 Javier Fenollar-Cortés
Javier Fenollar-Cortés Luis J. Fuentes
Luis J. Fuentes- 1Departamento de Psicología Evolutiva y de la Educación, Facultad de Psicología, Universidad de Murcia, Murcia, Spain
- 2Departamento de Psicología Básica y Metodología, Universidad de Murcia, Murcia, Spain
Introduction: Although the critical feature of attention-deficit/hyperactivity disorder (ADHD) is a persistent pattern of inattention and/or hyperactivity/impulsivity behavior, the disorder is clinically heterogeneous, and concomitant difficulties are common. Children with ADHD are at increased risk for experiencing lifelong impairments in multiple domains of daily functioning. In the present study we aimed to build a brief ADHD impairment-related tool -ADHD concomitant difficulties scale (ADHD-CDS)- to assess the presence of some of the most important comorbidities that usually appear associated with ADHD such as emotional/motivational management, fine motor coordination, problem-solving/management of time, disruptive behavior, sleep habits, academic achievement and quality of life. The two main objectives of the study were (i) to discriminate those profiles with several and important ADHD functional difficulties and (ii) to create a brief clinical tool that fosters a comprehensive evaluation process and can be easily used by clinicians.
Methods: The total sample included 399 parents of children with ADHD aged 6–18 years (M = 11.65; SD = 3.1; 280 males) and 297 parents of children without a diagnosis of ADHD (M = 10.91; SD = 3.2; 149 male). The scale construction followed an item improved sequential process.
Results: Factor analysis showed a 13-item single factor model with good fit indices. Higher scores on inattention predicted higher scores on ADHD-CDS for both the clinical sample (β = 0.50; p < 0.001) and the whole sample (β = 0.85; p < 0.001). The ROC curve for the ADHD-CDS (against the ADHD diagnostic status) gave an area under the curve (AUC) of.979 (95%, CI = [0.969, 0.990]).
Discussion: The ADHD-CDS has shown preliminary adequate psychometric properties, with high convergent validity and good sensitivity for different ADHD profiles, which makes it a potentially appropriate and brief instrument that may be easily used by clinicians, researchers, and health professionals in dealing with ADHD.
Introduction
It is amply accepted that Attention-Deficit/Hyperactivity Disorder (hereafter ADHD) impacts negatively on social, academic, and occupational functioning (American Psychiatric Association, 2013). Therefore, early detection and treatment of the disease is of crucial interest in the clinical and educational domains (Sonuga-Barke et al., 2011). Although the critical feature of ADHD is a persistent pattern of inattention and/or hyperactivity/impulsivity behavior, the disorder is rather heterogeneous at multiple levels (Wåhlstedt et al., 2009), and concomitant difficulties are the rule rather than the exception. The relationship between ADHD clinical profile and some functional impairment could be of especial interest not only to ADHD diagnosis/assessment but also to clinical intervention. Children with ADHD are at increased risk of experiencing serious, lifelong impairments in multiple domains of daily functioning. They include cognitive, language, adaptive functioning, motor development, emotion, school performance, task performance, and medical/health risks (Barkley, 2006). In the following sections we briefly comment on the main comorbidities exhibited by children with an ADHD diagnosis.
Emotional/Motivational Management
Several studies have highlighted some alterations in emotional processing (Anastopoulos et al., 2011; Classi et al., 2012), as well as higher sensitivity to reward and motivation impairments as core neurocognitive deficits associated to ADHD (e.g., Fosco et al., 2015; van Hulst et al., 2015). Importantly, both emotional and motivational difficulties also persist in adulthood (Retz et al., 2012; Jarrett, 2016). Accordingly, ADHD has been associated with risks of undergoing depression, negative self-concept and low self-esteem, persisting until adulthood (Edbom et al., 2006).
Fine Motor Coordination
Research has also suggested primary deficits in motor coordination associated to ADHD (Goulardins et al., 2013). It has mainly been observed in tasks that require rather complex motor skills (Scharoun et al., 2013), affecting up to 30–50% of ADHD cases (Fliers et al., 2008). Motor difficulties have also been related to poor quality and quantity of handwriting in ADHD (Rosenblum et al., 2008; Brossard-Racine et al., 2011; Shen et al., 2012). Although these impairments have a negative impact on academic achievement (Fliers et al., 2008), researchers have paid little attention to this comorbid problem, and consequently it has usually been excluded from the ADHD assessment (Fliers et al., 2010). In fact, motor difficulties have been thought of as an entity separated from the attention deficit (Pitcher et al., 2003; Miyahara et al., 2006), and pharmacological interventions do not seem to produce any remarkable improvement in motor coordination of ADHD individuals (e.g., Bart et al., 2010).
Problem-Solving/Management of Time
Time processing is also affected in ADHD as it is evidenced in both behavioral (Hwang et al., 2010; Zelaznik et al., 2012), and neuroimaging (Hart et al., 2012) studies. The representation of time is crucial not only for everyday functioning but also to make long-term life plans (see Noreika et al., 2013 for review). Related to the time perception deficit is the difficulty that children with ADHD experience in tasks that require order or sequence (Barkley and Murphy, 2006). Poor skills in the management of time may be on the basis of the poor problem solving strategies frequently shown by these children. Accordingly, training metacognitive skills has shown good results in ADHD children (Tamm et al., 2014).
Disruptive Behavior
The oppositional defiant disorder (ODD) is the most common comorbid condition associated to ADHD during childhood (Steinhausen et al., 2006). Children with ADHD have an increased risk to develop disruptive behavior (Bendiksen et al., 2014), which extends into the adulthood period (e.g., Reimherr et al., 2013). ADHD is also considered a predictor of risky sexual behavior (Flory et al., 2006), romantic partner problems (Wymbs et al., 2011), legal problems (Ginsberg et al., 2010), and unemployment in adulthood (Kessler et al., 2006).
Sleep Habits
Children and adults with ADHD may present some symptoms related to sleep disorders such as daytime sleep, insomnia, fractured sleep, restless legs syndrome and sleep-disordered breathing (for a review, see Yoon et al., 2012). Despite a relationship between ADHD and sleep disorders has been documented, whether such relationship is direct or indirect is still unclear (e.g., Accardo et al., 2012). Consequently, some authors have suggested including the assessment of children’s sleep habits as part of the ADHD clinical diagnosis routine (e.g., Spruyt and Gozal, 2011).
Academic Achievement
The relationship between ADHD and poor academic achievement is well established (Loe and Feldman, 2007; Langberg et al., 2011; for a review, see Arnold et al., 2015; for longitudinal studies, see Barbaresi et al., 2007; Sayal et al., 2015). In fact, learning disorders affecting language, reading, and math are common comorbidities of children diagnosed with ADHD (DuPaul et al., 2014; Taanila et al., 2014). Also, symptoms of inattention, hyperactivity, and impulsivity with or without formal diagnosis of ADHD are related with poor academic and educational outcomes (Birchwood and Daley, 2012), specially with inattentiveness (Wu and Gau, 2013). Similarly, poor productivity and low self-management of homework are frequent in children with ADHD (Power et al., 2006).
Quality of Life
Attention-deficit/hyperactivity disorder affects children and adolescents’ quality of life involving psychosocial, achievement, and self-evaluation domains (for a review, see Wehmeier et al., 2010). Families with an ADHD child show some functioning deficits regarding both economy (Harpin, 2005) and marital relations (Escobar et al., 2005). The divorce rate of parents with an ADHD child is higher compared with parents of children without ADHD (Wymbs et al., 2008; Kvist et al., 2013). Thus, quality of life is emerging as an important aspect of the comprehensive diagnosis of ADHD (Coghill, 2010).
The Current Study
Here we are concerned with developing a brief scale that provides both clinicians and researchers with an appropriate complementary diagnostic tool that takes into account the diversity of symptoms and the heterogeneity of the ADHD disease. The scale is also meant to providing clinicians with an instrument that can help design more comprehensive therapeutic targets that include not only the core ADHD symptoms but also some important difficulties associated with the disease. But, what would such a scale, which is intended to assess non-ADHD specific features that simply co-occur with the disease, add to already existing ADHD screening instruments?
First, most existing ADHD rating scales show certain constrains regarding the ADHD assessment process (e.g., Snyder et al., 2006), which may lead many clinicians to recruit additional clinical information (Pelham et al., 2005; Posserud et al., 2014; Shemmassian and Lee, 2014). Second, despite there are some scales that assess comorbid difficulties associated with an ADHD diagnosis, (e.g., Conners 3; Conners, 2008), the majority of them are rather long, expensive and are not intended to be used for rather wide screening processes (e.g., in schools). In addition, they hardly assess the presence of comorbidity beyond some behavioral disruptive symptoms. While their relevance is undeniable diagnostic-wise, it is more questionable treatment-wise. Third, although there are some brief screening scales (e.g., Impairment Rating Scale, Fabiano et al., 2006; Child Behavior Checklist, Achenbach and Rescorla, 2001; Child and Adolescent Functional Assessment Scale Hodges and Wong, 1996), they have not been specifically designed to assess comorbidity associated to ADHD. In addition, the majority of the screening scales for ADHD are primarily based on core symptoms of the disorder (i.e., inattention and hyperactivity/impulsivity symptoms), which generates a decrease in the sensibility of the scales due to subclinical heterogeneity (e.g., Ullebø et al., 2011).
In the present study we aimed to build a brief ADHD impairment-related tool, the ADHD Concomitant Difficulties Scale (hereafter ADHD-CDS), that serves two main functions: (i) to discriminate some profiles that present several and important ADHD functional difficulties; and (ii) to foster a comprehensive evaluation process that can be easily used by both clinicians and researchers. The aim of the ADHD-CDS was to assess the presence of some of the most important comorbidities, previously described, that usually appear associated to ADHD. It is important to highlight that the aforementioned deficits are not attributable directly to ADHD; they just co-occur frequently with the disease and therefore it cannot permit establishing any causal relation.
Materials and Methods
Participants
A sample of 696 families of children with and without a diagnosis of ADHD gave informed consent to participate in the study. Parents of ADHD children were recruited from some child mental health clinics and family support associations. The ADHD sample included parents of 399 children aged 6–18 years (M = 11.65; SD = 3.1; 280 males). Mental health professionals entirely blinded regarding the objectives of the study, performed the ADHD diagnosis. They all used the inattention (ADHD-IN) and hyperactivity/impulsivity (ADHD-HY) symptoms from the ADHD-Rating Scale-IV (DuPaul et al., 1998) for ADHD diagnosis purpose. From the ADHD group, 307 children were of the combined subtype and 92 from the inattentive subtype. The control group was composed of parents of 297 children aged 6–18 years without ADHD symptoms (M = 10.91; SD = 3.2; 149 male), recruited from some schools in the local area. Control participants were excluded if they scored above the clinical threshold of ADHD-RS-IV parent ratings. Demographic and clinical characteristics of the whole sample are shown in Table 1.
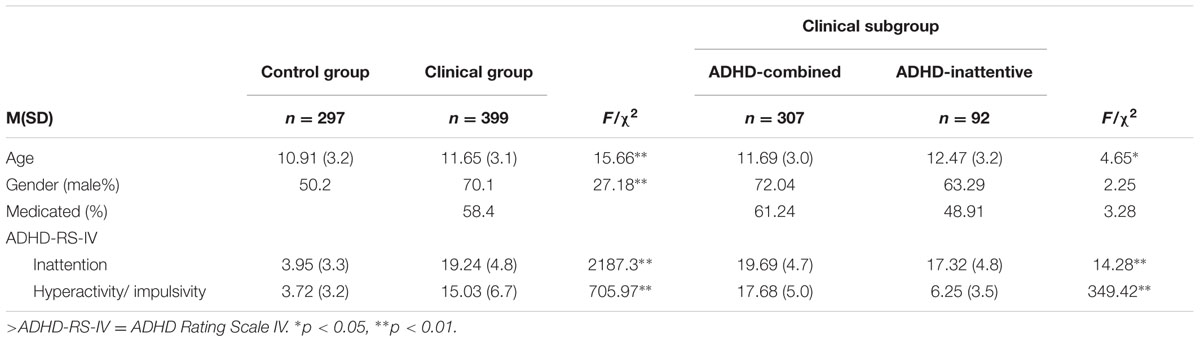
TABLE 1. Demographic and clinical information of clinical and control samples.
The Ethics Committee of the University of Murcia approved the study. All participants were informed of the objectives and methods of the study. Parents completed the clinical scales and a brief sociodemographic questionnaire in web format. We guaranteed confidentiality of participants throughout the study.
Procedure
The scale construction followed an item improved sequential process. The first pool of items was comprised of 55 items equally distributed along the seven areas. We first selected a committee of four experts from university academics and clinicians specialized in ADHD. The committee assessed the original pool and reduced it from 55 to 20 items by selecting the most comprehensive items on the basis of clarity, precision, and plainness. Those items which were agreed in terms of the precision in their definition and the degree of sufficiency were selected. Thirteen psychology postgraduate and 66 psychopedagogy undergraduate students that volunteered to participate, formed a second group. Students rated each remaining item with a score ranging from 0 to 4 on the basis of their clarity, intelligibility, and ease to understand (e.g., 0 = “Not clear at all” to 4 = “Absolutely clear”). Items reaching average scores of 3 or less, and/or Content Validity Index (i.e., experts’ ratings of item relevance) lower than 0.50 were further excluded, reducing the pool from 20 to 17 items (see Table 2).
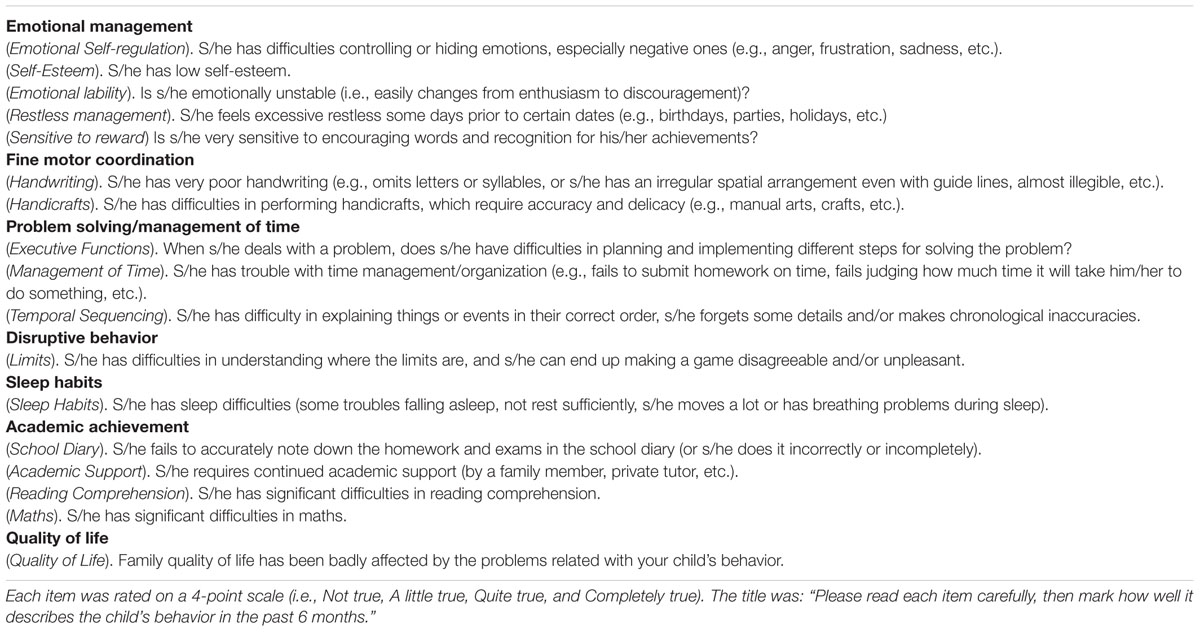
TABLE 2. Seven areas assessed for the current study by First Scale Model (abbreviated item form).
The resulting 17 items of the ADHD-CDS, as well as the rest of questionnaires and scales (sociodemographic, diagnosis, medication, and ADHD-Rating Scale-IV), were fitted into a web format. Parents were given access to the scales online and results were encrypted for later correction. Parents first rated the occurrence of inattention and hyperactivity/impulsivity symptoms affecting their children for the past 6 months on a Likert-type 4-point scale (0 = never or rarely, 1 = sometimes, 2 = often, 3 = very often), according to the ADHD Rating Scale-IV (DuPaul et al., 1998). The two types of ADHD-related symptoms have demonstrated adequate psychometric properties in previous studies with both American and Spanish children (Servera and Cardo, 2007). Cronbach’s alphas for the inattention and hyperactivity/impulsivity subscales for parents’ report were 0.91 and 0.90, respectively. Later on, parents provided sociodemographic and clinical information and filled in the current ADHD-CDS.
Statistical Analysis
Responses collected from parents to the ADHD-CDS were analyzed according to the following sequence:
(i) Differences between parents’ responses from the clinical and control groups were computed by using non-parametric tests. The Mann–Whitney U test was used to compare the control vs. the clinical groups, and the Kruskall–Wallis χ2 test was used to compare the control vs. the ADHD clinical presentations. We checked whether case-control differences were due to either age or gender.
(ii) Principal Axis Factoring was used to determine the latent structure of items. Such method of factoring is recommended for non-normal distributions (Costello and Osborne, 2005). We included all participants to maximize statistical power. Alternative models were also compared with the single-factor model, and at this end we forced the rotation.
(iii) Confirmatory Factor Analysis with diagonally weighted least squares method (cat-DWLS) was performed on the basis of the re-specified model from EFA. We used Mplus 14 software for that purpose.
(iv) ADHD-CDS single total scores (i.e., the sum of items) were computed and used to estimate correlations. We also computed unique effects among ADHD-IN, ADHD-HY, and ADHD-CDS total score (Spearman’s correlation and multiple regressions analysis, respectively).
(v) We conducted sensitivity and specificity analyses, and estimated the area under the ROC curve.
Results
Non-parametric analyses were conducted with the total sample because item-domain scores followed non-normal distributions (Kolmogorov–Smirnov test p < 0.05). Concretely, the Mann–Whitney U test was employed to assess the differences between the control and the clinical taken gender as a between-subjects factor; and Cliff’s delta was used to estimate the effect sizes. In contrast, the clinical sample scores followed a normal distribution (Kolmogorov–Smirnov test p > 0.05).
In the clinical group males outperformed females in handicrafts (U = 5124; δ = 0.25), limits (U = 5690; δ = 0.17), and school diary (U = 5482; δ = 0.20), whereas females outperformed males in mathematics (U = 5280; δ = -0.23). The same gender differences were also found in the control group, but the male superiority extended to handwriting (U = 3752; δ = 0.15), and quality of life (U = 3814; δ = 0.14). Children from the clinical group that were taking medication showed lower scores in both limits (U = 5746.5; δ = 0.20) and quality of life (U = 5911; δ = 0.22), compared to children that were not taking medication. Age correlated significantly with time management (ρ = 0.17, p < 0.01), quality of life (ρ = 0.15, p < 0.01), and mathematics (ρ = 0.28, p < 0.01).
Both the ADHD-combined and the ADHD-inattentive subgroups showed higher scores than the control group in all domains (see Table 3). Nevertheless, some differences between the two clinical subgroups were also found. The ADHD-inattentive subgroup showed lower scores than the ADHD-combined subgroup in emotional self-regulation, emotional lability, handwriting, problem solving, quality of life, and limits.
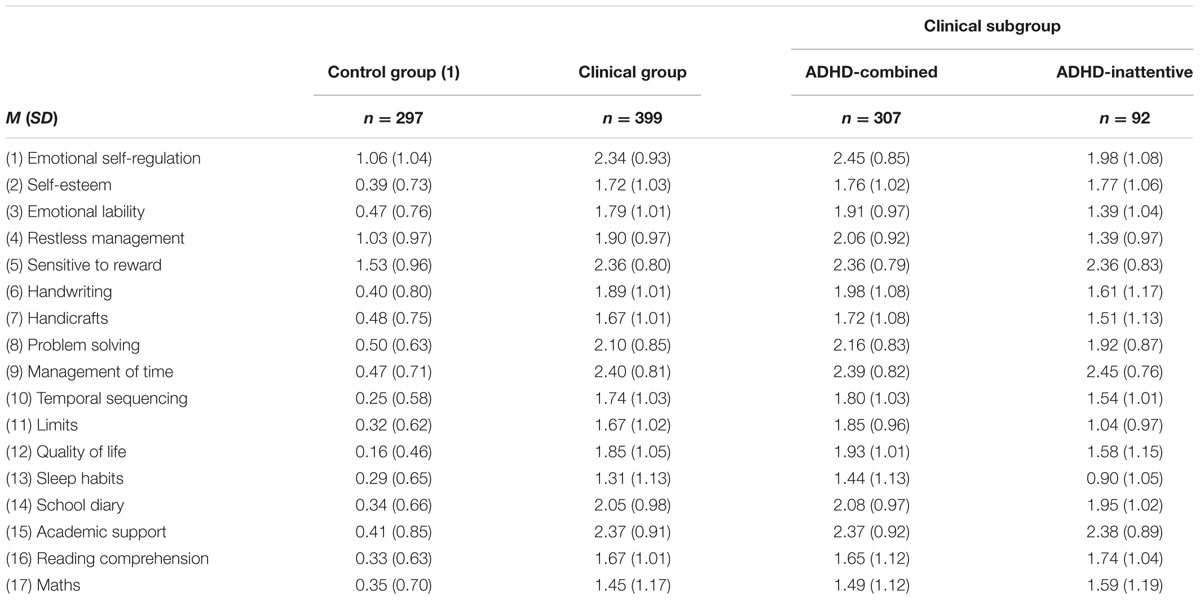
TABLE 3. Mean scores in the preliminary 17-item scale in both the clinical (and clinical subgroups) and the control groups.
The control group mean scores were greater than 1 in three items, emotional self-regulation, restless management, and sensitive to reward. As the mean scores of those three items were higher than the 0.5 exclusion criterion for controls, and almost three times greater than the mean of the remaining items (M = 0.37), they were further excluded from the scale. Additionally, the sleep habits item scored below 1.5 in the clinical group, and thus is was also excluded from the scale.
Spearman’s rank correlation coefficients were also computed (Table 4). Correlation between ADHD-dimensions and items were moderate-to-high for inattention (ρ = 0.52 to 0.81; ps < 0.001), and low-to-high for hyperactive/impulsivity (ρ = 0.37 to 0.70; ps < 0.001). With the exception of limits (ADHD-IN, ρ = 0.68, p < 0.001; ADHD-HY ρ = 0.72, p < 0.001), the correlations for each domain were greater for ADHD-IN (ρ ranged from 0.52 to 0.81; all ps < 0.001) than for ADHD-HY (ρ ranged from 0.34 to 0.72; all ps < 0.001).
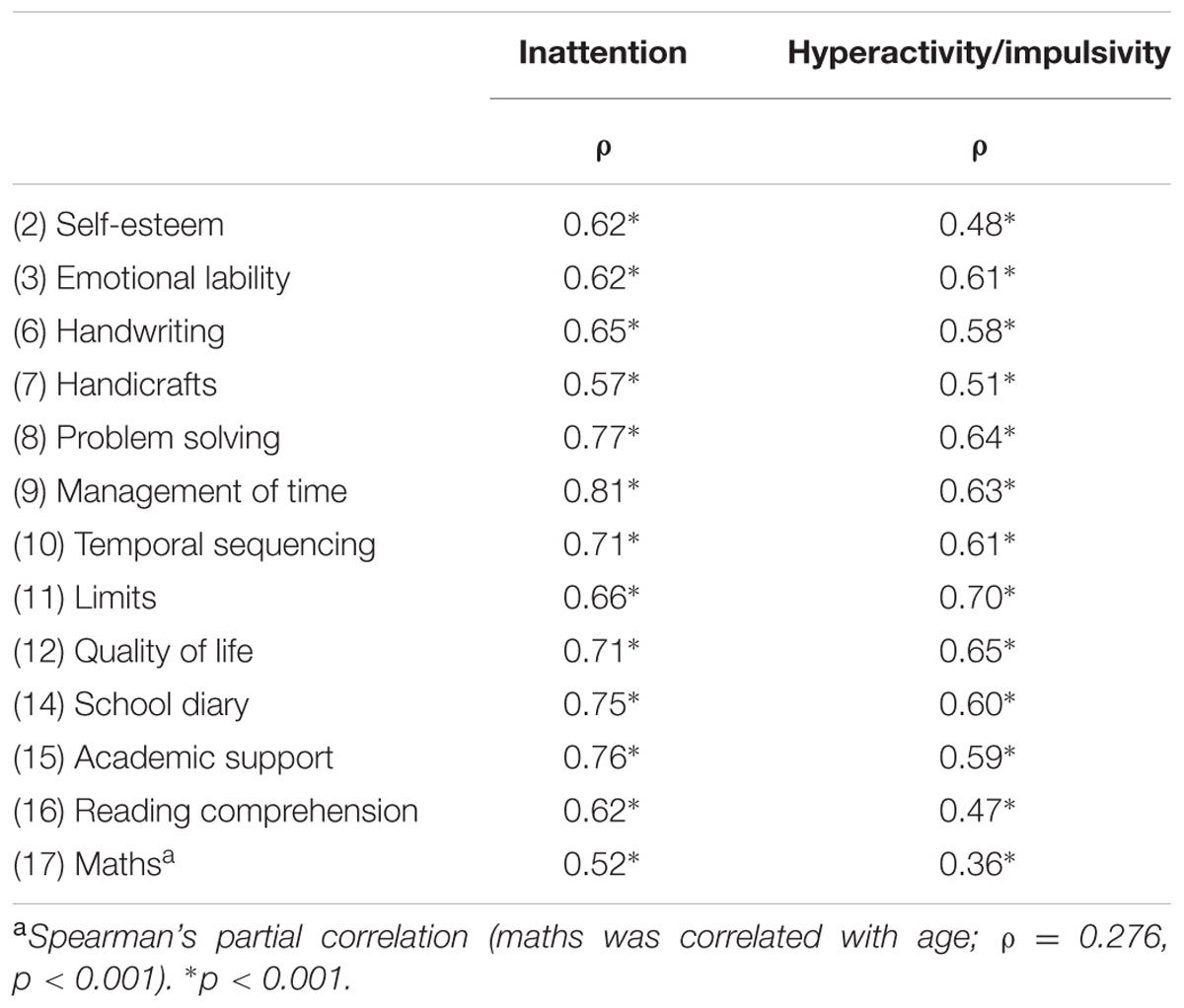
TABLE 4. Spearman’s correlations between items and ADHD dimensions (n = 696).
Factor Structure of ADHD-CDS Items
The results showed a 13-item single factor model with good fit indices (Table 5). Factor loadings ranged from 0.62 (maths) to 0.85 (academic support). Results of the 13-item exploratory factor analysis supported a single total score. The sum of 13 items generated an ADHD-CDS total score, with higher scores indicating greater degree of ADHD difficulties (total score ranging from 0 to 39). Cronbach’s alpha coefficient was 0.94, and corrected item-total correlations were medium-to-high, ranging 0.59 to 0.82, indicating high internal consistency reliability.
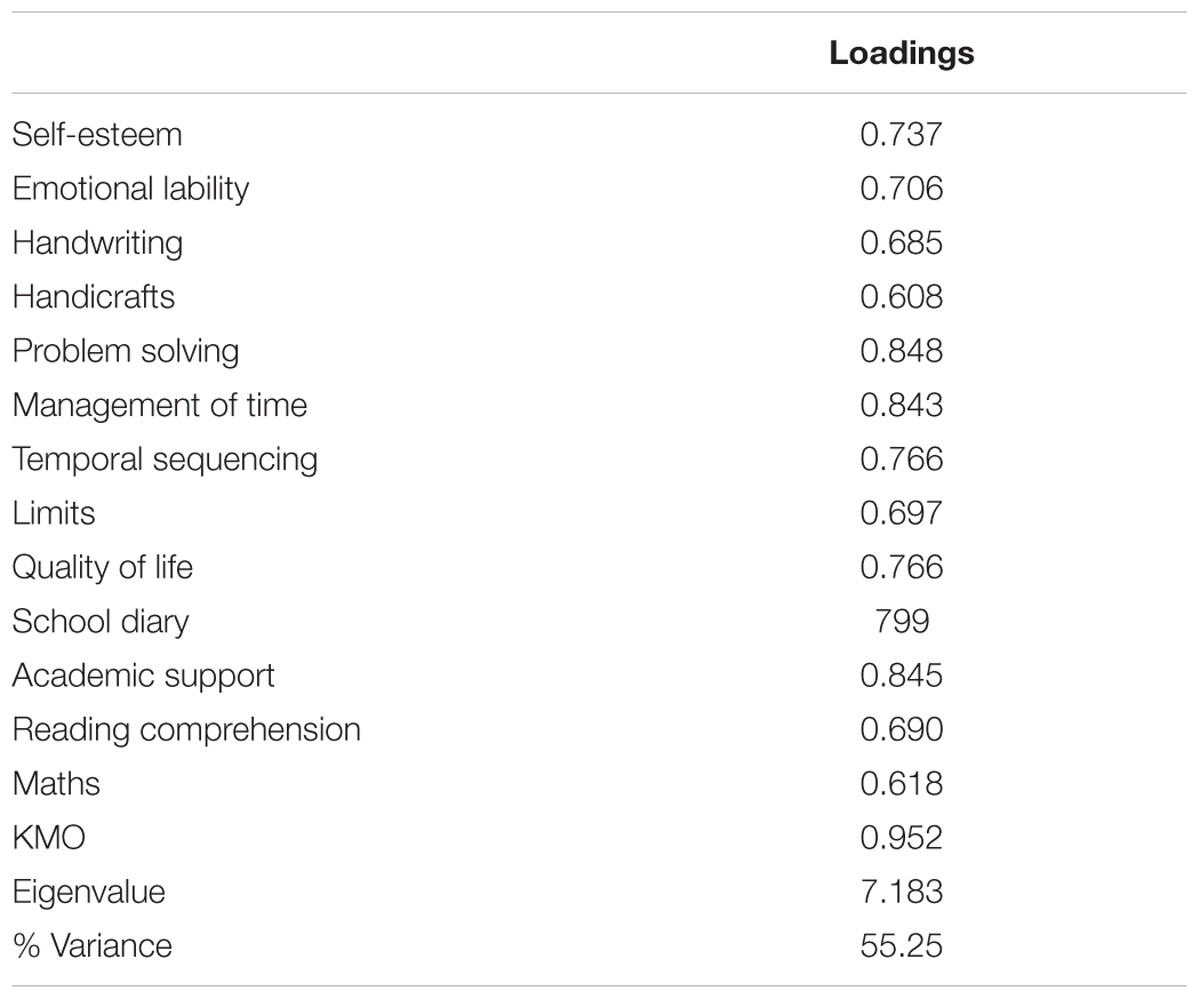
TABLE 5. Single factor loadings for the 13-items scale (principal axis factoring).
We also computed two- and three- exploratory factor models by forcing the rotations. However, because the eigenvalues were significantly lower than 1 (eigenvalues from 0.487 to 0.502) the multi-factor models were rejected (Kaiser’s criterion). Accordingly, we did not conduct any confirmatory factor analysis with the alternative models, nor did compare them with the single factor model.
An additional confirmatory factor analysis with diagonally weighted least squares method (cat-DWLS) was also conducted to verify that each item loaded onto one single component factor. All items converged into one general factor, ADHD concomitant difficulties, with χ2 (65) = 543.36; p < 0.001; RMSA = 0.01; WRMR = 1.586; CFI = 0.98; TLI = 0.98. Standardized factor loadings were from 0.61 to 0.91. Hence, the fit indices indicated a satisfactory fit to the single-factor structure1.
Correlations and Unique Effects among ADHD-IN, ADHD-HY and ADHD-CDS Total Score
We computed Spearman rank correlation coefficients between the ADHD dimensions and the total score. Total score was positive correlated with both ADHD-IN (ρ = 0.88; p < 0.001) and ADHD-HY (ρ = 0.74; p < 0.001). Nevertheless, when only the clinical sample was analyzed, the correlations were rather moderate (for ADHD-IN, ρ = 0.541; p < 0.001; for ADHD-HY, ρ = 0.345; p < 0.001). After controlling for ADHD-IN there was no relationship between ADHD-HY and ADHD-CDS (β = 0.05; SE = 0.06; p > 0.05). The ADHD-IN scores predicted ADHD-CDS scores for both the clinical sample (β = 0.50; SE = 0.08; p < 0.001) and the whole sample (β = 0.85; SE = 0.01; p < 0.001).
ROC Curve Analysis
The ROC curve for the ADHD-CDS (against the ADHD diagnostic status) gave an area under the curve (AUC) of 0.979 (95%, CI = [0.969, 0.989]), which can be considered very high (Sweet, 1988). The AUC was 0.980 (95%, CI = [0.967, 0.994]) for males, and 0.969 (95%, CI = [0.945, 0.992]) for females. ROC curve analyses were also conducted differentiating between the two clinical subgroups. According to the clinical diagnosis, AUC was 0.981 (95%, CI = [0.970, 0.992]) for the ADHD-combined subgroup and 0.974 (95%, CI = [0.959, 0.989]) for the ADHD-inattentive subgroup.
In addition, the percentage of ADHD cases that scored higher than the 90% of the control group scores was 94.3%. Differentiating between the two clinical subgroups, the percentages were 95.4 and 89.2% for the ADHD-combined and the ADHD-inattentive subgroups, respectively.
Discussion
It is clear that ADHD is a clinical and neuropsychological heterogeneous disorder. At the clinical level, the two main ADHD dimensions described in DSM (i.e., inattention and hyperactivity/impulsivity) are widely validated, although the bidimensional model of ADHD has been recently questioned (Parke et al., 2016). Further, the validity of the three nominal subtypes (i.e., the predominantly hyperactive/impulsive subtype, the predominantly inattentive subtype, and the combined subtype) is also under debate (Willcutt et al., 2012). The debate extends to the relationship between Sluggish Cognitive Tempo (SCT) and ADHD, questioning whether SCT fits well or not into the ADHD DSM model (Willcutt et al., 2014). These are good examples that suggest that the ADHD diagnosis is constantly being reviewed and updated.
At the neuropsychological level, multiple neurocognitive deficits have been associated with the disease. Delay aversion, inhibitory control, timing, time variability, decision-making, and working memory among others, are crucial neuropsychological areas that have been found to be altered in ADHD (e.g., Sonuga-Barke, 2003; Sonuga-Barke et al., 2010; de Zeeuw et al., 2012). Apart from the core clinical and neuropsychological deficits, individuals with ADHD usually show other concomitant difficulties, which are not solely related with ADHD. The nature of the relationship between ADHD and these concomitant difficulties is still unclear, but their high frequency of co-occurrence should be taken into consideration. Thus, an appropriate assessment of those concomitant difficulties associated with ADHD is of special relevance for future research and clinical practice.
In the present study we aimed at constructing a brief scale, the ADHD-CDS, that may be a useful and easy-to-use instrument to detect comorbidity associated to ADHD in both clinical and research contexts. These difficulties might also be the target of clinical interventions concerned with ADHD, such as behavioral modification therapy, emotional and motivational self-management skills, family therapy, and/or metacognitive strategies among others.
Regarding the ADHD-CDS structure, our results with a rather ample sample of both clinical and control participants, suggest that our scale follows a single-factor latent structure. Single-factor models have also been observed in other screening scales when they have been used in both clinical and non-clinical populations (Gomez et al., 2003, 2005). In addition, the present ADHD-CDS shows a high potential discriminatory value for screening ADHD profiles. The predictive value of ADHD-CDS is related to inattention symptoms (but not to hyperactivity/impulsivity symptoms), which allows us to discriminate ADHD profiles irrespective of their clinical subtypes. Thus, ADHD-CDS represents an important improvement from previous ADHD screening scales (e.g., the Strengths and Difficulties Questionnaire; Goodman, 1997), which seem to be influenced by clinical subtypes (e.g., Ullebø et al., 2011).
Finally, the present study has several limitations. First, ADHD-CDS assesses ADHD concomitant difficulties, and thus we cannot establish any causal relation between such deficits and the disorder. Second, as other disorders have not been included in the study we cannot assure that the impairment profile obtained with ADHD-CDS is unique to ADHD. Third, ADHD-CDS includes some but not all concomitant difficulties that may be associated with ADHD. Thus, the current scale should be considered as a preliminary proposal, which is open to the inclusion of other ADHD concomitant difficulties that clinicians may consider relevant in the diagnosis and treatment of ADHD. Four, from a methodological perspective, further studies are needed to test the psychometric properties of the scale on independent samples, particularly including people with other disorders different to ADHD (i.e., ODD, Autism Spectrum Disorders, Intellectual Disability).
In summary, the present results provide additional evidence that ADHD is a complex and highly heterogeneous disorder with some concomitant difficulties in several functional areas. The ADHD-CDS has shown preliminary adequate psychometric properties, with high convergent validity and good sensitivity for different ADHD profiles, which makes it a potentially appropriate and brief instrument that may be easily used by clinicians, researchers, and health professionals in dealing with ADHD.
Author Contributions
JF-C was involved all along the process, from the conception to the revision to the manuscript. LF was involved in the drafting and revision of the manuscript.
Funding
This study was supported by the Spanish Ministry of Economy and Competitivity (project PSI2014-53427-P) and Fundación Séneca (project 19267/PI/14).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
- ^ The ADHD sample includes 70% of males, a figure that fits well with the proportion of males compared with females that are diagnosed with ADHD. However, the control group sample size reflects what it should be expected by random selection. To rule out the possibility that the differences between the ADHD and control groups are due to differences in gender proportion (and probably sample size) in the two samples, we re-ran the analyses with a reduced sample, randomly chosen, from both the clinical and control groups, so that both gender proportion (fitting the male proportion of ADHD diagnosis) and sample size were matched between the two groups (n = 256; 71.8% males). The results also showed a 13-item single factor model with good fit indices, both for EFA (KMO = 0.953; p < 0.001; eigenvalue = 7.30; 56% variance explained; loads 0.62 to 0.86 and CFA [χ2 (65) = 378.32; p < 0.001; RMSA = 0.09; WRMR = 1.325; CFI = 0.98; TLI = 0.98. Standardized factor loadings were from 0.68 to 0.92]. The reliability was high (Cronbach’s alpha = 0.94). There were significant differences between the clinical and the control group for ADHD-CDS total score (Mann–Whitney U = 1695; p < 0.001 or T-test = -34.62; p < 0.001). The correlations between ADHD dimensions and ADHD-CDS total score were high (Spearman’s Rho = 0.88 for inattention and 0.76 for hyperactivity/impulsivity).
References
Accardo, J. A., Marcus, C. L., Leonard, M. B., Shults, J., Meltzer, L. J., and Elia, J. (2012). Associations between psychiatric comorbidities and sleep disturbances in children with attention-deficit/hyperactivity disorder. J. Dev. Behav. Pediatr. 33, 97.
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edn. Arlington, VA: American Psychiatric Publishing.
Anastopoulos, A. D., Smith, T. F., Garrett, M. E., Morrissey-Kane, E., Schatz, N. K., Sommer, J. L., et al. (2011). Self-regulation of emotion, functional impairment, and comorbidity among children with AD/HD. J. Atten. Disord. 15, 583–592. doi: 10.1177/1087054710370567
Arnold, L. E., Hodgkins, P., Kahle, J., Madhoo, M., and Kewley, G. (2015). Long-term outcomes of ADHD academic achievement and performance. J. Atten. Disord. doi: 10.1177/1087054714566076 [Epub ahead of print].
Barbaresi, W. J., Katusic, S. K., Colligan, R. C., Weaver, A. L., and Jacobsen, S. J. (2007). Long-term school outcomes for children with attention-deficit/hyperactivity disorder: a population-based perspective. J. Dev. Behav. Pediatr. 28, 265–273. doi: 10.1097/DBP.0b013e31811ff87d
Barkley, R. A. (2006). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment, 3rd Edn. New York, NY: Guilford.
Barkley, R. A., and Murphy, K. R. (2006). Identifying new symptoms for diagnosing ADHD in adulthood. ADHD Rep. 14, 7–11. doi: 10.1521/adhd.2006.14.4.7
Bart, O., Podoly, T., and Bar-Haim, Y. (2010). A preliminary study on the effect of methylphenidate on motor performance in children with comorbid DCD and ADHD. Res. Dev. Disabil. 31, 1443–1447. doi: 10.1016/j.ridd.2010.06.014
Bendiksen, B., Svensson, E., Aase, H., Reichborn-Kjennerud, T., Friis, S., Myhre, A. M., et al. (2014). Co-occurrence of ODD and CD in preschool children with symptoms of ADHD. J. Atten. Disord. doi: 10.1177/1087054714538655 [Epub ahead of print].
Birchwood, J., and Daley, D. (2012). Brief report: the impact of attention deficit hyperactivity disorder (ADHD) symptoms on academic performance in an adolescent community sample. J. Adolesc. 35, 225–231. doi: 10.1016/j.adolescence.2010.08.011
Brossard-Racine, M., Majnemer, A., Shevell, M., Snider, L., and Bélanger, S. A. (2011). Handwriting capacity in children newly diagnosed with attention deficit hyperactivity disorder. Res. Dev. Disabil. 32, 2927–2934. doi: 10.1016/j.ridd.2011.05.010
Classi, P., Milton, D., Ward, S., Sarsour, K., and Johnston, J. (2012). Social and emotional difficulties in children with ADHD and the impact on school attendance and healthcare utilization. Child Adolesc. Psychiatry Ment. Health 6, 33–33. doi: 10.1186/1753-2000-6-33
Coghill, D. (2010). The impact of medications on quality of life in attention-deficit hyperactivity disorder. CNS Drugs 24, 843–866. doi: 10.2165/11537450-000000000-00000
Costello, A. B., and Osborne, J. W. (2005). Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Pract. Assess. Res. Eval. 10, 1–9.
de Zeeuw, P., Weusten, J., van Dijk, S., Van Belle, J., and Durston, S. (2012). Deficits in cognitive control, timing and reward sensitivity appear to be dissociable in ADHD. PLoS ONE 7:e51416. doi: 10.1371/journal.pone.0051416
DuPaul, G. J., Gormley, M. J., and Laracy, S. D. (2014). School-based interventions for elementary school students with ADHD. Child Adolesc. Psychiatr. Clin. N. Am 23, 687–697. doi: 10.1016/j.chc.2014.05.003
DuPaul, G. J., Power, T. J., Anastopoulos, A. D., and Reid, R. (1998). ADHD Rating Scale-IV: Checklists, Norms, and Clinical Interpretation, Vol. 25. New York, NY: Guilford Press.
Edbom, T., Lichtenstein, P., Granlund, M., and Larsson, J. O. (2006). Long-term relationships between symptoms of attention deficit hyperactivity disorder and self-esteem in a prospective longitudinal study of twins. Acta Paediatr. 95, 650–657. doi: 10.1111/j.1651-2227.2006.tb02311.x
Escobar, R., Soutullo, C. A., Hervas, A., Gastaminza, X., Polavieja, P., and Gilaberte, I. (2005). Worse quality of life for children with newly diagnosed attention-deficit/hyperactivity disorder, compared with asthmatic and healthy children. Pediatrics 116, e364–e369. doi: 10.1542/peds.2005-0386
Fabiano, G. A., Pelham, W. E. Jr., Waschbusch, D. A., Gnagy, E. M., Lahey, B. B., Chronis, A. M., et al. (2006). A practical measure of impairment: psychometric properties of the impairment rating scale in samples of children with attention deficit hyperactivity disorder and two school-based samples. J. Clin. Child Adolesc. Psychol. 35, 369–385. doi: 10.1207/s15374424jccp3503_3
Fliers, E., Rommelse, N., Vermeulen, S. H. H. M., Altink, M., Buschgens, C. J. M., Faraone, S. V., et al. (2008). Motor coordination problems in children and adolescents with ADHD rated by parents and teachers: effects of age and gender. J. Neural. Transm. 115, 211–220. doi: 10.1007/s00702-007-0827-0
Fliers, E. A., Franke, B., Lambregts-Rommelse, N. N. J., Altink, M. E., Buschgens, C. J. M., Nijhuis-van der Sanden, M. W. G., et al. (2010). Undertreatment of motor problems in children with ADHD. Child Adolesce Ment. Health 15, 85–90. doi: 10.1111/j.1475-3588.2009.00538.x
Flory, K., Molina, B. S., Pelham, W. E. Jr., Gnagy, E., and Smith, B. (2006). Childhood ADHD predicts risky sexual behavior in young adulthood. J. Clin. Child Adolesc. Psychol. 35, 571–577. doi: 10.1207/s15374424jccp3504_8
Fosco, W. D., Hawk, L. W., Rosch, K. S., and Bubnik, M. G. (2015). Evaluating cognitive and motivational accounts of greater reinforcement effects among children with attention-deficit/hyperactivity disorder. Behav. Brain Funct. 11, 20. doi: 10.1186/s12993-015-0065-9
Ginsberg, Y., Hirvikoski, T., and Lindefors, N. (2010). Attention deficit hyperactivity disorder (ADHD) among longer-term prison inmates is a prevalent, persistent and disabling disorder. BMC psychiatry 10:112. doi: 10.1186/1471-244X-10-112
Gomez, R., Burns, G. L., Walsh, J. A., and De Moura, M. A. (2003). Multitrait-multisource confirmatory factor analytic approach to the construct validity of ADHD rating scales. Psychol. Assess. 15, 3–16. doi: 10.1037/1040-3590.15.1.3
Gomez, R., Burns, G. L., Walsh, J. A., and Hafetz, N. (2005). A multitrait–multisource confirmatory factor analytic approach to the construct validity of ADHD and ODD rating scales with Malaysian children. J. Abnorm. Child Psychol. 33, 241–254. doi: 10.1007/s10802-005-1831-1
Goodman, R. (1997). The strengths and difficulties questionnaire: a research note. J. Child Psychol. Psychiatry 38, 581–586. doi: 10.1111/j.1469-7610.1997.tb01545.x
Goulardins, J. B., Marques, J. C. B., Casella, E. B., Nascimento, R. O., and Oliveira, J. A. (2013). Motor profile of children with attention deficit hyperactivity disorder, combined type. Res. Dev. Disabil. 34, 40–45. doi: 10.1016/j.ridd.2012.07.014
Harpin, V. A. (2005). The effect of ADHD on the life of an individual, their family, and community from preschool to adult life. Arch. Dis. Child. 90(Suppl. 1), i2–i7. doi: 10.1136/adc.2004.059006
Hart, H., Radua, J., Mataix-Cols, D., and Rubia, K. (2012). Meta-analysis of fMRI studies of timing in attention-deficit hyperactivity disorder (ADHD). Neurosci. Biobehav. Rev. 36, 2248–2256. doi: 10.1016/j.neubiorev.2012.08.003
Hodges, K., and Wong, M. M. (1996). Psychometric characteristics of a multidimensional measure to assess impairment: the child and adolescent functional assessment scale. J. Child Fam. Stud. 5, 445–467. doi: 10.1007/BF02233865
Hwang, S. L., Gau, S. S. F., Hsu, W. Y., and Wu, Y. Y. (2010). Deficits in interval timing measured by the dual-task paradigm among children and adolescents with attention-deficit/hyperactivity disorder. J. Child Psychol. Psychiatry 51, 223–232. doi: 10.1111/j.1469-7610.2009.02163.x
Jarrett, M. A. (2016). Attention-deficit/hyperactivity disorder (adhd) symptoms, anxiety symptoms, and executive functioning in emerging adults. Psychol. Assess. 28, 245–250. doi: 10.1037/pas0000190
Kessler, R. C., Adler, L., Barkley, R., Biederman, J., Conners, C. K., Demler, O., et al. (2006). The prevalence and correlates of adult ADHD in the United States: results from the national comorbidity survey replication. Am. J. Psychiatry 163, 716–723. doi: 10.1176/appi.ajp.163.4.716
Kvist, A. P., Nielsen, H. S., and Simonsen, M. (2013). The importance of children’s ADHD for parents’ relationship stability and labor supply. Soc. Sci. Med. 88, 30–38. doi: 10.1016/j.socscimed.2013.04.001
Langberg, J. M., Molina, B. S., Arnold, L. E., Epstein, J. N., Altaye, M., Hinshaw, S. P., et al. (2011). Patterns and predictors of adolescent academic achievement and performance in a sample of children with attention-deficit/hyperactivity disorder. J. Clin. Child Adolesc. Psychol. 40, 519–531. doi: 10.1080/15374416.2011.581620
Loe, I. M., and Feldman, H. M. (2007). Academic and educational outcomes of children with ADHD. J. Pediatr. Psychol. 32, 643–654. doi: 10.1093/jpepsy/jsl054
Miyahara, M., Piek, J., and Barrett, N. (2006). Accuracy of drawing in a dual-task and resistance-to-distraction study: Motor or attention deficit? Hum. Mov. Sci. 25, 100–109. doi: 10.1016/j.humov.2005.11.004
Noreika, V., Falter, C. M., and Rubia, K. (2013). Timing deficits in attention-deficit/hyperactivity disorder (ADHD): evidence from neurocognitive and neuroimaging studies. Neuropsychologia 51, 235–266. doi: 10.1016/j.neubiorev.2012.08.003
Parke, E. M., Mayfield, A. R., Barchard, K. A., Thaler, N. S., Etcoff, L. M., and Allen, D. N. (2016). Factor Structure of Symptom Dimensions in Attention-Deficit/Hyperactivity Disorder (ADHD). Psychol. Assess. 27, 1427–2437. doi: 10.1037/pas0000121
Pelham, W. E. Jr., Fabiano, G. A., and Massetti, G. M. (2005). Evidence-based assessment of attention deficit hyperactivity disorder in children and adolescents. J. Clin. Child Adolesc. Psychol. 34, 449–476. doi: 10.1207/s15374424jccp3403_5
Pitcher, T. M., Piek, J. P., and Hay, D. A. (2003). Fine and gross motor ability in males with ADHD. Dev. Med. Child Neurol. 45, 525–535. doi: 10.1111/j.1469-8749.2003.tb00952.x
Posserud, M. B., Ullebø, A. K., Plessen, K. J., Stormark, K. M., Gillberg, C., and Lundervold, A. J. (2014). Influence of assessment instrument on ADHD diagnosis. Euro. Child Adolesc. Psychiatry 23, 197–205. doi: 10.1007/s00787-013-0442-6
Power, T. J., Werba, B. E., Watkins, M. W., Angelucci, J. G., and Eiraldi, R. B. (2006). Patterns of parent-reported homework problems among ADHD-referred and non-referred children. Sch. Psychol. Quart. 21, 13. doi: 10.1521/scpq.2006.21.1.13
Reimherr, F. W., Marchant, B. K., Olsen, J. L., Wender, P. H., and Robison, R. J. (2013). Oppositional defiant disorder in adults with ADHD. J. Atten. Disord. 17, 102–113. doi: 10.1177/1087054711425774
Retz, W., Stieglitz, R., Corbisiero, S., Retz-Junginger, P., and Rösler, M. (2012). Emotional dysregulation in adult ADHD: What is the empirical evidence? Exp. Rev. Neurother. 12, 1241–1251. doi: 10.1586/ern.12.109
Rosenblum, S., Epsztein, L., and Josman, N. (2008). Handwriting performance of children with attention deficit hyperactive disorders: a pilot study. Phys. Occup. Ther. Pediatr. 28, 219–234. doi: 10.1080/01942630802224934
Sayal, K., Washbrook, E., and Propper, C. (2015). Childhood behavior problems and academic outcomes in adolescence: longitudinal population-based study. J. Am. Acad. Child Adolesc. Psychiatry 54, 360–368. doi: 10.1016/j.jaac.2015.02.007
Scharoun, S. M., Bryden, P. J., Otipkova, Z., Musalek, M., and Lejcarova, A. (2013). Motor skills in Czech children with attention-deficit hyperactivity disorder and their neurotypical counterparts. Res. Dev. Disabil. 34, 4142–4153. doi: 10.1016/j.ridd.2013.08.011
Servera, M., and Cardo, E. (2007). ADHD Rating Scale-IV en una muestra escolar española: datos normativos y consistencia interna para maestros, padres y madres. Rev. Neurol. 45, 393–399.
Shemmassian, S. K., and Lee, S. S. (2014). Comparative validity of DSM-IV and alternative empirically derived approaches for the assessment of ADHD. J. Attent. Disord. doi: 10.1177/1087054714522511 [Epub ahead of print].
Shen, I. H., Lee, T. Y., and Chen, C. L. (2012). Handwriting performance and underlying factors in children with attention deficit hyperactivity disorder. Res. Dev. Disabil. 33, 1301–1309. doi: 10.1016/j.ridd.2012.02.010
Snyder, S. M., Hall, J. R., Cornwell, S. L., and Quintana, H. (2006). Review for clinical validation of ADHD behavior rating scales. Psychol. Rep. 99, 363–378. doi: 10.2466/pr0.99.2.363-378
Sonuga-Barke, E., Bitsakou, P., and Thompson, M. (2010). Beyond the dual pathway model: evidence for the dissociation of timing, inhibitory, and delay-related impairments in attention-deficit/hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 49, 345–355. doi: 10.1016/j.jaac.2009.12.018
Sonuga-Barke, E. J. (2003). The dual pathway model of AD/HD: an elaboration of neuro-developmental characteristics. Neurosci. Biobehav. Rev. 27, 593–604. doi: 10.1016/j.neubiorev.2003.08.005
Sonuga-Barke, E. J., Koerting, J., Smith, E., McCann, D. C., and Thompson, M. (2011). Early detection and intervention for attention-deficit/hyperactivity disorder. Exp. Rev. Neurother. 11, 557–563. doi: 10.1586/ern.11.39
Spruyt, K., and Gozal, D. (2011). Sleep disturbances in children with attention-deficit/hyperactivity disorder. Exp. Rev. Neurother. 11, 565–577. doi: 10.1586/ern.11.7
Steinhausen, H. C., Nøvik, T. S., Baldursson, G., Curatolo, P., Lorenzo, M. J., Pereira, R. R., et al. (2006). Co-existing psychiatric problems in ADHD in the ADORE cohort. Eur. Child Adolesc. Psychiatry 15, i25–i29. doi: 10.1007/s00787-006-1004-y
Sweet, J. A. (1988). Measuring the accuracy of diagnostic systems. Science 240, 1285–1293. doi: 10.1126/science.3287615
Taanila, A., Ebeling, H., Tiihala, M., Kaakinen, M., Moilanen, I., Hurtig, T., et al. (2014). Association between childhood specific learning difficulties and school performance in adolescents with and without ADHD symptoms: a 16-year follow-up. J. Atten. Disord. 18, 61–72. doi: 10.1177/1087054712446813
Tamm, L., Nakonezny, P. A., and Hughes, C. W. (2014). An open trial of a metacognitive executive function training for young children with ADHD. J. Attent. Disord. 18, 551–559. doi: 10.1177/1087054712445782
Ullebø, A. K., Posserud, M., Heiervang, E., Gillberg, C., and Obel, C. (2011). Screening for the attention deficit hyperactivity disorder phenotype using the strength and difficulties questionnaire. Euro. Child y Adolesc. Psychiatry 20, 451–458. doi: 10.1007/s00787-011-0198-9
van Hulst, B. M., de Zeeuw, P., and Durston, S. (2015). Distinct neuropsychological profiles within ADHD: a latent class analysis of cognitive control, reward sensitivity and timing. Psychol. Med. 45, 735–745. doi: 10.1017/S0033291714001792
Wåhlstedt, C., Thorell, L. B., and Bohlin, G. (2009). Heterogeneity in ADHD: neuropsychological pathways, comorbidity and symptom domains. J. Abnorm. Child Psychol. 37, 551–564. doi: 10.1007/s10802-008-9286-9
Wehmeier, P. M., Schacht, A., and Barkley, R. A. (2010). Social and emotional impairment in children and adolescents with ADHD and the impact on quality of life. J. Adolesc. Health 46, 209–217. doi: 10.1016/j.jadohealth.2009.09.009
Willcutt, E. G., Chhabildas, N., Kinnear, M., DeFries, J. C., Olson, R. K., Leopold, D. R., et al. (2014). The internal and external validity of sluggish cognitive tempo and its relation with DSM–IV ADHD. J. Abnorm. Child Psychol. 42, 21–35. doi: 10.1007/s10802-013-9800-6
Willcutt, E. G., Nigg, J. T., Pennington, B. F., Solanto, M. V., Rohde, L. A., Tannock, R., et al. (2012). Validity of DSM-IV attention deficit/hyperactivity disorder symptom dimensions and subtypes. J. Abnorm. Psychol. 121, 991–1010. doi: 10.1037/a0027347
Wu, S. Y., and Gau, S. S. F. (2013). Correlates for academic performance and school functioning among youths with and without persistent attention-deficit/hyperactivity disorder. Res. Dev. Disabil. 34, 505–515. doi: 10.1016/j.ridd.2012.09.004
Wymbs, B. T., Molina, B., Pelham, W., Cheong, J., Gnagy, E., Belendiuk, K., et al. (2011). Risk of intimate partner violence among young adult males with childhood ADHD. J. Attent. Disord. 16, 373–383. doi: 10.1177/1087054710389987
Wymbs, B. T., Pelham, W. E. Jr., Molina, B. S., Gnagy, E. M., Wilson, T. K., and Greenhouse, J. B. (2008). Rate and predictors of divorce among parents of youths with ADHD. J. Consult. Clin. Psychol. 76, 735. doi: 10.1037/a0012719
Yoon, S. Y. R., Jain, U., and Shapiro, C. (2012). Sleep in attention-deficit/hyperactivity disorder in children and adults: past, present, and future. Sleep Med. Rev. 16, 371–388. doi: 10.1016/j.smrv.2011.07.001
Keywords: attention-deficit/hyperactivity disorder, concomitant difficulties, screening, ADHD functional difficulties, academic achievement, problem-solving/management of time, quality of life
Citation: Fenollar-Cortés J and Fuentes LJ (2016) The ADHD Concomitant Difficulties Scale (ADHD-CDS), a Brief Scale to Measure Comorbidity Associated to ADHD. Front. Psychol. 7:871. doi: 10.3389/fpsyg.2016.00871
Received: 24 January 2016; Accepted: 26 May 2016;
Published: 14 June 2016.
Edited by:
René T. Proyer, Martin-Luther University Halle-Wittenberg, GermanyReviewed by:
Joshua Fredrick Wiley, Australian Catholic University, AustraliaChristine Hohensinn, University of Vienna, Austria
Copyright © 2016 Fenollar-Cortés and Fuentes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Javier Fenollar-Cortés, javier.fenollar@um.es