
- Department of Psychiatry, Ambulatory Research Center, University of Minnesota Medical Center, Minneapolis, MN, USA
Impulse control disorders (ICDs) are characterized by urges and behaviors that are excessive and/or harmful to oneself or others and cause significant impairment in social and occupational functioning, as well as legal and financial difficulties. ICDs are relatively common psychiatric conditions, yet are poorly understood by the general public, clinicians, and individuals struggling with the disorder. Although ICD treatment research is limited, studies have shown ICDs may respond well to pharmacological treatment. This article presents a brief overview about the clinical characteristics of ICDs and pharmacological treatment options for individuals with ICDs.
Introduction
The DSM-IV formally recognizes pathological gambling (PG), kleptomania (KM), trichotillomania (TTM), intermittent explosive disorder (IED), and pyromania as impulse control disorders (ICDs). Diagnostic criteria have been proposed for pathological skin picking (PSP), compulsive sexual behavior (CSB), and compulsive buying (CB), which are currently classified under ICDs not otherwise specified (NOS). The core characteristic of ICDs is difficulty resisting urges to engage in behaviors that are excessive and/or ultimately harmful to oneself or others (American Psychiatric Association, 2000). ICDs are relatively common among adolescents and adults, carry significant morbidity and mortality, and can often be effectively treated with behavioral and pharmacological therapies. A study of 791 college students found that 82 (10.4%) met criteria for at least one lifetime ICD, demonstrating the common nature of these disorders in the general population (Odlaug and Grant, 2010). The intent of this review is to provide an updated clinical picture of the previously mentioned ICDs and present evidence of potential pharmacological treatments for these disorders (see Table 1).
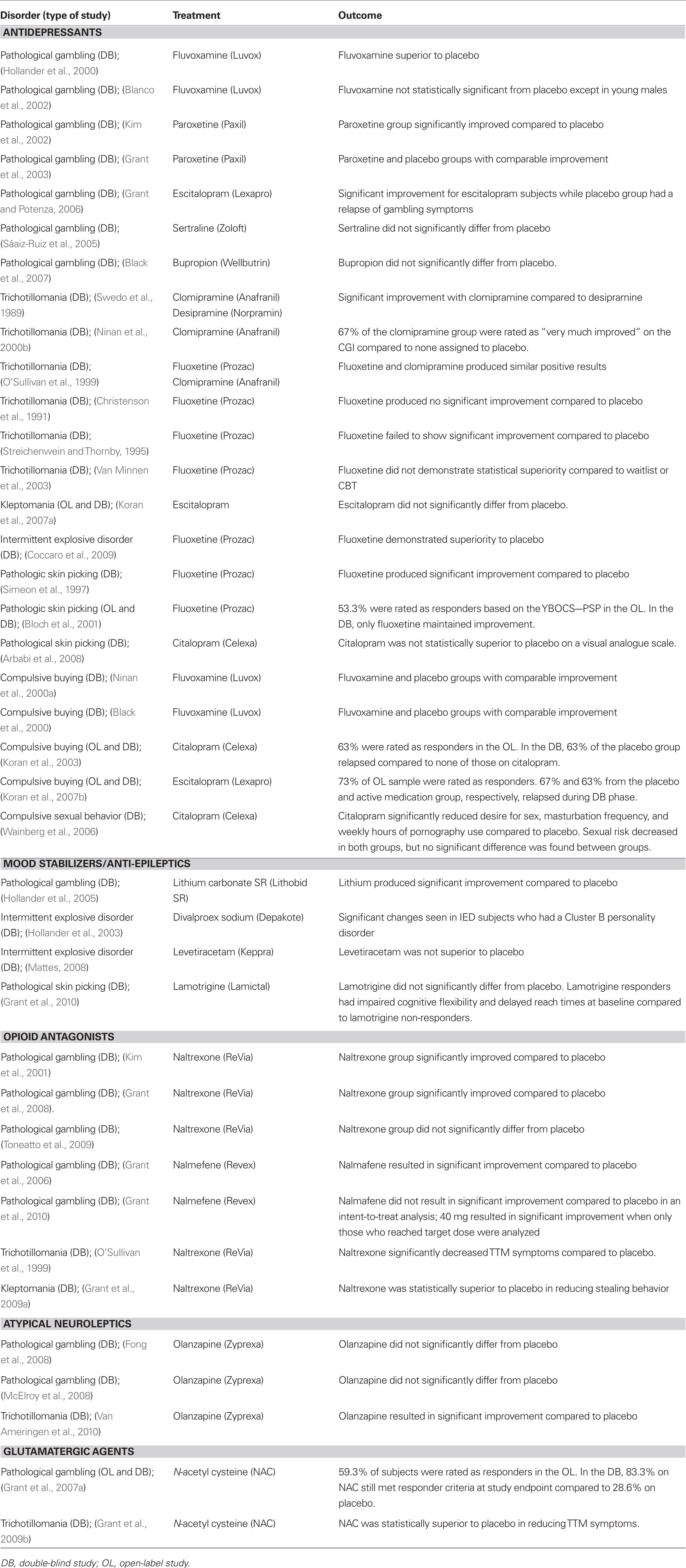
Table 1. Double-blind placebo-controlled pharmacological treatment studies of impulse control disorders.
Methods
Clinical and pharmacological treatment information was found using the electronic databases, PubMed and PsychINFO, using the search terms “impulse control disorders,” “pathological gambling,” “gambling addiction,” “kleptomania,” “trichotillomania,” “hair pulling,” “intermittent explosive disorder,” “pyromania,” “pathological skin picking,” “compulsive sexual behavior,” “sexual addiction,” “compulsive buying,” “compulsive shopping,” and “shopping addiction.” Presented pharmacological treatment data was based on randomized, double-blind, controlled clinical trials published in academic journals. Due to examining multiple disorders, we did not perform a formal meta-analysis.
Core Characteristics of Impulse Control Disorders
The degree to which ICDs overlap in terms of clinical, genetic, phenomenological, and biological characteristics is not completely understood. ICDs, however, have the following features in common: (1) repetitive or compulsive engagement in a behavior despite adverse consequences; (2) diminished control over the problematic behavior; (3) an appetitive urge or craving state prior to engagement in the problematic behavior; and (4) a hedonic quality during the performance of the problematic behavior (Grant and Potenza, 2004). These features have led to a description of ICDs as “behavioral addictions” (Holden, 2010).
More recently, using neurobiological and treatment research, DSM-V has proposed reclassifying PG as an addictive disorder (due to clinical and biological similarities to substance use disorders; Potenza, 2006), moving TTM into a category of obsessive– compulsive spectrum disorders (due to the rituals associated with TTM; Stein et al., 2010), and not including CSB, CB, or PSP due to lack of compelling biological evidence (American Psychiatric Association, 2010). Inclusion of PG among addictive disorders may advance treatment as pharmacotherapies studied in substance use disorders may be transferred into treatment research for PG. Inclusion of PG among other addictions may also give rise to research funding mechanisms currently unavailable to PG. However, not including other ICDs among addictions may continue to hamper treatment advances both due to a lack of awareness and funding. Discussion of where the various ICDs belong in DSM-V will likely be an ongoing debate.
Pathological Gambling
Approximately 0.4–1.6% of individuals in the United States meet criteria for PG (Gambling Impact and Behavior Study, 1999; Petry et al., 2005) characterized by persistent and recurrent maladaptive patterns of gambling behaviors (American Psychiatric Association, 2000). Individuals frequently start gambling in adolescence or young adulthood and often gamble for years before the behavior becomes problematic. The mean age of PG onset is approximately 30 years old (Grant and Kim, 2001). Even though most individuals with PG are men (who typically start gambling at a younger age than women) approximately 28% of pathological gamblers in the United States are women, and studies have shown that women tend to progress from recreational gambling to PG more quickly than men (Gambling Impact and Behavior Study, 1999; Grant and Kim, 2001; Petry et al., 2005; Sáiz-Ruiz et al., 2005). Impaired functioning, decreased quality of life, and financial, marital, and legal problems are associated with PG (Grant and Kim, 2001). Three proposed subtypes of PG include the impulsive (high risk-taking behavior and lack of planning ahead), the obsessive–compulsive (gambling is response to perceived psychological trauma), and the addictive (repetitively gambles a small amount of money) subtypes (Iancu et al., 2008).
It is not uncommon for pathological gamblers to struggle with another psychiatric disorder. Common lifetime comorbid Axis I disorders include mood (20–55.6%), substance use (35–76.3%), and anxiety (41.3–60.3%) disorders (Petry et al., 2005; Grant, 2008; Kessler et al., 2008). Suicide attempts are also common in PG with one study observing attempts in 58 (17%) of 342 individuals (Petry and Kiluk, 2002). Studies have observed high rates of personality disorders in pathological gamblers (Blaszczynski and Steel, 1998; Petry et al., 2005). An epidemiological study of 43,093 respondents found that 60.8% of individuals meeting DSM-IV criteria for PG also met criteria for a personality disorder (Petry et al., 2005). Having a family member with substance abuse or a gambling problem is also common within this population. One study found that 56.5% of pathological gamblers had at least one first-degree relative with alcohol abuse or dependence and 26.9% had a first-degree relative with symptoms of problematic gambling (Grant and Kim, 2001).
Kleptomania
Kleptomania is characterized by the repetitive, uncontrollable stealing of items not needed for personal use (American Psychiatric Association, 2000). Usually, stolen items are hoarded, given away, returned to the store, or thrown away (McElroy et al., 1991). Although no large-scale epidemiologic studies have been conducted to assess the prevalence of KM in the general population, a survey of college students (N = 791) found that 3 (0.38%) met DSM-IV criteria for KM (Odlaug and Grant, 2010). It has been estimated that between 3.8 and 24% of shoplifters struggle with KM (Arieff and Bowie, 1947; Schlueter et al., 1989). KM typically begins between ages 16 and 20 (Grant and Kim, 2002; Grant et al., 2009a), but has been reported in children as young as 4 (Phelan, 2002) and adults as old as 77 (McNeilly and Burke, 1998). Studies have found that between 63 and 75% of those with KM are female (McElroy et al., 1991; Grant and Kim, 2002). The majority (64–87%) of people with KM have been apprehended at some time due to their stealing (McElroy et al., 1991; Grant and Kim, 2002).
Psychiatric comorbidity is common within this population. High rates of mood (36–100%), anxiety (34–80%), and substance use (22–50%) disorders have been documented in individuals with KM (Grant and Kim, 2002; Grant, 2008). High rates of mood (21%), substance use (20%), and anxiety (13%) disorders have also been found in the first-degree relatives of individuals with KM (McElroy et al., 1991; Grant and Kim, 2002).
Trichotillomania
Trichotillomania occurs in approximately 0.5–3.9% in the United States (Christenson et al., 1991; Odlaug and Grant, 2010) and is characterized by repetitive hair-pulling causing noticeable hair loss and resulting in clinically significant distress or functional impairment (American Psychiatric Association, 2000). TTM usually begins in early puberty (11–13 years old) and is more common in females (93.2%; Cohen et al., 1995). Hair may be pulled from any area of the body, but common areas include the scalp (72.8%) and eyebrows (56.4%; Woods et al., 2006). TTM is associated with low self-esteem (Diefenbach et al., 2005). In a study of 1697 individuals with TTM, 34.6% with severe hair-pulling reported daily interference with occupational tasks and 48.7% reported avoiding social situations, such as dating or participating in group activities (Woods et al., 2006). Furthermore, most (79.1%) individuals with TTM reported that pulling episodes resulted in social anxiety due to alopecia (Woods et al., 2006). Despite significant distress, only 65% of people with TTM have ever sought treatment (Woods et al., 2006) and many go to great lengths to hide their pulling from family, friends, and treatment providers (Diefenbach et al., 2005).
Individuals with TTM may also struggle with other psychiatric conditions. Studies have found high rates of co-occurring anxiety (8.9–32%), affective (51.8%), substance use (15–20%), and obsessive–compulsive (8.3–30.4%) disorders (Lochner et al., 2002; Miltenberger et al., 2006; Odlaug and Grant, 2008a). Family history assessments have found that first-degree family members of TTM subjects have substance use (29%), depressive (20%), and anxiety (10%) disorders (Cohen et al., 1995).
Intermittent Explosive Disorder
Intermittent explosive disorder is characterized by recurrent, significant outbursts of aggression, which result in assaultive acts against people or property, are disproportionate to outside stressors, and not better explained by another psychiatric condition (American Psychiatric Association, 2000). It is estimated that 4–7% of people in the United States have IED and usually meet diagnostic criteria during adolescence (ages 14–18; Coccaro et al., 2004; Kessler et al., 2006; Coccaro, 2010). Some clinical studies suggest that the majority (77–87.5%) of individuals with IED are males (Mattes, 2008; Coccaro et al., 2009), however a community sample of 253 individuals found only 37.5% were male (Coccaro et al., 2004). The first outburst typically occurs in early adolescence and people with IED have an average of 43 lifetime attacks resulting in $1359 in property damage (Kessler et al., 2006). The majority (81.3%) also report significant psychosocial impairment due to IED symptoms (Coccaro et al., 2004). Individuals with IED consider their behavior distressing and problematic (McElroy et al., 1998), however, only 28.8% of people suffering from IED have ever received treatment (Kessler et al., 2006).
Approximately 82% of individuals with IED have co-occurring Axis I psychiatric disorders, most commonly mood (11–93%), anxiety (48–58.1%), and substance use (35.1–48%) disorders (Kessler et al., 2006; Grant, 2008). A recent family history study found that first-degree relatives of individuals with IED are more likely to have a psychiatric condition compared to control subjects, however specific rates of psychiatric conditions were not reported (Coccaro, 2010).
Pyromania
Pyromania is characterized by deliberate and purposeful fire-setting on more than one occasion (American Psychiatric Association, 2000). The prevalence of pyromania is not well established, but one study reported a rate of 1% in a college student sample (n = 791; Odlaug and Grant, 2010). A review of 282 arsonists’ hospital records (who were referred for a pre-trial psychiatric assessment) found that 23.6% who had committed other non-violent crimes and 12.4% who had committed other violent crimes met DSM-II-R criteria for pyromania (Repo et al., 1997). Studies of psychiatric patients found that 5.9% met lifetime criteria for pyromania and 2.8–3.4% met current criteria for pyromania (Lejoyeux et al., 2002; Grant et al., 2005; Grant and Kim, 2007). A study of 102 adolescent psychiatric inpatients reported that 6.9% met criteria for current pyromania (Grant et al., 2007b). Usually, pyromania develops during adolescence and is more common in males (Grant and Kim, 2007). Pyromania is associated with high rates of lifetime psychiatric comorbidity, such as affective (14–61.9%), anxiety (33.3%), substance use (33.3%), and impulse control (66.7%) disorders (Grant and Kim, 2007; Grant, 2008).
Pathological Skin Picking
Pathological skin picking is characterized by repetitive or compulsive picking of the skin resulting in tissue damage. The DSM does not formally recognize PSP, but the following criteria have been proposed: (1) preoccupation, impulses, or behaviors associated with skin excoriation; (2) which cause distress or interfere with daily functioning; and (3) are not better accounted for by another mental disorder or medical condition (Arnold et al., 2001). A random-sample, phone survey of 2513 US adults found that between 0.2 and 1.4% satisfied criteria for PSP (Keuthen et al., 2010). A community sample study of 345 individuals found a prevalence rate of 5.4% (Hayes et al., 2009). The majority of people with PSP are female (Keuthen et al., 2010). The area usually picked is the face, but any body part can be a focus (Odlaug and Grant, 2008b).
In addition to dealing with skin picking, individuals with PSP may also have a co-occurring psychiatric condition. Lifetime substance use (38%), affective (28.6–36.4%), and obsessive–compulsive (15.2–19%) disorders are common comorbid conditions (Lochner et al., 2002; Grant, 2008; Odlaug and Grant, 2008a). Psychiatric conditions are also common among first-degree relatives, however, no controlled family history studies have been completed (Arnold et al., 1998; Odlaug and Grant, 2008a,b).
Compulsive Buying
Although the DSM does not have formal diagnostic criteria for CB, it is characterized by a preoccupation with buying, buying more than one can afford or unneeded, items, and shopping for longer durations of time than originally intended, resulting in marked distress or interference with social and occupational functioning (McElroy et al., 1994). The estimated prevalence of CB in the United States is 5.8% (Koran et al., 2006). CB behavior usually appears in late teens or early twenties (Black, 2007), however one study found that age of onset was 30 years old (McElroy et al., 1994). The majority (80–95%) of individuals with CB are women (Black, 2007). Usually purchased items are usually not expensive, but are bought in large quantities resulting in excessive spending (Black, 2007). Purchased items typically go unused, are given away, or returned to the store (Schlosser et al., 1994).
Studies have also found high rates of comorbidity in the CB population, primarily mood (21–100%), anxiety (41–80%), and substance use (21–46%) disorders (Schlosser et al., 1994; Grant, 2008). One controlled study found that 78 (56.9%) of 137 compulsive buyers had a first-degree relative with a psychiatric disorder, most commonly alcoholism (19.7%) or depression (18.3%), which was significantly greater than psychiatric diagnoses (18 of 162, 11.1%) in the first-degree relatives of control subjects (Black et al., 1998).
Compulsive Sexual Behavior
Compulsive sexual behavior is not currently formally recognized by the DSM-IV, but proposed criteria include: (1) recurrent and intense sexual fantasies, urges or behaviors; (2) clinically significant distress or impairment in functioning associated with sexual fantasies, urges, or behaviors; and (3) sexual fantasies, urges, or behaviors that are not better explained by other medical conditions or physiological effect of an exogenous substance (Kafka, 2010). CSB may include a wide range of sexual behaviors, including paraphilic (e.g., exhibitionism, voyeurism, fetishes) and non-paraphilic (e.g., masturbation, promiscuity, pornography), that have become unmanageable and are typically the result of attempts to reduce anxiety or increase pleasure (Coleman, 1992). One study of college students found that 3.7% reported symptoms consistent with the proposed criteria for CSB (Coleman, 1992; Odlaug and Grant, 2010). The majority of treatment-seeking individuals with CSB are males with an onset during late adolescence (Black et al., 1997). The sexual urges and behaviors are often distressing and uncontrollable, triggered by certain mood states (most commonly sadness or depression), and result in feelings of shame (Black et al., 1997).
Individuals with CSB usually have another comorbid disorder. Studies have found that individuals with CSB report symptoms consistent with substance use (64%), affective (14–39%), anxiety (50%), and childhood conduct (44%) disorders (Kafka and Prentky, 1992; Black et al., 1997). In addition, childhood sexual abuse (28–78%) is common in individuals with CSB (Carries and Delmonico, 1996). No systematic family history studies have been completed, but an uncontrolled study of 75 individuals with CSB found that 40% had at least one chemically dependant parent and 36% had one or two sexually addicted parents (Schneider and Schneider, 1996).
Pharmacological Treatment
Despite the high prevalence rates of ICDs in the general population (Kessler et al., 2005) and in psychiatric cohorts (Grant et al., 2005), pharmacological treatments have been relatively understudied. There are no FDA-approved medications for any ICD. This treatment section focuses only on findings from double-blind, placebo-controlled trials.
Antidepressants
Pathological gambling
Studies assessing the efficacy of fluvoxamine in treating PG have produced mixed results. A 16-week study using 15 subjects found that percent improvement of gambling symptoms was significantly greater for fluvoxamine compared to placebo (Hollander et al., 2000). Yet, another trial in which 32 pathological gamblers participated in a 6-month trial failed to find fluvoxamine statistically superior to placebo. The results, however, were complicated by high rates of treatment discontinuation (only three subjects on medication completed the study) and by a high placebo response rate (59%; Blanco et al., 2002).
Paroxetine has also been examined in PG and demonstrated varying results. An 8-week study demonstrated significantly greater reductions in gambling urges and behavior compared to placebo (Kim et al., 2002). In contrast, a larger 16-week trial of 76 subjects found that paroxetine did not demonstrate statistical significance over placebo on any measure. A high placebo response rate (48%) was observed in those assigned to placebo compared to 59% response rate of those randomized to paroxetine (Grant et al., 2003).
An open-label, 12-week trial of escitalopram with an 8-week, double-blind discontinuation period for responders, was performed in 13 PG subjects with co-occurring anxiety disorders. Unlike many clinical trials in this population, current psychiatric comorbidity was not exclusionary. Of the 13 subjects treated with a mean dose of 25.4 mg/day, 8 (62%) were considered responders [defined as 30% or greater reduction in Yale-Brown Obsessive Compulsive Scale Modified for Pathological Gambling (PG-YBOCS) total score at endpoint compared to baseline] in terms of both PG and anxiety symptoms. Four of six subjects who were responders were randomized into an 8-week, double-blind discontinuation study. Of the three assigned to escitalopram, improvement continued for the next 8 weeks in all three cases, whereas both gambling symptoms and anxiety returned within 4 weeks to baseline levels for the subject assigned to placebo, suggesting that escitalopram may effectively decrease both anxiety and gambling (Grant and Potenza, 2006).
In a 6-month double-blind, placebo-controlled study using sertraline for 60 PG subjects, 23 of the 31 subjects randomized to sertraline (74%) and 21 of 29 subjects assigned to placebo (72%) were rated as responders [as measured by the Criteria for Control of Pathological Gambling Questionnaire (CCPGQ)] at endpoint. Scores between groups did not statistically differ (Sáiz-Ruiz et al., 2005).
In the only study to examine a non-serotonergic antidepressant, bupropion was tested in 39 PG subjects in a 12-week, flexible dose trial. The study found that there were no significant differences between the bupropion and the placebo groups in the improvement of gambling behavior and thoughts/urges, or time or money spent on gambling per week (Black et al., 2007).
Trichotillomania
Several controlled pharmacological trials using antidepressants have been conducted in TTM. One study examined clomipramine compared to desipramine in a 10-week, double-blind, cross-over (5 weeks for each agent) design (following 2 weeks of single-blind placebo lead-in) in 13 females. The clomipramine group experienced significant decreases in the severity, frequency, and intensity of hair-pulling compared to desipramine (Swedo et al., 1989). A 9-week, placebo-controlled, randomized, parallel-treatment study of cognitive behavioral therapy (CBT) and clomipramine with 16 subjects, however, found that clomipramine did not result in significantly greater response (Ninan et al., 2000b).
Pigott and colleagues (1992; as cited by O’Sullivan et al., 1999) compared fluoxetine with clomipramine in a double-blind, randomized, 20-week cross-over design (10 weeks on each medication) and found that both clomipramine and fluoxetine demonstrated a similar positive treatment effect in terms of reducing hair-pulling behavior (O’Sullivan et al., 1999). Three other studies investigating fluoxetine, however, failed to demonstrate efficacy in treating TTM. One study found that fluoxetine was no more effective than placebo in reducing number of hair-pulling episodes per week or the amount of hair pulled per week in 21 subjects randomized into a double-blind, cross-over study for 18 weeks (Christenson et al., 1991). A 31-week, double-blind, placebo-controlled, cross-over trail of fluoxetine of 16 subjects with TTM also failed to demonstrate any difference between fluoxetine and placebo in reducing hair-pulling behavior (Streichenwein and Thornby, 1995) The third study comparing fluoxetine treatment to behavioral therapy and a wait-list group, found that only 9% of the fluoxetine group achieved a clinically significant change in hair-pulling behavior compared to 64 and 20% of those in the behavioral therapy and wait-list group, respectively. Furthermore, the wait-list group had a significantly larger decrease in actual hair-pulling compared to the fluoxetine group (Van Minnen et al., 2003).
A meta-analysis of pharmacological and behavioral treatment of TTM found that clomipramine was superior to placebo, however overall SSRI treatment (including fluoxetine and sertraline) was not found to be superior to placebo (Bloch et al., 2007).
Kleptomania
Escitalopram has been evaluated in one clinical trial of KM. After completing 7 weeks of open-label escitalopram, 15 subjects (categorized as responders to the open-label portion) were randomized to receive either escitalopram or placebo for 17 weeks. No significant differences were found between the two groups. In those receiving escitalopram, 43% relapsed and 50% on placebo relapsed and both groups reported similar decreases in KM symptoms from baseline to end of treatment (Koran et al., 2007a).
Intermittent explosive disorder
Fluoxetine has also been evaluated in treating IED and demonstrated significant improvement in reducing frequency and severity of impulsive aggression and irritability in a sample of 100 subjects who were randomized into a 14-week, double-blind study. Despite a large decrease in impulsive aggression behavior from baseline, only 44% of fluoxetine responders and 29% of all fluoxetine subjects were considered to be in full remission at the end of the study (Coccaro et al., 2009).
Pathologic skin picking
Two double-blind studies have been conducted using fluoxetine for the treatment of PSP. A 10-week trial with 21 subjects found that fluoxetine resulted in significant improvements in skin picking symptomology on a visual analog scale compared to placebo (Simeon et al., 1997). Another study randomized 8 (53.3%) of 15 open-label fluoxetine responders (defined as a 30% or greater decrease in YBOCS–PSP scores) into a 6-week double-blind discontinuation period. The four subjects assigned to fluoxetine maintained their levels of improvement and demonstrated a 70% reduction in picking behavior while those on placebo returned to their baseline symptom severity level (Bloch et al., 2001).
One study examined the efficacy of citalopram in treating PSP and found that the 23 subjects randomized to receive 10–20 mg/day of citalopram for 4 weeks had decreased severity of skin picking behavior (measured by a visual analog scale) compared to the 22 subjects on placebo, however this decrease was not statistically significant (Arbabi et al., 2008).
Compulsive buying
Four double-blind randomized, placebo-controlled trials using antidepressants in CB have been published. In one study, 37 CB subjects were treated with fluvoxamine for 13 weeks. Both the fluvoxamine and placebo groups significantly improved from baseline on measures of CB thoughts/urges and behaviors (Ninan et al., 2000a). Similar results were found by Black et al. (2000) who found no difference in response rates when comparing fluvoxamine to placebo in 23 participants treated for 9 weeks.
In a 7-week citalopram study, researchers found a 63% response rate [measured by a CGI-I score of 1 or 2 and a 50% or greater score decrease in Yale-Brown Obsessive Compulsive Scale – Shopping Version (YBOCS–SV) from baseline] in 24 subjects. Those who responded were entered into the 9-week, double-blind treatment phase. Five (63%) on placebo compared to none on citalopram relapsed (defined as YBOCS–SV score or 17 or more and CGI-I score of “minimally improved” or less). Furthermore, shopping thoughts/urges and behavior increased in the placebo group while decreasing in the citalopram group from week 7 to endpoint (Koran et al., 2003).
An escitalopram study for CB failed to show efficacy for the treatment of CB. Seventeen participants were responders (defined as CGI-I score of a 1 or 2 and YBOCS–SV score of <17, with a 50% or greater decrease from baseline) in a 7-week open-label period and then randomized into a 9-week, double-blind, discontinuation phase. Six (67%) of the placebo group and five (63%) of the active group relapsed (defined as ≥17 and CGI-I score of minimally improved or less) in the discontinuation phase (Koran et al., 2007b).
Compulsive sexual behavior
There is limited research concerning pharmacotherapy in treating CSB. In one 12-week, double-blind, placebo-controlled study, citalopram demonstrated significant reductions in the desire for sex, frequency of masturbation, and hours of pornography use per week in a sample of 28 gay and bisexual men compared to placebo. However, subjects in both groups, reported similar reductions in risky sexual behavior (Wainberg et al., 2006).
Summary of antidepressant treatment of ICDs
Although far from conclusive, the limited data from antidepressant trials for ICDs provide some important clinical and research directions: (1) serotonergic antidepressants may be useful for some of the ICDs (IED, PSP, CB, and CSB); (2) not all serotonergic medications may be equally efficacious (clomipramine resulted in some improvement for TTM whereas fluoxetine did not; fluvoxamine was not effective for CB but citalopram demonstrated some benefit); (3) trials need to be longer due to the high placebo response in individuals with ICDs; and (4) a specific treatment may be beneficial for some individuals with certain ICDs but the treatment may not be broadly effective for everyone with a specific ICD diagnosis. The trials essentially demonstrate that serotonergic antidepressants may have a role in the treatment of certain ICDs or certain individuals with ICDs. For example, Iancu et al. (2008) suggests trying an SSRI for the obsessive–compulsive subtype of PG and starting with bupropion for the addictive subtype. Given the high rates of comorbidity in ICDs and the chronic natures of these disorders, however, the fact that the studies rarely included any comorbidity (except an escitalopram study for PG) and rarely went beyond 3–4 months (except one fluvoxamine and one sertraline study for PG), the generalizability of these findings is still unclear.
Mood Stabilizers/Anti-Epileptics
Pathological gambling
The only placebo-controlled study of a mood stabilizer in PG examined lithium in pathological gamblers with co-occurring bipolar spectrum disorders. The study randomized 40 subjects in a double-blind, placebo-controlled trial for 10 weeks. Results indicated that sustained-release lithium carbonate demonstrate significantly greater improvement than placebo in reducing gambling thoughts/urges and behaviors and overall gambling severity. Furthermore, significantly more subjects on the active medication were rated as responders (defined by a CGI score of 1 or 2 and 35% or greater reducing in PG–YBOCS score) compared to those on placebo (83.3 vs. 29.4%; Hollander et al., 2005).
Intermittent explosive disorder
Ninety-six subjects with Cluster B personality disorders, 116 with IED, and 34 with post-traumatic stress disorder were randomized to 12 weeks of divalproex sodium or placebo. Divalproex was not found to have a significant influence on aggression, irritability, or clinical improvement in the subjects with IED without a Cluster B personality disorder (Hollander et al., 2003).
Another study assessed levetiracetam in 40 subjects with clinically significant impulsive aggression (which met Coccaro and colleagues’ refined criteria for IED) in a 10-week, double-blind, placebo-controlled, variable dose study and found levetiracetam was not superior to placebo on measures of aggression [assessed by the Overt Aggression Scale-Modified (OAS-M)], hostility [assessed by the Brief Psychiatric Rating Scale (BPRS) hostility scale], or patient-rated global improvement (Mattes, 2008).
Pathologic skin picking
The anticonvulsant, lamotrigine, has been used in one double-blind study to treat PSP in 35 subjects in a 12-week study. Lamotrigine failed to demonstrate significant improvement on any measure of PSP severity. Further analysis, however, showed that those who responded to lamotrigine had impaired cognitive flexibility and longer reaction times at baseline compared to lamotrigine non-responders (Grant et al., 2010).
Summary of mood stabilizers/anti-epileptic treatments for ICDs
The data regarding mood stabilizer or anti-epileptic medications in the treatment of ICDs is far too limited to make any useful clinical conclusions. Not all medications in this category have the same pharmacological mechanism and these medications have been tested in only a few of the ICDs. The studies do however demonstrate that classifying subtypes of individuals with ICDs based on perceived pathophysiologies (e.g., gamblers with co-occurring bipolar spectrum disorders or pathological pickers with specific cognitive deficits) may allow for more targeted and more effective pharmacotherapies. Some research has suggested treating the impulsive subtype of PG with mood stabilizers (Iancu et al., 2008). Future studies may want to examine which ICDs, and/or which individuals with specific ICDs, may respond to these medications.
Opioid Antagonists
Pathological gambling
Studies investigating naltrexone in the treatment of PG have produced generally positive results. Forty-five pathological gamblers randomized to 12 weeks of naltrexone or placebo found that naltrexone was significantly more effective at reducing PG urges and behavior (Kim et al., 2001). Similar results were found in an 18-week trial of 77 PG subjects. The naltrexone group had significantly greater decreases in gambling urges and behaviors, and greater overall improvements in gambling severity (Grant et al., 2008). In contrast, Toneatto et al. (2009) found no differences between naltrexone and placebo in terms of gambling frequency or expenditures in a sample of 52 subjects with PG and co-current alcohol use disorder alcoholism. During the 11-week study, subjects also received up to seven sessions of CBT.
A 16-week study of 207 subjects treated with nalmefene found that those on active medication demonstrated significantly greater reductions in gambling symptoms compared to placebo (Grant et al., 2006). A second study of nalmefene in 233 PG subjects treated for 12 weeks with lower doses found that, using an intent-to-treat analysis, nalmefene was not superior to placebo on gambling thoughts/urges and behaviors and overall gambling behaviors. When the analyses were limited to those subjects who achieved the full assigned dose of medication, however, those assigned to 40 mg/day reported significantly greater reduction in gambling urges (Grant et al., 2010).
Trichotillomania
Using a 6-week, double-blind design, 17 individuals with TTM were randomized to receive either naltrexone or placebo. The naltrexone group experienced significant decreases in TTM symptom severity compared to placebo. About half (three of seven) taking naltrexone reported a 50% decrease in hair-pulling symptoms compared to none on placebo. However, groups were not significantly different on measures of number of hair-pulling episodes, level of impairment, and clinician’s ratings of symptoms (O’Sullivan et al., 1999).
Kleptomania
A study of 25 KM subjects randomized into an 8-week, double-blind, placebo-controlled study, found naltrexone significantly reduced urges to steal and stealing behavior compared to placebo. Nineteen of 25 (76%) of all subjects had at least one comorbid disorder, most commonly major depressive (44%) and anxiety (32%) disorders (Grant et al., 2009a).
Summary of opioid antagonist treatments for ICDs
The data regarding the use of opioid antagonists for PG are persuasive and provide the strongest evidence of any medication for the treatment of ICDs. There have been four positive studies and one negative study, although the negative study used dosing of naltrexone which was lower than previously reported in the successful trials. These studies may suggest that dosing of the opioid antagonist may be important for successful clinical outcome. One study also determined that those PG subjects with a family history of alcohol use disorders may respond more robustly to opioid antagonists (Grant et al., 2008). These studies, however, generally did not enroll those with comorbidities (except one naltrexone study which enrolled comorbid alcohol use disorders and one naltrexone study that enrolled subjects with depression and anxiety). The evidence for the use of opioid antagonists in KM is also promising and given that an escitalopram study was negative, this study suggests opioid antagonists may be the direction of choice for future research of this disorder. The evidence for opioid antagonists for TTM are limited by a study with mixed results (some measures positives, others not). This class of medications should be considered the first-line treatment for PG and KM based on the data thus far. Future studies should examine opioid antagonists for a wider range of ICDs.
Atypical Neuroleptics
Pathological gambling
Two studies have assessed the use of olanzapine in treating PG with both finding that olanzapine was no more effective than placebo. In a study of 21 PG subjects treated for 7 weeks with olanzapine, results indicated that all subjects had decreased gambling urges and behaviors but no statistical differences were found between the two groups (Fong et al., 2008). Similarly, McElroy et al. (2008) found that olanzapine was not superior to placebo in a study of 42 subjects in a 12-week study.
Trichotillomania
A 12-week randomized, double-blind, placebo-controlled trial of olanzapine, demonstrated significant improvement on measures of TTM severity in 25 subjects with TTM. Furthermore, 85% of subjects on active medication (compared to 17% in the placebo group) were considered to be full responders (Van Ameringen et al., 2010).
Summary of atypical antipsychotic treatment for ICDs
The data regarding the use of atypical antipsychotic treatment for PG strongly suggest that these medications provide no benefit. The data for TTM, however, are very persuasive although it was a very small study. The questions remains whether different atypical antipsychotics may produce different results in ICDs. Given the side effect profile of these medications, however, they should be used with caution and with monitoring of potential health-related side effects.
Glutamatergic Agents
Pathological gambling
N-acetyl cysteine (NAC) has been found to be effective in decreasing PG symptoms in an 8-week, open-label trial of NAC followed by 6-week, double-blind discontinuation phase, Grant et al. (2007a) found that NAC was effective in reducing gambling thoughts/urges and behaviors and improving level of functioning in 27 subjects. Of those responder subjects randomized to NAC, 83.3% still met responder criteria, while 28.6% assigned to placebo met responder criteria.
Trichotillomania
Using a sample of 50 individuals with TTM, subjects randomized to receive NAC for 12 weeks had significantly greater reductions in TTM symptomology on both the MGH-HPS (self-report scale) and the Psychiatric Institute Trichotillomania Scale (clinician- administered scale). Over half (56%) in the active medication group were rated as “much” or “very much” improved, compared to 16% of those assigned to placebo (Grant et al., 2009b).
Summary of glutamatergic agents for ICDs
The data regarding the use of NAC for both TTM and PG are encouraging. Both studies enrolled subjects with co-occurring anxiety and depression and therefore the results may generalize better to the population at large. The studies highlight that focusing on the glutamate system may be potentially beneficial when considering treatment for ICDs.
Summary
Treating ICDs is difficult because individuals with ICDs often are conflicted with the desire to engage in the behavior and their desire to stop the behavior. Thus, physicians should carefully assess the situations that cause individuals to seek help. Clinicians also need to stay cognizant of comorbid disorders because ICD symptomology may worsen with co-occurring disorders and co-occurring disorders may interfere with treatment outcomes. Most pharmacological trials have excluded individuals with current co-occurring primary Axis I disorders. With such high proportions of ICD patients enduring co-occurring conditions, future clinical trials should investigate how specific comorbidities distinctly influence treatment results. These findings will advance knowledge about the efficacy of treatment for these often co-occurring problems.
Although ICDs present significant public health concerns, researchers and clinicians have paid relatively little attention to these conditions. As represented in this article, significant advances have been made in the exploration of pharmacological treatments for ICDs. Further advances, however, must be made. Generalizability of these studies is limited as the majority of samples lack adequately powered samples, high placebo-response rates, and limited follow-up periods. Additional large-scale, placebo-controlled, comparative pharmacological treatment studies need to be completed to find the most effective treatments for ICDs. Furthermore, the replication of promising treatment studies and additional clinical trials comparing medications and therapies are needed to accurately assess which treatments are effective and in whom. Knowledge gained from these studies will not only advance the treatment of ICDs, but also significantly improve the lives of those with ICDs and those who are directly and indirectly affected by their conditions.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This research was supported in part by a Center for Excellence in Gambling Research grant by the Institute for Responsible Gaming and an American Recovery and Reinvestment Act (ARRA) Grant from the National Institute on Drug Abuse (1RC1DA028279-01; Dr. Grant). Dr. Grant has received research grants from Forest Pharmaceuticals. Mr. Odlaug has received honoraria from Oxford University Press and Current Medicine Group, LLC.
References
American Psychiatric Association. (2000). Diagnositic and Statistical Manual of Mental Disorders, 4th Edn, Text-Revised: DSM-IV-TR. Washington, DC: American Psychiatric Publishing, Inc.
American Psychiatric Association. (2010). DSM-5 Development. Available at: http://www.dsm5.org/ProposedRevisions/Pages/Impulse-ControlDisordersNotElsewhereClassified.aspx (accessed October 12, 2010).
Arbabi, M., Farina, V., Balighi, K., Mohammadi, M. R., Nejati-Safa, A. A., Yazdchi, K., Golestan, B., and Darvish, F. (2008). Efficacy of citalopram in treatment of pathological skin picking: a randomized double blind placebo controlled trial. Acta Med. Iran 46, 367–372.
Arieff, A. J. B., and Bowie, C. G. (1947). Psychiatric aspects of shoplifting. Arch. Neurol. Psychiatry 57, 777–778.
Arnold, L. M., Auchenbach, M. B., and McElroy, S. L. (2001). Psychogenic excoriation: clinical features, proposed diagnostic criteria, epidemiology and approaches to treatment. CNS Drugs 15, 351–359.
Arnold, L. M., McElroy, S. L., Mutasim, D. F., Dwight, M. M., Lamerson, C. L., and Morris, E. M. (1998). Characteristics of 34 adults with psychogenic excoriation. J. Clin. Psychiatry 59, 509–514.
Black, D. W., Arndt, S., Coryell, W. H., Argo, T., Forbush, K. T., Shaw, M. C., Perry, P., and Allen, J. (2007). Bupropion in the treatment of pathological gambling: a randomized, double-blind, placebo-controlled, flexible-dose study. J. Clin. Psychopharmacol. 27, 143–150.
Black, D. W., Gabel, J., Hansen, J., and Schlosser, S. (2000). A double-blind comparison of fluvoxamine versus placebo in the treatment of compulsive buying disorder. Ann. Clin. Psychiatry 12, 205–211.
Black, D. W., Kehrberg, L. L. D., Flumerfelt, D. L., and Schlosser, S. S. (1997). Characteristics of 36 subjects reporting compulsive sexual behavior. Am. J. Psychiatry 154, 243–249.
Black, D. W., Repertinger, S., Gaffney, G., and Gabel, J. (1998). Family history and psychiatric comorbidity in persons with compulsive buying: preliminary findings. Am. J. Psychiatry 155, 960–963.
Blanco, C., Petkova, E., Ibáñez, A., and Sáiz-Ruiz, J. (2002). A pilot placebo-controlled study of fluvoxamine for pathological gambling. Ann. Clin. Psychiatry 14, 9–15.
Blaszczynski, A., and Steel, Z. (1998). Personality disorders among pathological gamblers. J. Gambl. Stud. 14, 51–71.
Bloch, M. R., Elliott, M., Thompson, H., and Koran, L. M. (2001). Fluoxetine in pathologic skin-picking: open-label and double-blind results. Psychosomatics 42, 314–319.
Bloch, M. R., Landeros-Weisenberger, A., Dombrowski, P., Kelmendi, B., Wegner, R., Nudel, J., Pittenger, C., Leckman, J. F., and Coric, V. (2007). Systematic review: pharmacological and behavioral treatment for trichotillomania. Biol. Psychiatry 62, 839–846.
Carries, P., and Delmonico, D. (1996). Childhood abuse and multiple addictions: research findings in a sample of self-identified sexual addicts. Sex. Addict. Compulsivity 3, 258–268.
Christenson, G. A., Mackenzie, T. B., Mitchell, J. E., and Callies, A. L. (1991). A placebo-controlled, double-blind crossover study of fluoxetine in trichotillomania. Am. J. Psychiatry 148, 1566–1571.
Christenson, G. A., Pyle, R., and Mitchell, J. (1991). Estimated lifetime prevalence of trichotillomania in college students. J. Clin. Psychol. 52, 415–417.
Coccaro, E. F., (2010). A family history study of intermittent explosive disorder. J. Psychiatr. Res. 44, 1011–1015.
Coccaro, E., Lee, R., and Kavoussi, R. (2009). A double-blind, randomized, placebo-controlled trial of fluoxetine in patients with intermittent explosive disorder. J. Clin. Psychol. 70, 653–662.
Coccaro, E., Schmidt, C., Samuels, J., and Nestadt, G. (2004). Lifetime and 1-month prevalence rates of intermittent explosive disorder in a community sample. J. Clin. Psychol. 65, 820–824.
Cohen, L., Stein, D., Simeon, D., Spadaccini, E., Rosen, J., Aronowitz, B., and Hollander, E. (1995). Clinical profile, comorbidity, the treatment history in 123 hair pullers: a survey study. J. Clin. Psychol. 56, 319–326.
Coleman, E. (1992). Is your patient suffering from compulsive sexual behavior? Psychiatric Ann. 22, 320–325.
Diefenbach, G., Tolin, D., Hannan, S., Crocetto, J., and Worhunsky, P. (2005). Trichotillomania: impact on psychosocial functioning and quality of life. Behav. Res. Ther. 43, 869–884.
Fong, T., Kalechstein, A., Bernhard, B., Rosenthal, R., and Rugle, L. (2008). A double-blind, placebo-controlled trial of olanzapine for the treatment of video poker pathological gamblers. Pharmacol. Biochem. Behav. 89, 298–303.
Gambling Impact and Behavior Study. (1999). Report to the National Gambling Impact Study Commission. Chicago, IL: National Opinion Research Center at the University of Chicago. Available at: http://www.norc.uchicago.edu/new/gamb-fin.htm (accessed July 14, 2010).
Grant, J. E. (2008). Impulse Control Disorders: A Clinician’s Guide to Understanding and Treating Behavioral Addictions. New York: W.W. Norton & Company.
Grant, J. E., and Kim, S. W. (2001). Demographic and clinical features of 131 adult pathological gamblers. J. Clin. Psychiatry 62, 957–962.
Grant, J. E., and Kim, S. W. (2002). Clinical characteristics and associated psychopathology of 22 patients with kleptomania. Compr. Psychiatry 43, 378–384.
Grant, J. E., and Kim, S. W. (2007). Clinical characteristics and psychiatric comorbidity of pyromania. J. Clin. Psychol. 68, 1717–1722.
Grant, J. E., Kim, S. W., and Hartman, B. (2008). A double-blind, placebo-controlled study of the opiate antagonist naltrexone in the treatment of pathological gambling urges. J. Clin. Psychiatry 69, 783–739.
Grant, J. E., Kim, S. W., and Odlaug, B. L. (2007a). N-acetyl cysteine, a glutamate-modulating agent, in the treatment of pathological gambling: a pilot study. Biol. Psychiatry 62, 652–657.
Grant, J. E., Williams, K. A., and Potenza, M. N. (2007b). Impulse-control disorders in adolescent psychiatric inpatients: co-occurring disorders and sex differences. J. Clin. Psychiatry 68, 1584–1592.
Grant, J. E., Kim, S. W., and Odlaug, B. L. (2009a). A double-blind, placebo- controlled study of the opiate antagonist, naltrexone, in the treatment of kleptomania. Biol. Psychiatry 65, 600–606.
Grant, J. E., Odlaug, B. L., and Kim, S. W. (2009b). N-acetylcysteine, a glutamate modulator, in the treatment of trichotillomania: a double-blind, placebo-controlled study. Arch. Gen. Psychiatry 66, 756–763.
Grant, J. E., Kim, S. W., Potenza, M. N., Blanco, C., Ibáñez A., Steven, L., Hektner, J. M., and Zaninelli, R. (2003). Paroxetine treatment of pathological gambling: a multi-centre randomized controlled trial. Int. Clin. Psychopharmacol. 18, 243–249.
Grant, J. E., Levine, L., Kim, D., and Potenza, M. N. (2005). Impulse control disorders in adult psychiatric inpatients. Am. J. Psychiatry 162, 2184–2188.
Grant, J. E., Odlaug, B. L., Chamberlain, S., and Kim, S. W. (2010). A double-blind, placebo-controlled trial of lamotrigine for pathological skin picking: treatment efficacy and neurocognitive predictors of response. J. Clin. Psychopharmacol. 30, 396–403.
Grant, J. E., Odlaug, B. L., Potenza, M. N., Hollander, E., and Kim, S. W. (2010). Nalmefene in the treatment of pathological gambling: multicentre, double-blind, placebo-controlled study. Br. J. Psychiatry 197, 330–331.
Grant, J. E., and Potenza, M. N. (2004). Pathological Gambling: A Clinical Guide to Treatment. Washington, DC: American Psychiatric Publishing, Inc.
Grant, J. E., and Potenza, M. N. (2006). Escitalopram treatment of pathological gambling with co-occurring anxiety: an open-label pilot study with double-blind discontinuation. Int. Clin. Psychopharmacol. 21, 203–209.
Grant, J. E., Potenza, M. N., Hollander, E., Cunningham-Williams, R., Nurminen, T., Smits, G., and Kallio, A. (2006). Multicenter investigation of the opioid antagonist nalmefene in the treatment of pathological gambling. Am. J. Psychiatry 163, 303–312.
Hayes, S. L., Storch, E. A., and Berlanga, L. (2009). Skin picking behaviors: an examination of the prevalence and severity in a community sample. J. Anxiety Disord. 23, 314–319.
Hollander, E., DeCaria, C., Finkell, J., Begaz, T., Wong, C., and Cartwright, C. (2000). A randomized double-blind fluvoxamine/placebo crossover trial in pathologic gambling. Biol. Psychiatry 47, 813–817.
Hollander, E., Pallanti, S., Allen, A., Sood, E., and Rossi, N. (2005). Does sustained-release lithium reduce impulsive gambling and affective instability versus placebo in pathological gamblers with bipolar spectrum disorders? Am. J. Psychiatry 162, 137–145.
Hollander, E., Tracy, K., Swann, A., Coccaro, E. F., McElroy, S. L., Wozniak, P., Sommerville, K. W., and Nemerff, C. B. (2003). Divalproex in the treatment of impulsive aggression: efficacy in cluster B personality disorders. Neuropsychopharmacology 28, 1186–1197.
Iancu, I., Lowengrub, K., Dembinsky, Y., Kotler, M., and Dannon, P. N. (2008). Pathological gambling: an update on neuropathophysiology and pharmacotherapy. CNS Drugs 22, 123–138.
Kafka, M. (2010). Hypersexual disorder: a proposed diagnosis for DSM-V. Arch. Sex. Behav. 39, 377–400.
Kafka, M., and Prentky, R. (1992). A comparative study of nonparaphilic sexual addictions and paraphilias in men. J. Clin. Psychiatry 53, 345–350.
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K., and Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 62, 593–602.
Kessler, R. C., Coccaro, E., Fava, M., Jaeger, S., Jin, R., and Walters, E. (2006). The prevalence and correlates of DSM-IV intermittent explosive disorder in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 63, 669–678.
Kessler, R. C., Hwang, I., LaBrie, R., Petukhova, M., Sampson, N. A., Winters, K. C., and Shaffer, H. J. (2008). The prevalence and correlates of DSM-IV pathological gambling in the National Comorbidity Survey Replication. Psychol. Med. 38, 1351–1360.
Keuthen, N., Koran, L., Aboujaoude, E., Large, M., and Serpe, R. (2010). The prevalence of pathologic skin picking in US adults. Compr. Psychiatry 51, 183–186.
Kim, S. W., Grant, J. E., Adson, D., and Shin, Y. (2001). Double-blind naltrexone and placebo comparison study in the treatment of pathological gambling. Biol. Psychiatry 49, 914–921.
Kim, S. W., Grant, J. E., Adson, D., Shin, Y., and Zaninelli, R. (2002). A double-blind placebo-controlled study of the efficacy and safety of paroxetine in the treatment of pathological gambling. J. Clin. Psychiatry 63, 501–507.
Koran, L. M., Aboujaoude, E., and Gamel, N. N. (2007a). Escitalopram treatment of kleptomania: an open-label trial followed by double-blind discontinuation. J. Clin. Psychiatry 63, 422–427.
Koran, L. M., Aboujaoude, E., Solvason, B., Gamel, N., and Smith, E. (2007b). Escitalopram for compulsive buying disorder: a double-blind discontinuation study. J. Clin. Psychopharmacol. 27, 225–227.
Koran, L. M., Chuong, H., Bullock, K., and Smith, S. (2003). Citalopram for compulsive shopping disorder: an open-label study followed by double-blind discontinuation. J. Clin. Psychiatry 64, 793–798.
Koran, L. M., Faber, R. J., Aboujaoude, E., Large, M. D., and Serpe, R. T. (2006). Estimated prevalence of compulsive buying behavior in the United States. Am. J. Psychiatry 163, 1806–1812.
Lejoyeux, M., Arbaretaz, M., McLoughlin, M., and Adès, J. (2002). Impulse control disorders and depression. J. Nerv. Ment. Dis. 190, 310–314.
Lochner, C., Simeon, D., Niehaus, D., and Stein, D. (2002). Trichotillomania and skin-picking: a phenomenological comparison. Depress. Anxiety 15, 83–86.
Mattes, J. (2008). Levetiracetam in patients with impulsive aggression: a double-blind, placebo-controlled trial. J. Clin. Psychol. 69, 310–315.
McElroy, S. L., Keck, P. E. Jr., Pope, H. G. Jr., Smith, J. M., and Strakowski, S. M. (1994). Compulsive buying: a report of 20 cases. J. Clin. Psychiatry 55, 242–248.
McElroy, S. L., Nelson, E., Welge, J., Kaehler, L., and Keck, P. Jr. (2008). Olanzapine in the treatment of pathological gambling: a negative randomized placebo-controlled trial. J. Clin. Psychiatry 69, 433–440.
McElroy, S. L., Pope, H. G. Jr., Hudson, J. I., Keck, P. E. Jr., and White, K. L. (1991). Kleptomania: a report of 20 cases. Am. J. Psychiatry 148, 652–657.
McElroy, S. L., Soutullo, C. A., Beckman, D. A., Taylor, P. Jr., and Keck, P. E. Jr. (1998). DSM-IV intermittent explosive disorder: a report of 27 cases. J. Clin. Psychol. 59, 203.
McNeilly, D., and Burke, W. (1998). Stealing lately: a case of late-onset kleptomania. Int. J. Geriatr. Psychiatry 3, 116–121.
Miltenberger, R. G., Rapp, J., and Long, E. (2006). “Characteristics of trichotillomania,” in Tic Disorders, Trichotillomania, and Other Repetitive Behavior Disorders, eds D. W. Woods and R. G. Miltenberger (New York, NY: Springer), 133–150.
Ninan, P., McElroy, S., Kane, C. P., Knight, B. T., Casuto, L. S., Rose, S. E., Marsteller, F. A., and Nemeroff, C. B. (2000a). Placebo-controlled study of fluvoxamine in the treatment of patients with compulsive buying. J. Clin. Psychopharmacol. 20, 362–366.
Ninan, P., Rothbaum, B., Marsteller, F., Knight, B., and Eccard, M. (2000b). A placebo-controlled trial of cognitive-behavioral therapy and clomipramine in trichotillomania. J. Clin. Psychiatry 61, 47–50.
Odlaug, B. L., and Grant, J. E. (2008a). Trichotillomania and pathological skin picking: clinical comparison with an examination of comorbidity. Ann. Clin. Psychiatry 20, 57–63.
Odlaug, B. L., and Grant, J. E. (2008b). Clinical characteristics and medical complications of pathologic skin picking. Gen. Hosp. Psychiatry 30, 61–66.
Odlaug, B. L., and Grant, J. E. (2010). Impulse-control disorders in a college sample: results from the self-administered Minnestoa Impulse Disorders Interview (MIDI). Prim. Care Companion J. Clin. Psychiatry 12, e1–e5.
O’Sullivan, R., Christenson, G., and Stein, D. (1999). “Pharmacotherapy of trichotillomania,” in Trichotillomania, eds D. Stein, G. Christenson, and E. Hollander (Washington, DC: American Psychiatric Press), 93–124.
Petry, N. M., and Kiluk, B. (2002). Suicidal ideation and suicide attempts in treatment-seeking pathological gamblers. J. Nerv. Ment. Dis. 190, 462–469.
Petry, N. M., Stinson, F. S., and Grant, B. F. (2005). Comorbidty of DSM-IV pathological gambling and other psychiatric disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions. J. Clin. Psychiatry 66, 564–574.
Phelan, J. E. (2002). Childhood kleptomania: two clinical case studies with implications for further research. Psychol. Educ. 39,19–21.
Potenza, M. (2006). Should addictive disorders include non-substance related conditions. Addiction 101(Suppl. 1), 142–151.
Repo, E., Virkkunen, M., Rawlings, R., and Linnoila, M. (1997). Criminal and psychiatric histories of Finnish arsonists. Acta Psychiatr. Scand. 95, 318–323.
Sáiz-Ruiz, J., Blanco, C., Ibáñez, A., Masramon, X., Gomez, M. M., Madrigal, M., and Diez, T. (2005). Sertraline treatment of pathological gambling: a pilot study. J. Clin. Psychiatry 66, 28–33.
Schlosser, S., Black, D. W., Repertinger, S., and Freet, D. (1994). Compulsive buying: demography, phenomenology, and comorbidity in 46 subjects. Gen. Hosp. Psychiatry 16, 205–212.
Schlueter, G. R., O’Neal, F. C., Hickey, J., and Seiler, G. L. (1989). Rational vs. nonrational shoplifting types: the implications for loss prevention strategies. Int. J. Offender Ther. Comp. Criminol. 33, 227–229.
Schneider, J., and Schneider, B. (1996). Couple recovery from sexual addiction/co addiction: results of a survey of 88 marriages. Sex. Addict. Compulsivity 3, 111–126.
Simeon, D., Stein, D., Gross, S., Islam, N., Schmeidler, J., and Hollander, E. (1997). A double-blind trial of fluoxetine in pathologic skin picking. J. Clin. Psychiatry 58, 341–347.
Stein, D. J., Grant, J. E., Franklin, M. E., Keuthen, N., Lochner, C., Singer, H. S., and Woods, D. W. (2010). Trichotillomania (hair pulling disorder), skin picking disorder, and stereotypic movent disorder: toward DSM-V. Depress. Anxiety 27, 611–626.
Streichenwein, S., and Thornby, J. (1995). A long-term, double-blind, placebo-controlled crossover trial of the efficacy of fluoxetine for trichotillomania. Am. J. Psychiatry 152, 1192–1196.
Swedo, S., Leonard, H., Rapoport, J., Lenane, M., Goldberger, E., and Cheslow, D. (1989). A double-blind comparison of clomipramine and desipramine in the treatment of trichotillomania (hair pulling). N. Engl. J. Med. 321, 497–501.
Toneatto, T., Brands, B., and Selby, P. (2009). A randomized, double-blind, placebo-controlled trial of naltrexone in the treatment of concurrent alcohol use disorder and pathological gambling. Am. J. Addict. 18, 219–225.
Van Amerigen, M., Mancini, C., Patterson, B., Bennett, M., and Oakman, J. (2010). A randomized, double-blind, placebo-controlled trial of olanzapine in the treatment of trichotillomania. J. Clin. Psychiatry 71, 1336–1343.
Van Minnen, A., Hoogduin, K., Keijsers, G., Hellenbrand, I., and Hendriks, G. (2003). Treatment of trichotillomania with behavioral therapy or fluoxetine: a randomized, waiting-list controlled study. Arch. Gen. Psychiatry 60, 517–522.
Wainberg, M., Muench, F., Morgenstern, J., Hollander, E., Irwin, T. W., Parsons, J. T., Allen, A., and O’Leary, A. (2006). A double-blind study of citalopram versus placebo in the treatment of compulsive sexual behaviors in gay and bisexual men. J. Clin. Psychiatry 67, 1968–1973.
Woods, D. W., Flessner, C. A., Franklin, M. E., Keuthen, N. J., Goodwin, R. D., Stein, D. J., Walther, M. R., and the Trichotillomania Learning Center-Scientific Advisory Board. (2006). The Trichotillomania Impact Project (TIP): exploring phenomenology, functional impairment, and treatment utilization. J. Clin. Psychol. 67, 1877–1888.
Keywords: impulse control disorders, pharmacotherapy, clinical characteristics
Citation: Schreiber L, Odlaug BL and Grant JE (2011) Impulse control disorders: updated review of clinical characteristics and pharmacological management. Front. Psychiatry 2:1. doi: 10.3389/fpsyt.2011.00001
Received: 09 August 2010;
Accepted: 10 February 2011;
Published online: 21 February 2011.
Edited by:
Dan J. Stein, University of Cape Town, South AfricaReviewed by:
Dan J. Stein, University of Cape Town, South AfricaRobert David Rogers, Oxford University, UK
Copyright: © 2011 Schreiber, Odlaug and Grant. This is an open-access article subject to an exclusive license agreement between the authors and Frontiers Media SA, which permits unrestricted use, distribution, and reproduction in any medium, provided the original authors and source are credited.
*Correspondence: Jon E. Grant, Department of Psychiatry, University of Minnesota Medical Center, 2450 Riverside Avenue, Minneapolis, MN 55454, USA. e-mail: grant045@umn.edu