 Kathrin Malejko
Kathrin Malejko Birgit Abler
Birgit Abler Paul L. Plener2
Paul L. Plener2- 1Department of Psychiatry and Psychotherapy III, University Hospital Ulm, Ulm, Germany
- 2Department of Child and Adolescent Psychiatry and Psychotherapy, University Hospital Ulm, Ulm, Germany
Objectives: Post-traumatic stress disorder (PTSD) is a common psychiatric disease with changes in neural circuitries. Neurobiological models conceptualize the symptoms of PTSD as correlates of a dysfunctional stress reaction to traumatic events. Functional imaging studies showed an increased amygdala and a decreased prefrontal cortex response in PTSD patients. As psychotherapeutic approaches represent the gold standard for PTSD treatment, it is important to examine its underlying neurobiological correlates.
Methods: Studies published until August 2016 were selected through systematic literature research in the databases PubMed, PsychInfo, and Cochrane Library’s Central Register of Controlled Trials or were identified manually by searching reference lists of selected articles. Search terms were “neural correlates” OR “fMRI” OR “SPECT,” AND “therapy” AND “PTSD.” A total of 19 articles were included in the present review whereof 15 studies compared pre-to-post-therapy signal changes, six studies related pre-treatment activity to pre-to-post-symptom improvement, and four studies compared neural correlates of responders versus non-responders. The disposed therapy forms were cognitive behavioral therapy (CBT), eye movement desensitization and reprocessing, cognitive therapy, exposure therapy, mindfulness-based intervention, brief eclectic psychotherapy, and unspecified therapy.
Results: Successful psychotherapy of PTSD was repeatedly shown to be accompanied by decreased activity in the amygdala and the insula as well as increased activity in the dorsal anterior cingulate cortex (dACC) and hippocampus. Elevated dACC activity prior to treatment was related to subsequent treatment success and a positive predictor for treatment response. Elevated amygdala and insula pre-treatment activities were related to treatment failure.
Discussion: Decreased activity in limbic brain regions and increased activity in frontal brain areas in PTSD patients after successful psychotherapeutic treatment might reflect regained top-down control over previously impaired bottom-up processes.
Introduction
During lifetime, 60.7% of men and 51.2% of women experience at least one potentially traumatic event such as being taken hostage or being kidnaped, experiencing or witnessing sexual or physical assault, torture, a terrorist attack, a severe car accident, a natural disaster, war, or the unexpected death of a beloved person (1). A significant proportion of these events already occurs during young age, as 26% of male and 18% of female subjects reported of having experienced at least one traumatic event in a representative community sample (n = 3.021, age 14–24 years) (2). Of those experiencing potentially traumatic events, 10–40% develop psychiatric symptoms of clinical relevance (3–7) such as affective disorders, substance abuse, or post-traumatic stress disorder (PTSD). The latter goes hand in hand with significant impairments of psychological and physical health (1, 7), elevated levels of suicidality (8) as well as with a decreased level of social functioning (9).
The reason why some individuals, who have experienced a traumatic event develop a PTSD while others do not, is still not clearly understood (10). Some factors like an own or family history of psychiatric disorders before the traumatic event took place, the experience of a traumatic event early in lifetime, and/or female gender were shown to be associated with an elevated risk for developing PTSD (3, 11). Furthermore, sociodemographic and ethnologic factors play an important role, when it comes to varying prevalence rates for PTSD (7, 8, 12, 13).
Neurobiological models conceptualize the symptoms of PTSD as correlates of a dysfunctional stress reaction to traumatic events (14). This hypothesis is based on observations such as changes in the hypothalamic–pituitary–adrenal axis in PTSD patients. An abnormal downregulation of cortisol seems to result in sustained, increased levels of corticotropin-releasing hormone, which leads to a higher release of adrenocorticotropic hormone stimulating the release of glucocorticoids in turn (15). The sustained glucocorticoid exposure has been suggested to promote hippocampal atrophy as indicated by neuroimaging studies showing reduced hippocampal volumes in PTSD patients (16). Some initial hypotheses have been brought up linking neurobiological changes to altered mechanisms of extinction and hyperarousal, flashbacks, and avoidance behavior as the core symptoms of PTSD (14). For example, functional imaging studies including stressful tasks (stressful scripts, cues, and trauma reminders) showed a decreased response of the prefrontal cortex and an increased amygdala response in PTSD patients (17). Following this line of thought, it has been postulated that in patients with PTSD, stimulators of the limbic stress system prevail over inhibitors. Such an impaired top-down cognitive control over limbic areas, which is frequently associated with hypoactivation in the dlPFC might also explain flashbacks (18). In PTSD, neutral cues become associated with the traumatic event and may trigger a conditioned fear response. Failure to extinguish the conditioned fear is thought to lead to the persistence of symptoms (19). It has been suggested that the interaction between amygdala and the hippocampus, as two regions that play a critical role in the consolidation of emotionally laden memories, may contribute to the intrusive nature of trauma recollection in PTSD (20).
Diverse pharmacological as well as psychotherapeutic approaches have been suggested for the treatment of PTSD, while the latter represents the gold standard and pharmacological treatment rather constitutes an adjuvant form of symptom control. Following guidelines (21), patients should be offered a trauma-focused psychotherapy such as cognitive behavioral therapy (CBT) (22), eye movement desensitization and reprocessing (EMDR) (23), or prolonged exposure therapy (ET) (24).
CBT helps patients to question and alter dysfunctional trauma-associated cognitions. In vivo or in sensu confrontation with trauma reminders helps patients to overcome their avoidance of situations and thoughts that are no longer dangerous, which leads to habituation and a reorganization of trauma memories finally (25).
During EMDR, patients mentally focus a trauma-associated disturbing image, memory, emotion, or cognition. In comparison to CBT, confrontation is rather short and interrupted by saccadic eye movements that are initiated by the therapist (25, 26). The influence of rapid eye movements is not clearly understood yet. Mechanisms discussed are (1) focusing inner thoughts and feelings on the one hand and external stimuli (e.g., finger moves) on the other, might form an ideal attention level that is necessary for reconsolidation; (2) focusing external stimuli while reprocessing traumatic memories leads to a certain degree of distraction that prevents patients from being overwhelmed by their traumatic memories during the processing stage; (3) moving fingers might induce a certain degree of relaxation (activation of the parasympathetic system), which is then conditionally associated with traumatic memories resulting in releasing effects (25, 27, 28). Thus, besides habituation and conditioning learning processes as in CBT, modulation of attentional processing and facilitation of gaining cognitive control are suggested mechanisms of action.
Prolonged ET is a manualized (24) and effective (29, 30) psychotherapy for the treatment of PTSD. Virtual reality ET is a frequently used version of ET for treating combats, by providing realistic visual, auditory, and even tactile and olfactory cues that can be presented in a graduated manner. Habituation to anxious memories seems to be one of the key mechanisms here.
All treatment forms have in common that traumatic events or memories should no longer be avoided but confrontation on a behavioral (ET) or cognitive (CBT, EMDR) level should take place until a certain degree of fear extinction and habituation has been reached. CBT and EMDR furthermore question trauma-associated dysfunctional cognitions and replace them by more functional ones (top-down processing). Habitation and altered cognitions normally result in reduced feelings of anxiety and physiological arousal. Furthermore, confrontation with aversive stimuli and memories during therapy leads to fear extinction (31). Regarding PTSD, it was argued that extinction may not be based on an erasure of original information, but may rather reflect new learning (32).
Several neuroimaging studies attempted to examine neurobiological aspects of psychotherapeutic interventions in PTSD. The impact of trauma-focused psychotherapy on the stress system is thought to be primarily mediated by learning processes (33, 34), which is expected to be represented by changes in neurobiology. Conditional learning and extinction processes have been linked to the hippocampus and basal ganglia functioning. Biased memory for negative stimuli as in depression, but also PTSD has been suggested to result from an interaction of these regions with a hyperactive amygdala. Increased reciprocal signaling in this network may lead to sustained hyperactivity (18). Furthermore, biased processing of negative information has been linked to hypoactivity of the prefrontal cortex while biased attentional processes were also related to altered ACC activation (18). Psychotherapeutic interventions addressing these processes should, therefore, influence the activation within these areas. Accordingly, previous neuroimaging studies in adults with PTSD after psychotherapeutic intervention found decreased activity in the amygdala and an increased activity in frontal areas (35).
The assessment of neural correlates of successful psychotherapeutic treatment in adolescents with PTSD might allow for tailoring treatments to the special needs and characteristics of this population and has been suggested to have a potential for the identification of neurobiological markers that can serve as predictors for subsequent therapeutic success. We present a systematic review of the current state of the literature regarding neuroimaging and psychotherapy of PTSD.
Materials and Methods
Search Strategy and Inclusion Criteria
Studies published until August 2016 were selected through search in the databases PubMed, PsychInfo, and Cochrane Library’s Central Register of Controlled Trials. Additional studies were identified manually by searching reference lists of selected articles. Search terms were “neural correlates” OR “functional Magnetic Resonance Imaging (fMRI)” OR “Single Photon Emission Computed Tomography (SPECT),” AND “therapy” AND “PTSD.” The following inclusion criteria were applied: (a) published, peer-reviewed original articles, (b) studies focusing on PTSD, (c) assessment of neural correlates of PTSD by means of SPECT or fMRI, (d) active paradigms or resting state, (e) psychotherapeutic treatments, and (f) longitudinal design with respect to PTSD symptom assessment. Initial screening (titles and abstracts) and check for eligibility criteria on full-texts were conducted independently by the first author (Kathrin Malejko) and the last (Joana Straub) author. Discrepancies were finally resolved by consensus.
Results
Search Results and Study Characteristics
All together, 55 references were initially identified through database search and abstracts were read. One study was found by searching reference lists of selected articles manually. Finally, 19 articles were included in the present review. The other articles either did not deal with psychotherapeutic treatments, reported results of cross-sectional designs, or reported morphological data. The mean number of participants per study was M = 16.53 (SD = 8.04; span: 6–41), and studies were predominantly conducted in adults (n = 17) and only two in minors. Patients suffering from PTSD reported the experience of a vehicle accident in two studies, five studies were conducted on patients with a history of physical or sexual assault, five on war related-, two on job related- (e.g., as policeman), and five studies on various traumatic events. Ten studies also included a control group, such as PTSD waitlist patients (n = 2), healthy trauma controls (HTC) without PTSD (n = 6), healthy controls (HC) without the experience of a trauma (n = 3) and no control group (n = 8) (several answers possible). Neuroimaging assessments were done by means of fMRI (n = 14) and SPECT (n = 5). In two fMRI studies, resting state brain activation was assessed, the others applied an emotional face paradigm (n = 4), paradigms with other emotional content (n = 3), trauma script (n = 4), an (emotional) stroop task (n = 3), or a Go/NoGo task (n = 2). The disposed therapy forms were CBT (n = 9), EMDR (n = 4), cognitive therapy (n = 1), ET (n = 2), mindfulness-based intervention (n = 1), brief eclectic psychotherapy (n = 1), and unspecified psychotherapy (n = 1). Seventeen studies compared pre-to-post-therapy signal changes and two studies related pre-treatment activity to pre-to-post-symptom improvement.
Neurobiological Markers
The majority of studies included in the present literature review found that clinical symptom improvement went along with pre-to-post-treatment signal reductions in the (left-/middle-) insula (three out of four studies) (36–39) and amygdala (four out of five studies) (35, 37, 38, 40, 41) as well as with signal enhancement in the dACC (five out of six studies) (36, 37, 39–42), hippocampus (two out of three studies) (35, 43, 44), PFC (three out of five studies) (35, 37, 40–42), and vACC (two out of three studies) (35, 43, 44). Less consistent results, regarding the direction of pre-to-post-differences, were found for the frontal cortex, thalamus, and temporal gyrus (35, 43, 45–47). Inconsistent results might be drawn back on different paradigms and control groups applied as well as to divergent types of underlying traumas.
Elevated pre-treatment activities in the insula and amygdala were associated with treatment failure (three out of four studies) (39, 48, 49). However, enhanced pre-treatment dACC activity was related to subsequent treatment success (two out of three studies) (37, 39, 48) as well as altered pre-treatment activities in the frontal cortex and IPL (16, 50, 51).
Treatment responders revealed decreased ventral insula activity and increased dACC while non-responders revealed increased amygdala and vACC activity prior to treatment (48, 51).
Taking a closer look at the insula, studies named inferior (36) and anterior areas (37) as important. Considering the ACC more closely, authors found activation of the rostral (43), subgenual (44), and dorsal (36) parts to be associated with successful treatment of PTSD. Also, when it comes to the frontal cortex, authors highlighted subregions such as the prefrontal lobe (35, 40), inferior frontal gyrus (43), dlPFC (37, 47), and ventromedial PFC (41).
In the following, differences concerning within- versus between-group analyses will be depicted: within-group analyses in PTSD patients revealed a decreased pre-to-post-treatment insula activity (37, 38) and the comparison with HTC showed heterogeneous findings (36, 39). A decreased pre-to-post-treatment amygdala activity in PTSD patients were found in both, within-group analyses (37, 38) and when being compared to PTSD waitlist patients (35, 40). Within-group analyses with respect to pre-to-post-treatment activity changes in the hippocampus revealed heterogeneous results (43, 44) and the comparison of PTSD patients with PTSD waitlist patients (35) showed a pre-to-post-signal increase in the hippocampus and vACC. In PTSD patients, increased pre-to-post-treatment dACC activity was shown for within-group analyses (37) as well as compared to PTSD waitlist patients (40, 42). There was no difference between PTSD patients and PTSD waitlist patients found before treatment (42). However, heterogeneous activity changes were shown when being compared to HTC (36, 39, 41). PTSD patients after successful treatment revealed decreased within-group activity (37) and increased pre-to-post-treatment activity in the PFC as compared to PTSD waitlist patients (35, 42). PTSD patients showed an increased global tracer uptake compared to HTC, which disappeared after treatment (50). In PTSD patients, an increased pre-treatment activity was found in the insula, dACC, and frontal gyrus compared to HTC (36, 47).
Only a few studies compared activity levels of patients with PTSD to activity levels of HC (41, 48). Bryant et al. (48) compared pre-treatment activity in PTSD patients with HC and found elevated dACC activity levels in treatment responders compared to HC. However, none of them studied whether activity levels post-treatment indeed approximate those of HC.
For detailed results, see Table 1 and Figure 1.
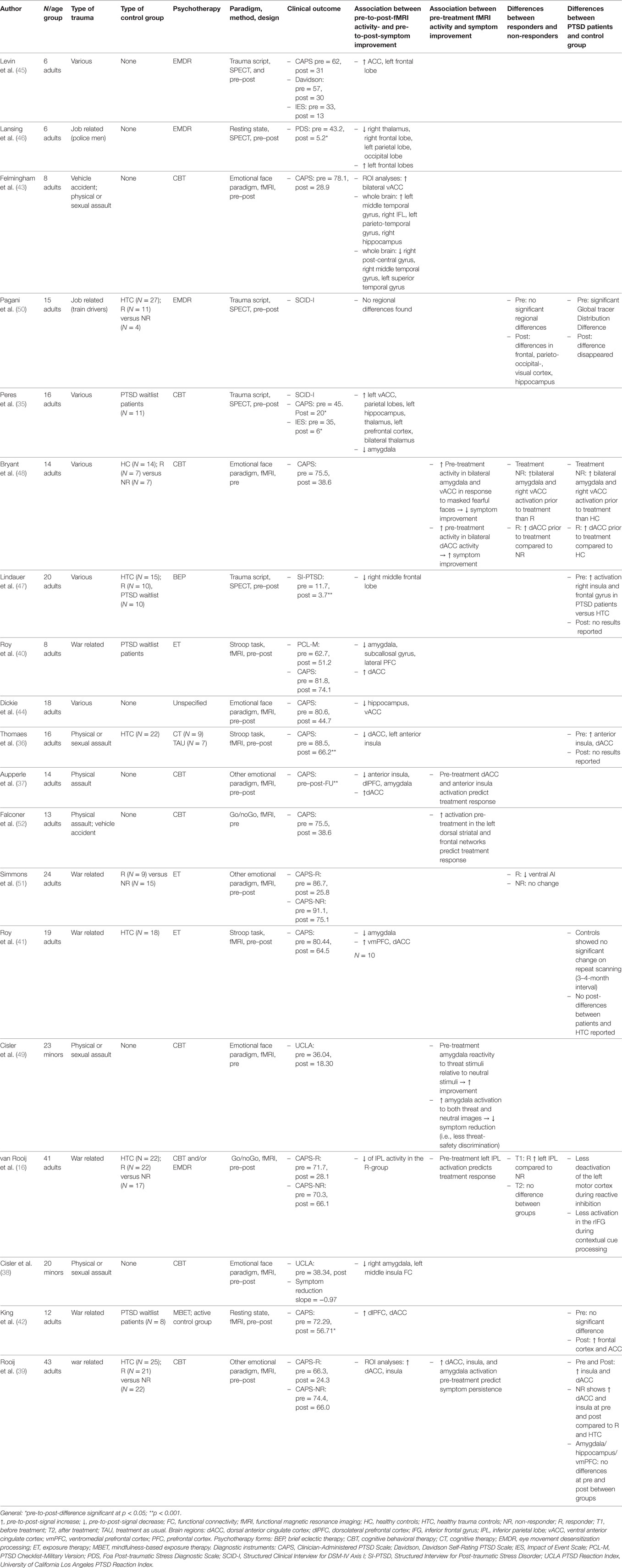
Table 1. Studies that investigated neural correlates of psychotherapeutic treatment of PTSD.
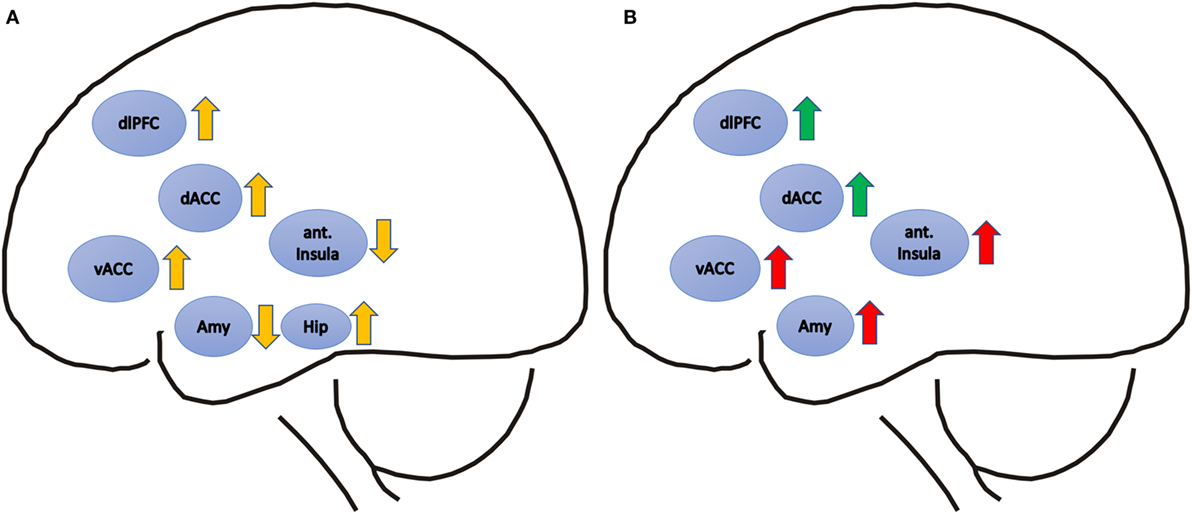
Figure 1. (A) Pre-to-post-treatment signal differences in post-traumatic stress disorder patients are depicted with yellow arrows. Upward arrows represent relatively increased, downward arrows relatively decreased activation after treatment. (B) Positive correlations of pre-treatment functional magnetic resonance imaging (fMRI) activity and symptom improvement are depicted with green arrows, and positive correlations of pre-treatment fMRI activity and symptom persistence are depicted with red arrows. Brain regions: dACC, dorsal anterior cingulate cortex; vACC, ventral anterior cingulate cortex; ant. Insula, anterior Insula; dlPFC, dorsolateral prefrontal cortex; Amy, amygdale; Hip, hippocampus.
Discussion
Results of the present systematic literature review regarding the neurobiology of PTSD treatment indicate that symptom improvement was shown to be accompanied with a pre-to-post-signal reduction in the amygdala. Accordingly, high amygdala activation prior to treatment was associated with subsequent treatment failure or non-response to treatment. Additionally, pre-to-post-signal decrease in the insula was associated with symptom improvement and increased insula activity prior to treatment was shown to be related to treatment resistance. Besides that symptom improvement goes hand in hand with fMRI signal increase in the hippocampus, dACC, PFC, and vACC, elevated dACC activity prior to treatment was shown to be related to subsequent treatment success and was a positive predictor for treatment response. Regarding cerebral networks involved, there were not obvious differences between CBT as the predominant treatment in nine of the studies listed, and ET or EMDR that were applied in three studies each. This may be interpreted in a way that changes in brain functioning rather represent changes in clinical symptoms and improvement than the different techniques that facilitate these changes. This interpretation is furthered by the finding that these therapy forms seemed to be equally effective. Therefore, changes in cerebral networks can hardly be related to distinct types of therapy but rather to elements like habituation, extinction learning, cognitive control, or attention direction.
The insular cortex is involved in emotions, salience, consciousness, motor control, and homeostasis (54, 55). Task-related fMRI studies showed increased activation in the insular cortex in individuals with PTSD, and this activation was positively correlated with the severity of PTSD symptoms (56–58). Neuroimaging studies investigating anxiety disorders also showed greater insular activation (59), pointing to a role in anxiety processing in general. With respect to the latter, the insula can be functionally divided into anterior and posterior parts: anterior insula activation, as shown to relate to salience and error processing (54), has been interpreted as a warning signal that is associated with symptoms of hyperarousal (51), whereas the posterior insular cortex is more strongly linked to the representation of interoceptive/bodily state changes, such as sympathetic arousal during negative affective states (53). Concerning the results of the present review, psychotherapeutic treatment success was associated with pre-to-post-decrease of insula activity especially in anterior parts. This can be interpreted as a correlate of reduced alertness and hyperarousal with traumatic and other emotional stimuli after treatment (55). Regarding therapeutic techniques, these changes could relate to interventions strengthening cognitive control and modulating attention as used in CBT.
Previous fMRI studies consistently showed increased amygdala activation in patients with PTSD compared to controls (60–63) and, with respect to the present review, a reduction of pre-to-post-treatment activity. As the amygdala has been suggested to play a crucial role in the processing of threatening stimuli, fear learning and fear expression (64, 65), the findings at hand might be a neurobiological correlate of a reduced response to threatening stimuli after treatment. Habituation to aversive stimuli as a result of confrontation treatment which is an element of CBT, EMDR, and ET could be a process underlying this observation. Furthermore, the present review highlights that an increased amygdala activity during fear processing prior to treatment was associated with subsequent treatment failure and non-response (48). The authors concluded that those patients, who reveal excessive fear-related amygdala activity, might have problems in regulating upcoming anxiety during confrontation with traumatic memories in therapy, which in turn might be a necessary requirement to experience subsequent habituation. In line with this, Cisler et al. (49) found that an increased amygdala reactivity to both neutral and threat stimuli before treatment was associated with poor treatment response in adolescents with PTSD. However, increased amygdala activity to threat relative to neutral stimuli was related to symptom improvement. The study of Cisler et al. (49) highlights the influence of paradigms and ways of analyses applied.
The amygdala and the hippocampus have both been suggested to play critical roles in the consolidation of emotionally laden memories in healthy adults. The interaction between these two hyper-responsive regions may contribute to the intrusive nature of trauma recollection in PTSD (20). Prolonged exposure to stress such as in patients with PTSD induces high glucocorticoid levels, which seem to harm the hippocampus (impairment of neurogenesis and loss of dendritic spines) (66). Structural imaging studies showed that PTSD patients have reduced hippocampal volume compared to HC (67–70). Whether the smaller hippocampal volumes in PTSD patients are associated with functional abnormalities still remains unclear. fMRI studies that compared PTSD patients with HC revealed both increased (71) and decreased hippocampal activation (72). The present review found pre-to-post-treatment increase of the hippocampus activity. It has been speculated that this might relate to improved short- and long-term consolidation and memory processes, improved encoding and recognition of episodic memory as well as an improved evaluation of experiences (35, 66). Furthermore, increased hippocampus activity might point toward improved identification of safe contexts, improved learning, and alteration of existing memories (20). Habituation and exposition as integral parts of the majority of treatments applied may be linked to these changes observed.
In the context of the processing of traumatic events, the ACC has been implicated in helping modulate fight/flight reactions to perceived threats (45). Altered activity in the ACC after successful psychotherapy of PTSD was, therefore, interpreted as a correlate of improved conflict monitoring and emotion regulation (37). The ACC can be subdivided functionally in ventral and dorsal parts: the vACC has been proposed to play a particular role in emotion processing, automatic emotion control, and social decision making (37, 73). The vACC was shown to be interconnected with the amygdala, nucleus accumbens, hypothalamus, and anterior insula and is assumed to be involved in assessing the salience of emotion and motivational information (74). The dACC has been proposed to be involved in cognitive processing or appraisal of emotion and the saliency of the source of social information (37, 73). The dACC is particularly connected with the prefrontal cortex and parietal cortex as well as the motor system and the frontal eye fields, making it a central node for processing top-down and bottom-up stimuli and assigning appropriate control over other areas in the brain (74). Following the results of the present review, pre-to-post-enhancement of dorsal and ventral ACC activity might be a correlate of improved cognitive processing of trauma-associated cognitions, better appraisal of trauma-associated emotions as well as in improved emotion control, all of these being processes that are directly addressed particularly in CBT. The present review found that treatment success was rather associated with an elevated pre-treatment activity in the dACC, which in turn might relate to better preconditions regarding cognitive control and emotion regulation.
Frontal brain areas have been strongly associated with PTSD in the literature before. The majority of studies revealed an increased pre-to-post-treatment activity in the PFC, which might be interpreted as a correlate of improved top-down regulation of emotional systems as well as a potential correlate of improved processing of risk and fear, decision making and emotion regulation (20, 75) as established during psychotherapy, particularly CBT. Changed prefrontal functioning might also relate to findings from structural neuroimaging studies that found reduced volumes in prefrontal brain regions (75–77) in PTSD patients. In a similar vein, results of a connectivity study of King et al. (42) showed increased connectivity to dlPFC regions within the central executive network after successful PTSD treatment, which was interpreted as a potential correlate of improved emotion regulation. The dlPFC was shown to play a critical role in working memory. Regarding PTSD, it was argued that extinction may not be based on an erasure of original information, but may rather reflect new learning (32). Increased activation in the dlPFC in the context of successful psychotherapy might represent a correlate of newly gained control of unwanted memories (47).
Post-traumatic stress disorder patients after successful treatment point toward a predominantly increased pre-to-post-treatment activity in “cognitive brain areas” like the PFC, dACC, and hippocampus when being compared to PTSD waitlist patients (35, 40, 42). Decreased pre-to-post-treatment activity in “emotional brain areas” like the insula and amygdala was more pronounced in within-group analyses (37, 53) and compared to patients of the waitlist control group (35, 40). Those findings underscore the importance of taking into consideration the control group applied when interpreting data of treatment studies.
Among others the impact of the review presented here might, therefore, be limited due to cross-study variations in control groups applied, different trauma histories, subject characteristics, and paradigms applied as this makes it very difficult to draw valid conclusions regarding subgroup and overall results.
Neurocircuitry models emphasize reduced activation of frontal brain areas and elevated activity of limbic regions in patients with PTSD and a loss of top-down inhibition is thought to be one of the main factors resulting in impaired extinction of traumatic memories or insufficient modulation of affect (e.g., re-experiencing) (20). The present review was able to show that brain activation results partly fit into this picture with relatively consistent signal increases in the dACC as a frontal brain area, while activity in key areas related to emotional processing like the anterior insula and amygdala rather decreased from pre-to-post-psychotherapy. This can be seen as an improved bottom-up and top-down regulation in response to successful treatment. Future studies should investigate whether abnormal activity patterns in patients with PTSD indeed normalize after treatment and become comparable to those of HC.
Author Contributions
JS and KM contributed substantially to the work, analyzed and interpreted the data, and drafted the manuscript. BA and PP contributed substantially to the work, interpreted the data, and revised the manuscript critically for important intellectual content. All the authors approved the final version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of Interest Statement
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organization for the submitted work and no other relationships or activities that could appear to have influenced the submitted work.
References
1. Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry (1995) 52(12):1048–60. doi:10.1001/archpsyc.1995.03950240066012
2. Perkonigg A, Kessler RC, Storz S, Wittchen HU. Traumatic events and post-traumatic stress disorder in the community: prevalence, risk factors and comorbidity. Acta Psychiatr Scand (2000) 101(1):46–59. doi:10.1034/j.1600-0447.2000.101001046.x
3. Breslau N, Chilcoat HD, Kessler RC, Davis GC. Previous exposure to trauma and PTSD effects of subsequent trauma: results from the Detroit area survey of trauma. Am J Psychiatry (1999) 156(6):902–7. doi:10.1176/ajp.156.6.902
4. Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI, Koffman RL. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med (2004) 351(1):13–22. doi:10.1056/NEJMoa040603
5. Stein DJ, Seedat S, Iversen A, Wessely S. Post-traumatic stress disorder: medicine and politics. Lancet (2007) 369(9556):139–44. doi:10.1016/S0140-6736(07)60075-0
6. O’Donnell ML, Bryant RA, Creamer M, Carty J. Mental health following traumatic injury: toward a health system model of early psychological intervention. Clin Psychol Rev (2008) 28(3):387–406. doi:10.1016/j.cpr.2007.07.008
7. Sareen J. Posttraumatic stress disorder in adults: impact, comorbidity, risk factors, and treatment. Can J Psychiatry (2014) 59(9):460–7. doi:10.1177/070674371405900902
8. Wilcox HC, Storr CL, Breslau N. Posttraumatic stress disorder and suicide attempts in a community sample of urban American young adults. Arch Gen Psychiatry (2009) 66(3):305–11. doi:10.1001/archgenpsychiatry.2008.557
9. Silverman AB, Reinherz HZ, Giaconia RM. The long-term sequelae of child and adolescent abuse: a longitudinal community study. Child Abuse Negl (1996) 20(8):709–23. doi:10.1016/0145-2134(96)00059-2
10. Hidalgo RB, Davidson JR. Posttraumatic stress disorder: epidemiology and health-related considerations. J Clin Psychiatry (2000) 61(Suppl 7):5–13.
11. Breslau N. Epidemiologic studies of trauma, posttraumatic stress disorder, and other psychiatric disorders. Can J Psychiatry (2002) 47(10):923–9. doi:10.1177/070674370204701003
12. Creamer M, Burgess P, McFarlane AC. Post-traumatic stress disorder: findings from the Australian National Survey of Mental Health and Well-Being. Psychol Med (2001) 31(7):1237–47. doi:10.1017/S0033291701004287
13. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry (2005) 62(6):617–27. doi:10.1001/archpsyc.62.6.617
14. Heim C, Nemeroff CB. Neurobiology of posttraumatic stress disorder. CNS Spectr (2009) 14(1 Suppl 1):13–24.
15. Sherin JE, Nemeroff CB. Post-traumatic stress disorder: the neurobiological impact of psychological trauma. Dialogues Clin Neurosci (2011) 13(3):263–78.
16. van Rooij SJ, Kennis M, Sjouwerman R, van den Heuvel MP, Kahn RS, Geuze E. Smaller hippocampal volume as a vulnerability factor for the persistence of post-traumatic stress disorder. Psychol Med (2015) 45(13):2737–46. doi:10.1017/S0033291715000707
17. Shin LM, Wright CI, Cannistraro PA, Wedig MM, McMullin K, Martis B, et al. A functional magnetic resonance imaging study of amygdala and medial prefrontal cortex responses to overtly presented fearful faces in posttraumatic stress disorder. Arch Gen Psychiatry (2005) 62(3):273–81. doi:10.1001/archpsyc.62.3.273
18. Disner SG, Beevers CG, Haigh EAP, Beck AT. Neural mechanisms of the cognitive model of depression. Nat Rev (2011) 12:467–77. doi:10.1038/nrn3027
19. VanElzakker MB, Dahlgren MK, Davis FC, Dubois S, Shin LM. From Pavlov to PTSD: the extinction of conditioned fear in rodents, humans, and anxiety disorders. Neurobiol Learn Mem (2014) 113:3–18. doi:10.1016/j.nlm.2013.11.014
20. Patel R, Spreng RN, Shin LM, Girard TA. Neurocircuitry models of posttraumatic stress disorder and beyond: a meta-analysis of functional neuroimaging studies. Neurosci Biobehav Rev (2012) 36:2130–42. doi:10.1016/j.neubiorev.2012.06.003
21. Flatten G, Gast U, Hofmann A, Knaevelsrud C, Lampe A, Liebermann P, et al. S3 – Leitlinie Posttraumatische Belastungsstörung. Trauma Gewalt (2011) 3:202–10.
22. Gillies D, Taylor F, Gray C, O’Brien L, D’Abrew N. Psychological therapies for the treatment of post-traumatic stress disorder in children and adolescents. Cochrane Database Syst Rev (2012) 12:CD006726. doi:10.1002/14651858.CD006726.pub2
23. Forbes EE, Olino TM, Ryan ND, Birmaher B, Axelson D, Moyles DL, et al. Reward-related brain function as a predictor of treatment response in adolescents with major depressive disorder. Cogn Affect Behav Neurosci (2010) 10:107–18. doi:10.3758/CABN.10.1.107
24. Foa E, Hembree EA, Rothbaum BO. Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences Therapist Guide. New York, NY: Oxford Press (2007).
25. Robertson M, Humphreys L, Ray R. Psychological treatments for posttraumatic stress disorder: recommendations for the clinician based on a review of the literature. J Psychiatr Pract (2004) 10(2):106–18. doi:10.1097/00131746-200403000-00005
26. Herkt D, Tumani V, Groen G, Kammer T, Hofmann A, Abler B. Facilitating access to emotions: neural signature of EMDR stimulation. PLoS One (2014) 9(8):e106350. doi:10.1371/journal.pone.0106350
27. Davidson PR, Parker KC. Eye movement desensitization and reprocessing (EMDR): a meta-analysis. J Consult Clin Psychol (2001) 69(2):305–16.
28. Shapiro F. EMDR-Basic Principles, Protocols and Procedures. Paderborn: Junfermann Verlag (2013) 69(2):305–16.
29. Bradley R, Greene J, Russ E, Dutra L, Westen D. A multidimensional meta-analysis of psychotherapy for PTSD. Am J Psychiatry (2005) 162:214–27. doi:10.1176/appi.ajp.162.2.214
30. Foa EB. Psychosocial therapy for posttraumatic stress disorder. J Clin Psychiatry (2006) 67(Suppl 2):40–5.
31. LeDoux JE. Emotion circuits in the brain. Annu Rev Neurosci (2000) 23:155–84. doi:10.1146/annurev.neuro.23.1.155
32. Bouton ME. Context, ambiguity, and unlearning: sources of relapses after behavioural extinction. Biol Psychiatry (2002) 52:976–86. doi:10.1016/S0006-3223(02)01546-9
33. Pezze MA, Feldon J. Mesolimbic dopaminergic pathways in fear conditioning. Prog Neurobiol (2004) 74(5):301–20. doi:10.1016/j.pneurobio.2004.09.004
34. Nawijn L, van Zuiden M, Frijling JL, Koch SB, Veltman DJ, Olff M. Reward functioning in PTSD: a systematic review exploring the mechanisms underlying anhedonia. Neurosci Biobehav Rev (2015) 51:189–204. doi:10.1016/j.neubiorev.2015.01.019
35. Peres JFP, Newberg AB, Mercante JP, Simao M, Albuquerque VE, Peres MJP, et al. Cerebral blood flow changes during retrieval of traumatic memories before and after psychotherapy: a SPECT study. Psychol Med (2007) 37:1481–91. doi:10.1017/S003329170700997X
36. Thomaes K, Dorrepaal E, Draijer ND, Ruiter MB, Elzinga BM, Balkom AJ, et al. Treatment effects on insular and anterior cingulate cortex activation during classic and emotional Stroop interference in child abuse-related complex post-traumatic stress disorder. Psychol Med (2012) 42:2337–49. doi:10.1017/S0033291712000499
37. Aupperle RL, Allard CB, Simmons AN, Flagan T, Thorp SR, Norman SB, et al. Neural responses during emotional processing before and after cognitive trauma therapy for battered women. Psychiatry Res (2013) 214:48–55. doi:10.1016/j.pscychresns.2013.05.001
38. Cisler JM, Sigel BA, Steele JS, Smitherman S, Vanderzee K, Pemberton J, et al. Changes in functional connectivity of the amygdala during cognitive reappraisal predict symptom reduction during trauma-focused cognitive-behavioral therapy among adolescent girls with post-traumatic stress disorder. Psychol Med (2016) 46(14):3013–23. doi:10.1017/S0033291716001847
39. Rooij S, Kennis M, Vink M, Geuze E. Predicting treatment outcome in PTSD: a longitudinal functional MRI study on trauma-unrelated emotional processing. Neuropsychopharmacology (2016) 41:1156–65. doi:10.1038/npp.2015.257
40. Roy MJ, Francis J, Friedlander J, Banks-Williams L, Lande RG, Taylor P, et al. Improvement in cerebral function with treatment of posttraumatic stress disorder. Ann N Y Acad Sci (2010) 1208:142–9. doi:10.1111/j.1749-6632.2010.05689.x
41. Roy MJ, Costanzo ME, Blair JR, Rizzo AA. Compelling evidence that exposure therapy for PTSD normalizes brain function. Stud Health Technol Inform (2014) 199:61–5.
42. King AP, Block SR, Sripada RK, Rauch S, Giardino N, Favorite T, et al. Altered default mode network (DMN) resting state functional connectivity following a mindfulness-based exposure therapy for posttraumatic stress disorder (PTSD) in combat veterans of Afghanistan and Iraq. Depress Anxiety (2016) 33:289–99. doi:10.1002/da.22481
43. Felmingham K, Kemp A, Williams L, Das P, Hughes G, Peduto A, et al. Changes in anterior cingulate and amygdala after cognitive behavior therapy of posttraumatic stress disorder. Psychol Sci (2007) 18(127):127–9. doi:10.1111/j.1467-9280.2007.01860.x
44. Dickie EW, Brunet A, Akerib V, Armony JL. Neural correlates of recovery from post-traumatic stress disorder: a longitudinal fMRI investigation of memory encoding. Neuropsychologia (2011) 49:1771–8. doi:10.1016/j.neuropsychologia.2011.02.055
45. Levin P, Lazrove S, van der Kolk B. What psychological and neuroimaging tell us about the treatment of posttraumatic stress disorder by eye movement desensitization and reprocessing. J Anxiety Disord (1999) 13(1–2):159–72. doi:10.1016/S0887-6185(98)00045-0
46. Lansing K, Amen DG, Hanks C, Rudy L. High-resolution brain SPECT imaging and eye movement desensitization and reprocessing in police officers with PTSD. J Neuropsychiatry Clin Neurosci (2005) 17(4):526–32. doi:10.1176/jnp.17.4.526
47. Lindauer RJL, Booij J, Habraken JBA, Meijel EPM, Uylings HBM, Olff M, et al. Effects of psychotherapy on regional cerebral blood flow during trauma imagery in patients with post-traumatic stress disorder: a randomized clinical trial. Psychol Med (2008) 38:543–54. doi:10.1017/S0033291707001432
48. Bryant RA, Felmingham K, Kemp A, Das P, Hughes G, Peduto A, et al. Amygdala and ventral anterior cingulate activation predicts treatment response to cognitive behavior therapy for post-traumatic stress disorder. Psychol Med (2008) 38:555–61. doi:10.1017/S0033291707002231
49. Cisler JM, Sigel BA, Kramer TL, Smitherman S, Vanderzee K, Pemberton J, et al. Amygdala response predicts trajectory of symptom reduction during trauma-focused cognitive-behavioral therapy among adolescent girls with PTSD. J Psychiatr Res (2015) 71:33–40. doi:10.1016/j.jpsychires.2015.09.011
50. Pagani M, Hoegberg G, Salmaso D, Nardo D, Sundin O, Jonsson C, et al. Effects of EMDR psychotherapy on 99mTc-HMPAO distribution in occupation-related post-traumatic stress disorder. Nucl Med Commun (2007) 28:257–765. doi:10.1097/MNM.0b013e3282742035
51. Simmons AN, Norman SB, Spadoni AD, Strigo IA. Neurosubstrates of remission following prolonged exposure therapy in veterans with posttraumatic stress disorder. Psychother Psychosom (2013) 82:382–9. doi:10.1159/000348867
52. Falconer E, Allen A, Felmingham KL, Williams LM, Bryant RA. Inhibitory neural activity predicts response to cognitive-behavioral therapy for post-traumatic stress disorder. J Clin Psychiatry (2013) 74(9):895–901.
53. Cisler JM, Sigel BA, Kramer TL, Smitherman S, Vanderzee K, Pemberton J, et al. Modes of large-scale brain network organization during threat processing and posttraumatic stress disorder symptom reduction during TF-CBT among adolescent girls. PLoS One (2016) 11(8):1–16. doi:10.1371/journal.pone.0159620
54. Menon V, Uddin LQ. Saliency, switching, attention and control: a network model of insula function. Brain Struct Funct (2010) 214(5–6):655–67. doi:10.1007/s00429-010-0262-0
55. Gu X, Hof PR, Friston KJ, Fan J. Anterior insular cortex and emotional awareness. J Comp Neurol (2013) 521(15):3371–88. doi:10.1002/cne.23368
56. Simmons AN, Paulus MP, Thorp SR, Matthews SC, Norman SB, Stein MB. Functional activation and neural networks in women with posttraumatic stress disorder related to intimate partner violence. Biol Psychiatry (2008) 64(8):681–90. doi:10.1016/j.biopsych.2008.05.027
57. Strigo IA, Simmons AN, Matthews SC, Grimes EM, Allard CB, Reinhardt LE, et al. Neural correlates of altered pain response in women with posttraumatic stress disorder from intimate partner violence. Biol Psychiatry (2010) 68(5):442–50. doi:10.1016/j.biopsych.2010.03.034
58. Aupperle RL, Allard CB, Grimes EM, Simmons AN, Flagan T, Behrooznia M, et al. Dorsolateral prefrontal cortex activation during emotional anticipation and neuropsychological performance in posttraumatic stress disorder. Arch Gen Psychiatry (2012) 69(4):360–71. doi:10.1001/archgenpsychiatry.2011.1539
59. Etkin A, Wager TD. Functional neuroimaging of anxiety: a meta-analysis of emotional processing in PTSD, social anxiety disorder, and specific phobia. Am J Psychiatry (2007) 164(10):1476–88. doi:10.1176/appi.ajp.2007.07030504
60. Koenigs M, Grafman J. Posttraumatic stress disorder: the role of medial prefrontal cortex and amygdala. Neuroscientist (2009) 15(5):540–8. doi:10.1177/1073858409333072
61. Milad MR, Pitman RK, Ellis CB, Gold AL, Shin LM, Lasko NB, et al. Neurobiological basis of failure to recall extinction memory in posttraumatic stress disorder. Biol Psychiatry (2009) 66(12):1075–82. doi:10.1016/j.biopsych.2009.06.026
62. Pitman RK, Rasmusson AM, Koenen KC, Shin LM, Orr SP, Gilbertson MW, et al. Biological studies of post-traumatic stress disorder. Nat Rev Neurosci (2012) 13(11):769–87. doi:10.1038/nrn3339
63. McLaughlin KA, Busso DS, Duys A, Green JG, Alves S, Way M, et al. Amygdala response to negative stimuli predicts PTSD symptom onset following a terrorist attack. Depress Anxiety (2014) 31(10):834–42. doi:10.1002/da.22284
64. LaBar KS, Gatenby JC, Gore JC, LeDoux JE, Phelps EA. Human amygdala activation during conditioned fear acquisition and extinction: a mixed-trial fMRI study. Neuron (1998) 20(5):937–45. doi:10.1016/S0896-6273(00)80475-4
65. Barad M, Gean PW, Lutz B. The role of the amygdala in the extinction of conditioned fear. Biol Psychiatry (2006) 60(4):322–8. doi:10.1016/j.biopsych.2006.05.029
66. Fuchs E, Gould E. Mini-review: in vivo neurogenesis in the adult brain: regulation and functional implications. Eur J Neurosci (2000) 12(7):2211–4. doi:10.1046/j.1460-9568.2000.00130.x
67. Bremner JD, Randall P, Scott TM, Bronen RA, Seibyl JP, Southwick SM, et al. MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry (1995) 152(7):973–81. doi:10.1176/ajp.152.7.973
68. Gurvits TV, Shenton ME, Hokama H, Ohta H, Lasko NB, Gilbertson MW, et al. Magnetic resonance imaging study of hippocampal volume in chronic, combat-related posttraumatic stress disorder. Biol Psychiatry (1996) 40(11):1091–9. doi:10.1016/S0006-3223(96)00229-6
69. Bremner JD, Randall P, Vermetten E, Staib L, Bronen RA, Mazure C, et al. Magnetic resonance imaging-based measurement of hippocampal volume in posttraumatic stress disorder related to childhood physical and sexual abuse – a preliminary report. Biol Psychiatry (1997) 41(1):23–32. doi:10.1016/S0006-3223(96)00162-X
70. Stein MB, Koverola C, Hanna C, Torchia MG, McClarty B. Hippocampal volume in women victimized by childhood sexual abuse. Psychol Med (1997) 27(4):951–9. doi:10.1017/S0033291797005242
71. Shin LM, Liberzon I. The neurocircuitry of fear, stress, and anxiety disorders. Neuropsychopharmacology (2010) 35(1):169–91. doi:10.1038/npp.2009.83
72. Bremner JD, Vythilingam M, Vermetten E, Southwick SM, McGlashan T, Nazeer A, et al. MRI and PET study of deficits in hippocampal structure and function in women with childhood sexual abuse and posttraumatic stress disorder. Am J Psychiatry (2003) 160(5):924–32. doi:10.1176/appi.ajp.160.5.924
73. Behrens TE, Hunt LT, Woolrich MW, Rushworth MF. Associative learning of social value. Nature (2008) 456(7219):245–9. doi:10.1038/nature07538
74. Beckmann M, Johansen-Berg H, Rushworth MF. Connectivity-based parcellation of human cingulate cortex and its relation to functional specialization. J Neurosci (2009) 29(4):1175–90. doi:10.1523/JNEUROSCI.3328-08.2009
75. Shin LM, Rauch SL, Pitman RK. Amygdala, medial prefrontal cortex, and hippocampal function in PTSD. Ann N Y Acad Sci (2006) 1071:67–79. doi:10.1196/annals.1364.007
76. Rauch SL, Shin LM, Segal E, Pitman RK, Carson MA, McMullin K, et al. Selectively reduced regional cortical volumes in post-traumatic stress disorder. Neuroreport (2003) 14(7):913–6. doi:10.1097/01.wnr.0000071767.24455.10
Keywords: post-traumatic stress disorder, functional magnetic resonance imaging, review, psychotherapeutic treatment, therapy
Citation: Malejko K, Abler B, Plener PL and Straub J (2017) Neural Correlates of Psychotherapeutic Treatment of Post-traumatic Stress Disorder: A Systematic Literature Review. Front. Psychiatry 8:85. doi: 10.3389/fpsyt.2017.00085
Received: 09 February 2017; Accepted: 28 April 2017;
Published: 19 May 2017
Edited by:
José Alexandre Crippa, University of São Paulo, BrazilReviewed by:
Wi Hoon Jung, Korea University, South KoreaWissam El-Hage, François Rabelais University, France
Copyright: © 2017 Malejko, Abler, Plener and Straub. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kathrin Malejko, kathrin.malejko@uni-ulm.de