 Susan G. Simpson1,2*
Susan G. Simpson1,2* Giada Pietrabissa3,4
Giada Pietrabissa3,4 Alessandro Rossi3
Alessandro Rossi3 Tahnee Seychell5
Tahnee Seychell5 Gian Mauro Manzoni3,4,5,6
Gian Mauro Manzoni3,4,5,6 Calum Munro7
Calum Munro7 Julian B. Nesci8
Julian B. Nesci8 Gianluca Castelnuovo3,4
Gianluca Castelnuovo3,4- 1School of Psychology, Social Work and Social Policy, University of South Australia, Adelaide, SA, Australia
- 2Regional Eating Disorders Unit, St. John's Hospital, NHS Lothian, Livingston, United Kingdom
- 3Psychology Research Laboratory, Ospedale San Giuseppe, IRCCS Istituto Auxologico Italiano, Verbania, Italy
- 4Department of Psychology, Catholic University of Milan, Milan, Italy
- 5Psychology Department, University of Adelaide, Adelaide, SA, Australia
- 6Faculty of Psychology, eCampus University, Como, Italy
- 7Department of Psychiatry, Royal Edinburgh Hospital, University of Edinburgh, Edinburgh, United Kingdom
- 8Spectrum: Personality Disorder Service, Victoria, Melbourne, VIC, Australia
Objective: The aim of this study was to examine the psychometric properties and factorial structure of the Schema Mode Inventory for Eating Disorders (SMI-ED) in a disordered eating population.
Method: 573 participants with disordered eating patterns as measured by the Eating Disorder Examination Questionnaire (EDE-Q) completed the 190-item adapted version of the Schema Mode Inventory (SMI). The new SMI-ED was developed by clinicians/researchers specializing in the treatment of eating disorders, through combining items from the original SMI with a set of additional questions specifically representative of the eating disorder population. Psychometric testing included Confirmatory Factor Analysis (CFA) and internal consistency (Cronbach's α). Multivariate Analyses of Covariance (MANCOVA) was also run to test statistical differences between the EDE-Q subscales on the SMI-ED modes, while controlling for possible confounding variables.
Results: Factorial analysis confirmed an acceptable 16-related-factors solution for the SMI-ED, thus providing preliminary evidence for the adequate validity of the new measure based on internal structure. Concurrent validity was also established through moderate to high correlations on the modes most relevant to eating disorders with EDE-Q subscales. This study represents the first step in creating a psychometrically sound instrument for measuring schema modes in eating disorders, and provides greater insight into the relevant schema modes within this population.
Conclusion: This research represents an important preliminary step toward understanding and labeling the schema mode model for this clinical group. Findings from the psychometric evaluation of SMI-ED suggest that this is a useful tool which may further assist in the measurement and conceptualization of schema modes in this population.
Introduction
Schema Therapy (ST) was developed to address long-standing psychological disorders and entrenched personality traits (Young et al., 2003), and a growing number of studies have demonstrated its effectiveness (Masley et al., 2012; Jacob and Arntz, 2013; de Klerk et al., 2016). ST is based on the notion that Early Maladaptive Schemas (EMS) develop as a result of the interaction between temperament and unmet core emotional needs during childhood. EMS consist of patterns of memories, cognitions, emotions and physical reactions that drive coping mechanisms, and become increasingly maladaptive over time. Whereas EMS refer to stable “traits,” schema modes represent the moment-to-moment “states” and coping responses that we all experience. Schema modes are traditionally grouped into four main categories: (1) Innate Child Modes, that represent the emotions experienced in the context of unmet needs; (2) Internalized/Introject [Parent] Modes, which represent the internalized messages from childhood, including parents, teachers, other caregivers, and culture; (3) Coping Modes, which are the survival mechanisms developed during childhood and adolescence to cope with unmet emotional needs, and (4) Adaptive (Healthy) Modes. In ST, the emphasis is on developing healthy coping mechanisms that facilitate the process of developing adaptive ways of meeting one's interpersonal and emotional needs, whilst weakening maladaptive modes and associated EMS (Young et al., 2003).
The (124-item) Schema Mode Inventory (SMI) (Young et al., 2007) was developed to measure schema modes through self-report. A shortened (118 item) version of the original SMI (Young et al., 2007) was validated within a sample of healthy controls, axis I and axis II patients (Lobbestael et al., 2010) and found to have acceptable internal consistency and test-rest reliability. A 14-factor model emerged, consisting of: five child modes, five dysfunctional coping modes, two dysfunctional parent modes and the adaptive Healthy Adult mode. The SMI was primarily developed to measure schema modes in the Borderline and Antisocial PDs, however, it has recently successfully been adapted (SMI-2) to more appropriately measure schema modes as they manifest within Cluster C and paranoid, histrionic and narcissistic PDs (Bamelis et al., 2011). Previous studies have highlighted the need for exploratory research that examines schema modes within specific clinical groups in order to begin to delineate the profiles and new sub-modes that may be identified in these populations (Lobbestael et al., 2010).
A significant proportion of those with Eating Disorders (EDs) do not respond or do not complete treatment (Waller et al., 2009) and go on to develop chronic symptoms (Keller et al., 2006; Castelnuovo et al., 2011). Rigid personality traits are common in this population, with up to 69% of the ED population meeting criteria for a co-morbid personality disorder (PD) (Blinder et al., 2006), a factor that has been shown to adversely affect treatment outcomes (Grilo et al., 2007; Sallet et al., 2010; Farstad et al., 2016). In spite of improved outcomes with Enhanced CBT (CBT-E) (Fairburn et al., 2008; Castelnuovo et al., 2017; Pietrabissa et al., 2017), it remains less effective at addressing rigid co-morbid personality characteristics, such as perfectionism and avoidant traits (Byrne et al., 2011). The Schema Therapy Model for EDs has evolved over the past 10 years (Waller, 2003; Waller et al., 2007; Simpson, 2012), prompted by the need for therapeutic approaches that address deeper level cognitions and entrenched behaviors that do not respond to first-line treatments (Waller, 1997; Waller and Kennerley, 2003; Sorgente et al., 2017).
Preliminary research suggests that Schema Therapy may be highly suited to the needs of those with EDs, particularly those with high levels of complexity or chronicity (Simpson et al., 2010; Simpson and Slowey, 2011; McIntosh et al., 2016). This approach goes beyond maintenance factors to address the core schema-level beliefs that underpin ED psychopathology. Preliminary studies in this area suggest that those with EDs may experience significantly higher levels of maladaptive modes than community samples (Voderholzer et al., 2014; Talbot et al., 2015). Preliminary conceptualizations of the ED population suggest that all three coping styles (avoidance, surrender and overcompensation) play a significant role in driving and perpetuating ED behaviors (Waller and Kennerley, 2003; Simpson, 2012). Recent evidence supports the notion that maladaptive coping modes mediate the relationship between perceived negative parenting and eating disorder symptoms (Sheffield et al., 2009; Brown et al., 2016). In particular, the “Eating Disorder Overcontroller (Coping) Mode (EDO)” has been proposed as highly relevant to the ED population in recent theoretical conceptualizations (Simpson, 2012, 2016), and supported by findings from a recent study (Brown et al., 2016). This mode is theoretically linked to the Unrelenting Standards schema, and functions as a form of overcompensation, whereby perfectionism, achievement, and competitiveness, often focused on the body and eating patterns, are utilized to provide distance from underlying feelings of vulnerability and distress by generating a sense of competence, omnipotence and control.
The EDO has some parallels with the “Perfectionistic Overcontroller” mode that has been identified as highly relevant within Obsessive-Compulsive Personality Disorder (Bamelis et al., 2011), which has high comorbidity with EDs (Halmi et al., 2005). However, in eating disorders, it is proposed that the EDO has a more substantial focus on controlling the body, attaining a state of purity, and an emotional “high” associated with overcoming basic human needs (Simpson, 2016). Although the EDO is tapping into a similar construct to that of other clinical perfectionism measures, it is focused on specific characteristics and behaviors of the ED population, and focused on a broader concept than that measured by these other scales. In addition, the Helpless Surrenderer has been proposed as a mode which has particular relevance to those with EDs. In this mode the patient avoids expressing vulnerability or emotional needs directly, but instead seeks help passively, such as through withdrawal, complaint, or seeking “quick-fix” solutions. This mode may be mistaken for the Vulnerable Child mode due to what appears to be overt distress. It is hypothesized that this mode may be closely linked with Dependence, Emotional Deprivation, and Subjugation schemas (Simpson, 2016).
The purpose of this study was to develop a psychometrically sound adapted version of the Schema Mode Inventory in order to facilitate more precise measurement of mode states within a population with self-reported disordered eating behaviors. The result, a new Schema Mode Inventory for Eating Disorders (SMI-ED) would contribute to the ST conceptualization of schema modes in this sample. More specifically, this study aimed to conduct a Confirmatory Factorial Analysis (CFA) in order to examine the structure and psychometric properties of the SMI-ED, and to determine the internal reliability of its subscales. The relationship between eating disorder symptoms (restraint, binge-eating, and purging) and schema modes was also explored. In addition, we investigated whether specific EDE-Q subscales discriminated schema modes.
Materials and Methods
Participants
Between February 2014 and April 2015 participants were recruited through advertisements placed on Facebook and websites of various local and international not-for-profit eating disorder organizations and support groups. Websites that advertised the survey to members included the Butterfly Association in Australia, and BEAT in the United Kingdom. Specifically, a small paragraph invited those with symptoms of disordered eating to take part in the study. In addition, flyers were placed around University campuses and in clinical waiting rooms of local eating disorder services in South Australia. The first page of the survey provided participants with details of the study and ethics approval to enable them to give informed consent.
The study was open to individuals aged between 18 and 70, who were English-speaking with disordered eating. Selection criteria were chosen in order to capture a wide sample of participants with any disordered eating, including those with subthreshold eating disorders. Our screening criteria were based on previous research (Mond et al., 2004, 2006) based on a sample of young Australian women. We used their 75th percentile as a cut-point for the global Eating Disorder Examination Questionnaire (EDE-Q 6.0) (Fairburn and Beglin, 2008) score, indicating “probable eating disorder case.” However, we extended their criteria to additionally include participants who reached the 75th percentile on any of the 4 EDE-Q subscales. Specifically, to be included in the final data set, participants were required to meet at least one of the 2 inclusion criteria: (Young et al., 2003) a global EDE-Q score of 2.3 or higher, in conjunction with repeated bingeing episodes and/or use of exercise or other compensatory behavior over the past 4 weeks (Mond et al., 2004, 2006); and/or (de Klerk et al., 2016) a mean score at or above the 75 percentile on at least one of the EDE-Q subscales—Restraint: 2.2; Eating Concern: 1; Weight Concern: 2.8; Shape Concern: 3.5.
A total of 672 people participated in the survey. Of these, 45 participants did not complete the survey and were excluded from the final analyses. Of the remaining 573 participants, 519 met all of the recommended inclusion criteria of the study, and 54 scored at or above the 75% percentile rank on at least one EDE-Q subscale. The final sample comprised 573 participants [33 males (5.8%) and 540 females (94.2%)] aged from 18 to 61 years (mean = 27.08, SD = 8.84, 95%CImean = from 26.35 to 27.81). Participants' self-reported BMI ranged from 12.07 to 85.44 (mean = 23.43; SD = 8.60), with 25.7% of the sample under 18.5. 353 subjects were single, 100 in a de facto relationship, and 88 were married. Of the total sample, 36.1% of the total sample had been educated to at least year 12 of high school, while 28.8% were university graduates and 13.6% had a postgraduate degree. The majority of the sample was Australian (62.8%), and 93.4% of the total sample spoke English as their first language.
Of the 573 participants, 201 reported that they had been diagnosed by a mental health professional with Anorexia Nervosa (AN), 74 with Bulimia Nervosa (BN), 21 with Binge Eating Disorder (BED), and 97 with Eating Disorders Not Otherwise Specified (EDNOS). The remaining 180 participants had not received a formal diagnosis and/or had not consulted a mental health professional. Descriptive statistics are presented in Table 1. Diagnoses could not be verified by the researchers due to the online nature of this study, therefore Table 1 refers to EDE-Q subscales.
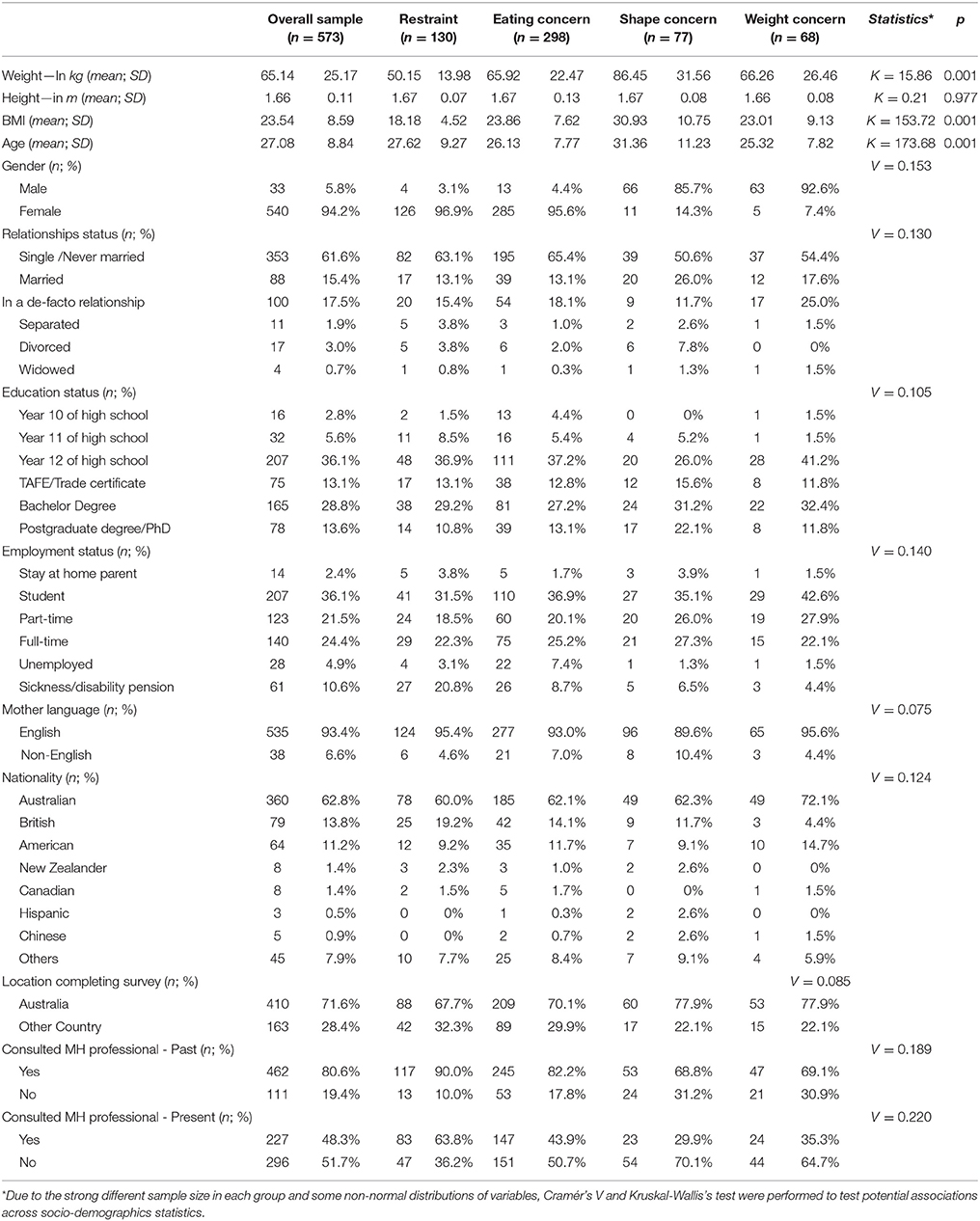
Table 1. Descriptive statistics for the EDE-Q subscales.
Sample Size Calculation
Sample size was based on Comrey and Lee's (1992) recommendation that 500 or more observations can be considered “very good” for conducting factor analyses (MacCallum et al., 1999).
Measures
Demographic Survey
Prior to commencing the questionnaire, general demographic information was collected (weight in kg; height in meters; BMI; age; gender; relationships, education and employment status; mother language; nationality; location completing survey; current or past consultation with a mental health professional). Those who were not receiving support were invited to provide contact details so that they could be contacted if it was indicated that they would benefit from treatment.
The Eating Disorder Examination Questionnaire (EDE-Q)
The EDE-Q 6.0 (Fairburn and Beglin, 2008) is a 28-item self-report measure of the range and severity of ED features. The questions concern the frequency in which the patient engages in behaviors indicative of an eating disorder over a 28-day period. The test is scored on a 7-point scale from 0 to 6, rated using four subscales (Restraint; Eating concern; Shape concern, and Weight concern) and a global score. The EDE-Q has generally received support as an adequately reliable and valid measure of eating-related pathology and specific disordered eating behaviors (Peterson et al., 2007) and the scale has moderate to strong positive correlations with the gold standard Eating Disorder Examination structured interview (Berg et al., 2011). Similarly, in the present sample, the dimensions of the EDE-Q have demonstrated acceptable internal consistency (R-α = 0.828; EC-α = 0.811; SC-α = 0.894; WC-α = 0.831; General/Total-α = 0.942).
The Schema Mode Inventory for Eating Disorders (SMI-ED)
The item-pool for the new SMI-ED was developed through combining selected items from the original SMI (Young et al., 2007), with a set of additional items (Table 2). The SMI-ED was constructed based on items derived from 3 main sources: (1) Items from the original SMI that were considered most relevant to those with EDs (n = 117); (2) A new set of items (n = 73) that were generated by clinicians/researchers specialized in the treatment of eating disorders, two psychologists (authors SS and JN) and one psychiatrist (author CM). All had experience in the field ranging from 6 to 20 years. Items were based on typical self-statements made by patients across all diagnostic groups and the Schema Therapy theoretical conceptualization of eating disorders (Simpson, 2016), and (3) Items put forward by patients with EDs who volunteered to contribute. Four patients (two with a diagnosis of AN, one with BED and one with BN) suggested items that were relevant to their most commonly experienced emotional and coping states. The patients also contributed to the way in which items were clustered together under specific mode categories. This was particularly the case for the “Helpless Surrenderer” mode, whereby the items were clustered together based on their experience of the different elements of this mode.
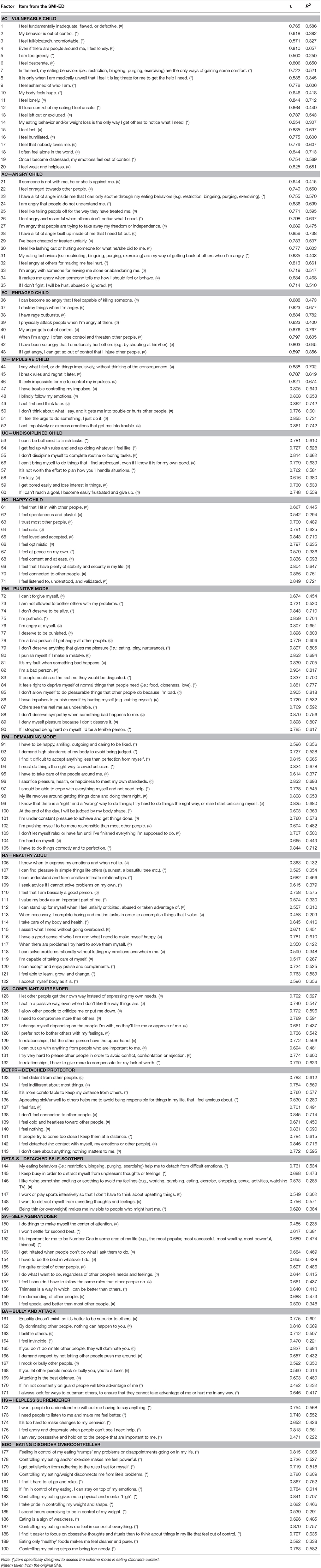
Table 2. Factor loadings (λ) and the explained variance (R2) of the SMI-ED.
The Self Aggrandizer mode was adapted by adding one item that specifically mentions using thinness as a way of feeling superior to others. In addition, an existing item was adapted to include thinness as a way of being “Number One,” where the original scale just referred to success, popularity, wealth and power. These adaptations were designed to highlight the specific ways in which ED behaviors may be used by some to compensate for an underlying sense of inadequacy, whereby their superiority in this specific regard is perceived as protection from future risk of humiliation or shame. Bully and Attack mode largely consisted of items from the original SMI, with three additional items generated by patients with EDs who were involved in developing the SMI-ED, linked to the need to be on guard and outsmart others to ensure that they don't take advantage. When piloting the new scale, patients indicated that they preferred the wording of “I am invincible” to “I am invulnerable,” even though the concept is basically similar. The patients identified with the concept of invincibility as a coping solution to avoid underlying vulnerability. Controlling and dominating others is also used as a way of achieving invincibility (to mask underlying vulnerability). This concept of invincibility is a thread that seems to connect all overcompensatory coping modes in eating disorders.
The Helpless Surrenderer Mode included 5 new items, and is conceptualized as a “surrender” coping mode whereby the person feels dependent on others to meet their emotional needs without taking the risk of explicitly expressing authentic vulnerability. This mode has a feel of helplessness, whereby the person wants others to understand them, whilst being resigned to the belief that others will never meet their needs (“I need people to listen to me and make me feel better”; “I want people to understand me without me having to say anything”). This coping mode appears to be driven by an acute underlying sense of feeling emotionally deprived whereby needs for emotional attunement, empathy and guidance have not been adequately met. In this mode, they often feel “stuck” and unable to find other [healthy] ways of coping, due to an overwhelming sense of impotence (“It's too hard to make changes to my behavior”). In this mode, the person may cling and act in a possessive way to cope with the pain of the unmet need, but feels unable to ask for emotional needs to be met in an open or direct way (“I am very possessive and hold on to the people that are important to me”). They express frustration that others won't provide solutions and relief from emotional suffering, whilst avoiding genuine engagement and connection (“I feel angry and desperate when people can't see I need help”) (Simpson, 2016).
Through a screening process highly similar items were identified; those items most representative of the ED population under consideration were retained and any redundant questions removed. This resulted in a 190 item SMI-ED with 16 different modes clustered thematically (Table 2): (A) five innate child modes; (B) two maladaptive [internalized/introject] modes; (C) seven maladaptive coping modes; and (D) two healthy factors. Specifically, the three child modes are: (1) Vulnerable Child—VC; (2) Angry Child– AC; (3) Enraged Child—EC; (4) Impulsive Child—IC; and (5) Undisciplined Child—UC. The two maladaptive (internalized/introject) modes are: (6) Punitive mode—PM and (7) Demanding Mode—DM. The 12 modes were comprised of both original and new statements. Two modes (Impulsive Child—IC and Enraged Child—EC) only included items retrieved from the original version of the SMI, while the Helpless Surrenderer—HS and the Eating Disorder Overcontroller—EDO modes exclusively consisted of new ED-specific statements. For each item, participants responded on a 6-point scale ranging from 1 (“never or hardly ever”) to 6 (“all of the time”) regarding how often they believe or feel the statement to be true for them. The items of the SMI-ED were presented clustered by mode rather than in random order. In fact, while it has been previously argued that randomizing items prevents response bias (Lobbestael et al., 2010), recent findings indicated that clustering items results in more accurate measurement of schema modes as it allows participants to reflect upon different aspects of themselves (Marais et al., 2017). Within each mode the items were randomized. Administration time for the SMI-ED was approximately 30 minutes.
The seven maladaptive coping modes are: Compliant Surrenderer—CS; (9) Helpless Surrenderer—DS; (10) Detached Protector—Det.P; (11) Detached Self-Soother—Det.S-S; (12) Self Aggrandizer—SA; (13) Bully and Attack—BA; (14) Eating Disorder Overcontroller—EDO. Finally, the functional healthy modes are: (15) Happy Child—HC and (16) Healthy Adult—HA.
The number of items between scales varies from 5 (Helpless Surrenderer–DS) to 20 (Vulnerable Child–VC). To compute the scale score for each mode, the scale sum score is divided by the number of items in that scale. The higher the score, the more frequent were the manifestations of the modes. No total score was computed.
Procedure
This study was completed entirely online and was hosted by the questionnaire tool Survey Monkey. Recruitment advertisements included a link to the information page where participants provided informed consent before commencing. At the completion of the questionnaire, participants were directed to a debrief page where they were provided with contact details for support services. This study was approved by the Human Research Ethics Committees at the University of South Australia.
Statistical Analyses
Confirmatory Factor Analysis (CFA) was performed using “lavaan” package (Rosseel, 2012; Rosseel et al., 2015) for R software [R-core project (Team RC., 2014, 2015) in order to test the factorial structural model of the SMI-ED based on prior empirical and theoretical grounds. All the other statistical analysis were carried out with SPSS software (version 20.0, SPSS Inc., Bologna, Italy) (Nie et al., 1970).
Preparation of Data for Statistical Analysis
Items' descriptive statistics revealed a non-perfect normal distribution of some indicators. No missing data was detected. Consequently, the Robust Maximum Likelihood method (MLM) (Bentler, 1995; Muthén et al., 1997; Muthén and Muthén, 1998; Hoyle, 2012) was used to estimate the model via CFA. The MLM is a “robust” variant of Maximum likelihood (Bentler, 1995) that provides robust standard errors and a Satorra-Bentler test statistic (Satorra and Bentler, 1988, 1994; Rosseel, 2012). Factor loadings were tested for statistical significance, setting the level of p at 0.005. The ratio of χ2 to the degrees of freedom (df) (Jöreskog, 1969), the Comparative Fit Index (CFI) (Bentler, 1990), the Root-Mean Square Error of Approximation (RMSEA) (Steiger and Lind, 1980; Steiger, 1990) and the Standard Root Mean square Residual (SRMR) (Bentler, 1995) were also used to assess the model fit (Barrett, 2007). A non-significant χ2 is desirable (Bentler and Bonett, 1980) and smaller χ2 values indicate a better model fit. The χ2/df ratio is considered as an easily computed measure of fit (Marsh and Hocevar, 1985; Hoyle, 2012), and a χ2/df ratio value of 3 or less indicates good fit (Wheaton et al., 1977). Comparative Fit Index (CFI) designates the amount of variance and covariance accounted by the model compared with a baseline model, without sample size dependence; values higher than 0.90 are considered good/adequate (Hu and Bentler, 1999). However, Kenny and McCoach (2003) mathematically demonstrate that the number of variables being analyzed negatively affects this fit index (Russell, 2002; Kenny and McCoach, 2003; Iacobucci, 2010). The RMSEA expresses fit per degrees of freedom of the model, with values lower than 0.08 suggesting an acceptable model fit (Hu and Bentler, 1999) and values below 0.05 indicating a good fit (Browne and Cudeck, 1990). The SRMR, derives from the residual correlation matrix, and represents the average discrepancy between correlations observed in the input matrix and those predicted by the model (Bentler, 1995; Brown, 2015). A cutoff value higher than 0.8 is considered good (Hu and Bentler, 1999; Hoyle, 2012). Cronbach's alpha was computed to measure internal consistency for each SMI-ED subscale with values al least of 0.7 deemed acceptable (Cronbach, 1951). In addition, Multivariate Analysis of Covariance (MANCOVA) was conducted to assess for possible statistical differences between the disordered eating subgroups simultaneously, as measured by the (EDE-Q), on the SMI-ED subscales, while adjusting for differences on age and past and/or present consultation with a Mental Health professional as possible confounding variables.
Results
Item analysis revealed a non-perfect normal distribution, with Kolmogorov-Smirnov and Shapiro-Wilk tests being significant (p < 0.001). Skewness ranged between −1.14 and 3.87 (meansk = 0.23, SDsk = 0.78; meansk/std.err = 2.24; SDsk/std.err = 7.61), and kurtosis ranged between −1.47 and 18.1 (meank = −0.22, SDk = 2.10; meank/std.err = −1.05; SDk/std.err = 10.32).
Results from the CFA suggest an acceptable sixteen-related-factors solution for the SMI-ED, despite not all the fix indexes achieving the desired value (Hu and Bentler, 1999). Indeed, the chi-square model for fit was statistically significant [ = 38210.465; p < 0.001] whilst the Comparative Fit Index value did not meet the threshold suggesting ideal fit [CFI > 0.90; (Hu and Bentler, 1999): CFI = 0.767]. However, the RMSEA showed a good approximation fit of the model to the data [RMSEA = 0.045 (90% CI: from 0.044 to 0.046), p (RMSEA < 0.05)= 1]. Moreover, by dividing the χ2 for the degrees of freedom (df) of the model (Jöreskog, 1969; Hu and Bentler, 1999), the proposed model is potentially acceptable (χ2/df = 2.16; <3) (Hoyle, 2012). Finally, the SRMR further suggested the goodness of model fit [SRMR = 0.077 (Hu and Bentler, 1999)].
As shown in Table 2 each item loaded significantly on the factor associated with it (p < 0.001), meanloadings = 0.727; SDloadings = 0.110; ranging from 0.350 (item #117) to 0.905 (item #85). In addition, correlations between the sixteen factors ranged from 0.082 to 0.838; meanr−factors = 0.258; SDr−factors = 0.404 (Table 3).
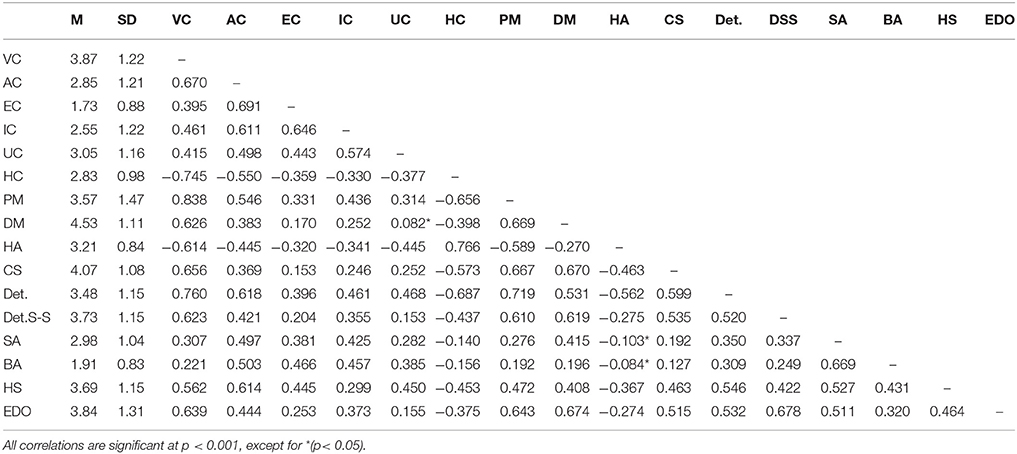
Table 3. Means, standard deviations and correlations between subscales of the Schema Mode Inventory for eating disorders (SMI-ED).
The scales had acceptable internal consistency, with coefficients ranging from 0.807 to 0.976; meanα−factors = 0.914; SDα−factors = 0.048. Specifically, the highest value was registered for the Punitive Mode subscale (0.976), followed by the Vulnerable Child (0.956), Impulsive Child (0.950), Angry Child (0.948), Demanding Mode (0.947), Eating Disorder Overcontroller (0.946), Happy Child (0.933), Detached Protector (0.932), Compliant Surrender (0.926), Enraged Child (0.915), Undisciplined Child and Healthy Adult (0.908), Self Aggrandizer and Bully and Attack (0.883), Helpless Surrenderer (0.808), and Detached Self-Soother (0.807).
Concurrent Validity: Correlation Between SMI-ED Factors and Eating Disorder Variables
Bivariate correlations calculated with direct scores indicated that all SMI-ED factors were significantly correlated (ranging from low to high levels) with EDE-Q subscales and eating disorder symptoms (Table 4). The adaptive modes (Happy Child and Healthy Adult) were negatively associated with all of the eating disorder variables.
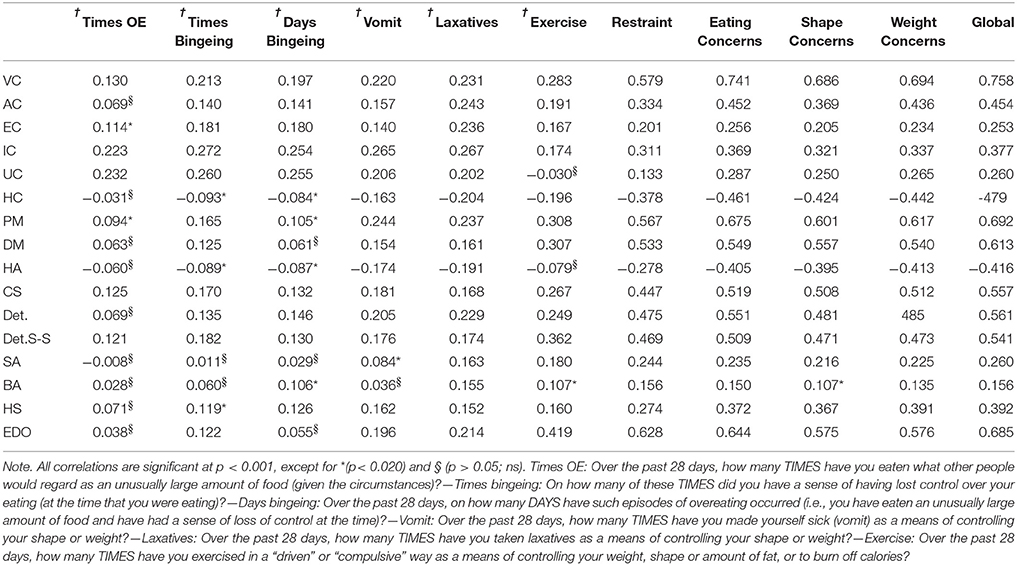
Table 4. Correlations between SMI-ED' subscales, ED Symptoms (†) and EDE-Q subscales (‡).
Mode Scores Across Disordered Eating Subscales
While controlling for age and past and/or present consultation with a Mental Health professional as possible confounding variables, Multivariate Analysis of Covariance (MANCOVA) revealed a significant difference, between disordered eating behaviors (EDE-Q subscales) on the majority of the SMI-ED subscales: Wilks's Λ = 0.693, F = 4.473, p < 0.001, η2 = 115. No differences emerged between the EDE-Q subscales for the Healthy Adult, Self-Aggrandizer, Bully and Attack, and Helpless Surrenderer modes as measured by the SMI-ED. Also, in order to test differences between groups within SMI-ED subscales, ANCOVAs with focused contrasts were conducted for each dependent variable. Results are shown in Table 5. Mean scores are shown for each EDE-Q subscale in relation to each of the schema modes. In particular, in relation to the “new” modes (Helpless Surrenderer and Eating Disorder Overcontroller), means were above the 75% percentile rank for young adult women (Mond et al., 2006) except for the Shape Concern Subscale (particularly for the Overcontroller), demonstrating the adequacy of these modes in reflecting eating disorder behaviors. In particular, the means of the new subscales were higher for Restraint, reflecting the high degree of restrictive behavior and preoccupation with food in this sample. The “Restraint” and “Eating Concern” subscales of the EDE-Q discriminated the majority of modes most representative of eating disorder populations (i.e., Impulsive Child, Punitive Parent, Demanding Parent, Detached Self-Soother, Compliant Surrenderer and Eating Disorder Overcontroller). Only the Vulnerable Child Mode did not show significant contrasts between EDE-Q subscales. In the case of Demanding and Punitive Modes, the “Restraint” subscale also significantly discriminated at a higher level than the “Eating Concern” subscale. In particular, focused contrasts indicated that “Restraint” and “Eating Concern” subscales significantly discriminated the following modes at a higher level than the “Shape-” and “Weight concern” subscales: Eating Disorder Overcontroller, Compliant Surrenderer, Detached Self-Soother, Demanding Parent and Punitive Parent Modes. Both Restraint and Eating Concern subscales significantly discriminated the Impulsive Child Mode over and above the Weight Concern subscale.
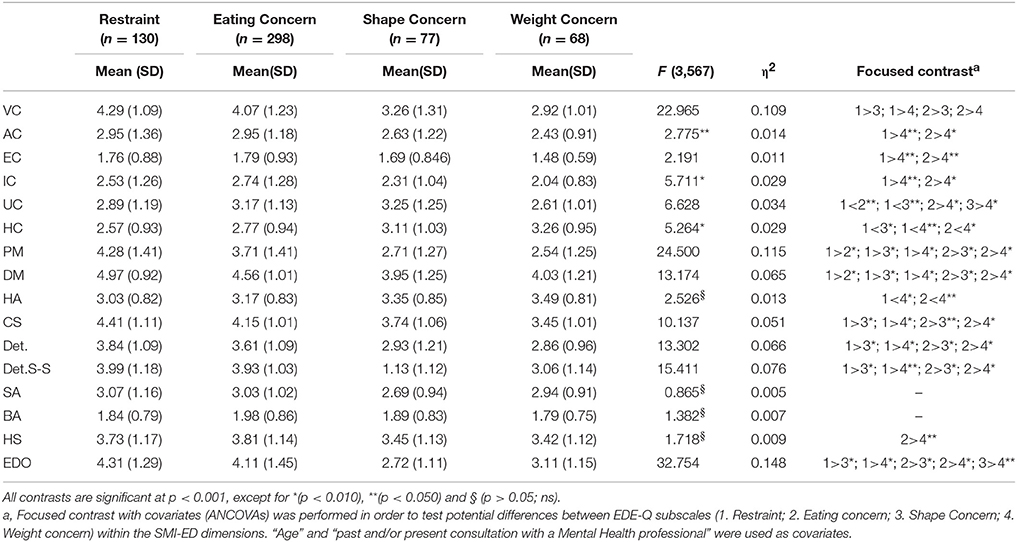
Table 5. Mean (SD) for the ED subscale, results of Multivariate Analysis of Covariance.
Discussion
This study tested the psychometric properties of the SMI-ED, an adapted version of the original SMI, and investigated its psychometric properties within a population characterized by disordered eating patterns. Findings indicated an adequate fit for a 16-factor model, with moderate intercorrelations between subscales, and high internal consistency within subscales.
Although the chi-square model for fit and the CFI values resulted in a less than ideal fit, it must be highlighted that fit indices are affected by the sample size [i.e., chi-square (Jöreskog, 1969; Tuker and Lewis, 1973; Bentler and Bonett, 1980; James and Mulaik, 1982; Kline, 2015)] and the number of considered indicators respectively [i.e., CFI (Hu and Bentler, 1998; Russell, 2002; Kenny and McCoach, 2003; Fan and Sivo, 2005; Iacobucci, 2010; Kline, 2015)]. Indeed, as suggested by Kenny and McCoach (2003), testing well-fitting models with too many indicators, may cause malfunctioning in the CFI index, but it should not be a cause for concern if the SRMR and RMSEA reveal a good approximation fit of the model to the data (Hu and Bentler, 1998, 1999; Russell, 2002; Kenny and McCoach, 2003; Fan and Sivo, 2005; Iacobucci, 2010; Kline, 2015).
The final SMI-ED comprised 190 items that were found to best represent and distinguish 16 schema modes within this sample (the Helpless Surrenderer-HS and the ED-Overcontroller—EDO modes were specifically added for adapting the tool to the EDs sample). The final 16 factors indicated 5 maladaptive child modes; 2 maladaptive internalized/introject modes; 7 maladaptive coping modes; and 2 healthy factors, and included 73 new items. This supports our suggestion that the original SMI may not adequately capture the mode presentations for EDs, and that they may be better represented by the inclusion of items more directly related to the experiences reported by this specific population. The potential utility of measuring schema modes using separate subscales is therefore confirmed. The addition of two new coping modes, as well as additional items added to existing mode scales within the SMI-ED are likely to be of clinical utility in facilitating identification of ED-specific behaviors that characterize specific modes. Although mode scale scores may remain relatively unaffected by the new items, the qualitative examination of specific high-scoring items is likely to be of clinical value.
In support of Lobbestael et al.'s (2010) original findings (Lobbestael et al., 2010), Vulnerable, Angry, Enraged, Undisciplined, Impulsive, and Contented Child modes and the two “parent” (or introject) modes retained some items from the original SMI, with the addition of some new items. The ED-Overcontroller Mode (EDO) was found to be differentiated in the SMI-ED, supporting the notion that what was previously identified as a clinically important concept forms a measurable and coherent mode (Simpson, 2012, 2016) and upholding previous findings (Brown et al., 2016). All of these were new items. This mode is overcontrolling of the self and/or others and uses over-control of the body and perfectionism, to overcompensate for an underlying sense of powerlessness, shame or guilt. This overcompensatory coping mode can lead to feelings of mastery, powerfulness and pseudo-control (Arntz, 2010; Simpson, 2012, 2016). Results indicated that the one new item and one adapted item in Self Aggrandizer mode clustered with the 9 items that were retained from this mode within the original SMI. This supports our clinical observations that this mode may take on a slightly different “flavour” to the Self Aggrandizer in the original SMI, as the emphasis is on extreme high standards and a sense of pride or even superiority, often with an excessive emphasis on shape, weight and thinness which is perceived to provide protection from further shame or criticism (Simpson, 2016). This is consistent with findings for those with Obsessive-Compulsive Personality Disorder, who in this mode experience themselves as superior to others who are perceived as less principled and scrupulous (Beck et al., 2004; Weertman et al., 2008; Bamelis et al., 2015). Two of the three new items proposed for the Bully and Attack mode (“I feel invincible” and “If I'm not constantly on guard people will take advantage of me”) did not have a high loading on this scale, and will therefore be removed from the shorter scale in the second study. This may be because they are both likely to function as passive mechanisms for defending themselves against possible attack from others, rather than overtly bullying others.
The Helpless (or “Aggrieved”) Surrenderer Mode included 5 new items, and all but one had high loadings on this factor. The lower loading on the item “I am very possessive and hold on to the people that are important to me” may be indicative of the pattern of passivity and resignation connected with this mode, whereby the person feels helpless to find direct ways of asking for support and connection from others. This mode is characterized by a pattern whereby others are expected to intuitively know what they feel and need, with a tendency to feel frustrated when this does not materialize (Simpson, 2016). This mode has some overlap with the Complaining Protector mode (Bernstein and van den Broek, 2009) and also perhaps the Self-Pity/Victim Mode (Edwards, 2012, 2015) in the sense that all of these modes are represented by a passive-aggressive style of communication and a tendency to externalize responsibility for getting one's needs met. In this mode, self-deprivation, and physical frailty become an indirect means of communicating a need for emotional support (e.g., “if I am physically unwell, they will see how much I need them”). The remaining coping modes (Compliant Surrenderer, Detached Protector, Detached Self-Soother) and Healthy Adult mode were parallel to those described in the original validation study (Lobbestael et al., 2010) with the addition of some new items.
Correlations between modes were generally high. As expected, correlations between Punitive and Demanding Parent modes and Vulnerable and Angry Child modes were high, reflecting the toxic effect of internalized critical messages in generating emotional distress. Detached Protector and ED-Overcontroller were also surprisingly highly correlated with Vulnerable Child mode, which may be an indication of mode-flipping, whereby one closely follows the other. Indeed, coping modes are generally utilized to keep Vulnerable child mode (and attendant distress) outside conscious awareness. There was a significant difference between disordered eating behaviors (EDE-Q subscales) on the majority of the SMI-ED subscales, with most indicating higher levels of restraint and eating concern compared with shape and weight concern (Table 5). Both “Restraint” and “Eating Concern” subscales of the EDE-Q discriminated the modes most representative of eating disorder populations. In the case of the “Parent” (Introject) modes “Restraint” discriminated these more significantly than “Eating Concern” subscale. The higher mean scores on the “Restraint” and “Eating Concern” subscales compared with the “Shape-”and “Weight-Concerns” subscales may be due to the high number of participants with high levels of restrictive behaviors in this sample (as indicated by endorsement of: restraint over eating, avoidance of eating, food avoidance, dietary rules and desire for an empty stomach). Indeed, “Restraint” remained significantly higher than “Eating Concern” in spite of the fact that it comprised less than half of the number of participants (compared with “Eating Concern”), further corroborating this result. “Restraint” represents an attitude and behaviors that are highly relevant across all eating disorders. It is the main symptom that perpetuates AN, precedes binges in bulimic disorders, and also functions as a compensatory behavior in BN. In addition, the mean BMI in the “Restraint” category was low (18.18), indicating the majority of participants were characterized by restrictive eating patterns.
As expected, in this clinical sample the majority of eating disorder symptoms were positively correlated with Internalized/Introject and Coping modes and negatively correlated with the Healthy modes. Three of the coping modes, Bully-Attack, Self-Aggrandizer and Helpless Surrenderer only showed low correlations with eating disorder symptoms. It may be that these modes are more relevant to maintenance cycles or to other co-morbid symptoms, rather than directly influencing specific ED symptoms. Alternatively, it seems plausible that as the majority of these modes are described for a wide range of disorders, they may have a stronger association with general psychopathology than specific symptoms associated with eating disorders. Future studies may explore the role of these modes further within the ED population, and investigate whether they are more relevant to specific ED diagnostic groups. However, there were moderate to high correlations between the majority of coping modes and restraint and eating/weight/shape concerns. This is consistent with previous studies which have highlighted the link between avoidant coping, numbness, feelings of “lightness” and even euphoria, and restrictive eating/starvation syndrome (Spranger et al., 2001; Wildes et al., 2010; Kaye et al., 2013; Brown et al., 2016). The fact that these coping modes emerged as significant factors is consistent with findings from previous studies (Talbot et al., 2015; Brown et al., 2016). Low correlations were identified between other specific ED symptoms (e.g., bingeing, vomiting, exercise) and schema modes, however correlations between global eating disorder ratings and schema modes were mostly moderate to high.
Practical Implications
The adapted SMI-ED was developed to increase the relevance of the measure for an ED population. At this preliminary stage of development, this measure is likely to be of potential clinical utility both quantitatively and qualitatively. In fact, the two new schema coping modes—the Eating Disorder Overcontroller and Helpless Surrenderer modes—provide additional information regarding coping styles that are specific of the ED population, still not available from the original SMI. The adaptation of the SMI for EDs offers an opportunity for clinicians to identify and explore a wider range of mechanisms through which modes are expressed in this population. In turn, this will facilitate the development of individually tailored case conceptualizations and treatment. It is hoped that the scale will enable a greater shared understanding of ED difficulties within treatment settings, and will give those with EDs greater therapeutic opportunities for making important links between eating disorder symptoms/behaviors, and schema modes.
Limitations and Recommendations for Future Research
Given the large number of items in the SMI-ED, it is questionable whether the sample was large enough to allow for definitive findings. This survey was specifically developed to identify participants with disordered eating, including those with subthreshold eating disorders, and therefore is not directly generalizable to a clinical population. In addition, as this was an online survey that asked participants to take part if they identified themselves as having disordered eating behaviors, there is likely to have been some self-selection bias, with an under-representation of those who were “pre-contemplative” (i.e., characterized by a reduced capacity to recognize and/or acknowledge their eating disordered behaviors). It is also possible that those with more severe eating disorders who may be more isolated, and/or avoidant of eating disorder clinical and support services may have been under-represented. Furthermore, as the sample was purely recruited via online survey in a naturalistic setting, it was not possible to ensure gender homogeneity among respondents. Still, although only a small proportion of the sample was male, this is representative of the gender ratio found in clinical settings (Striegel-Moore et al., 2009). In addition, the use of self-report measures did not allow diagnosis, nor a comprehensive assessment of eating disordered symptoms. A relatively low proportion of participants endorsed binge eating behaviors compared with other dysfunctional eating patterns. Future studies should ideally include a larger percentage of males in the sample. In addition, diagnostic measures should be utilized to ensure that all ED subgroups are adequately represented within the sample, so as to ascertain whether particular profiles of schema modes exist within specific diagnostic groups. However, given that it is becoming increasingly recognized that a transdiagnostic approach is more appropriate for capturing the complexities of individual presentations, it may be that the complex interplay between personality disorders and eating disorder diagnoses will make this a difficult task. Indeed, previous studies have identified that schema modes may be more strongly explained by strength of personality disorder than non-characterological (Axis I) disorders (Lobbestael et al., 2010). This highlights the potential importance for future researchers and clinicians to measure personality disorder alongside eating disorder symptomatology.
This study represents a preliminary step in understanding the schema modes represented within the ED population. An independent replication and assessment of test-retest reliability and construct validity across the range of eating disorder diagnostic groups is required. There is a need for further differentiation of modes within specific ED diagnostic groupings, and the degree to which this is statistically viable. Finally, future studies are needed to explore the psychometric properties and factorial structure of the SMI-ED in both clinical and non-clinical populations, across other countries and languages, as well as to identify whether a shortened version of the scale is feasible.
Conclusion
This study represents the first step in creating a psychometrically sound instrument for the assessment of schema modes in EDs, and provides greater insight for the conceptualization and treatment of this population. This measure was comprised of a hybrid of 117 items from the original SMI with 73 new eating-disorder-specific items relating to schema modes. Confirmatory Factor Analysis confirmed the sixteen-related-factors solution for the 190-item SMI-ED, thus providing preliminary evidence for the adequate reliability of the new measure. The adaptation of the SMI for those with disordered eating represents the first step in developing a tailor-made measure of schema modes for the ED population. The adapted SMI-ED provides a tool for identifying and exploring a wide range of mechanisms through which modes are manifested in this population. Further studies are warranted to further refine and shorten the SMI-ED, in order to improve its utility as a research and clinical tool with this population.
Author Contributions
SS conceived the study and wrote the manuscript with support from GP and AR. GP also contributed to data interpretation, and AR performed the analysis. GM helped supervise the project. TS contributed to data collection and preparation. CM and JN revised the advanced versions of the manuscript. GC approved the final version of the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
EDs, Eating Disorders; CBT, Cognitive Behavioral Therapy; BN, Bulimia Nervosa; BED, Binge Eating Disorder; AN, Anorexia Nervosa; CBT-E, Enhanced CBT; ST, Schema Therapy; EMS, Early Maladaptive Schemas; SMI-ED, Schema Mode Inventory for Eating Disorders; VC, Vulnerable Child; AC, Angry Child; EC, Enraged Child; IC, Impulsive Child; UC, Undisciplined Child; PM, Punitive Mode; DM, Demanding Mode; CS, Compliant Surrender; Det.P, Detached Protector; Det.S-S, Detached Self-Soother; S-A, Self Aggrandizer; BA, Bully and Attack; HS, Helpless Surrenderer; EDO, Eating Disorder Overcontroller; HC, Happy Child; CFA, Confirmatory Factor Analysis; SMI, Schema Mode Inventory; SMI-ED, Schema Mode Inventory for Eating Disorders; CFI, Comparative Fit Index; RMSEA, Root-Mean Square Error of Approximation; SRMR, Standard Root Mean square Residual; MANCOVA, Multivariate analysis of covariance.
References
Arntz, A. (2010). “Schematherapie bei Cluster C Persänlichkeitsstämngen,” in Fortschritte der Schematherapie, Konzepte and Amvendungen, eds E. Roediger and G. Jacob (Göttingen: Hogrefe. S.), 146–182.
Bamelis, L. L., Arntz, A., Wetzelaer, P., Verdoorn, R., and Evers, S. M. (2015). Economic evaluation of schema therapy and clarification-oriented psychotherapy for personality disorders: a multicenter, randomized controlled trial. J. Clin. Psychiatry 76, e1432–e1440. doi: 10.4088/JCP.14m09412
Bamelis, L. L., Renner, F., Heidkamp, D., and Arntz, A. (2011). Extended schema mode conceptualizations for specific personality disorders: an empirical study. J. Pers. Disord. 25, 41–58. doi: 10.1521/pedi.2011.25.1.41
Barrett, P. (2007). Structural equation modelling: adjudging model fit. Pers. Individ. Dif. 42, 815–824. doi: 10.1016/j.paid.2006.09.018
Beck, A. T., Freeman, A., and Davis, D. D. (2004). Cognitive Therapy of Personality Disorders, 2nd Edn. New York, NY: Guilford Press.
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychol. Bull. 107, 238–246. doi: 10.1037/0033-2909.107.2.238
Bentler, P. M., and Bonett, D. G. (1980). Significance tests and goodness of fit in the analysis of covariance structures. Psychol. Bull. 88, 588–606. doi: 10.1037/0033-2909.88.3.588
Berg, K. C., Peterson, C. B., Frazier, P., and Crow, S. J. (2011). Convergence of scores on the interview and questionnaire versions of the Eating Disorder Examination: a meta-analytic review. Psychol. Assess. 23, 714–724. doi: 10.1037/a0023246
Bernstein, D. P., and van den Broek, E. (2009). Schema Mode Observer Rating Scale (SMORS). Unpublished manuscript, Department of Psychology, Maastricht University, The Netherlands.
Blinder, B. J., Cumella, E. J., and Sanathara, V. A. (2006). Psychiatric comorbidities of female inpatients with eating disorders. Psychosom. Med. 68, 454–462. doi: 10.1097/01.psy.0000221254.77675.f5
Brown, J., Selth, S., Stretton, A., and Simpson, S. (2016). Do dysfunctional coping modes mediate the relationship between perceived parenting style and disordered eating behaviours? J. Eat. Disord. 4:27. doi: 10.1186/s40337-016-0123-1
Brown, T. A. (2015). Confirmatory Factor Analysis for Applied Research. 2nd Edn. New York, NY: The Guilford Press.
Browne, M. W., and Cudeck, R. (1990). Single sample cross-validation indices for covariance structures. Multivariate Behav. Res. 24, 445–455. doi: 10.1207/s15327906mbr2404_4
Byrne, S. M., Fursland, A., Allen, K. L., and Watson, H. (2011). The effectiveness of enhanced cognitive behavioural therapy for eating disorders: an open trial. Behav. Res. Ther. 49, 219–226. doi: 10.1016/j.brat.2011.01.006
Castelnuovo, G., Manzoni, G. M., Villa, V., Cesa, G. L., Pietrabissa, G., and Molinari, E. (2011). The STRATOB study: design of a randomized controlled clinical trial of Cognitive Behavioral Therapy and Brief Strategic Therapy with telecare in patients with obesity and binge-eating disorder referred to residential nutritional rehabilitation. Trials 12:114. doi: 10.1186/1745-6215-12-114
Castelnuovo, G., Pietrabissa, G., Manzoni, G. M., Cattivelli, R., Rossi, A., Novelli, M., et al. (2017). Cognitive behavioral therapy to aid weight loss in obese patients: current perspectives. Psychol. Res. Behav. Manag. 10, 165–173. doi: 10.2147/PRBM.S113278
Cronbach, L. J. (1951). Coefficient alpha and the internal structure of tests. Psychometrika 16, 297–334. doi: 10.1007/BF02310555
de Klerk, N., Abma, T. A., Bamelis, L. L., and Arntz, A. (2016). Schema therapy for personality disorders: a qualitative study of patients' and therapists' perspectives. Behav. Cogn. Psychother. 1–15, 31–45. doi: 10.1017/S1352465816000357
Edwards, D. (ed.). (2012). Overcoming Obstacles to Reparenting the Inner Child. New York, NY: International Society of Schema Therapy World Trade Center.
Edwards, D. (2015). Self Pity/Victim: A Surrender Schema Mode. Schema Therapy Bulletin. Available online at: http://www.schematherapysouthafrica.co.za/wp-content/uploads/2015/05/-Edwards-Self-pity-Victim-mode-ST-Bulletin.pdf
Fairburn, C. G., and Beglin, S. (2008). “Eating disorder examination questionnaire (EDE-Q 6.0),” in Cognitive Behavior Therapy and Eating Disorders, ed G. Fc (New York, NY: Guilford Press), 309–313.
Fairburn, C. G., Cooper, Z., Shafran, R., Bohn, K., Hawker, D., Murphy, R., et al. (2008). “Enhanced cognitive behavior therapy for eating disorders: the core protocol,” in Cognitive Behavior Therapy and Eating Disorders, ed C. G. Fairburn (New York, NY: Guilford Press), 45–193.
Fan, X., and Sivo, S. A. (2005). Sensitivity of fit indexes to misspecified structural or measurement model components. Struct. Equat. Model. 12, 343–367. doi: 10.1207/s15328007sem1203_1
Farstad, S. M., McGeown, L., and von Ranson, K. M. (2016). Eating Disorders and personality, 2004-2016: a systematic review and meta-analysis. Clin. Psychol. Rev. 46, 91–105. doi: 10.1016/j.cpr.2016.04.005
Grilo, C. M., Pagano, M. E., Skodol, A. E., Sanislow, C. A., McGlashan, T. H., Gunderson, J. G., et al. (2007). Natural course of bulimia nervosa and of eating disorder not otherwise specified: 5-year prospective study of remissions, relapses, and the effects of personality disorder psychopathology. J. Clin. Psychiatry 68, 738–746. doi: 10.4088/JCP.v68n0511
Halmi, K. A., Tozzi, F., Thornton, L. M., Crow, S., Fichter, M. M., Kaplan, A. S., et al. (2005). The relation among perfectionism, obsessive-compulsive personality disorder and obsessive-compulsive disorder in individuals with eating disorders. Int. J. Eat. Disord. 38, 371–374. doi: 10.1002/eat.20190
Hu, L., and Bentler, P. M. (1998). Fit indexes in covariance structure modeling: sensitivity to underparameterized model misspecification. Psychol. Methods 3, 424–453. doi: 10.1037/1082-989X.3.4.424
Hu, L. T., and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct. Equ. Model. 6, 1–55. doi: 10.1080/10705519909540118
Iacobucci, D. (2010). Structural equations modeling: fit indices, sample size, and advanced topics. J. Consumer Psychol. 20, 90–98. doi: 10.1016/j.jcps.2009.09.003
Jacob, G., and Arntz, A. (2013). Schema therapy for personality disorders: a review. Int. J. Cogn. Ther. 6, 171–185. doi: 10.1521/ijct.2013.6.2.171
James, L. R., and Mulaik, S. A. (1982). Causal Analysis: Assumptions, Models and Data. Beverly Hills, CA: Sage.
Jöreskog, K. G. (1969). A general approach to confirmatory maximum likelihood factor analysis. Psychometrika 34, 183–202. doi: 10.1007/BF02289343
Kaye, W. H., Wierenga, C. E., Bailer, U. F., Simmons, A. N., Wagner, A., and Bischoff-Grethe, A. (2013). Does a shared neurobiology for foods and drugs of abuse contribute to extremes of food ingestion in anorexia and bulimia nervosa? Biol. Psychiatry 73, 836–842. doi: 10.1016/j.biopsych.2013.01.002
Keller, M. B., Herzog, D. B., Lavori, P. W., Bradburn, I. S., and Mahoney, E. S. (2006). The naturalistic history of bulimia nervosa: extraordinarily high rates of chronicity, relapse, recurrence, and psychosocial morbidity. Int. J. Eating Disord. 12, 1–9. doi: 10.1002/1098-108X(199207)12:1<1::AID-EAT2260120102>3.0.CO;2-E
Kenny, D. A., and McCoach, D. B. (2003). Effect of the number of variables on measures of fit in structural equation modeling. Struct. Equ. Model. 10, 333–351. doi: 10.1207/S15328007SEM1003_1
Kline, R. B. (2015). Principles and Practice of Structural Equation Modeling. New York, NY: The Guilford Press.
Lobbestael, J., van Vreeswijk, M., Spinhoven, P., Schouten, E., and Arntz, A. (2010). Reliability and validity of the short Schema Mode Inventory (SMI). Behav. Cogn. Psychother. 38, 437–458. doi: 10.1017/S1352465810000226
MacCallum, R. C., Widaman, K. F., and Zhang, S., (1999). Sample size in factor analysis. Psychol. Methods 4, 84–99. doi: 10.1037/1082-989X.4.1.84
Marais, I., Moir, V. K., and Lee, C. W. (2017). The effects of item placement in the Young Schema Questionnaire. J. Appl. Meas. 18, 370–382.
Marsh, H. W., and Hocevar, D. (1985). Application of confirmatory factor analysis to the study of self-concept: first-and higher order factor models and their invariance across groups. Psychol. Bull. 97, 562–582. doi: 10.1037/0033-2909.97.3.562
Masley, S. A., Gillanders, D. T., Simpson, S. G., and Taylor, M. A. (2012). A systematic review of the evidence base for Schema therapy. Cogn. Behav. Ther. 41, 185–202. doi: 10.1080/16506073.2011.614274
McIntosh, V. V. M., Jordan, J., Carter, J. D., Frampton, C. M. A., McKenzie, J. M., Latner, J. D., et al. (2016). Psychotherapy for transdiagnostic binge eating: a randomized controlled trial of cognitive-behavioural therapy, appetite-focused cognitive-behavioural therapy, and schema therapy. Psychiatry Res. 240, 412–420. doi: 10.1016/j.psychres.2016.04.080
Mond, J. M., Hay, P. J., Rodgers, B., and Owen, C. (2006). Eating disorder examination questionnaire (EDE-Q): norms for young adult women. Behav. Res. Ther. 44, 53–62. doi: 10.1016/j.brat.2004.12.003
Mond, J. M., Hay, P. J., Rodgers, B., Owen, C., and Beumont, P. J. (2004). Validity of the Eating Disorder Examination Questionnaire (EDE-Q) in screening for eating disorders in community samples. Behav. Res. Ther. 42, 551–567. doi: 10.1016/S0005-7967(03)00161-X
Muthén, B. O., du Toit, S. H. C., and Spisic, D. (1997). Robust Inference Using Weighted Least Squares and Quadratic Estimating Equations in Latent Variable Modeling With Categorical and Continuous Outcomes. Unpublished technical report. Available online at: https://www.statmodel.com/download/Article_075.pdf
Muthén, L. K., and Muthén, B. O. (1998). Mplus User's Guide. Seventh Edn. Los Angeles, CA: Muthén and Muthén-2012.
Nie, N. H., Bent, D. H., and Hull, C. H. (1970). SPSS: Statistical Package for The Social Sciences. New York, NY: McGraw-Hill.
Peterson, C. B., Crosby, R. D., Wonderlich, S. A., Joiner, T., Crow, S. J., Mitchell, J. E., et al. (2007). Psychometric properties of the eating disorder examination-questionnaire: factor structure and internal consistency. Int. J. Eat. Disord. 40, 386–389. doi: 10.1002/eat.20373
Pietrabissa, G., Manzoni, G. M., Rossi, A., and Castelnuovo, G. (2017). The motiv-heart study: a prospective, randomized, single-blind pilot study of brief strategic therapy and motivational interviewing among cardiac rehabilitation patients. Front. Psychol. 8:83. doi: 10.3389/fpsyg.2017.00083
Rosseel, Y. (2012). lavaan: an R package for structural equation modeling. J. Stat. Softw. 48, 1–36. doi: 10.18637/jss.v048.i02
Rosseel, Y., Oberski, D., Byrnes, J., Vanbrabant, L., Savalei, V., Merkle, E., et al. (2015). Package ‘Lavaan’: Latent Variable Analysis. R Package. Available online at: http://lavaan.org
Russell, D. W. (2002). In search of underlying dimensions: the use (and abuse) of factor analysis in personality and social psychology bulletin. Personality Soc. Psychol. Bull. 28, 1629–1646. doi: 10.1177/014616702237645
Sallet, P. C., de Alvarenga, P. G., Ferrão, Y., de Mathis, M. A., Torres, A. R., Marques, A., et al. (2010). Eating disorders in patients with obsessive-compulsive disorder: prevalence and clinical correlates. Int. J. Eat. Disord. 43, 315–325. doi: 10.1002/eat.20697
Satorra, A., and Bentler, P. M. (eds) (1988). Scaling Corrections for Chi-Square Statistics in Covariance Structure Analysis. Business and Economic Section of the American Statistical Association. Alexandria, VA: American Statistical Association.
Satorra, A., and Bentler, P. M. (1994). “Corrections to test statistics and standard errors in covariance structure analysis,” in Latent Variables Analysis: Applications for Developmental Research, eds A. von Eye and C. C. Clogg (Thousand Oaks, CA: Sage), 399–419.
Sheffield, A., Waller, G., Emanuelli, F., Murray, J., and Meyer, C. (2009). Do schema processes mediate links between parenting and eating pathology? Eur. Eat. Disord. Rev. 17, 290–300. doi: 10.1002/erv.922
Simpson, S. (2016). “Schemamodi bei Essstörungen,” in Schematherapie Bei Essstörungen, eds C. Archonti, E. Roediger, and M. de Zwaan (Weinheim: Beltz), 70–82.
Simpson, S. G. (2012). “Schema therapy for eating disorders: a case illustration of the mode approach,” in The Wiley-Blackwell Handbook of Schema Therapy: Theory, Research, and Practice, eds M. van Vreeswijk, J. Broersen, and M. Nadort (Chichester: Wiley), 145–171.
Simpson, S. G., Morrow, E., van Vreeswijk, M., and Reid, C. (2010). Group schema therapy for eating disorders: a pilot study. Front. Psychol. 1:182. doi: 10.3389/fpsyg.2010.00182
Simpson, S. G., and Slowey, L. (2011). Video therapy for atypical eating disorder and obesity: a case study. Clin. Pract. Epidemiol. Ment. Health 7, 38–43. doi: 10.2174/1745017901107010038
Sorgente, A., Pietrabissa, G., Manzoni, G. M., Re, F., Simpson, S., Perona, S., et al. (2017). Web-based interventions for weight loss or weight loss maintenance in overweight and obese people: a systematic review of systematic reviews. J. Med. Internet Res. 19:e229. doi: 10.2196/jmir.6972
Spranger, S. C., Waller, G., and Bryant-Waugh, R. (2001). Schema avoidance in bulimic and non-eating-disordered women. Int. J. Eat. Disord. 29, 302–306. doi: 10.1002/eat.1022
Steiger, J. H. (1990). Structural model evaluation and modification: an interval estimation approach. Multivariate Behav. Res. 25, 173–180. doi: 10.1207/s15327906mbr2502_4
Steiger, J. H., and Lind, J. C. (1980). “Statistically-based test for the number of common factors,” in Annual Meeting of the Psychometric Society (Iowa City, IA).
Striegel-Moore, R. H., Rosselli, F., Perrin, N., DeBar, L., Wilson, G. T., May, A., et al. (2009). Gender difference in the prevalence of eating disorder symptoms. Int. J. Eating Disord. 42, 471–474. doi: 10.1002/eat.20625
Talbot, D., Smith, E., Tomkins, A., Brockman, R., and Simpson, S. (2015). Schema modes in eating disorders compared to a community sample. J. Eat. Disord. 3:41. doi: 10.1186/s40337-015-0082-y
Team RC. (2015). R: A Language and Environment For Statistical Computing. R Foundation for Statistical Computing. Team RC.
Tuker, L. R., and Lewis, C. (1973). A reliability coefficient for maximum likelihood factor analysis. Psychometrika 38, 1–10. doi: 10.1007/BF02291170
Voderholzer, U., Schwartz, C., Thiel, N., Kuelz, A. K., Hartmann, A., Scheidt, C. E., et al. (2014). A comparison of schemas, schema modes and childhood traumas in obsessive-compulsive disorder, chronic pain disorder and eating disorders. Psychopathology 47, 24–31. doi: 10.1159/000348484
Waller, G. (1997). Drop-out and failure to engage in individual outpatient cognitive behavior therapy for bulimic disorders. Int. J. Eat. Disord. 22, 35–41. doi: 10.1002/(SICI)1098-108X(199707)22:1<35::AID-EAT4>3.0.CO;2-3
Waller, G. (2003). Schema-level cognitions in patients with binge eating disorder: a case control study. Int. J. Eat. Disord. 33, 458–464. doi: 10.1002/eat.10161
Waller, G., and Kennerley, H. (2003). “Cognitive-behavioral treatments,” in Handbook of Eating Disorders, 2nd Edn., eds J. Treasure, U. Schmidt, and E. Furth (Chichester: Wiley), 233–251.
Waller, G., Kennerley, H., and Ohanian, V. (2007). “Schema-focused cognitive-behavioral therapy for eating disorders,” in Cognitive Schemas and Core Beliefs in Psychological Problems: A Scientist-Practitioner Guide, eds P. Riso, P. L. du Toit, D. J. Stein, and J. E. Young (Washington, DC: American Psychological Association), 139–175.
Waller, G., Schmidt, U., Treasure, J., Murray, K., Aleyna, J., Emanuelli, F., et al. (2009). Problems across care pathways in specialist adult eating disorder services. Psychiatr. Bull. 33, 26–29. doi: 10.1192/pb.bp.107.018325
Weertman, A., Arntz, A. R., de Jong, P. J., and Rinck, M. (2008). Implicit self- and other-associations in obsessive-compulsive personality disorder traits. Cogn. Emot. 22, 1253–1275. doi: 10.1080/13546780701739790
Wheaton, B., Muthén, B., Alwin, D., and Summers, G. (1977). “Assessing reliability and stability in panel models,” in Sociological Methodology, ed D. R. Heise (San Francisco, CA: Jossey-Bass, Inc.,), 84–136.
Wildes, J. E., Ringham, R. M., and Marcus, M. D. (2010). Emotion avoidance in patients with anorexia nervosa: initial test of a functional model. Int. J. Eat. Disord. 43, 398–404. doi: 10.1002/eat.20730
Young, J. E., Arntz, A., Atkinson, T., Lobbestael, J., Weishaar, M. E., and van Vreeswijk, M. F. (2007). The Schema Mode Inventory. New York, NY: Schema Therapy Institute.
Keywords: factorial structure, psychometric properties, schema therapy, modes, assessment, eating disorders, eating behaviors
Citation: Simpson SG, Pietrabissa G, Rossi A, Seychell T, Manzoni GM, Munro C, Nesci JB and Castelnuovo G (2018) Factorial Structure and Preliminary Validation of the Schema Mode Inventory for Eating Disorders (SMI-ED). Front. Psychol. 9:600. doi: 10.3389/fpsyg.2018.00600
Received: 25 September 2017; Accepted: 10 April 2018;
Published: 24 April 2018.
Edited by:
Nuno Conceicao, Universidade de Lisboa, PortugalReviewed by:
Nelson Silva Filho, Universidade Estadual Paulista Júlio de Mesquita Filho, BrazilJacqueline C. Carter, Memorial University of Newfoundland, Canada
Copyright © 2018 Simpson, Pietrabissa, Rossi, Seychell, Manzoni, Munro, Nesci and Castelnuovo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susan G. Simpson, susan.simpson@unisa.edu.au