 María-Teresa Cortés-Tomás1*
María-Teresa Cortés-Tomás1* José-Antonio Giménez-Costa1
José-Antonio Giménez-Costa1 Patricia Motos-Sellés1
Patricia Motos-Sellés1 María-Dolores Sancerni-Beitia2
María-Dolores Sancerni-Beitia2- 1Department of Basic Psychology, Faculty of Psychology, University of Valencia, Valencia, Spain
- 2Department of Methodology of the Behavioural Sciences, Faculty of Psychology, University of Valencia, Valencia, Spain
This study analyzes the appropriateness of an improved version of one of the most frequently used instruments for the screening of high-risk alcohol consumption. This adaptation was created in accordance with certain limitations recognized by other researchers and in an attempt to adjust the content and scales of some items to a more consensual definition of binge drinking. After revising items 2 and 3, the areas under the ROC curves of the AUDIT and of different abbreviated versions were calculated. A total of 906 minors (468 females) between the ages of 15 and 17 were evaluated. Stratified sampling was conducted on a population of high school students in the city of Valencia (Spain). One school was randomly chosen from each of the city’s 16 school districts. Information was collected on sociodemographic aspects, consumption patterns and the AUDIT containing the improved items. The percentage of underage BD reached 36%, regardless of gender or age. BD groups have been differentiated by different intensity levels, both in males and females. Upon comparing the effectiveness of the distinct versions of the AUDIT, it is recommended that researchers and clinics use the combination of the revised items 2 and 3 to ensure a more precise identification of underage BD. A cut-off point of 5 for this test would permit identification of 94% of the underage BD and would notably reduce false positives.
Introduction
One of the most frequently used screening instruments for the identification of high-risk alcohol consumption in youth is the AUDIT and its abbreviated versions (Patton et al., 2014; Cortés et al., 2016; Hagman, 2016) which was designed to identify persons with hazardous and harmful patterns of alcohol consumption (Babor et al., 2001). Specifically, research on the young brain refers mainly to these tools to compile consumption data and classify youth as either binge drinking (BD) or no binge drinking (non-BD) (Mota et al., 2013; López-Caneda et al., 2014a,b). Other studies have used the AUDIT score for correlation with structural and functional aspects of certain brain areas (Wahlstrom et al., 2012; Howell et al., 2013; Smith and Mattick, 2013; Kvamme et al., 2015).
Of the three dimensions included in the AUDIT (quantity-frequency, symptoms of dependency, and consequences of consumption), the first of these dimensions is the most frequently used to determine consumption in youth (Chung et al., 2002; Thomas and McCambridge, 2008; Seguel et al., 2013). The three items making up this first dimension, AUDIT-C, obtain higher sensitivity and specificity values in the detection of high-risk consumption as compared to the overall scale (DeMartini and Carey, 2012; Barry et al., 2015; Cortés et al., 2016; García et al., 2016).
These results support the conclusions obtained in the revision conducted by Clark and Moss (2010) with regards to the abbreviated AUDIT versions appearing to be more useful for youth, even when limited to item 3. This item, used to classify underage BD, has revealed psychometric properties that are similar to those of the AUDIT-C (Bowring et al., 2013; Blank et al., 2015; Paiva et al., 2015).
Despite the fact that they are very frequently used instruments, limitations have been suggested with regards to their efficiency in identifying BD. On the one hand, reference has been made to the measurement scales used for the different items. Letourneau et al. (2017) warned that in item 3, a drinker who engaged in three BD days per week (e.g., Friday through Sunday) is forced to describe their drinking as either “weekly” or “daily or almost daily” on the AUDIT-C, even though said drinking took place only three times a week. For Question 2, the numerical amount for any respondent who reports consuming 10 or more drinks on a typical day, whether it is 12, 15, or 30 drinks, will be coded as 10.
On the other hand, in an attempt to better identify underage BD, an effort has been made to more precisely specify the cut-off points of the scales. In this regard, no consensus has been reached either, and there is still a very wide range for the AUDIT, varying between 2 and 10 points (Knight et al., 2003; Kelly et al., 2004; Clark and Moss, 2010). For minors, the most frequently used cut-off point is 4 (Chung et al., 2002; Santis et al., 2009; Cortés et al., 2016) and 3 in the AUDIT-C (Chung et al., 2002; Cortés et al., 2016).
Furthermore, some researchers have tried out new combinations of items in order to better predict the pattern of underage consumption. Again, in this case, consensus has yet to be reached. McCambridge and Thomas (2009) allude to the fact that the best combination would consist of items 3, 5, and 8. Bowring et al. (2013) suggest that the best combination is 3, 4, 8, and 9. More recently, Blank et al. (2015) referred to separately using items 2 and 3, increasing the number of response options to obtain more precise information on the consumption pattern. In this way, sensitivity and specificity of the items are improved until reaching 0.8 and 0.7, respectively. Furthermore, some studies have noted the low correlation of item 1 with the total of the scale (Gmel et al., 2001; McCambridge and Thomas, 2009), recommending its elimination.
All of this disagreement has led to an interest in making improvements in the wording of the consumption items (AUDIT-C) given that these are the most explanatory of the youth consumption pattern. Included in the suggested changes is the modification of item 3, reducing the number of drinks (five or more on one consumption occasion -Kokotailo et al., 2004-; four or more drinks for women and five or more drinks for men -Olthuis et al., 2011-); or transforming the number of drinks to standard drinking units (SDUs), according to the country of origin (García et al., 2016). Other proposals have narrowed the time limit to “one single consumption occasion” in item 2 (García et al., 2016), although it has also been suggested that grams of alcohol should be used instead of number of drinks to evaluate the quantity ingested for this item (Gmel et al., 2001).
None of the suggested improvements has been overwhelmingly accepted by researchers, perhaps because they do not comply with a consensual definition of BD. Recent revisions of the operationalization of this consumption pattern (Courtney and Polich, 2009; Parada et al., 2011; Cortés and Motos, 2016) coincide in identifying the National Institute on Alcohol Abuse, and Alcoholism [NIAAA] (2004) definition as being the most well-adjusted, although limiting it to consumption engaged in over the past 6 months – given that it is intermittent behavior- and adapting it to the SDU value of each country. In the case of Spain, BD is identified as the consumption, during a 2 h interval, of six or more SDUs for women and seven or more for men, at least once over the past 6 months. Furthermore, it is important to note that this definition only establishes a limit for a very heterogeneous group of consumers; therefore it is necessary to differentiate the most homogenous subgroups possible.
In this work, we have modified the content of the consumption items included in the AUDIT-C, adapting them both in terms of wording as well as in their measurement scales, to the proposed consensual definition of BD. This shall permit the identification of which of these items best classifies heavy youth drinkers, and therefore, shall optimize the selection of BD sample participants, thereby improving the precision of the obtained results.
Materials and Methods
Participants
Nine hundred and six participants, 468 women and 438 men, took part in the study. Their ages ranged from 15 to 17, with mean age M = 15.99 years, SD = 0.8 years. All of the participants were high school students. Table 1 shows the distribution of the participants based on gender, age and whether or not they engage in BD. Overall, 36.1% of these adolescents (n = 327) engaged in BD, 52.9% (n = 173) were female and 47.1% (n = 154) were male. Differences were not found based on gender [F(1,904) = 0.191; p = 0.612], or age [F(1,904) = 3.929; p = 0.54].
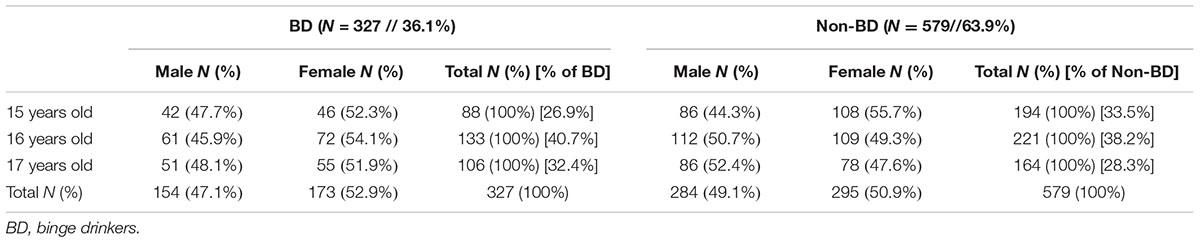
TABLE 1. Demographic characteristics of sample.
Procedure
Stratified sampling was carried out on a population of mandatory secondary school (grades 7–10), upper secondary (grades 11–12), and vocational training students in the city of Valencia (Spain). One school was randomly chosen from each of the 16 school districts in the city. Questionnaires were administered in classrooms during the school day. In all cases, participation was voluntary and anonymous.
A self-report diary was used, in which, for each day of the week, participants were to indicate the type and number of drinks consumed and the approximate time when the drinking took place. Each use was converted to grams of alcohol, based on the Spanish SDU (1 hard liquor = 20 g; 1 beer/wine = 10 g) (Rodríguez-Martos et al., 1999). This value was multiplied by the number of glasses of each type of alcoholic beverage that were consumed.
Based on the SDUs consumed and the number of hours in which this consumption took place, participants were classified as BD or non-BD. In all cases, there was compliance with the consumption proportion of seven or more SDUs in a 2 h interval for males and the consumption of six or more SDUs during the same time interval for females (National Institute on Alcohol Abuse, and Alcoholism [NIAAA], 2004).
Participants also filled out the 10 AUDIT items (Spanish version validated by Contel Guillamon et al., 1999). Three variables were extracted from this instrument: the sum of the 10 items (AUDIT), the sum of the first three items (AUDIT-C), and the score on the third question (AUDIT-3). In this study, the internal consistency of the AUDIT and the AUDIT-C was 0.74 and 0.83, respectively.
Next, the consensual definition of BD was used to improve item 3. It was worded as follows: During the past 6 months, what is the average number of days per month with BD consumptions (seven or more Spanish SDUs for males and six or more SDUs for females over a 2 h period)? The response scale was adapted based on the results obtained in prior studies conducted with minors and university students (Patrick et al., 2013; Cortés et al., 2016; Hagman, 2016). Following the revision of consumption quantity and frequency, it is considered more representative to use response alternatives that qualify normal situations, such as that some youth have engaged in BD once over the past 6 months, hence alternative 1 which considers this behavior to be sporadic and different from that of the other alternatives. The measurement scale definitively consists of the following: (0) Never; (1) Sporadically -less than once a month-; (2) between 1 and 4 times; (3) between 5 and 8 times; (4) between 9 and 12 times; (5) 13 or more times.
The wording of item 2 was also improved, changing number of drinks for number of Spanish SDUs consumed in 1 day. Finally, it is worded as follows: How many SDUs do you tend to have on a day when you drink alcohol? And maintaining its original response scale (0) 1 or 2; (1) 3 or 4; (2) 5 or 6; (3) 7 to 9; and (4) 10 or more.
Then, based on self-reports, these two new variables were generated. Later the value of the AUDIT-CR was calculated (A1+A2revised+A3revised), and the usefulness of the A3revised item was assessed. Finally, considering the recommendations from some prior studies, the A2revised+A3revised variable was also calculated.
Statistical Analyses
Four cluster analyses were also conducted with the BD and non-BD youth, based on the values of number of grams consumed in a BD session and number of hours of consumption for females and for males. In all cases, the extraction procedure consisted of two phases, which led to a natural classification of the subjects into different groups.
An analysis of variance (ANOVA) was performed, with its corresponding a posteriori tests, using the eight groups obtained in the clusters as independent variables (IVs) to determine whether there were differences in the grams consumed and the number of hours.
The area under the ROC (Receiver Operating Characteristic) curve was calculated using the method proposed by Hanley and McNeil (1983), which provides a graphic representation of a classifier’s performance.
To determine the optimal AUDIT cut-off score, our goal was to minimize false negatives and thus improve, as much as possible, the detection of youth engaging in this activity. Therefore, cut-off scores that maximized sensitivity were used. This methodology is based on prior studies (Cortés et al., 2016; Cortés Tomás et al., 2017). In the absence of a gold standard, Zweig and Campbell (1993) suggest using a consensus or majority expert opinion. As described in the introduction, the gold standard used in this study was consumption during a 2 h interval of ≥6 SDUs for women and ≥7 SDUs for men at least once over the past 6 months.
It is possible to compare the discriminatory capacity of the different versions of this screening tool based on their respective ROC curves, given that they were measured simultaneously, were applied to the same subjects and were contrasted with the same consensual definition of the revisions of BD operationalization.
Results
The cluster analysis among BD females produced two differentiated groups (BD1F/BD2F) (Table 2). In the case of the BD males, two groups were produced (BD1M/BD2M). Of the non-BD, two female (NONBD1F/NONBD2F) and two male (NONBD1M/NONBD2M) groups were produced.
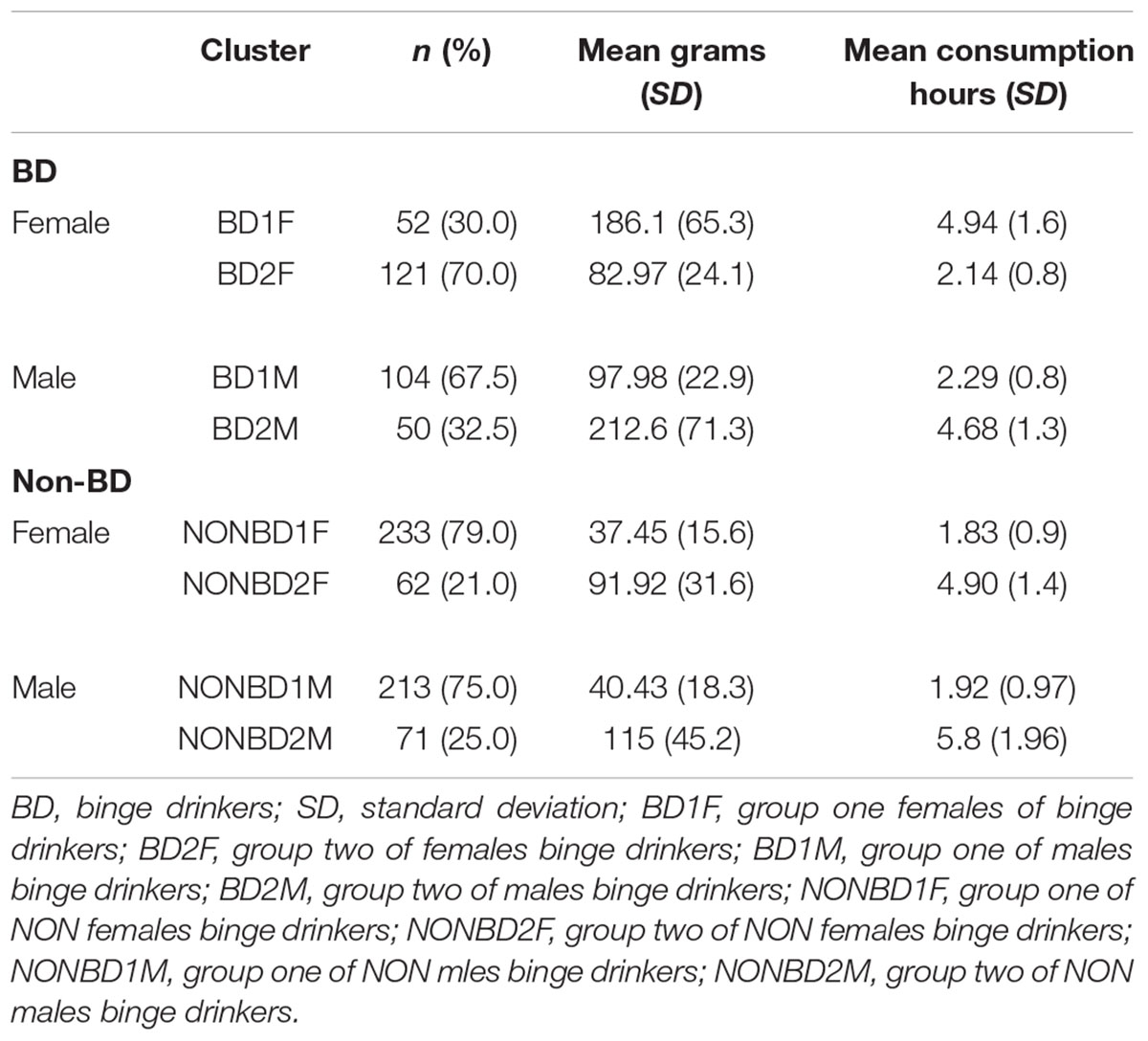
TABLE 2. Binge drinking (BD) and non-binge drinking (non-BD) groups differentiated by sex resulting from the clusters analyses.
The ANOVA performed among the eight groups (four BD and four non-BD) indicated that there were significant differences in the number of grams consumed [F(7,898) = 326.905; p < 0.0001] and in the number of consumption hours [F(7,898) = 203.304; p < 0.0001].
Upon comparison of the four BD groups (Table 3), it was found that the subgroups consuming the larger number of grams (BD1F and BD2M) took twice the amount of time in drinking this quantity. Furthermore, both are similar in terms of quantity consumed, as well as in time spent drinking.
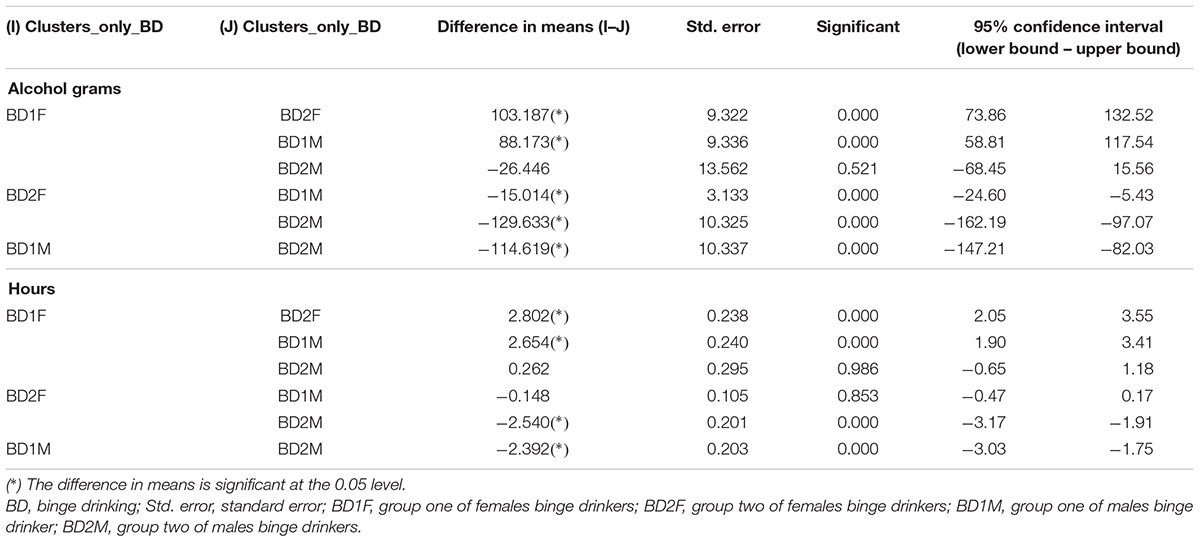
TABLE 3. A posteriori Games-Howell test.
Of the non-BD females, it is noteworthy that the NONBD2F group consumes a similar quantity of grams as the BD2F and BD1M groups, but it does so over a much longer time period, equivalent to that of groups BD1F and BD2M.
As for the non-BD males, the NONBD2M group is similar to BD1F in terms of quantity of grams consumed but it takes a greater number of hours to do so, therefore this is not considered BD.
When considering all of the interviewees, differentiated according to the eight resulting groups of the BD/non-BD clusters, the three classic versions of the AUDIT yielded lower values in the area under the ROC curve as compared to the results obtained for the modified versions of this instrument (Table 4). This area ranges from 0.741 in the case of the AUDIT to 0.801 in the case of the AUDIT-C.
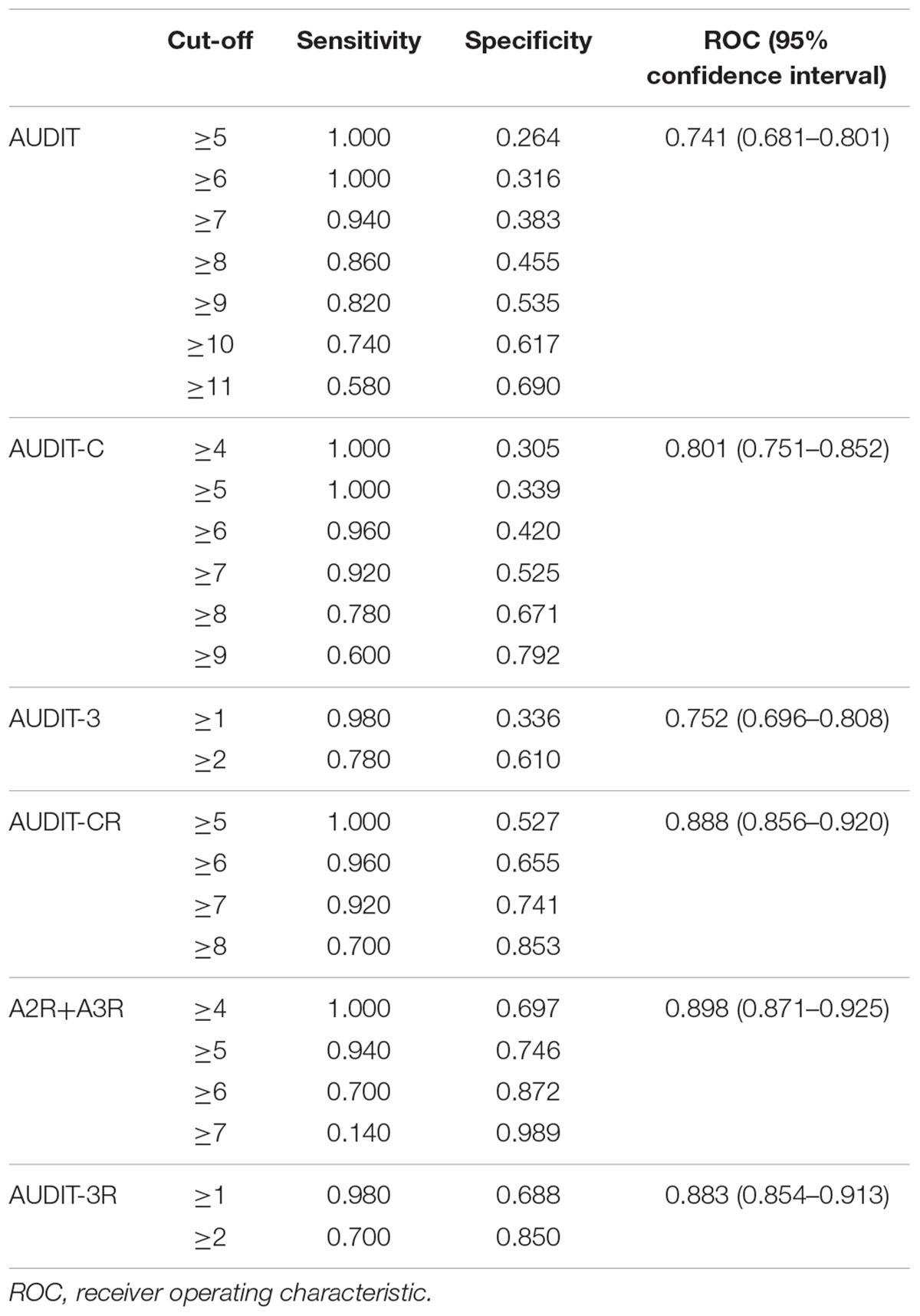
TABLE 4. Performance of the three versions of the AUDIT in detecting binge drinking for the entire sample.
The adjustment of the AUDIT questions to the definition of what is considered BD allows for the significant increase in the area under the ROC curve. Both when considering the AUDIT-CR, which includes the revision of the two items as well as when considering the A3R, the ROC area reaches 0.88.
But the most parsimonious combination that also permits a slight increase in the explained area is the one that includes the sum of the A2R and A3R (Figure 1).
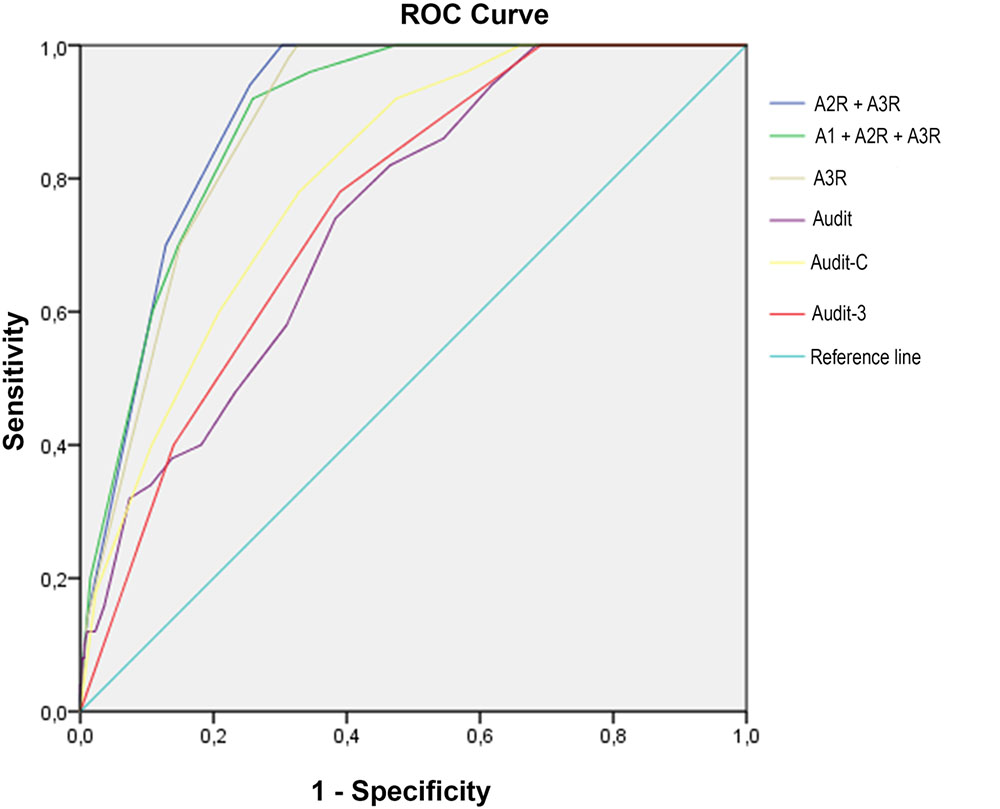
FIGURE 1. Receiver operating characteristic (ROC) curves for all AUDIT versions to detect BD.
Using the score of 5 on the A2R+A3R, 94% of the BD young people were detected (sensitivity) and 75% of the non-BD (specificity). When the cut-off score was established at 4, the sensitivity increased slightly, but the specificity was much worse.
Discussion
This study analyzes the appropriateness of an improved version of the AUDIT. The adaptation has been carried out based on the limitations recognized by other researchers (McCambridge and Thomas, 2009; Olthuis et al., 2011; Bowring et al., 2013; Blank et al., 2015; Cortés et al., 2016; García et al., 2016; Letourneau et al., 2017) and by attempting to adjust the content and the scales of some items to a more consensual definition of BD.
Within the group of heavy drinkers, the underage population warrants special attention due to the potential repercussions on its bio-psycho-social development and maturity (Squeglia et al., 2011; Pascual et al., 2014). In Spain, 4 out of every 10 minors have access to this substance which is not legally authorized until the age of 18, eventually engaging in BD (Observatorio Español sobre Drogas [OED], 2016). This same percentage has been observed in the population of youth evaluated in this study.
Furthermore, the presence of females of this age is also evident, confirming the trend that has been warned of in prior national epidemiological surveys (Observatorio Español sobre Drogas [OED], 2016) that found a similar number of males and females engaging in intense alcohol consumption.
Our findings provide further insight into the understanding of the existence of different subgroups within the BD collective, both males and females, based on the seriousness of their behavior -a greater quantity of alcohol consumed, for more hours and at a greater frequency-. In addition, it should not be forgotten that among the BD groups that consume the most, both males and females drink similar amounts of alcohol and they do so in the same number of hours. This leads to a clearly greater risk for females, given that they are more vulnerable to the consequences of alcohol consumption. Furthermore, this result quantifies results of previous research (Valencia-Martín et al., 2007; Pilatti et al., 2013) claiming that there is a higher level of consumption by BD males, limiting it only to the subgroups that consume less.
The healthcare and social implications that are generated in the BD minors would be reduced if it were possible to detect and intervene in this behavior as early as possible. This suggests the need for sufficiently powerful screening measures to identify this consumption pattern with the least possible error. This would offer improvements not only in the clinical and prevention areas but also in the area of research (Foxcroft et al., 2015; Walton et al., 2015; Arnaud et al., 2016) given that a more adjusted classification of the subjects would permit greater precision in the obtained results.
As found in the literature that was consulted (DeMartini and Carey, 2012; Barry et al., 2015; Cortés et al., 2016; García et al., 2016), of all of the AUDIT versions used, the AUDIT-C is the version that classifies adolescents by improving the correct identification of the non-BD, compared to the AUDIT. However, upon transforming the items, adjusting them through both wording and in response scale to the most widely accepted BD definition, the adjustment of identification of this consumption pattern is increased.
Upon comparing the three versions of the revised AUDIT -AUDITCR/A3r/A2r+A3r- the last combination stands out (A2r+A3r) given that it identifies the greatest number of BDs and reduces the number of false positives. It may be stated that the recommendations of Blank et al. (2015) to focus on items 2 and 3, as well as those of Gmel et al. (2001) and McCambridge and Thomas (2009) to ignore item 1, contribute to an improved classification of BD. In addition to this, if we add improvement in the wording of the items and their response scales, adjusting them to the operational definition of BD, a greater area is obtained under the ROC curve. This suggests that this is a test with the greatest discriminatory capacity of all evaluated in this study. Having an instrument with an area under the ROC curve of 0.898 means that there is an 89.8% probability that, when considering two randomly selected minors, one BD and the other non-BD, the test will correctly classify them.
The reliability obtained through this new combination of items is very similar to that of the complete original scale -0.74, qualified as an acceptable reliability coefficient-. This result is not surprising, given that the items have been reformulated in order to note different aspects of BD. Item 2 reveals a more than intense consumption, as it is conducted over one entire day, whereas item 3 notes the frequency with which BD is engaged in. The combination of both not only informs of having reached a limit in BD in the form of overconsumption, but also if the youth drinks in a manner that extends over a longer period of time.
Conclusion
Despite the fact that the AUDIT and its abbreviated versions appear to be appropriate tools to screen adolescents who are engaging in this behavior, the identification of heavy drinkers is improved by using a more parsimonious combination of two items. Even in those cases in which researchers recur to item 3 in order to classify BD/non-BD (Bowring et al., 2013; Mota et al., 2013; López-Caneda et al., 2014b; Blank et al., 2015) it would be more appropriate, given the notable improvement in discrimination of this test, to recur to the revised item 3.
In fact, it is recommended that researchers and clinics use the combination of the two items (A2r+A3r) proposed in this work for a more precise identification of BD minors. Specifically, starting from a cut-off point of 5, it may be possible to identify 94% of the underage BD. The sensitivity and specificity values attained are three points higher than those achieved using the three-item combination proposed by McCambridge and Thomas (2009), but using one less item, facilitating its applicability.
Our study may be limited in that it relies on self-reporting. This method of data collection has been questioned in adult samples, given that it may present an underestimation of consumption (Smith et al., 1990). However, in adolescent populations, self-reports have been found to be reliable and valid when conducted in a confidential manner, compared with other survey protocols (e.g., household survey) (Winters et al., 1990; Knight et al., 2003) in which youth perceived they were at great risk of being identified (Fowler and Stingfellow, 2001; Degenhardt et al., 2013).
According to the recommendations made by Santis et al. (2009), additional research is necessary in order to generalize these results to other geographic areas.
Ethics Statement
It was not necessary for the study because there was no ethics relevant problems. People just filled out questionnaires/tests, afterward they got feedback on their scores. No manipulation or violation was done. The study was undertaken in compliance with Spanish legislation (approved by the Department of Education) and the code of ethics for research involving human subjects outlined by the University of Valencia Human Research Ethics Committee. The adolescents and their legal representatives signed an informed consent form.
Author Contributions
M-TC-T and J-AG-C conceived of the study and collected the data. M-TC-T and M-DS-B analyzed the data. M-TC-T, PM-S, and J-AG-C wrote the paper. M-TC-T, J-AG-C, PM-S, and M-DS-B approved the final version to be published.
Funding
Funding for this study was provided by Plan Nacional sobre Drogas (PND2008-056). PNSD had no further role in study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Arnaud, N., Baldus, C., Elgán, T. H., De Paepe, N., Tønnesen, H., Csémy, L., et al. (2016). Effectiveness of a web-based screening and fully automated brief motivational intervention for adolescent substance use: a randomized controlled trial. J. Med. Internet. Res. 18:e103. doi: 10.2196/jmir.4643
Babor, T., Higgins-Biddle, J. C., Saunders, J. B., and Monteiro, M. G. (2001). The Alcohol Use Disorders Identification Test. Guidelines for Use in Primary Care, 2nd Edn. Geneva: World Health Organization.
Barry, A. E., Chaney, B. H., Stellefson, M. L., and Dodd, V. (2015). Evaluating the psychometric properties of the AUDIT-C among college students. J. Subst. Use 20, 1–5. doi: 10.3109/14659891.2013.856479
Blank, M. L., Connor, J., Gray, A., and Tustin, K. (2015). Screening for hazardous alcohol use among university students using individual questions from the Alcohol Use Disorders Identification Test-Consumption. Drug Alcohol Rev. 34, 540–548. doi: 10.1111/dar.12272
Bowring, A. L., Gouillou, M., Hellard, M., and Dietze, P. (2013). Comparing short versions of the AUDIT in a community-based survey of young people. BMC Public Health 13:301. doi: 10.1186/1471-2458-13-301
Chung, T., Colby, S. M., Barnett, N. P., and Monti, P. M. (2002). Alcohol use disorders identification test: factor structure in an adolescent emergency department sample. Alcohol. Clin. Exp. Res. 26, 223–231. doi: 10.1111/j.1530-0277.2002.tb02528.x
Clark, D. B., and Moss, H. B. (2010). Providing alcohol-related screening and brief interventions to adolescents through health care systems: obstacles and solutions. PLoS Med. 7:e1000214. doi: 10.1371/journal.pmed.1000214
Contel Guillamon, M., Gual Solé, A., and Colom Farran, J. (1999). Test para la identificación de trastornos por uso de alcohol (AUDIT): traducción y validación del AUDIT al catalán y castellano. Adicciones 11, 337–347. doi: 10.20882/adicciones.613
Cortés, M. T., Giménez, J. A., Motos, P., and Sancerni, M. D. (2016). Different versions of the alcohol use disorders identification test (AUDIT) as screening instruments for underage binge drinking. Drug Alcohol Depend. 158, 52–59. doi: 10.1016/j.drugalcdep.2015.10.033
Cortés, M. T., and Motos, P. (2016). “Cómo definir y medir el consumo intensivo de alcohol,” in Guía Clínica. Consumo Intensivo de Alcohol en Jóvenes, ed. M. T. Cortés (Barcelona: Socidrogalcohol), 25–46.
Cortés Tomás, M. T., Giménez-Costa, J. A., Motos-Sellés, P., Sancerni-Beitia, M. D., and Cadaveira Mahía, F. (2017). The utility of the alcohol use disorders identification test (AUDIT)for the analysis of binge drinking in university students. Psicothema 29, 229–235. doi: 10.7334/psicothema2016.271
Courtney, K. E., and Polich, J. (2009). Binge drinking in young adults: data, definitions, and determinants. Psychol. Bull. 135, 142–156. doi: 10.1037/a0014414
Degenhardt, L., O’Loughlin, C., Swift, W., Romaniuk, J. C., Coffey, C., Hall, W., et al. (2013). The persistence of adolescent binge drinking into adulthood: findings from a 15-year prospective cohort study. BMJ Open 3, 1–11. doi: 10.1136/bmjopen-2013-003015
DeMartini, K. S., and Carey, K. B. (2012). Optimizing the use of the AUDIT for alcohol screening in college students. Psychol. Assess. 24, 954. doi: 10.1037/a0028519
Fowler, F. J., and Stingfellow, V. L. (2001). Learning from experience: estimating teen use of alcohol, cigarettes, and marijuana from three survey protocols. J. Drug Issues 31, 643–664. doi: 10.1177/002204260103100304
Foxcroft, D. R., Smith, L. A., Thomas, H., and Howcutt, S. (2015). Accuracy of alcohol use disorders identification test for detecting problem drinking in 18–35 year-olds in England: method comparison study. Alcohol Alcohol. 50, 244–250. doi: 10.1093/alcalc/agu095
García, M. A., Novalbos, J. P., Martínez, J. M., and O’Ferrall, C. (2016). Validation of the alcohol use disorders identification test in university students: AUDIT and AUDIT-C. Adicciones 28, 194–204. doi: 10.20882/adicciones.775
Gmel, G., Heeb, J. L., and Rehm, J. (2001). Is frequency of drinking an indicator of problem drinking? A psychometric analysis of a modified version of the alcohol use disorders identification test in Switzerland. Drug Alcohol Depend. 64, 151–163. doi: 10.1016/S0376-8716(01)00117-X
Hagman, B. T. (2016). Performance of the AUDIT in detecting DSM-5 alcohol use disorders in college students. Subst. Use Misuse 51, 1521–1528. doi: 10.1080/10826084.2016.1188949
Hanley, J. A., and McNeil, B. J. (1983). A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 148, 839–843. doi: 10.1148/radiology.148.3.6878708
Howell, N. A., Worbe, Y., Lange, I., Tait, R., Irvine, M., Banca, P., et al. (2013). Increased ventral striatal volume in college-aged binge drinkers. PLoS ONE 8:e74164. doi: 10.1371/journal.pone.0074164
Kelly, T. M., Donovan, J. E., Chung, T., Cook, R. L., and Delbridge, T. R. (2004). Alcohol use disorders among emergency department–treated older adolescents: a new brief screen (RUFT-Cut) using the AUDIT, CAGE, CRAFFT, and RAPS-QF. Alcohol. Clin. Exp. Res. 28, 746–753. doi: 10.1097/01.ALC.0000125346.37075.85
Knight, J. R., Sherritt, L., Harris, S. K., Gates, E. C., and Chang, G. (2003). Validity of brief alcohol screening tests among adolescents: a comparison of the AUDIT, POSIT, CAGE, and CRAFFT. Alcohol. Clin. Exp. Res. 27, 67–73. doi: 10.1111/j.1530-0277.2003.tb02723.x
Kokotailo, P. K., Egan, J., Gangnon, R., Brown, D., Mundt, M., and Fleming, M. (2004). Validity of the alcohol use disorders identification test in college students. Alcohol. Clin. Exp. Res. 28, 914–920. doi: 10.1097/01.ALC.0000128239.87611.F5
Kvamme, T. L., Schmidt, C., Strelchuk, D., Chang-Webb, Y. C., Baek, K., and Voon, V. (2015). Sexually dimorphic brain volume interaction in college-aged binge drinkers. Neuroimage Clin. 10, 310–317. doi: 10.1016/j.nicl.2015.12.004
Letourneau, E. J., McCart, M. R., Sheidow, A. J., and Mauro, P. M. (2017). First evaluation of a contingency management intervention addressing adolescent substance use and sexual risk behaviors: risk reduction therapy for adolescents. J. Subst. Abuse Treat. 72, 56–65. doi: 10.1016/j.jsat.2016.08.019
López-Caneda, E., Holguín, S. R., Cadaveira, F., Corral, M., and Doallo, S. (2014a). Impact of alcohol use on inhibitory control (and viceversa) during adolescence and young adulthood: a review. Alcohol Alcohol. 49, 173–181. doi: 10.1093/alcalc/agt168
López-Caneda, E., Holguín, S. R., Corral, M., Doallo, S., and Cadaveira, F. (2014b). Evolution of the binge drinking pattern in college students: neurophysiological correlates. Alcohol 48, 407–418. doi: 10.1016/j.alcohol.2014.01.009
McCambridge, J., and Thomas, B. A. (2009). Short forms of the AUDIT in a web-based study of young drinkers. Drug Alcohol Rev. 28, 18–24. doi: 10.1111/j.1465-3362.2008.00010.x
Mota, N., Parada, M., Crego, A., Doallo, S., Caamaño-Isorna, F., Holguín, S. R., et al. (2013). Binge drinking trajectory and neuropsychological functioning among university students: a longitudinal study. Drug Alcohol Depend. 133, 108–114. doi: 10.1016/j.drugalcdep.2013.05.024
National Institute on Alcohol Abuse, and Alcoholism [NIAAA] (2004). Council Approves Definition of Binge Drinking. Bethesda, MA: NIAAA.
Observatorio Español sobre Drogas [OED] (2016). Informe 2016: Delegación del Gobierno para el Plan Nacional sobre Drogas. Madrid: Ministerio de Sanidad y Política Social (PNSD).
Olthuis, J. V., Zamboanga, B. L., Martens, M. P., and Ham, L. S. (2011). Social influences, alcohol expectancies, and hazardous alcohol use among college athletes. J. Clin. Sport Psychol. 5, 24–43. doi: 10.1123/jcsp.5.1.24
Paiva, P. C. P., Paiva, H. N. D., Lamounier, J. A., Ferreira, E. F., César, C. A. S., and Zarzar, P. M. (2015). Binge drinking among 12-year-old adolescent schoolchildren and its association with sex, socioeconomic factors and alcohol consumption by best friends and family members. Cien. Saude Colet. 20, 3427–3435. doi: 10.1590/1413-812320152011.18792014
Parada, M., Corral, M., Caamaño-Isorna, F., Mota, N., Crego, A., Holguín, S. R., et al. (2011). Definición del concepto de consumo intensivo de alcohol adolescente (binge drinking). Adicciones 23, 53–63. doi: 10.20882/adicciones.167
Pascual, M., Pla, A., Miñarro, J., and Guerri, C. (2014). Neuroimmune activation and myelin changes in adolescent rats exposed to high-dose alcohol and associated cognitive dysfunction: a review with reference to human adolescent drinking. Alcohol Alcohol. 49, 187–192. doi: 10.1093/alcalc/agt164
Patrick, M. E., Schulenberg, J. E., Martz, M. E., Maggs, J. L., O’Malley, P. M., and Johnston, L. D. (2013). Extreme binge drinking among 12th-grade students in the United States: prevalence and predictors. JAMA Pediatr. 167, 1019–1025. doi: 10.1001/jamapediatrics.2013.2392
Patton, R., Deluca, P., Kaner, E., Newbury-Birch, D., Phillips, T., and Drummond, C. (2014). Alcohol screening and brief intervention for adolescents: the how, what and where of reducing alcohol consumption and related harm among young people. Alcohol Alcohol. 49, 207–212. doi: 10.1093/alcalc/agt165
Pilatti, A., Caneto, F., Garimaldi, J. A., Del Valle, B., and Pautassi, R. M. (2013). Contribution of time of drinking onset and family history of alcohol problems in alcohol and drug use behaviors in argentinean college students. Alcohol Alcohol. 49, 128–137. doi: 10.1093/alcalc/agt176
Rodríguez-Martos, A., Gual Solé, A., and Llopis Llácer, J. J. (1999). The “standard drink unit” as a simplified recording system of alcohol consumption and its measurement in Spain. Med. Clin. 112, 446–450.
Santis, R., Garmendia, M. L., Acuña, G., Alvarado, M. E., and Arteaga, O. (2009). The alcohol use disorders identification test (AUDIT) as a screening instrument for adolescents. Drug Alcohol Depend. 103, 155–158. doi: 10.1016/j.drugalcdep.2009.01.017
Seguel, F., Santander, G., and Alexandre, O. (2013). Validez y confiabilidad del test de identificación de los trastornos debidos al consumo de alcohol (AUDIT) en estudiantes de una universidad chilena. Cienc. Enferm. 19, 23–35. doi: 10.4067/S0717-95532013000100003
Smith, J. L., and Mattick, R. P. (2013). Evidence of deficits in behavioural inhibition and performance monitoring in young female heavy drinkers. Drug Alcohol Depend. 133, 398–404. doi: 10.1016/j.drugalcdep.2013.06.020
Smith, P. F., Remington, P. L., Williamson, D. F., and Anda, R. F. (1990). A comparison of alcohol sales data with survey data on self-reported alcohol use in 21 states. Am. J. Public Health 80, 309–312. doi: 10.2105/AJPH.80.3.309
Squeglia, L. M., Schweinsburg, A. D., Pulido, C., and Tapert, S. F. (2011). Adolescent binge drinking linked to abnormal spatial working memory brain activation: differential gender effects. Alcohol. Clin. Exp. Res. 35, 1831–1841. doi: 10.1111/j.1530-0277.2011.01527.x
Thomas, B. A., and McCambridge, J. (2008). Comparative psychometric study of a range of hazardous drinking measures administered online in a youth population. Drug Alcohol Depend. 96, 121–127. doi: 10.1016/j.drugalcdep.2008.02.010
Valencia-Martín, J. L., Galán, I., and Rodríguez-Artalejo, F. (2007). Binge drinking in Madrid, Spain. Alcohol. Clin. Exp. Res. 31, 1723–1730. doi: 10.1111/j.1530-0277.2007.00473.x
Wahlstrom, L. C., McChargue, D. E., and Mackillop, J. (2012). DRD2/ANKK1 TaqI A genotype moderates the relationship between alexithymia and the relative value of alcohol among male college binge drinkers. Pharmacol. Biochem. Behav. 102, 471–476. doi: 10.1016/j.pbb.2012.06.012
Walton, M. A., Chermack, S. T., Blow, F. C., Ehrlich, P. F., Barry, K. L., Booth, B. M., et al. (2015). Components of brief alcohol interventions for youth in the emergency department. Subst. Abus. 36, 339–349. doi: 10.1080/08897077.2014.958607
Winters, K. C., Stinchfield, R. D., Henly, G. A., and Schwartz, R. H. (1990). Validity of adolescent self-report of alcohol and other drug involvement. Subst. Use Misuse 25, 1379–1395. doi: 10.3109/10826089009068469
Keywords: binge drinking, underage, AUDIT, alcohol screening, ROC
Citation: Cortés-Tomás M-T, Giménez-Costa J-A, Motos-Sellés P and Sancerni-Beitia M-D (2017) Revision of AUDIT Consumption Items to Improve the Screening of Youth Binge Drinking. Front. Psychol. 8:910. doi: 10.3389/fpsyg.2017.00910
Received: 27 March 2017; Accepted: 17 May 2017;
Published: 08 June 2017.
Edited by:
Eduardo López-Caneda, University of Minho, PortugalReviewed by:
Antoni Gual, Hospital Clinic of Barcelona, SpainMiguel Ángel García-Carretero, University of Cádiz, Spain
Copyright © 2017 Cortés-Tomás, Giménez-Costa, Motos-Sellés and Sancerni-Beitia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María-Teresa Cortés-Tomás, maria.t.cortes@uv.es