associated with reduced risk for incident dementia among persons 65 years of age and older. Scand. J. Med. Sci. Sports 16, 294–295.
Lee, C., and Russel, A. (2003). Effects of physical activity on emotional well-being among older Australian women: cross sectional and longitudinal analysis. J. Psychosom. Res. 54, 155–160.
Li, J. X., Hong, Y., and Chan, K. (2001). Tai chi: physiological characteristics and beneficial effects on health. Br. J. Sports Med. 35, 148–156.
Lindenberger, U., and Ghisletta, P. (2009). Cognitive and sensory declined in old age: gauging the evidence for a common cause. Psychol. Aging 1, 1–16.
Netz, Y., Wu, M. J., Becker, B. J., and Tenenbaum, G. (2005). Physical activity and psychological well-being in advanced age: a meta-analysis of intervention studies. Psychol. Aging 20, 272–284.
Oswald, W. D., and Fleischmann, U. M. (1997). Nürnberger-Alters-Inventar (NAI). Testinventar & NAI-Testmanual und Textband (4. Auflage). Göttingen: Hogrefe.
Richmann, C. L., and Rehberg, L. (1986). The development of self-esteem through the martial arts. Int. J. Sport Psychol. 17, 234–239.
Royall, D. R., Palmer, R., Chiodo, L. K., and Polk, M. J. (2012). Depressive symptoms predict longitudinal change in executive control but not memory. Int. J. Geriatr. Psychiatry 27, 89–96.
Schaie, K. W., and Willis, S. L. (1986). Can adult intellectual decline be reversed? Dev. Psychol. 22, 223–232.
Smith, J., and Baltes, P. B. (2010). “Altern aus psychologischer Perspektive: trends und Profile im hohen Alter” [Getting older from a psychology perspective: trends and profiles in the elderly], in Die Berliner Altersstudie (3. Auflage), eds U. Lindenberger, J. Smith, K. U. Mayer, and P. B. Baltes (Berlin: Akademie Verlag), 245–274.
Stine-Morrow, E. A. L., Parisi, J. M., Morrow, D. G., and Park, D. C. (2008). The effects of an engaged lifestyle on cognitive vitality: a field experiment. Psychol. Aging 23, 778–786.
Strawbridge, W. J., Deleger, S., Roberts, R. E., and Kaplan, G. (2002). Physical activity reduces the risk of subsequent depression for older adults. Am. J. Epidemiol. 156, 328–334.
Tranter, L. J., and Koutstall, W. (2008). Age and flexibility thinking: an experimental demonstration of the beneficial effects of increased cognitively stimulating activity on fluid intelligence in healthy older adults. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 15, 184–207.
Völcker-Rehage, C., Godde, B., and Staudinger, U. (2011). Cardiovascular and coordination training differentially improve cognitive performance and neural processing in older adults. Front. Hum. Neurosci. 5:26. doi:10.3389/fnhum.2011.00026
Willis, S. L., Tennstedt, S. L., Marsiske, M., Ball, K., Elias, J., Koepke, K. M., Moriis, J. N., Rebok, G. W., Unverzagt, F., and Stoddard, A. M. (2006). Long term effects of cognitive training on everyday functional outcomes in older adults. JAMA 296, 2805–2814.
Yaffe, K., Blackwell, T., Gore, R., Sands, L., Reus, V., and Browner, W. S. (1999). Depressive symptoms and cognitive decline in nondemented elderly women. Arch. Gen. Psychiatry 56, 425–430.
Keywords: elderly, physical exercise, cognitive improvement, emotional well-being
Citation: Jansen P and Dahmen-Zimmer K (2012) Effects of cognitive, motor, and karate training on cognitive functioning and emotional well-being of elderly people. Front. Psychology 3:40. doi: 10.3389/fpsyg.2012.00040
Received: 06 December 2011;
Accepted: 05 February 2012;
Published online: 20 February 2012.
Edited by:
Mark R. Wilson, University of Exeter, UKReviewed by:
Bettina Edna Blaesing, Bielefeld University, GermanyKevin Shockley, University of Cincinnati, USA
Copyright: © 2012 Jansen and Dahmen-Zimmer. This is an open-access article distributed under the terms of the Creative Commons Attribution Non Commercial License, which permits non-commercial use, distribution, and reproduction in other forums, provided the original authors and source are credited.
*Correspondence: Petra Jansen, Department of Sport Science, Institute of Sport Science, University of Regensburg, University Street 31, 93053 Regensburg, Germany. e-mail: petra.jansen@psk.uni-regensburg.de