 Johanna C. Badcock
Johanna C. Badcock Hedwige Dehon
Hedwige Dehon Frank Larøi
Frank Larøi- 1Centre for Clinical Research in Neuropsychiatry, Division of Psychiatry, Faculty of Health and Medical Sciences, The University of Western Australia, Perth, WA, Australia
- 2Australia and Perth Voices Clinic, Murdoch University Child and Adult Psychology Service, Murdoch University, Murdoch, WA, Australia
- 3Psychology and Neuroscience of Cognition Research Unit, University of Liege, Liege, Belgium
- 4Department of Biological and Medical Psychology, University of Bergen, Bergen, Norway
- 5NORMENT – Norwegian Centre of Excellence for Mental Disorders Research, University of Oslo, Oslo, Norway
KEY POINTS
➢ Studies suggest a substantial minority of healthy older adults have hallucinatory experiences, in line with existing evidence on hallucinations in other age groups, though it is still unclear if hallucination prevalence increases or declines with age in older cohorts.
➢ Stigma attached to both hallucinations and ageing leads to considerable under-reporting of these experiences in healthy older adults and may negatively bias how professionals, family members, and the public respond.
➢ Why and when hallucinations in healthy older adults remit, persist, or progress to other clinical disorders remains poorly understood.
➢ Current evidence points to a range of factors associated with hallucinations in older adults including decline in sensory or cognitive functioning, poor sleep, and psychosocial stressors (e.g., social isolation, loneliness, and bereavement), highlighting the need for accurate assessment and tailored interventions.
Hallucinations, though common in youth and younger adults, are not the preserve of these age groups. Accumulating evidence shows that hallucinatory experiences are also present at surprisingly high rates in healthy older adults in the general community. Furthermore, stigma and misunderstanding of hallucinations, together with ageism, may lead to under-reporting of these experiences by older adults, and misdiagnosis or mismanagement by health and mental health practitioners. Consequently, improved public and professional knowledge is needed about the nature and significance of hallucinations with advancing age. The purpose of this review is to provide a comprehensive overview, and critical analysis, of research on the prevalence, psychosocial, and neurobiological factors associated with hallucinations in people aged 60 years and over. To the best of our knowledge, this is the first review of its kind in the literature. The evidence supports a dynamic conceptualization of hallucinations, in which the emergence of hallucinations is viewed as a balance between the sensory, cognitive, or social impairments accompanying advancing age and the degree to which compensatory processes elicited by these impairments are successful. We briefly summarize the implications of the literature for aged care services and interventions, and stress that far more studies are needed in this important field of research.
Introduction
The world's population is aging, with the number of adults aged 60 years and over expected to reach 2 billion by 2050 (United Nations, 2013). Furthermore, the average life span continues to increase. In Australia, for example, from 2002 to 2012 life expectancy increased from 78.1 to 79.9 years (for men) and from 83 to 84.3 years (for women) (Australian Bureau of Statistics, 2014). As a consequence, there is a growing focus on the physical and mental health needs of older adults to ensure that healthy ageing is possible. Hallucinatory experiences are particularly significant in this regard since they can indicate the presence of mental illness but are also known to occur in healthy individuals in the general population (Sommer et al., 2010; Johns et al., 2014; Kråkvik et al., 2015).
Hallucinations are hard to pin down, with a standard definition remaining elusive (David, 2004; Larøi et al., 2012). At the broadest level, hallucinations are characterized as the abnormal perception of something not present (see Table 1 for a glossary of terms); though the genesis of these experiences seems to be far more dynamic than previously realized. Thus, rather than being passive phenomena arising from deficits in cognitive-perceptual processes, this “positive” conceptualization of hallucinations maintains that a range of active, adaptive processes are involved as well, that compensate for such deficits. Since compensatory processes have been well-studied in the context of normal ageing (e.g., Reuter-Lorenz and Park, 2014; Peelle and Wingfield, 2016), hallucinatory experiences in healthy older adults may provide a particularly valuable window on the underlying mechanisms involved. Despite this, later-onset hallucinations have mostly been examined in the context of Lewy Body disorders and dementia (Collerton et al., 2012; El Haj et al., 2015). In contrast, the diversity and significance of hallucinations in healthy older adults have received much less attention (Tien, 1991). However, new epidemiological data indicate that nearly a quarter of first onsets of hallucinations occur after the age of 40 years (McGrath et al., 2016). Such findings suggest that hallucinatory experiences in later life (i.e., in the absence of mental disease or disorder) warrant considerably more attention. Against the backdrop of an aging population, they also emphasize the need for a greater understanding of the causes, correlates, and consequences of hallucinations in healthy older individuals in order to guide the planning and provision of aged-care services.
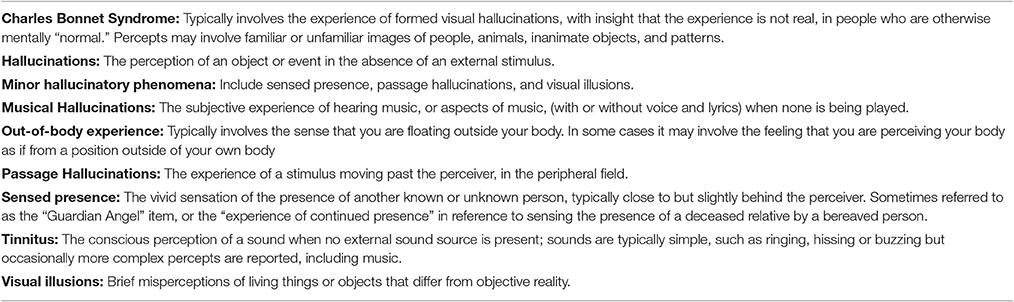
Table 1. Glossary of terms and definitions.
The purpose of this article is to provide the first synthesis and critique of the literature on hallucinations in healthy (non-clinical) older adults. We summarize research on the prevalence, psychosocial, and neurobiological factors associated with hallucinations in samples predominantly aged over 60 years. Where relevant, we highlight the similarities and differences in our findings with the literature on hallucinations in younger and/or clinical populations, and discuss implications for aged care services and intervention. Finally, we summarize the strengths and gaps in the evidence base and outline priorities for future research.
Methods
Methodological Difficulties and Search Process
Initial scoping of the literature revealed a number of difficulties in attempting to conduct a systematic review of all the evidence on hallucinations in healthy older adults. Hallucinations can occur at any age and studies do not always report results by age group. Limiting the search to studies of healthy samples only, missed many reports which focused on clinical groups/disorders but were then further divided into clinical and non-clinical categories. Restricting the search to current or recent evidence resulted in an under-representation of research in less popular, but significant, areas (such as bereavement), whilst limiting the search term to “hallucinations” missed studies with a focus on specific experiences such as tinnitus, Charles Bonnet Syndrome, or sensed presence. In view of the large variety of aims, methods, and perspectives in research on hallucinations in older adults we synthesized the literature into three major themes, presented below (prevalence and characteristics; stigma and distress; factors associated with hallucinations in older adults). In order to focus on hallucinations in healthy individuals, studies on abnormal perceptual experience in older adults with dementia, neurological disease (e.g., tumor, epilepsy, Parkinson's), delirium, or psychotic disorder were excluded. The review covers a wide spectrum of experiences, including complex, simple, and minor hallucinations (such as sensed presence and passage hallucinations) in any modality.
The Prevalence and Characteristics of Hallucinations in Older Adults
Very few studies have directly and specifically examined the prevalence (and other aspects) of hallucinations in the elderly, non-clinical population. Either studies simply do not include older age groups (e.g., older than 60 years), or they do, but combine all age groups into one or do not report specific prevalence rates for each age group. Nevertheless, in general, there seems to be a significant minority of this population that has these experiences—which is in line with recent conclusions regarding the experience of hallucinations in younger, non-clinical populations (Jardri et al., 2014; Johns et al., 2014). However, the documented prevalence rates of hallucinations in older adults vary between 0.4 and 37%. For example, Turvey et al. (2001) report 20%, Cole et al. (2002) report 2.5%, Lyketsos et al. (2000) report 0.6%, Larøi et al. (2005) report 37%, Geda et al. (2008) 0.4%, Okura et al. (2011) 2.2%, Kråkvik et al. (2015) 3.7%, and Subramaniam et al. (2016) 2.7%. A summary of important details regarding these studies (e.g., age of participants, particular characteristics of participants, how hallucinations were assessed, whether only hallucinations alone, or combined with other experiences, etc.) is provided in Supplementary Table 1, which have undoubtedly contributed to the variability of these estimates (see Pang, 2016 for variations in reported prevalence of Charles Bonnet Syndrome). Of these differences between studies, how hallucinations were assessed is most probably the most important characteristic that explains this large variability in prevalence rates and, in particular, which timeframe was adopted. For instance, the highest rate (37%) is reported in Larøi et al. (2005) where items from the LSHS were used—and where the timeframe is lifetime prevalence (e.g., “In the past, have you ever had the following experience?”). In contrast, the lowest prevalence rates are reported in studies (e.g., Lyketsos et al., 2000; Cole et al., 2002; Geda et al., 2008; Okura et al., 2011) where a 1-month timeframe (many of these studies use the NPI to assess hallucinations) is utilised (“Have you had the following experience in the past month?”) and thus large differences in prevalence rates are to be expected.
For those studies that included prevalence rates for specific age groups, the results seem to suggest that prevalence rates of hallucinations decrease with age, although this is not always the case. For example, drawing on a large national survey, Kråkvik et al. (2015) reported a decrease in prevalence from 14.6% (<30 years) to 2.8% (≥70 years) for auditory verbal hallucinations. Similarly, Ohayon (2000), reported a decrease in hypnagogic hallucinations, from 31.1% (15–44 years) to 15.5% (≥65 years) and for hypnopompic hallucinations, from 8.2 to 4.8%. In Soulas et al. (2016), prevalence rates of auditory hallucinations reported at interview in the age-group 60–69 years was 2.84%, 1.01% in 70–79 years, and 1.37% in ≥80. In the same study, prevalence rates of hallucinations in any modality was: 10.64% (60–69 years), 8.08% (70–79), and 8.22% (≥80). However, these differences across age groups were not statistically significant. In contrast, the prevalence of minor phenomena, such as sensed presence and passage hallucinations, increased with age in those aged 60 years and over (Soulas et al., 2016). Similarly, an age-dependent increase in the prevalence of tinnitus has been reported (Kim et al., 2015). This highlights the fact that the definition and/or type of hallucination, method of assessment and participants' personal and social characteristics, must be carefully considered when evaluating prevalence data (Larøi et al., 2005). Prevalence statistics are also complicated by variable rates of disclosure of hallucinations by older adults striving to avoid the negative stereotypes attached to these experiences, considered next.
Stigma and Distress
Studies on visual hallucinations in older adults often present qualitative evidence on the reluctance of participants to disclose their experiences for fear they are going “mad” or “demented” (self-stigma) and how they will be treated by others (public stigma) (Cox and ffytche, 2014; Pang, 2016). Similarly, studies examining post-bereavement hallucinations in older adults (a field discussed in more detail later in the article) have observed high rates of underreporting (e.g., with sometimes over 50% of people never disclosing their hallucinatory experiences to family, friends, or professionals). Of those who offered explanations why these experiences were not disclosed, participants mentioned for instance “fear to be ridiculed” (most common explanation), “too personal,” “people would not be interested,” “upset relatives if they knew,” “unlucky to talk about it” (Rees, 1971). Such beliefs may rest, in no small part, on routine portrayals of mental illness in the media (Owen, 2012). Stigma may also lead to under-reporting of hallucinatory voices in healthy adults (in all age groups), potentially preventing access to accurate information or social support and contributing to distress (Vilhauer, 2017). The addition of ageist stereotypes of cognitive incompetence (Cuddy et al., 2005; Barber, 2017) would be expected to exacerbate both self and public stigma of hallucinations in older people, but this issue has not yet been systematically explored.
Responses to hallucinatory experiences vary from person to person, and not all are found distressing. In fact, Rees (1971) reported that 68.6% of older people with post-bereavement hallucinations found the experience helpful. In general, however, compared to the literature on psychosis, fewer studies have explored the emotional reactions to hallucinations in healthy older individuals. Nonetheless, recent studies suggest that around 35% of people with Charles Bonnet Syndrome find their hallucinatory experiences distressing and are more persistent than previously thought (Cox and ffytche, 2014). Furthermore, around 10–20% of people with tinnitus report significant levels of distress, which appears to be largely independent of psychoacoustic factors and more closely related to perceived control over the experience (Wallhäusser-Franke et al., 2012). Perceived lack of control and distress typically cluster together in the experience of hallucinations in schizophrenia, suggesting shared etiological processes and the need for specific treatment (Woodward et al., 2014). A 5 year follow-up of non-psychotic adults (the majority by then aged 40–70 years) with frequent auditory verbal hallucinations, also found that distress arising from these experiences significantly predicted the need for care (Daalman et al., 2016)—a pattern that is common in younger adults with hallucinations (Johns et al., 2014). Whilst stigma may be partly responsible for the distress arising from hallucinatory experiences, a range of inter-related factors is likely to be involved. For example, Lai et al. (2016), reported that appraisals of complex visual hallucinations—as malevolent, omnipotent, or predictive of negative outcomes—were linked to high levels of distress in older, non-psychotic adults (though patients with other disorders were also included in this sample). Such findings are, however, in keeping with a larger body of evidence that negative appraisals about hallucinations are related to the level of distress experienced in both clinical and non-clinical samples (Dudley et al., 2012; Varese et al., 2016; Baumeister et al., 2017). A separate line of studies shows a consistent association between hallucinations and suicidal behaviour in younger (Connell et al., 2016; Cederlöf et al., 2017) and older samples (DeVylder et al., 2015) from the general population, probably reflecting more severe states of psychological disturbance (Honings et al., 2016).
Factors Associated with Hallucinations in Older Adults
Genetic Factors
Multiple studies have explored the link between genetic polymorphisms (e.g., dopamine, ApoE, cholecystokinin [CCK], HOMER, tau, and COMT), and hallucinations in psychiatric disorders typical in younger (e.g., schizophrenia, bipolar disorder) and older (Alzheimer's disease, Parkinson's disease) adults. For example, changes in serotonin receptor 5HT2A expression have been implicated in the presence of visual hallucinations in Parkinson's disease, whilst the novel 5-HT2A inverse agonist, Pimavanserin, appears to be a promising treatment for these symptoms (Stahl, 2016). In general, however, conflicting results are frequent in this literature (Lenka et al., 2016). Substantially fewer studies have investigated the genetic basis of hallucinations in the general community. Nonetheless, recent evidence indicates that hallucinations are the least heritable psychotic experience in community samples (Hur et al., 2012), with no significant role for common genetic variants, at least in complex hallucinations in adolescents (Ronald, 2015; Sieradzka et al., 2015)—though a considerable influence of environmental factors. There appears to be no comparable data from older adult samples, though Lopez-Escamez et al. (2016) have argued that simple acoustic hallucinations such as tinnitus are likely to reflect a build-up of epigenetic and environmental factors over the lifetime. Consequently, although a role for rare genetic variants cannot be excluded, the literature points to a more prominent role for environmental determinants than genetic factors, in the experience of hallucinations across age all groups.
Sensory-Perceptual Functioning
A common effect of ageing is the gradual decline in sensory and perceptual functioning (for a brief review see Roberts and Allen, 2016). For example, age-related hearing loss is one of the most prevalent health conditions in older adults (Mudar and Husain, 2016). UK data indicate that moderate (or worse) hearing loss affects between 39 and 45% of people aged over 601, whilst visual impairment occurs in ~10% of adults aged 65–75 and 20% of those aged over 75 (Evans and Rowlands, 2004). Similar declines occur in the perception of odour, taste, and touch (Doty and Kamath, 2014; Rawal et al., 2016). In fact, dual-sensory (vision and hearing) and multi-sensory impairments are prevalent, lending support to the notion of a single, common factor underlying sensory ageing (Schneider et al., 2012; Dawes et al., 2014; Correia et al., 2016), though differential ageing of specific perceptual functions is inconsistent with this view (Billino et al., 2008).
Age-related decline in sensory functioning is often associated with a deterioration in cognitive functioning as well as poorer mental health and well-being (Hayman et al., 2007; Ciorba et al., 2012; Eramudugolla et al., 2013). Of relevance here, a recent meta-analysis of epidemiological data showed that hearing impairment (irrespective of the type, origin, or severity) is a significant risk factor for the presence of hallucinations, odds ratio = 1.4; 95 CI: 1.18–1.65 (Linszen et al., 2016). Of 5 eligible studies, 2 focused specifically on healthy older adults (70 years +) in the general community (Turvey et al., 2001; Östling and and Skoog, 2002). A major limitation in these studies is the absence of longitudinal data (Linszen et al., 2016), hence the precise nature of the relationship between auditory function and hallucinations and how they unfold in later life is unknown. In addition, details about hearing function (e.g., aetiology), co-occurring sensory impairment, and hallucinatory characteristics (such as modality) are often sparse. As a consequence, it is still unclear if hearing impairment is preferentially linked to auditory hallucinations (implicit in many explanatory models), whether hearing impairment (being the most common type of sensory impairment in old age) is associated with hallucinations in general (regardless of modality) or whether multi-sensory impairment common in older adults is associated with multi-modal hallucinations.
The idea of a modality-dependent effect for hallucinations (i.e., that auditory sensory deficits result in auditory hallucinations, visual sensory deficits result in visual hallucinations etc) is far from clear and much theoretical and empirical work, here as well, is needed. Linszen et al. (2016) in their meta-analysis (that only looked at hearing impairment and not other sensory deprivation modalities) comment that whilst this modality specific relation is implicitly suggested in contemporary models, 3 out of 5 studies included in their meta-analysis included hallucinations in other modalities as well. Further, they comment that a relation may well exist between hearing impairment and hallucinations in several different modalities, albeit most likely visual hallucinations (as they are most prevalent). They further mention that there are no current hypotheses on mechanisms underlying a connection between hearing impairment and visual hallucinations. Thus, more theoretical and empirical work is needed.
Additional evidence linking sensory functioning and hallucinations comes from clinical, neurobiological and case studies of specific types of hallucinations such as tinnitus and Charles Bonnet Syndrome (Pang, 2016; Sedley et al., 2016). Many of these reports include data from a mix of clinical and non-clinical samples (e.g., Golden and Josephs, 2015) or include selected subgroups of older adults (e.g., referred for audiometric testing) that may be vulnerable to bias (Teunisse and Olde Rikkert, 2012). In addition, though sensory impairment is common in ageing it is not inevitably associated with hallucinations, suggesting that multiple factors are involved (Roberts et al., 2010). Similar conclusions have been drawn from hallucination research on psychiatric disorders (Badcock, 2010; Waters et al., 2012; Ford et al., 2014). This multiplicity is stimulating more detailed examination of the similarities and differences in the combination of factors driving hallucinations in healthy and clinical samples (Badcock and Hugdahl, 2012) though age and clinical status are often confounded in these comparisons. For example, a recent meta-analysis of neuroimaging data on psychosis, Parkinson's disease, Charles Bonnet Syndrome and healthy hallucinators showed significant cross-study activation in auditory and visual cortices, pointing to similar mechanisms of sensory over-stimulation in the genesis of hallucinations (Zmigrod et al., 2016). The most common explanations for this increase in activation include disturbances in cortical inhibition and neurotransmitter function arising from a reduction of sensory input (Roberts et al., 2010; Pang, 2016). However, deafferentation alone may not be sufficient to account for the observed hyperexcitability associated with hallucinations: active adaptation to impairments in sensory functioning may also lead to an increased sensitivity to intact sensory inputs. Further understanding of how the excitatory-inhibitory balance changes with age is likely to provide valuable insights into the neural mechanisms and characteristic features of hallucinations. Sensory-perceptual impairments and hallucinations may also be related via a range of direct and indirect effects (i.e., increased demand) on cognitive and psychosocial functioning, reviewed below.
Cognitive Functioning
Cognitive functioning and, more specifically, inhibitory processes, context binding, and reality monitoring (i.e., the processes by which perceived and imagined events are discriminated; Johnson and Raye, 1981) as well as metacognition seems to play a significant role in the generation of hallucinations (Waters et al., 2012; Badcock et al., 2014; Baumeister et al., 2017). Indeed, inhibitory processes are important to suppress distractive memories, intrusive or unwanted thoughts or interfering mental images. Their dysfunction may lead to the emergence of redundant and/or irrelevant information from long-term memory into awareness, resulting in the experience of hallucinations. In support, the ability to suppress mental representation from episodic memory has been associated with the severity of hallucinations (but not delusions) in schizophrenia (Waters et al., 2003; Badcock et al., 2005; Hemsley, 2005). Similarly, Soriano et al. (2009) compared directed forgetting performance in schizophrenia patients with and without hallucination and found that patients with hallucinations presented inhibitory deficits compared to patients without hallucinations (Soriano et al., 2009). Interestingly, similar (though milder) difficulties with intentional inhibition have also been found in healthy young adults prone to hallucinations (Paulik et al., 2007, 2008), leading some authors to suggest that what may differ between clinical and non-clinical hallucinators is how they cope with and/or interpret the experience (Morrison, 2005).
Additionally, context binding deficits have been observed in schizophrenia patients and associated with more frequent hallucinations experiences, though a similar relationship has not been observed in young healthy individuals prone to hallucinations (Badcock et al., 2008). In contrast, studies have found that schizophrenia patients experiencing auditory hallucinations were more likely to incorrectly attribute the source of words they uttered themselves to the experimenter (i.e., a reality monitoring problem called an externalizing bias) compared to controls and similar effects were found in samples of non-clinical individuals prone to hallucinations (Brookwell et al., 2013) especially for negative materials compared to neutral and positive materials (Kanemoto et al., 2013). Moreover, there is some evidence that young, healthy adults predisposed to hallucinations exhibit an externalizing bias when emotionally charged material is involved and when more cognitive effort is required. Of particular relevance, compared to those with a low tendency to hallucinate, these individuals had higher scores on a scale assessing beliefs and worry about intrusive thoughts (i.e., the Meta-Cognition Questionnaire, Cartwright-Hatton and Wells, 1997) and these scores were positively associated with their source discrimination errors (Morrison et al., 2000; Larøi et al., 2004).
All these cognitive components postulated to be involved in the etiology of hallucinations are directly or indirectly affected (e.g., through reduced speed of processing, attentional resources, or working memory capacity; Park and Reuter-Lorenz, 2009) in healthy aging (Hasher and Zacks, 1988; Lustig et al., 2007; Rast, 2011). Thus, one might expect an increased likelihood of hallucinations in the elderly population compared to younger groups. That is, age-related deficits in inhibition (Lustig et al., 2007; Clarys et al., 2009; Collette et al., 2009), demanding memory processes (i.e., specific and/or distinctive recollection processes and accurate source memory, e.g., Dehon and Bredart, 2004; Dehon, 2006; Fairfield and Mammarella, 2009) as well as context binding (Mitchell et al., 2000; Piolino et al., 2010) may result in a greater likelihood of generating hallucinations in this population. However, again, only a few studies on cognitive functioning and hallucinations including healthy older adults are available and these studies are substantially limited by the fact that their samples of older adults are relatively small and/or the older adults were not their target population. That is, either some older adults were included in the general healthy sample (e.g., Stirling et al., 2007) or they served as controls for studies on hallucinations in Alzheimer's patients (El Haj et al., 2015, 2016).
Notwithstanding, in a recent set of studies, Alzheimer's disease patients and healthy older adults were asked to complete tests tapping several cognitive functions. These tasks included measures of general cognitive functioning, episodic memory, working memory (forward and backward span), verbal fluency as well as a measure of inhibition (a Stroop task; El Haj et al., 2015) or a measure of directed forgetting (El Haj et al., 2016) and a measure of auditory and visual hallucinations (i.e., 6 items from the Launay Slade Hallucinations Scale-Revised, LSHS-R; Launay and Slade, 1981). Overall, healthy older controls reported less hallucinations and had better performance on the cognitive tests than Alzheimer's disease patients. Interestingly, although most of the cognitive measures were not further included in the analyses, hallucinations were found to be mediated by inhibitory decline either as measured by the ability to supress a pre-potent response (i.e., performance in the Stroop task) or by the ability to supress memory representation (i.e., performance in a directed-forgetting task) in Alzheimer's disease (El Haj et al., 2015, 2016) but not in healthy aged-matched controls. However, the interpretation of these results needs caution due to the small samples of older adults recruited in these studies (i.e., 20–24 older control participants), the very low rates of reported hallucinations in these older adult groups that may prevent any relationship between cognitive functioning and inhibition to be observed, and the absence of younger adults that preclude any comparison based on age.
Likewise, another study on hallucination in healthy individuals that included a few older adults has shown that healthy individuals differentiated in terms of their hallucinatory experiences (i.e., high, medium, or low scores on the LSHS-R) presented distinct patterns of meta-cognitive processing—as measured on the Meta-Cognition Questionnaire (Cartwright-Hatton and Wells, 1997), but again, the data are difficult to interpret due to the inadequate sample size of older participants (Stirling et al., 2007). Other aspects that would also deserve attention are the insight associated with hallucinatory experiences in older adults and the extent to which the emotional content of hallucinations yields similar effects as those observed in young adults (Larøi et al., 2004; Kanemoto et al., 2013). Indeed, it is interesting to note that hallucinations might be associated with differing levels of insight in healthy individuals, ranging from the firm belief of the actual existence of the hallucination to the acceptance of their internal origin (see Castelnovo et al., 2015) but, again, little is known about this issue in older adults with hallucinatory experiences.
Thus, so far, the data do not seem to indicate a higher probability of hallucinations in older (compared to younger) healthy adults, but further studies are needed that focus on this population and on their cognitive particularities with large samples as there is also considerable variability in cognitive abilities with increasing age (Park and Reuter-Lorenz, 2009). In addition, the inclusion of a comparison group of younger adults would be necessary in these studies, in order to determine whether the hallucinatory experiences and their potential links with cognitive abilities that would be observed in older adults are due to direct effects of age or to other factors (e.g., reduced cognitive resources or individual differences; Park and Reuter-Lorenz, 2009). Finally, cognitive function per se might not be the major factor (or be sufficient alone) in hallucination generation but may instead define older adults at risk of perceptual anomalies in some situations (such as when impairment in sensory processes increases cognitive demands or when psychological and/or social factors may increase distress) or combinations of these effects. Similarly, hallucinations may be influenced by age-related effects on cognition and poor sleep quality as reviewed below.
Sleep Disturbance
Disturbance in sleep—though not exclusive to ageing—is common in older adults. Estimates suggest that around 32—36% of people over 60 years, with otherwise good health, report problems with the quantity or quality of their sleep (Foley et al., 2004; Mattis and Sehgal, 2016; Kim et al., 2017). This percentage increases in the presence of comorbid physical and mental disorders, polypharmacy, and psychosocial factors (such as social isolation, loneliness, and bereavement) and, for many, these sleep problems are chronic and undiagnosed (Miner and Kryger, 2017).
The association between sleep disturbance and psychotic disorders or symptoms has long been recognized (Kraepelin, 1919). For example, studies suggest that schizophrenia patients have more disrupted sleep-wake cycles and sleep quality than healthy controls, which exacerbates delusions and hallucinations (Monti and Monti, 2005; Afonso et al., 2011, 2014). Similarly, disturbance of sleep is common both in neurodegenerative disorders and bereavement, in which hallucinations are frequently experienced (Monk et al., 2008; Wulff et al., 2010; Burghaus et al., 2012; Llorca et al., 2016). Beyond the literature on clinical groups, surveys of the general population show that disturbances of sleep, such as insomnia, are associated with a greater likelihood of reporting current hallucinations and developing new episodes of hallucinations, suggesting that disrupted sleep may causally contribute to these experiences (Reeve et al., 2015; Sheaves et al., 2016). Whilst the relationship between sleep problems and hallucinations does not appear to be mediated by depression, anxiety or paranoia, the specific mechanistic pathways involved have not been established. However, a number of possibilities exist, including the effects of poor sleep quality on neuronal atrophy and poor cognitive functioning with increasing age (Miyata et al., 2013; Del Brutto et al., 2016). Unfortunately, large community studies have a number of limitations, including reliance on subjective report of sleep changes, lack of precision in the assessment of hallucinations or in the moderating effects of age. Consequently, a more nuanced understanding is needed of age-related changes in sleep and hallucinatory experiences. For example, it has recently been proposed that, with advancing age, hyperarousal of the sympathetic nervous system promotes the development of both tinnitus and insomnia (Wallhäusser-Franke et al., 2013). A final point worth noting is that caregivers or partners may sometimes interpret the vivid dreams reported by older adults as hallucinatory experiences. The similarities between these experiences (both involve vivid mental events) make them difficult to distinguish, though they are different, in that hallucinations entail unusual sensory experience perceived to be occurring whilst awake whilst reporting that a vivid dream felt real is based on recollection of events whilst asleep.
Psychosocial and Cultural Factors
If there is strong evidence linking sensory and/or cognitive functioning and hallucinations, other factors such as loneliness and grief, which increase with age, may also affect the likelihood of hallucinations in older adults but, again, only a few empirical studies are currently available. Loneliness is the subjective experience of distress caused by lack of social support and belonging (Gierveld, 1998; Cacioppo and Cacioppo, 2014b) and is a common experience in older adults (Dykstra, 2009; Nicolaisen and Thorsen, 2014). Indeed, with increasing age, retirement, loss of partners, and/or friends, health and functional problems may limit social network size and affect social contacts which consequently increase loneliness (Aartsen and Jylhä, 2011). Increased loneliness in turn has been found to be related to depression (Prince et al., 1997), cardiovascular disease (Barth et al., 2010), and increased rates of mortality (Steptoe et al., 2013). In addition to the subjective experience of lacking social relations (i.e., loneliness; Weiss, 1973), having an objectively diminished social network (i.e., social isolation; Weiss, 1973) have been found to negatively affect cognition in old age (e.g., Bassuk et al., 1999; Fratiglioni et al., 2000; Wilson et al., 2007; Cacioppo and Cacioppo, 2014a). Recently, El Haj and colleagues specifically explored the relationship between social isolation, loneliness and hallucinations in Alzheimer's disease patients and healthy older adults. In both groups, they observed a significant correlation between hallucinations and loneliness, on the one hand, and hallucinations and social isolation on the other; although further analysis found that hallucinations were only predicted by social isolation (El Haj et al., 2016). These results are interesting as the relationship between social isolation, loneliness, and hallucinations appears to be related to ageing rather than to cognitive decline (i.e., similar correlations were observed in both healthy controls and Alzheimer's disease participants). This suggests that healthy older adults, when lacking exchange of thoughts and feelings with others or experiencing a need to communicate or express themselves, may attempt to fullfil these needs by generating internal stimulation leading to some forms of hallucination-like experiences similar to that observed in psychotic states (Hoffman, 2007, 2008). Hence, verbal and visual hallucinations may be viewed as experiences that allow individuals to escape boredom, emptiness, or distress prompted by the lack of external stimulation observed in social isolation (Hoffman, 2008). Of particular relevance for this suggestion is research showing that extreme isolation has been associated with hallucinations in prisoners and hostages confined and/or with sensory restrictions (Launay and Slade, 1981; Siegel, 1984).
Similarly, post-bereavement hallucinations have also been regarded as a compensatory mechanism for social isolation and affective deprivation or distress that may play an important part in the mourning process (Grimby, 1993). Indeed, it is not unusual for the bereaved (especially during acute grief) to sense the presence of their dead spouse, feel them watching out for or protecting them, feel they had been touched by their dead partner, to rehearse discussions, heard their voice or “speak” to them, seen them or smelled their presence (e.g., Grimby, 1993; Keen et al., 2013, see Castelnovo et al., 2015 for a recent review). Studies showed similar symptoms irrespective of gender, in sudden vs. anticipated death and religious and non-religious individuals (Wiener et al., 1996; Sacks, 2012). More relevant for the current review, these findings were largely replicated in older populations (Rees, 1971; Grimby, 1993, 1998). For instance, Rees (1971) observed that 46.7% of his participants (n = 293) reported post-bereavement hallucinations. Among them, adults over 40 years of age (mostly people of 60 years old and older) were more likely to be widowed and slightly more likely to see and have conversations with their dead ones than adults below 40 years of age. Similarly, Grimby (1993) observed that 82% of her older adults groups (n = 50) reported hallucinations and illusions following bereavement. About one half reported feeling the presence of their deceased partner (52%) and about one third reported seeing (26%), hearing (30%), and talking to her/him (30%). Additionally, marital harmony (i.e., happy marriage) was more associated with low mood, loneliness, crying, and hallucinations (for similar results see Grimby, 1998). Moreover, although manifestations of grief are influenced by social and cultural rituals, such as funerals or other customs, post-bereavement hallucinations appear to be common in many different cultures (Yamamoto et al., 1969; Lindstrõm, 1995; Grimby, 1998; Chan et al., 2005). For example, Grimby (1998) examined the incidence of hallucinations in Swedish elderly widows and widowers, within the first year after the partner's death. She found that feeling the presence of the deceased and reporting actually seeing, hearing, and talking to the deceased were the most commonly reported phenomena. Although post-bereavement hallucinations are common in many different cultures, some studies suggest that there may be important cultural differences in their prevalence, whereby certain cultures have particularly high rates of post-bereavement hallucinations. More work is needed but, for instance, Yamamoto et al. (1969) mention that prevalence rates may be higher in Japan compared to other cultures due, in part, to religions in Japan (Shintoism and Buddhism) that permit the mourner to maintain contact with the deceased, and Bell (2008) cites case reports that suggest that this phenomenon may also be particular prevalent among the Hopi Indians, Mu Ghayeb people from Oman and in Hispanic populations. Again, very little systematic work has been done in this area.
Pharmacological Issues
Polypharmacy is quite common among the elderly population as the need to treat various diseases developing with age increases. Overall, the available studies showed that nearly 50% of older adults take one or more medications that are not medically necessary (e.g., Rossi et al., 2007; Qato et al., 2008; Rambhade et al., 2012). For this reason, the clinical consequences of polypharmacy have received growing attention in recent years (Hajjar et al., 2007; Maher et al., 2014). Research has shown an increased risk of greater health costs (Hovstadius and Petersson, 2013) as well as adverse drugs events and interactions (e.g., Hohl et al., 2001) that, in turn, have huge effects on functional and cognitive capacities (Jyrkka et al., 2011) and may contribute to the development of hallucinations. Similarly, although substance abuse in older adults has received little attention in the past, illicit drugs, and substance abuse (e.g., alcohol) because of loneliness and/or boredom or overuse of prescription drugs (e.g., barbiturates) is likely to be a frequent problem in an increasing elderly population (Dowling et al., 2008). This acute or chronic abuse may be an additional factor in the development of hallucinations in this population (Wood et al., 1988; Targum, 2001). Moreover, the resulting acute withdrawal from these substances can also elicit vivid hallucinations and delusions. Whether evoked by polypharmacy or (illicit) drug abuse, close attention should be drawn on these manifestations as they may often be erroneously attributed to early signs of dementia or advancing age (Wood et al., 1988; Jyrkka et al., 2011; Rambhade et al., 2012).
Discussion of Findings
Hallucinations experienced later in life have not been a major area of interest. This first comprehensive overview the literature highlights the fact that hallucinations occur in a substantial minority of healthy older adults in the general community (McGrath et al., 2016; Soulas et al., 2016). However, public understanding of these experiences is lagging behind the evidence base, with many older (and younger) adults assuming that they are synonymous with mental illness. Consequently, more accurate information is needed in the general community to raise awareness of the varieties of hallucinatory phenomena and the many factors associated with them.
A number of issues arise from the existing literature that merit further attention. First, the considerable variation in prevalence of hallucinations in older adults is a challenge. The finding that the prevalence of auditory and visual hallucinations seems to diminish with age is surprising. Advancing age is associated with a host of risk factors for hallucinations, including impairments in sensory, cognitive, and social functioning, so the rate of hallucinations might be expected to increase. How might this discrepancy be interpreted?
One possibility is that current prevalence estimates are inaccurate. The different assessment tools used across studies (each capturing a different range of symptoms and experiences and each assessing hallucinations in different time-frames ranging from the past month to lifetime prevalence), together with the sparsity of samples aged over 80 years, makes it difficult to draw firm conclusions about the prevalence of hallucinations in different age groups. In addition, due to reluctance to disclose these experiences, it is possible that the true prevalence of hallucinations in older adults may be higher. Indeed, when reluctance to talk is overcome—as in studies of post-bereavement hallucinations—substantially higher rates have been found (Castelnovo et al., 2015).
Another possibility is that presence of individual risk factors is insufficient for hallucinations to develop. As is often noted, despite the preponderance of sensory decline with age, the majority of older adults don't hallucinate. Indeed, single factor models of hallucinations—in psychosis, dementia, eye-disease, and healthy hallucinators—have been superseded by more complex, multifactorial accounts (Waters et al., 2012; Collerton et al., 2016). To illustrate, occasional case reports suggest that in older people with pre-existing eye disease, the death of a spouse may increase the likelihood of Charles Bonnet Syndrome, indicating that biological and psychological mechanisms may interact (e.g., Adair and Keshavan, 1988).
A third possibility governing the relationship between age and the emergence of hallucinations is that, with age, older adults actively adjust to sensory, cognitive and social decline by reorganizing neural, psychological, and social responses (Daselaar et al., 2015; Qualter et al., 2015). For example, compared to younger individuals, older adults commonly show greater task-related cortical activation (even when performance is equivalent)—argued to reflect a compensatory increase in neural response to ameliorate the adverse effects of neural decline (Reuter-Lorenz and Park, 2014). At a social level of analysis, loneliness has been shown to motivate people of all ages to re-connect with others, to fulfill the basic need for belonging (Qualter et al., 2015). Consequently, the onset of hallucinations is likely to be influenced by prior and current levels of sensory, cognitive and social (dys)function combined with the relative success of compensatory processes as well (see Figure 1).
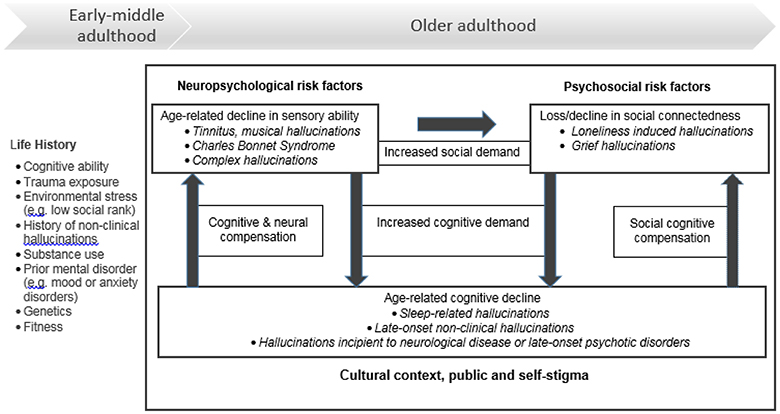
Figure 1. Hallucinatory experiences in healthy older adults (i.e., without psychosis, delirium, or dementia).
A final consideration is whether older adults prone to hallucinatory experiences tend to die younger, reflecting an accumulation of structural and functional pathology in the central nervous system.
Implications for Aged-care Services and Interventions
The evidence reviewed above means that a range of aged-care health and service providers (e.g., general practitioners, pharmacists, nurses, opticians, psychologists) need to be aware that hallucinations in older adults are possible, and these may, or may not, indicate the presence of a mental disorder. Unfortunately, qualitative feedback suggests that hallucinatory experiences in the aged population are often under-recognized and/or misunderstood by many clinicians, suggesting there is significant scope for improvement in the training of both current and future professionals working with this population. In particular, service providers need to be mindful that older adults may not disclose their experience of hallucinations unless directly questioned. A wide variety of approaches have been used to assess hallucinations in older adults, though no systematic analysis of the scope and suitability of these tools for assessing these experiences in healthy older adults has yet been undertaken. In view of current evidence, screening for sleep disturbance, sensory impairments, psychosocial stressors (especially bereavement) and internalized stigma as potential causes or correlates of hallucinations, and targets for intervention, is recommended.
Gaps in the Evidence Base and Directions for Future Research
The lack of longitudinal studies is a major weakness in the current evidence base on hallucinations in older adults. Long term follow-up of healthy individuals is essential to determine the extent, and conditions under which hallucinations remit, or predict the development of future mental disease or disorders. For instance, there has been an ongoing debate as to whether visual hallucinations in Charles Bonnet Syndrome are, or are not, an early risk marker for dementia (Pliskin et al., 1996; Lapid et al., 2013). However, recent prospective data from Russell et al. (2017) point to an increased incidence of dementia in people over 65 with this syndrome. On the other hand, minor hallucinations are reported in 42% of new, untreated cases of Parkinson's disease (Pagonabarraga et al., 2016), with early evidence of visual hallucinations predicting an increased risk of dementia (ffytche et al., 2017). However, the trajectory from minor hallucinations in healthy ageing (Soulas et al., 2016) to illness onset in Parkinson's disease is unknown. Similarly, hallucinations in younger cohorts are associated with the later development of suicide attempts. However, although suicidal behaviour in older adulthood is a major problem (Conwell, 2014; Stanley et al., 2016), the long-term predictive value of hallucinations in people over 60 years has not been investigated. Notably, there is also a paucity of long term follow-up studies (see Daalman et al., 2016, as an exception) exploring hallucinations as early warning signs of late-onset psychotic disorders; consequently, the processes involved in the development of a need for care remain unclear.
A second obvious gap concerns research on post-bereavement hallucinations. Bereavement is a time when hallucinations are so common they may be viewed as the norm rather than the exception (Bell, 2008), yet studies in this area are still rare. Post-bereavement hallucinations may be particularly informative about the mechanisms driving the onset, and offset, of hallucinations, since they typically remit over time. However, although some researchers have theorized about the role of post-traumatic stress in this type of hallucination (Hayes and Leudar, 2016), empirical investigation of stress-related (biological, cognitive or social) responses is missing. In addition, understanding family members' and carer's responses to post-bereavement and other hallucinatory phenomena has received little investigation, but warrants further investigation given existing evidence that the presence of hallucinations in those with Parkinson's disease or dementia is a strong predictor of caregiver stress and nursing home admission (Oh et al., 2015; Cepoiu-Martin et al., 2016).
A final observation is the general lack of studies in this age group. Compared to the large amount of research on hallucinations in the general population, which are mostly focused on children or individuals 18–40 years, and the sizeable number of studies examining hallucinations in clinical samples (in younger and older adults)—there is a clear paucity of studies on hallucinations in healthy ageing (de Leede-Smith and Barkus, 2013; Baumeister et al., 2017). Moreover, the few studies that have examined hallucinations in community dwelling older adults have typically adopted a narrow lens (e.g., assessing sensory or cognitive factors in isolation) and relatively simple methods of investigation (e.g., self-report or behavioural measures). Future research would benefit from a more sophisticated approach examining multiple, interacting factors within the context of older people's lives. Based on the issues detailed above, some practical recommendations are proposed in Table 2 to stimulate future research.
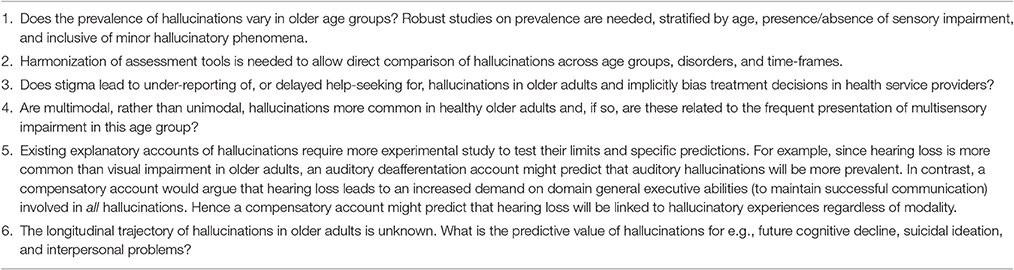
Table 2. Issues for future research.
Author Contributions
JB and FL jointly conceived the idea for the manuscript. JB, HD, and FL all contributed to reviewing the literature, and wrote separate subsections of the manuscript. All authors provided critical commentary on all drafts, approved the final version to be published, and agree to be accountable for the content of the work.
Conflict of Interest Statement
JB receives salary support from the Cooperative Research Centre-Mental Health, Carlton, Victoria, Australia. The Cooperative Research Centre-Mental Health had no role in the conduct of this review or the decision to submit the manuscript for publication.
The other authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: http://journal.frontiersin.org/article/10.3389/fpsyg.2017.01134/full#supplementary-material
Footnotes
1. ^Defined as >35 hearing level in decibels (dB HL) in the better ear averaged over 0.5, 1, 2, and 4 kHz frequencies (Davies, 2012).
References
Aartsen, M., and Jylhä, M. (2011). Onset of loneliness in older adults: results of a 28 year prospective study. Eur. J. Ageing 8, 31–38. doi: 10.1007/s10433-011-0175-7
Adair, D. K., and Keshavan, M. S. (1988). The Charles Bonnet syndrome and grief reaction. Am. J. Psychiatry 145, 895–896.
Afonso, P., Brissos, S., Figueira, M. L., and Paiva, T. (2011). Schizophrenia patients with predominantly positive symptoms have more disturbed sleep-wake cycles measured by actigraphy. Psychiatry Res. 189, 62–66. doi: 10.1016/j.psychres.2010.12.031
Afonso, P., Figueira, M. L., and Paiva, T. (2014). Sleep–wake patterns in schizophrenia patients compared to healthy controls. World J. Biol. Psychiatry 15, 517–524. doi: 10.3109/15622975.2012.756987
Badcock, J. C. (2010). The cognitive neuropsychology of auditory hallucinations: a parallel auditory pathways framework. Schizophr. Bull. 36, 576–584. doi: 10.1093/schbul/sbn128
Badcock, J. C., Chhabra, S., Maybery, M. T., and Paulik, G. (2008). Context binding and hallucination predisposition. Person. Indiv. Diff. 45, 822–827. doi: 10.1016/j.paid.2008.08.016
Badcock, J. C., and Hugdahl, K. (2012). Cognitive mechanisms of auditory verbal hallucinations in psychotic and non-psychotic groups. Neurosci. Biobehav. Rev. 36, 431–438. doi: 10.1016/j.neubiorev.2011.07.010
Badcock, J. C., Larøi, F., Allen, P., and Diederen, K. (2014). Current Perspectives on the Mechanisms of Auditory Hallucinations in Clinical and Non-clinical Groups Frontiers Research Topic EBook, 144. Available online at: http://www.frontiersin.org/Human_Neuroscience/researchtopics/Current_perspectives_on_the_mechanisms_of_auditory_hallucinations_in_clinical_and_non-clinical_populations/992. doi: 10.3389/978-2-88919-203-8
Badcock, J. C., Waters, F. A., Maybery, M. T., and Michie, P. T. (2005). Auditory hallucinations: failure to inhibit irrelevant memories. Cogn. Neuropsychiatry 10, 125–136. doi: 10.1080/13546800344000363
Barber, S. J. (2017). An examination of age-based stereotype threat about cognitive decline. Perspect. Psychol. Sci. 12, 62–90. doi: 10.1177/1745691616656345
Barth, J., Schneider, S., and von Kanel, R. (2010). Lack of social support in the etiology and the prognosis of coronary heart disease: a systematic review and meta-analysis. Psychosom. Med. 72, 229–238. doi: 10.1097/PSY.0b013e3181d01611
Bassuk, S. S., Glass, T. A., and Berkman, L. F. (1999). Social disengagement and incident cognitive decline in community-dwelling elderly persons. Ann. Internal. Med. 131, 165–173. doi: 10.7326/0003-4819-131-3-199908030-00002
Baumeister, D., Sedgwick, O., Howes, O., and Peters, E. (2017). Auditory verbal hallucinations and continuum models of psychosis: a systematic review of the healthy voice-hearer literature. Clin. Psychol. Rev. 51, 125–141. doi: 10.1016/j.cpr.2016.10.010
Bell, V. (2008). Ghost Stories: Visits from the Deceased. Scientific American. Available online at: https://www.scientificamerican.com/article/ghost-stories-visits-from-the-deceased/
Billino, J., Bremmer, F., and Gegenfurtner, K. R. (2008). Differential aging of motion processing mechanisms: evidence against general perceptual decline. Vision Res. 48, 1254–1261. doi: 10.1016/j.visres.2008.02.014
Brookwell, M. L., Bentall, R. P., and Varese, F. (2013). Externalizing biases and hallucinations in source-monitoring, self-monitoring and signal detection studies: a meta-analytic review. Psychol. Med. 43, 2465–2475. doi: 10.1017/s0033291712002760
Burghaus, L., Eggers, C., Timmermann, L., Fink, G. R., and Diederich, N. J. (2012). Hallucinations in neurodegenerative diseases. CNS Neurosci. Ther. 18, 149–159. doi: 10.1111/j.1755-5949.2011.00247.x
Cacioppo, J. T., and Cacioppo, S. (2014a). Older adults reporting social isolation or loneliness show poorer cognitive function 4 years later. Evid. Based Nurs. 17, 59–60. doi: 10.1136/eb-2013-101379
Cacioppo, J. T., and Cacioppo, S. (2014b). Social relationships and health: the toxic effects of perceived social isolation. Soc. Personal. Psychol. Compass 8, 58–72. doi: 10.1111/spc3.12087
Cartwright-Hatton, S., and Wells, A. (1997). Beliefs about worry and intrusions: the meta-cognitions questionnaire and its correlates. J. Anxiety Disord. 11, 279–296. doi: 10.1016/S0887-6185(97)00011-X
Castelnovo, A., Cavallotti, S., Gambini, O., and D'Agostino, A. (2015). Post-bereavement hallucinatory experiences: a critical overview of population and clinical studies. J. Affect. Disord. 186, 266–274. doi: 10.1016/j.jad.2015.07.032
Cederlöf, M., Kuja-Halkola, R., Larsson, H., Sjölander, A., Östberg, P., Lundström, S., et al. (2017). A longitudinal study of adolescent psychotic experiences and later development of substance use disorder and suicidal behavior. Schizophr. Res. 181, 13–16. doi: 10.1016/j.schres.2016.08.029
Cepoiu-Martin, M., Tam-Tham, H., Patten, S., Maxwell, C. J., and Hogan, D. B. (2016). Predictors of long-term care placement in persons with dementia: a systematic review and meta-analysis. Int. J. Geriatr. Psychiatry 31, 1151–1171. doi: 10.1002/gps.4449
Chan, C. L., Chow, A. Y., Ho, S. M., Tsui, Y. K., Tin, A. F., Koo, B. W., et al. (2005). The experience of Chinese bereaved persons: a preliminary study of meaning making and continuing bonds. Death Stud. 29, 923–947. doi: 10.1080/07481180500299287
Ciorba, A., Bianchini, C., Pelucchi, S., and Pastore, A. (2012). The impact of hearing loss on the quality of life of elderly adults. Clin. Interv. Aging 7, 159–163. doi: 10.2147/CIA.S26059
Clarys, D., Bugaiska, A., Tapia, G., and Baudouin, A. (2009). Ageing, remembering, and executive function. Memory 17, 158–168. doi: 10.1080/09658210802188301
Cole, M. G., Dowson, L., Dendukuri, N., and Belzile, E. (2002). The prevalence and phenomenology of auditory hallucinations among elderly subjects attending an audiology clinic. Int. J. Geriatr. Psychiatry 17, 444–452. doi: 10.1002/gps.618
Collerton, D., Mosimann, U. P., and Archibald, N. (2012). “Disorders of visual perception in Parkinson's disease and other Lewy body disorders,” in Psychiatry of Parkinson's Disease, Vol. 27, eds K. P. Ebmeier, J. T. O'Brien, and J.-P. Taylor (Basel: Karger), 41–52.
Collerton, D., Taylor, J. P., Tsuda, I., Fujii, H., Nara, S., Aihar, K., et al. (2016). How can we see things that are not there?: current insights into complex visual hallucinations. J. Conscious. Stud. 23, 195–227. Available online at: http://www.ingentaconnect.com/content/imp/jcs/2016/00000023/F0020007/art00009
Collette, F., Germain, S., Hogge, M., and Van der Linden, M. (2009). Inhibitory control of memory in normal ageing: dissociation between impaired intentional and preserved unintentional processes. Memory 17, 104–122. doi: 10.1080/09658210802574146
Connell, M., Betts, K., McGrath, J. J., Alati, R., Najman, J., Clavarino, A., et al. (2016). Hallucinations in adolescents and risk for mental disorders and suicidal behaviour in adulthood: prospective evidence from the MUSP birth cohort study. Schizophr. Res. 176, 546–551. doi: 10.1016/j.schres.2016.06.009
Conwell, Y. (2014). Suicide later in life: challenges and priorities for prevention. Am. J. Prev. Med. 47(3Suppl. 2), S244–S250. doi: 10.1016/j.amepre.2014.05.040
Correia, C., Lopez, K. J., Wroblewski, K. E., Huisingh-Scheetz, M., Kern, D. W., Chen, R. C., et al. (2016). Global sensory impairment in older adults in the United States. J. Am. Geriatr. Soc. 64, 306–313. doi: 10.1111/jgs.13955
Cox, T. M., and ffytche, D. H. (2014). Negative outcome charles bonnet syndrome. Br. J. Ophthalmol. 98, 1236–1239. doi: 10.1136/bjophthalmol-2014-304920
Cuddy, A. J. C., Norton, M. I., and Fiske, S. T. (2005). This old stereotype: the pervasiveness and persistence of the elderly stereotype. J. Soc. Issues 61, 267–285. doi: 10.1111/j.1540-4560.2005.00405.x
Daalman, K., Diederen, K. M. J., Hoekema, L., van Lutterveld, R., and Sommer, I. E. C. (2016). Five year follow-up of non-psychotic adults with frequent auditory verbal hallucinations: are they still healthy? Psychol. Med. 46, 1897–1907. doi: 10.1017/S0033291716000386
Daselaar, S. M., Iyengar, V., Davis, S. W., Eklund, K., Hayes, S. M., and Cabeza, R. E. (2015). Less wiring, more firing: low-performing older adults compensate for impaired white matter with greater neural activity. Cereb. Cortex 25, 983–990. doi: 10.1093/cercor/bht289
David, A. S. (2004). The cognitive neuropsychiatry of auditory verbal hallucinations: an overview. Cogn. Neuropsychiatry 9, 107–123. doi: 10.1080/13546800344000183
Davies, S. C. (2012). Annual Report of the Chief Medical Officer, Volume One, 2011, On the State of the Public's Health. London: Department of Health.
Dawes, P., Dickinson, C., Emsley, R., Bishop, P. N., Cruickshanks, K. J., Edmondson-Jones, M., et al. (2014). Vision impairment and dual sensory problems in middle age. Ophthalm. Physiol. Optics 34, 479–488. doi: 10.1111/opo.12138
de Leede-Smith, S., and Barkus, E. (2013). A comprehensive review of auditory verbal hallucinations: lifetime prevalence, correlates and mechanisms in healthy and clinical individuals. Front. Hum. Neurosci. 7:367. doi: 10.3389/fnhum.2013.00367
Dehon, H. (2006). Variations in processing resources and resistance to false memories in younger and older adults. Memory 14, 692–711. doi: 10.1080/09658210600648456
Dehon, H., and Bredart, S. (2004). False memories: young and older adults think of semantic associates at the same rate, but young adults are more successful at source monitoring. Psychol. Aging 19, 191–197. doi: 10.1037/0882-7974.19.1.191
Del Brutto, O. H., Mera, R. M., Zambrano, M., and Castillo, P. R. (2016). The association between poor sleep quality and global cortical atrophy is related to age. Results from the Atahualpa Project. Sleep Sci. 9, 147–150. doi: 10.1016/j.slsci.2016.06.004
DeVylder, J. E., Lukens, E. P., Link, B. G., and Lieberman, J. A. (2015). Suicidal ideation and suicide attempts among adults with psychotic experiences: data from the collaborative psychiatric epidemiology surveys. JAMA Psychiatry 72, 219–225. doi: 10.1001/jamapsychiatry.2014.2663
Doty, R. L., and Kamath, V. (2014). The influences of age on olfaction: a review. Front. Psychol. 5:20. doi: 10.3389/fpsyg.2014.00020
Dowling, G. J., Weiss, S. R., and Condon, T. P. (2008). Drugs of abuse and the aging brain. Neuropsychopharmacology 33, 209–218. doi: 10.1038/sj.npp.1301412
Dudley, R., Wood, M., Spencer, H., Brabban, A., Mosimann, U. P., and Collerton, D. (2012). Identifying specific interpretations and use of safety behaviours in people with distressing visual hallucinations: an exploratory study. Behav. Cogn. Psychother. 40, 367–375. doi: 10.1017/s1352465811000750
Dykstra, P. A. (2009). Older adult loneliness: myths and realities. Eur. J. Ageing 6, 91–100. doi: 10.1007/s10433-009-0110-3
El Haj, M., Jardri, R., Larøi, F., and Antoine, P. (2016). Hallucinations, loneliness, and social isolation in Alzheimer's disease. Cogn. Neuropsychiatry 21, 1–13. doi: 10.1080/13546805.2015.1121139
El Haj, M., Larøi, F., Gély-Nargeot, M. C., and Raffard, S. (2015). Inhibitory deterioration may contribute to hallucinations in Alzheimer's disease. Cogn. Neuropsychiatry 20, 281–295. doi: 10.1080/13546805.2015.1023392
Eramudugolla, R., Wood, J., and Anstey, K. J. (2013). Co-morbidity of depression and anxiety in common age-related eye diseases: a population-based study of 662 adults. Front. Aging Neurosci. 5:56. doi: 10.3389/fnagi.2013.00056
Evans, B. J., and Rowlands, G. (2004). Correctable visual impairment in older people: a major unmet need. Ophthalm. Physiol. Opt. 24, 161–180. doi: 10.1111/j.1475-1313.2004.00197.x
Fairfield, B., and Mammarella, N. (2009). The role of cognitive operations in reality monitoring: a study with healthy older adults and Alzheimer's-type dementia. J. Gen. Psychol. 136, 21–39. doi: 10.3200/genp.136.1.21-40
ffytche, D. H., Creese, B., Politis, M., Chaudhuri, K. R., Weintraub, D., Ballard, C., et al. (2017). The psychosis spectrum in Parkinson disease. Nat. Rev. Neurol. 13, 81–95. doi: 10.1038/nrneurol.2016.200
Foley, D., Ancoli-Israel, S., Britz, P., and Walsh, J. (2004). Sleep disturbances and chronic disease in older adults: results of the 2003 National Sleep Foundation Sleep in America Survey. J. Psychosom. Res. 56, 497–502. doi: 10.1016/j.jpsychores.2004.02.010
Ford, J. M., Morris, S. E., Hoffman, R. E., Sommer, I., Waters, F. A., McCarthy-Jones, S., et al. (2014). Studying hallucinations within the NIMH RDoC framework. Schizophr. Bull. 40(Suppl. 4),S295–S304. doi: 10.1093/schbul/sbu011
Fratiglioni, L., Wang, H. X., Ericsson, K., Maytan, M., and Winblad, B. (2000). Influence of social network on occurrence of dementia: a community-based longitudinal study. Lancet 355, 1315–1319. doi: 10.1016/S0140-6736(00)02113-9
Geda, Y. E., Roberts, R. O., Knopman, D. S., Petersen, R. C., Christianson, T. J., Pankratz, V. S., et al. (2008). Prevalence of neuropsychiatric symptoms in mild cognitive impairment and normal cognitive aging: population-based study. Arch. Gen. Psychiatry 65, 1193–1198. doi: 10.1001/archpsyc.65.10.1193
Gierveld, J. D. J. (1998). A review of loneliness: concept and definitions, determinants and consequences. Rev. Clin. Gerontol. 8, 73–80.
Golden, E. C., and Josephs, K. A. (2015). Minds on replay: musical hallucinations and their relationship to neurological disease. Brain 138(Pt 12), 3793–3802. doi: 10.1093/brain/awv286
Grimby, A. (1993). Bereavement among elderly people: grief reactions, post-bereavement hallucinations and quality of life. Acta Psychiatr. Scand. 87, 72–80.
Grimby, A. (1998). Hallucinations following the loss of a spouse: Common and normal events among the elderly. J. Clin. Geropsychol. 4, 65–74.
Hajjar, E. R., Cafiero, A. C., and Hanlon, J. T. (2007). Polypharmacy in elderly patients. Am. J. Geriatr. Pharmacother. 5, 345–351. doi: 10.1016/j.amjopharm.2007.12.002
Hasher, L., and Zacks, R. T. (1988). “Working memory, comprehension and aging: a review and a new view,” in The Psychology of Learning and Motivation, ed G. H. Bower (New York, NY: Academic Press), 193–225.
Hayes, J., and Leudar, I. (2016). Experiences of continued presence: on the practical consequences of ‘hallucinations’ in bereavement. Psychol. Psychother. Theor. Res. Pract. 89, 194–210. doi: 10.1111/papt.12067
Hayman, K. J., Kerse, N. M., La Grow, S. J., Wouldes, T., Robertson, M. C., and Campbell, A. J. (2007). Depression in older people: visual impairment and subjective ratings of health. Opt. Vis. Sci. 84, 1024–1030. doi: 10.1097/OPX.0b013e318157a6b1
Hemsley, D. R. (2005). The development of a cognitive model of schizophrenia: placing it in context. Neurosci. Biobehav. Rev. 29, 977–988. doi: 10.1016/j.neubiorev.2004.12.008
Hoffman, R. E. (2007). A social deafferentation hypothesis for induction of active schizophrenia. Schizophr. Bull. 33, 1066–1070. doi: 10.1093/schbul/sbm079
Hoffman, R. E. (2008). Auditory/Verbal hallucinations, speech perception neurocircuitry, and the social deafferentation hypothesis. Clin. EEG Neurosci. 39, 87–90. doi: 10.1177/155005940803900213
Hohl, C. M., Dankoff, J., Colacone, A., and Afilalo, M. (2001). Polypharmacy, adverse drug-related events, and potential adverse drug interactions in elderly patients presenting to an emergency department. Ann. Emerg. Med. 38, 666–671. doi: 10.1067/mem.2001.119456
Honings, S., Drukker, M., Groen, R., and van Os, J. (2016). Psychotic experiences and risk of self-injurious behaviour in the general population: a systematic review and meta-analysis. Psychol. Med. 46, 237–251. doi: 10.1017/s0033291715001841
Hovstadius, B., and Petersson, G. (2013). The impact of increasing polypharmacy on prescribed drug expenditure-a register-based study in Sweden 2005-2009. Health Policy 109, 166–174. doi: 10.1016/j.healthpol.2012.09.005
Hur, Y. M., Cherny, S. S., and Sham, P. C. (2012). Heritability of hallucinations in adolescent twins. Psychiatry Res. 199, 98–101. doi: 10.1016/j.psychres.2012.04.024
Jardri, R., Bartels-Velthuis, A. A., Debbane, M., Jenner, J. A., Kelleher, I., Dauvilliers, Y., et al. (2014). From phenomenology to neurophysiological understanding of hallucinations in children and adolescents. Schizophr. Bull. 40(Suppl. 4), S221–S232. doi: 10.1093/schbul/sbu029
Johns, L. C., Kompus, K., Connell, M., Humpston, C., Lincoln, T. M., Longden, E., et al. (2014). Auditory verbal hallucinations in persons with and without a need for care. Schizophr. Bull. 40, S255–S264. doi: 10.1093/schbul/sbu005
Johnson, M. K., and Raye, C. L. (1981). Reality monitoring. Psychol. Rev. 88, 67–85. doi: 10.1037/0033-295X.88.1.67
Jyrkka, J., Enlund, H., Lavikainen, P., Sulkava, R., and Hartikainen, S. (2011). Association of polypharmacy with nutritional status, functional ability and cognitive capacity over a three-year period in an elderly population. Pharmacoepidemiol. Drug Saf. 20, 514–522. doi: 10.1002/pds.2116
Kanemoto, M., Asai, T., Sugimori, E., and Tanno, Y. (2013). External misattribution of internal thoughts and proneness to auditory hallucinations: the effect of emotional valence in the Deese-Roediger-McDermott paradigm. Front. Hum. Neurosci. 7:351. doi: 10.3389/fnhum.2013.00351
Keen, C., Murray, C. D., and Payne, S. (2013). A qualitative exploration of sensing the presence of the deceased following bereavement. Mortality 18, 339–357. doi: 10.1080/13576275.2013.819320
Kim, H. J., Lee, H. J., An, S. Y., Sim, S., Park, B., Kim, S. W., et al. (2015). Analysis of the prevalence and associated risk factors of tinnitus in adults. PLoS ONE 10:e0127578. doi: 10.1371/journal.pone.0127578
Kim, K. W., Kang, S.-H., Yoon, I.-Y., Lee, S. D., Ju, G., Han, J. W., et al. (2017). Prevalence and clinical characteristics of insomnia and its subtypes in the Korean elderly. Arch. Gerontol. Geriatr. 68, 68–75. doi: 10.1016/j.archger.2016.09.005
Kråkvik, B., Larøi, F., Kalhovde, A. M., Hugdahl, K., Kompus, K., Salvesen, O., et al. (2015). Prevalence of auditory verbal hallucinations in a general population: a group comparison study. Scand. J. Psychol. 56, 508–515. doi: 10.1111/sjop.12236
Lai, S., Bruce, V., and Collerton, D. (2016). Visual hallucinations in older people: appraisals but not content or phenomenology influence distress. Behav. Cogn. Psychother. 44, 705–710. doi: 10.1017/S1352465815000727
Lapid, M. I., Burton, M. C., Chang, M. T., Rummans, T. A., Cha, S. S., Leavitt, J. A., et al. (2013). Clinical phenomenology and mortality in Charles Bonnet syndrome. J. Geriatr. Psychiatry Neurol. 26, 3–9. doi: 10.1177/0891988712473800
Larøi, F., DeFruyt, F., van Os, J., Aleman, A., and Van der Linden, M. (2005). Associations between hallucinations and personality structure in a non-clinical sample: comparison between young and elderly samples. Pers. Individ. Dif. 39, 189–200. doi: 10.1016/j.paid.2005.01.001
Larøi, F., Sommer, I. E., Blom, J. D., Fernyhough, C., ffytche, D. H., Hugdahl, K., et al. (2012). The characteristic features of auditory verbal hallucinations in clinical and nonclinical groups: state-of-the-art overview and future directions. Schizophr. Bull. 38, 724–733. doi: 10.1093/schbul/sbs061
Larøi, F., Van der Linden, M., and Marczewski, P. (2004). The effects of emotional salience, cognitive effort and meta-cognitive beliefs on a reality monitoring task in hallucination-prone subjects. Br. J. Clin. Psychol. 43(Pt 3), 221–233. doi: 10.1348/0144665031752970
Launay, G., and Slade, P. (1981). The measurement of hallucinatory predisposition in male and female prisoners. Pers. Individ. Dif. 2, 221–234. doi: 10.1016/0191-8869(81)90027-1
Lenka, A., Arumugham, S. S., Christopher, R., and Pal, P. K. (2016). Genetic substrates of psychosis in patients with Parkinson's disease: a critical review. J. Neurol. Sci. 364, 33–41. doi: 10.1016/j.jns.2016.03.005
Lindstrõm, T. C. (1995). Experiencing the presence of the dead: discrepancies in “the sensing experience” and their psychological concomitants. OMEGA J. Death Dying 31, 11–21. doi: 10.2190/FRWJ-U2WM-V689-H30K
Linszen, M. M., Brouwer, R. M., Heringa, S. M., and Sommer, I. E. (2016). Increased risk of psychosis in patients with hearing impairment: Review and meta-analyses. Neurosci. Biobehav. Rev. 62, 1–20. doi: 10.1016/j.neubiorev.2015.12.012
Llorca, P. M., Pereira, B., Jardri, R., Chereau-Boudet, I., Brousse, G., Misdrahi, D., et al. (2016). Hallucinations in schizophrenia and Parkinson's disease: an analysis of sensory modalities involved and the repercussion on patients. Sci. Rep. 6:38152. doi: 10.1038/srep38152
Lopez-Escamez, J. A., Bibas, T., Cima, R. F. F., Van de Heyning, P., Knipper, M., Mazurek, B., et al. (2016). Genetics of tinnitus: an emerging area for molecular diagnosis and drug development. Front. Neurosci. 10:377. doi: 10.3389/fnins.2016.00377
Lustig, C., Hasher, L., and Zacks, R. T. (2007). “Inhibitory deficits theory: Recent development in a “new view”.” in Inhibition in Cognition, eds D. S. Gorfein and C. M. McLeod (Washington, DC: American Psychological Association), 145–162.
Lyketsos, C. G., Steinberg, M., Tschanz, J. T., Norton, M. C., Steffens, D. C., and Breitner, J. C. (2000). Mental and behavioral disturbances in dementia: findings from the Cache County Study on Memory in Aging. Am. J. Psychiatry 157, 708–714. doi: 10.1176/appi.ajp.157.5.708
Maher, R. L., Hanlon, J., and Hajjar, E. R. (2014). Clinical consequences of polypharmacy in elderly. Expert Opin. Drug Saf. 13, 57–65. doi: 10.1517/14740338.2013.827660
Mattis, J., and Sehgal, A. (2016). Circadian rhythms, sleep, and disorders of aging. Trends Endocrinol. Metabol. 27, 192–203. doi: 10.1016/j.tem.2016.02.003
McGrath, J. J., Saha, S., Al-Hamzawi, A. O., Alonso, J., Andrade, L., Borges, G., et al. (2016). Age of onset and lifetime projected risk of psychotic experiences: cross-national data from the world mental health survey. Schizophr. Bull. 42, 933–941. doi: 10.1093/schbul/sbw011
Miner, B., and Kryger, M. H. (2017). Sleep in the aging population. Sleep Med. Clin. 12, 31–38. doi: 10.1016/j.jsmc.2016.10.008
Mitchell, K. J., Johnson, M. K., Raye, C. L., and D'Esposito, M. (2000). fMRI evidence of age-related hippocampal dysfunction in feature binding in working memory1. Cogn. Brain Res. 10, 197–206. doi: 10.1016/S0926-6410(00)00029-X
Miyata, S., Noda, A., Iwamoto, K., Kawano, N., Okuda, M., and Ozaki, N. (2013). Poor sleep quality impairs cognitive performance in older adults. J. Sleep Res. 22, 535–541. doi: 10.1111/jsr.12054
Monk, T. H., Germain, A., and Reynolds, C. F. (2008). Sleep disturbance in bereavement. Psychiatr. Ann. 38, 671–675.
Monti, J. M., and Monti, D. (2005). Sleep disturbance in schizophrenia. Int. Rev. Psychiatry 17, 247–253. doi: 10.1080/09540260500104516
Morrison, A. P. (2005). “Psychosis and the phenomenon of unwanted intrusive thoughts,” in Intrusive Thoughts in Clinical Disorders: Theory, Research, and Treatment, ed D. A. Clark (New York, NY: The Guilford Press), 175–198.
Morrison, A. P., Wells, A., and Nothard, S. (2000). Cognitive factors in predisposition to auditory and visual hallucinations. Br. J. Clin. Psychol. 39 (Pt 1), 67–78. Available online at: http://www.brown.uk.com/schizophrenia/morrison.pdf
Mudar, R. A., and Husain, F. T. (2016). Neural alterations in acquired age-related hearing loss. Front. Psychol. 7:828. doi: 10.3389/fpsyg.2016.00828
Nicolaisen, M., and Thorsen, K. (2014). Who are lonely? loneliness in different age groups (18–81 years old), using two measures of loneliness. Int. J. Aging Hum. Dev. 78, 229–257. doi: 10.2190/AG.78.3.b
Oh, Y. S., Lee, J. E., Lee, P. H., and Kim, J. S. (2015). Neuropsychiatric symptoms in Parkinson's disease dementia are associated with increased caregiver burden. J. Mov. Disord. 8, 26–32. doi: 10.14802/jmd.14019
Ohayon, M. M. (2000). Prevalence of hallucinations and their pathological associations in the general population. Psychiatry Res. 97, 153–164. doi: 10.1016/S0165-1781(00)00227-4
Okura, T., Plassman, B. L., Steffens, D. C., Llewellyn, D. J., Potter, G. G., and Langa, K. M. (2011). Neuropsychiatric symptoms and the risk of institutionalization and death: the aging, demographics, and memory study. J. Am. Geriatr. Soc. 59, 473–481. doi: 10.1111/j.1532-5415.2011.03314.x
Östling, S., and Skoog, I. (2002). Psychotic symptoms and paranoid ideation in a nondemented population–based sample of the very old. Arch. Gen. Psychiatry 59, 53–59. doi: 10.1001/archpsyc.59.1.53
Owen, P. R. (2012). Portrayals of schizophrenia by entertainment media: a content analysis of contemporary movies. Psychiatr. Serv. 63, 655–659. doi: 10.1176/appi.ps.201100371
Pagonabarraga, J., Martinez-Horta, S., Fernandez de Bobadilla, R., Perez, J., Ribosa-Nogue, R., Marin, J., et al. (2016). Minor hallucinations occur in drug-naive Parkinson's disease patients, even from the premotor phase. Mov. Disord. 31, 45–52. doi: 10.1002/mds.26432
Pang, L. (2016). Hallucinations experienced by visually impaired: charles bonnet syndrome. Opt. Vis. Sci. 93, 1466–1478. doi: 10.1097/opx.0000000000000959
Park, D. C., and Reuter-Lorenz, P. (2009). The adaptive brain: aging and neurocognitive scaffolding. Annu. Rev. Psychol. 60, 173–196. doi: 10.1146/annurev.psych.59.103006.093656
Paulik, G., Badcock, J. C., and Maybery, M. T. (2007). Poor intentional inhibition in individuals predisposed to hallucinations. Cogn. Neuropsychiatry 12, 457–470. doi: 10.1080/13546800701394329
Paulik, G., Badcock, J. C., and Maybery, M. T. (2008). Dissociating the components of inhibitory control involved in predisposition to hallucinations. Cogn. Neuropsychiatry 13, 33–46. doi: 10.1080/13546800701775683
Peelle, J. E., and Wingfield, A. (2016). The neural consequences of age-related hearing loss. Trends Neurosci. 39, 486–497. doi: 10.1016/j.tins.2016.05.001
Piolino, P., Coste, C., Martinelli, P., Mace, A. L., Quinette, P., Guillery-Girard, B., et al. (2010). Reduced specificity of autobiographical memory and aging: do the executive and feature binding functions of working memory have a role? Neuropsychologia 48, 429–440. doi: 10.1016/j.neuropsychologia.2009.09.035
Pliskin, N. H., Kiolbasa, T. A., Towle, V. L., Pankow, L., Ernest, J. T., Noronha, A., et al. (1996). Charles Bonnet syndrome: an early marker for dementia? J. Am. Geriatr. Soc. 44, 1055–1061.
Prince, M. J., Harwood, R. H., Blizard, R. A., Thomas, A., and Mann, A. H. (1997). Social support deficits, loneliness and life events as risk factors for depression in old age. The Gospel Oak Project VI. Psychol. Med. 27, 323–332.
Qato, D. M., Alexander, G. C., Conti, R. M., Johnson, M., Schumm, P., and Lindau, S. T. (2008). Use of prescription and over-the-counter medications and dietary supplements among older adults in the United States. JAMA 300, 2867–2878. doi: 10.1001/jama.2008.892
Qualter, P., Vanhalst, J., Harris, R., Van Roekel, E., Lodder, G., Bangee, M., et al. (2015). Loneliness across the life span. Perspect. Psychol. Sci. 10, 250–264. doi: 10.1177/1745691615568999
Rambhade, S., Chakarborty, A., Shrivastava, A., Patil, U. K., and Rambhade, A. (2012). A survey on polypharmacy and use of inappropriate medications. Toxicol. Int. 19, 68–73. doi: 10.4103/0971-6580.94506
Rast, P. (2011). Verbal knowledge, working memory, and processing speed as predictors of verbal learning in older adults. Dev. Psychol. 47, 1490–1498. doi: 10.1037/a0023422
Rawal, S., Hoffman, H. J., Bainbridge, K. E., Huedo-Medina, T. B., and Duffy, V. B. (2016). Prevalence and risk factors of self-reported smell and taste alterations: results from the 2011-2012 US National Health and Nutrition Examination Survey (NHANES). Chem. Senses 41, 69–76. doi: 10.1093/chemse/bjv057
Rees, W. D. (1971). The Hallucinations of Widowhood. Br. Med. J. 4, 37–41. doi: 10.1136/bmj.4.5778.37
Reeve, S., Sheaves, B., and Freeman, D. (2015). The role of sleep dysfunction in the occurrence of delusions and hallucinations: a systematic review. Clin. Psychol. Rev. 42, 96–115. doi: 10.1016/j.cpr.2015.09.001
Reuter-Lorenz, P. A., and Park, D. C. (2014). How does it STAC up? revisiting the scaffolding theory of aging and cognition. Neuropsychol. Rev. 24, 355–370. doi: 10.1007/s11065-014-9270-9
Roberts, K. L., and Allen, H. A. (2016). Perception and cognition in the ageing brain: a brief review of the short- and long-term links between perceptual and cognitive decline. Front. Aging Neurosci. 8:39. doi: 10.3389/fnagi.2016.00039
Roberts, L. E., Eggermont, J. J., Caspary, D. M., Shore, S. E., Melcher, J. R., and Kaltenbach, J. A. (2010). Ringing ears: the neuroscience of tinnitus. J. Neurosci. 30, 14972–14979. doi: 10.1523/JNEUROSCI.4028-10.2010
Ronald, A. (2015). Recent quantitative genetic research on psychotic experiences: new approaches to old questions. Curr. Opin. Behav. Sci. 2, 81–88. doi: 10.1016/j.cobeha.2014.10.001
Rossi, M. I., Young, A., Maher, R., Rodriguez, K. L., Appelt, C. J., Perera, S., et al. (2007). Polypharmacy and health beliefs in older outpatients. Am. J. Geriatr. Pharmacother. 5, 317–323. doi: 10.1016/j.amjopharm.2007.12.001
Russell, G., Harper, R., Allen, H., Baldwin, R., and Burns, A. (2017). Cognitive impairment and Charles Bonnet syndrome: a prospective study. Int. J. Geriatr. Psychiatry. doi: 10.1002/gps.4665. [Epub ahead of print].
Schneider, J., Gopinath, B., McMahon, C., Teber, E., Leeder, S. R., Wang, J. J., et al. (2012). Prevalence and 5-year incidence of dual sensory impairment in an older Australian population. Ann. Epidemiol. 22, 295–301. doi: 10.1016/j.annepidem.2012.02.004
Sedley, W., Friston, K. J., Gander, P. E., Kumar, S., and Griffiths, T. D. (2016). An integrative tinnitus model based on sensory precision. Trends Neurosci. 39, 799–812. doi: 10.1016/j.tins.2016.10.004
Sheaves, B., Bebbington, P. E., Goodwin, G. M., Harrison, P. J., Espie, C. A., Foster, R. G., et al. (2016). Insomnia and hallucinations in the general population: findings from the 2000 and 2007 British Psychiatric Morbidity Surveys. Psychiatry Res. 241, 141–146. doi: 10.1016/j.psychres.2016.03.055
Siegel, R. K. (1984). Hostage hallucinations. Visual imagery induced by isolation and life-threatening stress. J. Nerv. Ment. Dis. 172, 264–272.
Sieradzka, D., Power, R. A., Freeman, D., Cardno, A. G., Dudbridge, F., and Ronald, A. (2015). Heritability of individual psychotic experiences captured by common genetic variants in a community sample of adolescents. Behav. Genet. 45, 493–502. doi: 10.1007/s10519-015-9727-5
Sommer, I. E., Daalman, K., Rietkerk, T., Diederen, K. M., Bakker, S., Wijkstra, J., et al. (2010). Healthy individuals with auditory verbal hallucinations; who are they? psychiatric assessments of a selected sample of 103 subjects. Schizophr. Bull. 36, 633–641. doi: 10.1093/schbul/sbn130
Soriano, M. F., Jimenez, J. F., Roman, P., and Bajo, M. T. (2009). Intentional inhibition in memory and hallucinations: directed forgetting and updating. Neuropsychology 23, 61–70. doi: 10.1037/a0013739
Soulas, T., Cleret de Langavant, L., Monod, V., and Fenelon, G. (2016). The prevalence and characteristics of hallucinations, delusions and minor phenomena in a non-demented population sample aged 60 years and over. Int. J. Geriatr. Psychiatry 31, 1322–1328. doi: 10.1002/gps.4437
Stahl, S. M. (2016). Mechanism of action of pimavanserin in Parkinson's disease psychosis: targeting serotonin 5HT2A and 5HT2C receptors. CNS Spectr. 21, 271–275. doi: 10.1017/s1092852916000407
Stanley, I. H., Hom, M. A., Rogers, M. L., Hagan, C. R., and Joiner, T. E. Jr. (2016). Understanding suicide among older adults: a review of psychological and sociological theories of suicide. Aging Ment. Health 20, 113–122. doi: 10.1080/13607863.2015.1012045
Steptoe, A., Shankar, A., Demakakos, P., and Wardle, J. (2013). Social isolation, loneliness, and all-cause mortality in older men and women. Proc. Natl. Acad. Sci.U.S.A. 110, 5797–5801. doi: 10.1073/pnas.1219686110
Stirling, J., Barkus, E., and Lewis, S. (2007). Hallucination proneness, schizotypy and meta-cognition. Behav. Res. Ther. 45, 1401–1408. doi: 10.1016/j.brat.2006.06.003
Subramaniam, M., Abdin, E., Vaingankar, J., Picco, L., Shahwan, S., Jeyagurunathan, A., et al. (2016). Prevalence of psychotic symptoms among older adults in an Asian population. Int. Psychogeriatr. 28, 1211–1220. doi: 10.1017/s1041610216000399
Targum, S. D. (2001). Treating psychotic symptoms in elderly patients. Prim. Care Companion J. Clin. Psychiatry 3, 156–163.
Teunisse, R. J., and Olde Rikkert, M. G. (2012). Prevalence of musical hallucinations in patients referred for audiometric testing. Am. J. Geriatr. Psychiatry 20, 1075–1077. doi: 10.1097/JGP.0b013e31823e31c4
Tien, A. Y. (1991). Distributions of hallucinations in the population. Soc. Psychiatry Psychiatr. Epidemiol. 26, 287–292.
Turvey, C. L., Schultz, S. K., Arndt, S., Ellingrod, V., Wallace, R., and Herzog, R. (2001). Caregiver report of hallucinations and paranoid delusions in elders aged 70 or older. Int. Psychogeriatr. 13, 241–249.
United Nations, D., Department of Economic and Social Affairs,and Population Division (2013). World Population Ageing 2013.
Varese, F., Morrison, A. P., Beck, R., Heffernan, S., Law, H., and Bentall, R. P. (2016). Experiential avoidance and appraisals of voices as predictors of voice-related distress. Br. J. Clin. Psychol. 55, 320–331. doi: 10.1111/bjc.12102
Vilhauer, R. P. (2017). Stigma and need for care in individuals who hear voices. Int. J. Soc. Psychiatry 63, 5–13. doi: 10.1177/0020764016675888
Wallhäusser-Franke, E., Brade, J., Balkenhol, T., D'Amelio, R., Seegmüller, A., and Delb, W. (2012). Tinnitus: distinguishing between subjectively perceived loudness and tinnitus-related distress. PLoS ONE 7:e34583. doi: 10.1371/journal.pone.0034583
Wallhäusser-Franke, E., Schredl, M., and Delb, W. (2013). Tinnitus and insomnia: Is hyperarousal the common denominator? Sleep Med. Rev. 17, 65–74. doi: 10.1016/j.smrv.2012.04.003
Waters, F. A. V., Allen, P., Aleman, A., Fernyhough, C., Woodward, T. S., Badcock, J. C., et al. (2012). Auditory hallucinations in schizophrenia and nonschizophrenia populations: a review and integrated model of cognitive mechanisms. Schizophr. Bull. 38, 683–693. doi: 10.1093/schbul/sbs045
Waters, F. A. V., Badcock, J. C., and Maybery, M. T. (2003). Revision of the factor structure of the Launay-Slade Hallucination Scale (LSHS-R). Pers. Individ. Dif. 35, 1351–1357. doi: 10.1016/S0191-8869(02)00354-9
Weiss, R. S. (1973). Loneliness: The Experience of Emotional and Social Isolation. Cambridge, MA: The MIT Press.
Wiener, L., Aikin, A., Gibbons, M. B., and Hirschfeld, S. (1996). Visions of those who left too soon. Am. J. Nurs. 96, 57–61.
Wilson, R. S., Krueger, K. R., Arnold, S. E., Schneider, J. A., Kelly, J. F., Barnes, L. L., et al. (2007). Loneliness and risk of Alzheimer Disease. Arch. Gen. Psychiatry 64, 234–240. doi: 10.1001/archpsyc.64.2.234
Wood, K. A., Harris, M. J., Morreale, A., and Rizos, A. L. (1988). Drug-induced psychosis and depression in the elderly. Psychiatr. Clin. North Am. 11, 167–193.
Woodward, T. S., Jung, K., Hwang, H., Yin, J., Taylor, L., Menon, M., et al. (2014). Symptom dimensions of the psychotic symptom rating scales in psychosis: a multisite study. Schizophr. Bull. 40(Suppl. 4), S265–S274. doi: 10.1093/schbul/sbu014
Wulff, K., Gatti, S., Wettstein, J. G., and Foster, R. G. (2010). Sleep and circadian rhythm disruption in psychiatric and neurodegenerative disease. Nat. Rev. Neurosci. 11, 589–599. doi: 10.1038/nrn2868
Yamamoto, J., Okonogi, K., Iwasaki, T., and Yoshimura, S. (1969). Mourning in Japan. Am. J. Psychiatry 125, 1660–1665. doi: 10.1176/ajp.125.12.1660
Keywords: hallucinations, perception, psychotic experiences, ageing, cognition, prevalence
Citation: Badcock JC, Dehon H and Larøi F (2017) Hallucinations in Healthy Older Adults: An Overview of the Literature and Perspectives for Future Research. Front. Psychol. 8:1134. doi: 10.3389/fpsyg.2017.01134
Received: 24 April 2017; Accepted: 21 June 2017;
Published: 07 July 2017.
Edited by:
Éric Laurent, Université Bourgogne Franche-Comté, FranceReviewed by:
Timo Partonen, National Institute for Health and Welfare, FinlandMahesh Menon, University of British Columbia, Canada
Copyright © 2017 Badcock, Dehon and Larøi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Johanna C. Badcock, Johanna.badcock@uwa.edu.au
Frank Larøi, frank.laroi@uib.no