 Susanne Thümmler1,2*
Susanne Thümmler1,2* Emmanuelle Dor1,2
Emmanuelle Dor1,2 Renaud David2
Renaud David2 Graziella Leali3Michele Battista1,4
Graziella Leali3Michele Battista1,4 Alexia David1Florence Askenazy1,2
Alexia David1Florence Askenazy1,2 Céline Verstuyft5,6
Céline Verstuyft5,6
- 1University Department of Child and Adolescent Psychiatry, Children’s Hospitals of Nice CHU-Lenval, Nice, France
- 2CoBTek, Université Côte d’Azur, Nice, France
- 3Department of Child Psychiatry, Nice Children’s Hospitals CHU-Lenval, Nice, France
- 4Department of Child and Adolescent Psychiatry, Hospital of Fréjus, Fréjus, France
- 5Service de génétique moléculaire, pharmacogénétique et hormonologie, Centre de Ressource Biologie Paris-Sud, Hôpital Bicêtre, Groupe Hospitalier Paris Sud, AP-HP, Le Kremlin Bicêtre, Nice, France
- 6Université Paris-Sud, UMR 1184, Faculté de médecine, Paris, France
Background: Severe mental health disorders in children and adolescents represent a major public health problem. Despite adequate drug treatment, some patients develop pharmacoresistant disease. As a consequence, physicians are confronted with prescribing challenges, prolonged hospitalization and increased risk of adverse events, thus aggravating short-, medium-, and long-term prognosis. The majority of psychotropic treatments, particularly antipsychotics and antidepressants, are metabolized at hepatic level by cytochrome P450 (CYP), particularly by CYP3A4 and CYP2D6. Several CYP2D6 genetic polymorphisms are described to be associated with ultrarapid (UM) or poor drug metabolism (PM), inducing clinical resistance and/or adverse events, and might therefore be related to pharmacoresistant severe mental health disease.
Case presentation: A total of nine pharmacoresistant patients (four females, five males) aged 11–16 (mean 14.1) years have been genotyped for CYP2D6 between January, 2015 and April, 2016. Patients were diagnosed with schizophrenia (n = 5), autism spectrum disorders (n = 2), intellectual disability with challenging behavior (n = 2), oppositional defiant disorder (n = 1), and post-traumatic stress and borderline personality disorders (n = 1). They had a treatment history with on average 6.1 (3–9) psychotropic, 5 (3–7) antipsychotic, and 3.4 (2–5) CYP2D6-metabolized antipsychotic and antidepressant molecules. Five patients (56%) presented functional anomalies of the CYP2D6 gene: three patients were UM metabolizers with gene duplication and two patients were PM with *4/*41 and *3/*4 polymorphisms.
Conclusion: Functional anomalies of CYP2D6 concerned more than half of our pediatric inpatient sample with pharmacoresistant disease. However, our case reports are limited by the low sample size. Nevertheless, knowledge of individual metabolism and in particular CYP2D6 genotyping should be considered for clinical workup and therapy adjustment in resistant patients in child and adolescent psychiatry and might permit better treatment outcome, increased treatment adherence and diminished adverse events.
Background
Pharmacoresistant severe mental illness is an important public health burden, especially in children and adolescents with chronic disabling disease. Treatment decisions in those children and adolescents are generally challenging and many of these patients are hospitalized in inpatient children and adolescent psychiatry (CAP) departments at one point of their illness. Clinicians are therefore in the need of complementary explorations aiming to optimize treatment in order to increase the probability of clinical efficacy and to minimize eventual adverse events, improving treatment adherence and long-term outcome.
Cytochromes P450 (CYP450) are proteins implicated in metabolism and expressed in different organs such as liver, gut and brain (1, 2). There are about 18 families of CYP450 with CYP1, CYP2, and CYP3 most involved in drug metabolism, as well as different subfamilies (e.g., CYP1A, CYP3A, and CYP2D) and isoenzymes (e.g., CYP1A2, CYP3A4, and CYP2D6).
The CYP2D6 enzyme is of special interest for child and adolescent psychiatrists. At hepatic level, CYP450 enzymes are responsible for about 80% of all phase I metabolism reactions. Even though CYP2D6 constitutes only 2% of all CYP450 enzymes expressed at the hepatic level, it is involved in the metabolism of about 20% of drugs (1), and especially of psychotropic drugs frequently used in CAP (see also Table 1).
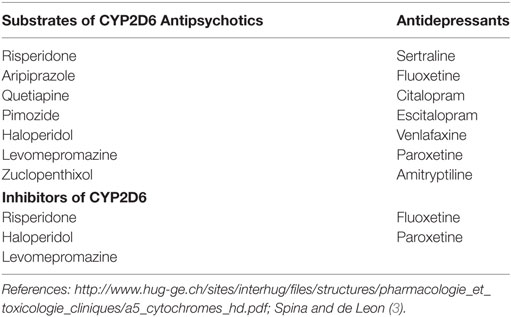
Table 1. Examples of CYP2D6 metabolism or interaction of antipsychotic and antidepressant medications used in Child and Adolescent Psychiatry.
The CYP2D6 and CYP2C19 are highly polymorphic with over 100 allelic variants identified for CYP2D61 and over 30 allelic variants for CYP2C192 (4, 5).
Phenotypes of the CYP2D6 activity, resulting from the analyses of these polymorphisms, are classified into extensive (EM), poor (PM), and ultrarapid (UM) metabolizers accordingly to the enzymatic activities (6). The most common EM have normal CYP2D6 function. Decreased or no CYP2D6 function is observed in PM, and increased CYP2D6 function is related to UM. Individual CYP2D6 genotype and function also depend on ethnic origin. Polymorphisms leading to poor metabolization (PM) are present in about 3–10% of Caucasians (7–9). Gene duplication resulting in UM concerns about 1% of the general population in Northern European Caucasians and up to 10% in Southern Europeans (7) and might be as high 29% in African Ethiopians (10).
In addition, several studies underline that certain CYP2D6 genotypes are associated with psychotropic treatment response as well as to the occurrence of adverse events in children and adolescents (11–14).
Despite the increasing use of pharmacogenetic (PGx) testing for treatment decisions in different fields of medicine, especially in oncology (15), CYP genotyping is only rarely used in French CAP practice.
In this case report, we present PGx results for CYP2D6 genotyping in an inpatient sample of pediatric individuals hospitalized in CAP and presenting severe mental illness with repeated psychotropic treatment failure. We hypothesized that functional anomalies of the CYP2D6 gene, especially those leading to ultrarapid metabolism, might be present in some of these patients.
Methods
A retrospective chart review was conducted in order to evaluate CYP2D6 genotyping data from children and adolescents of the inpatient units of the University Child and Adolescent Psychiatry department, Nice, France, between January 2015 and April 2016. CYP2D6 PGx has been introduced since January 2015 as a complementary analysis of inpatients presenting with pharmacoresistant mental health disease. The factors determining pharmacoresistance were multiple failed responses to psychotropic medications and polypharmacy. All patients/guardians gave written informed consent for CYP450 PGx testing and for the use of this data for research purposes and publication. The data collection has been declared to the French national commission on informatics and liberty (CNIL No. 1970115v0).
Patients were systematically genotyped for the major CYP2D6 genetic polymorphisms and classified into three CYP2D6 phenotype subgroups (PM, EM, and UM). Genomic DNA was extracted from circulating blood leukocytes by using Qiagen Blood Kits according to the manufacturer’s protocol (Qiagen, S.A., Courtaboeuf, France).
Patients were genotyped for the major alleles CYP2D6: loss of function alleles (CYP2D6 *3 rs35742686, *4 rs3892097, *6 rs5030655, *41 rs28371725); using TaqMan allelic discrimination (16) with the ABI Prism® 7900HT Sequence Detection System (Applied Biosystem, Courtaboeuf, France). The complete deletion (CYP2D6*5) and gene duplication (CYP2D6 *2xN) were detected by quantitative PCR according to the methods of Ref. (17). We employed descriptive statistics using mean and SD.
Case Presentation
A total of nine individuals, four females and five males, aged 11–16 years (14.1 ± 1.8) have been genotyped for CYP2D6. Patient characteristics are detailed in Table 2. Patients had a treatment history with the failure of 3– 9 psychotropic medications (6.1 ± 2.3) including 3–7 antipsychotics (5 ± 1.5), 2– 5 CYP2D6-metabolized molecules (3.4 ± 0.9), and 1–3 CYP2D6-inhibitor drugs (2.2 ± 0.83). Most patients were diagnosed with childhood-onset schizophrenia (COS, n = 5) with one also having been diagnosed with autism spectrum disorder (ASDs). Two patients presented with intellectual disability (ID) associated with severe behavioral disorder (BD) such as aggressive behavior. The other two patients have been diagnosed with ASD and oppositional defiant disorder (ODD), and posttraumatic stress disorder (PTSD) and borderline personality disorder (BPD).
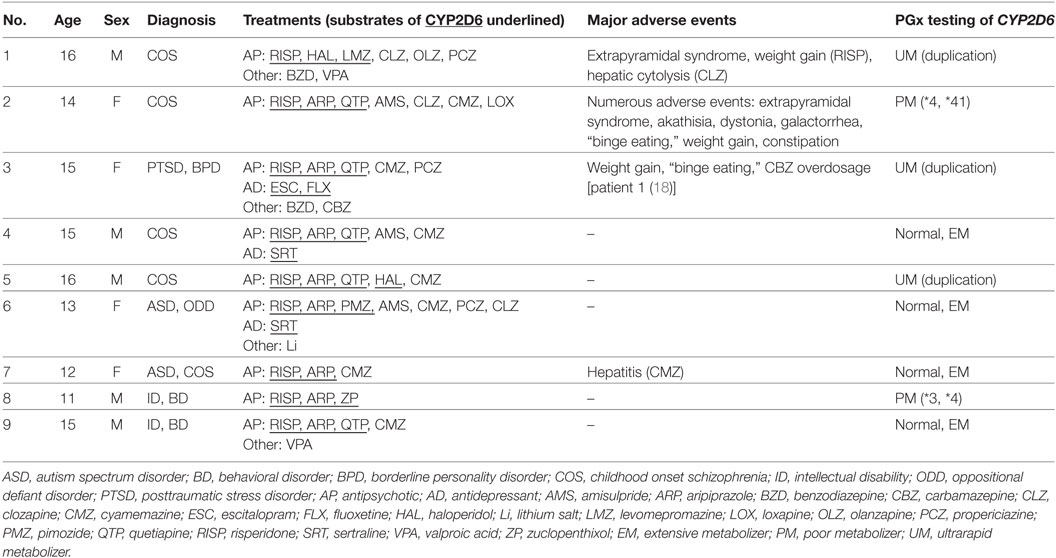
Table 2. Patient characteristics and results of CYP2D6 genotyping.
Five of the nine (55.6%) inpatients with pharmacoresistant mental health disease presented functional CYP2D6 abnormalities. Gene duplication associated with UM has been found in three patients. Two patients were shown to present PM as the consequence of *4/*41 and *3/*4 polymorphisms.
Major adverse events were described in 4/9 patients representing 1/2 of PM and 2/3 of UM (see Table 2).
Discussion
More than half of our inpatient sample with pharmacoresistant mental health disease presented functional defects in CYP2D6 drug metabolism. This result is somewhat surprising with regard to two aspects. First, we did not expect such a high percentage in our patients. Even if those patients presented with severe mental illness with repeated treatment failure, we attributed treatment refractoriness to diagnosis such as COS, known to be associated with failure of AP treatment (19). In addition, CYP2D6 anomalies don’t explain resistance to both 2D6 and non-2D6 metabolized drugs.
Second, treatment resistance is generally associated with UM and adverse advents with PM (4, 8). Nevertheless, in our sample both, PM and UM, functional abnormalities are present and no clear relation can be established with the occurrence or absence of major adverse events. Also, whereas one cannot draw conclusions because of the small sample size, the complexity of individual drug metabolism beyond CYP2D6 metabolism needs to be considered for the interpretation of the results. In fact, the accumulation of metabolites, dependent on individual PGx, might explain some side effects. This might be comparable to morphine accumulation leading to intoxication upon codeine treatment in individuals presenting CYP2D6 UM (20, 21). Nevertheless, pharmacokinetics and pharmacodynamics of psychotropic drugs are not yet fully understood, and include additional CYP450 enzymes (e.g., CYP1A2, 3A4/5, 2C9, 2C19) as well as transporter and receptor genes (22). Moreover, CYP expression patterns alter with age and might thus modify the relative contribution of the different enzymes for drug metabolism in children compared to adult patients (23).
In addition to direct metabolism by CYP2D6, some AP (e.g., risperidone) and AD drugs (e.g., fluoxetine) are inhibitors of CYP2D6 or other CYP, and therefore important for treatment interaction which might also be related to pharmacoresistance or side effects (see Table 1).
Moreover, CYP2D6 function outside the hepatic pathway still needs to be elucidated. CYP2D6 has been described to be expressed in the brain, playing a role in acute and chronic drug response as well as in neurotransmitter formation (24). In addition, CYP might be associated with mental health disorders (25, 26). The impact of abnormal function of CYP in pediatric patients with ongoing neurodevelopment might therefore be beyond the only hepatic level.
The knowledge of the individual metabolism of psychotropic drugs is very important for treatment decisions, especially for pharmacoresistant patients. Therapy in line with PGx in those patients should improve treatment outcome and decrease the burden of chronic mental health disease and eventual adverse events in line with predictable inefficient treatment and often polypharmacy. In fact, it has been shown that carriers of abnormal CYP2D6 phenotypes (PM as well as UM) experience an increased duration of hospitalization in psychiatry compared to patients with normal metabolism (27). Nevertheless, so far there are no studies in CAP providing evidence of better treatment outcome when using PGx, and our case descriptions should therefore be interpreted with caution.
In clinical practice, pharmacoresistant UM patients might benefit from increased dosage of CYP2D6-metabolized psychotropics (3). Nevertheless, in the case of adverse events or pharmacoresistance related to PM, treatment options should consider psychotropics not metabolized by CYP2D6 [e.g., olanzapine, clozapine metabolized by CYP1A2; lithium, amisulpride without hepatic metabolism (3), see also http://www.hug-ge.ch/sites/interhug/files/structures/pharmacologie_et_toxicologie_cliniques/a5_cytochromes_hd.pdf]. In general, the clinical benefit of CYP2D6 metabolized molecules should be carefully re-evaluated in patients with abnormal metabolism. Some alternative treatments might not have market authorization in pediatric patients, and should therefore be discussed by a specialized multidisciplinary team. Treatment adjustment should also consider the intensification of non-pharmacological treatments such as psychotherapy.
Conclusion
Functional anomalies of CYP genotypes might concern a significant number of treatment resistant children and adolescents with severe mental health disorder. Nevertheless, additional studies are needed in order to better understand nonresponding in this population. Considering PGx testing might therefore be important for the clinical workup and treatment decisions in those patients. In fact, the knowledge of individual metabolism should permit better treatment outcome, increased adherence and diminished adverse events (22, 28).
Perspectives
Our preliminary data underline the need of larger controlled studies of PGx factors in pharmacoresistant children and adolescents in CAP. They should include a broader set of pharmacokinetic and pharmacodynamics parameters, as well as detailed assessment of diagnosis, clinical and treatment history. Moreover, studies are needed to provide evidence of better treatment outcome when using PGx.
A prospective study including children and adolescent with pharmacoresistance to two or more AP and/or AD metabolized by CYP2D6 has been implemented in our department following the preliminary results described in this study. Pharmacoresistance has been defined based on guidelines of the European Medicines Agency (EMA) as lack of satisfactory improvement despite the use of adequate doses of at least two different AP/AD agents, prescribed for adequate duration with adequate confirmation of treatment adherence (EMA/CHMP/40072/2010; EMA/CHMP/185423/2010). PGx explorations will include pharmacokinetic and pharmacodynamic factors, such as CYP2D6 but also additional CYP450 enzymes as well as transporter and receptor genes. In addition to the results of classic CYP2D6 genotyping used in our patients, next-generation sequencing will allow rapid DNA sequencing of various genes and thus permit to find additional rare polymorphisms not being discovered with the standard technique.
Ethics Statement
All patients/guardians gave written informed consent for CYP450 PGx testing and for the use of these data for research purposes and publication. The data collection has been declared to the French national commission on informatics and liberty (CNIL No. 1970115v0).
Author Contributions
ST, ED, GL, MB, AD, and FA were involved in clinical follow-up. CV has been responsible for pharmacogenetic studies. ST, RD, FA, and CV were responsible for data analysis. ST and CV have been involved in drafting the first version of the MS. All authors have been involved in revising it critically for important intellectual content and approved the final version.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Preliminary data have been presented at the SFPT congress (29).
Footnotes
References
1. Kapur BM, Lala PK, Shaw JL. Pharmacogenetics of chronic pain management. Clin Biochem (2014) 47:1169–87. doi:10.1016/j.clinbiochem.2014.05.065
2. Chinta SR, Pai HV, Upadhya SC, Boyd MD, Ravindranath V. Constitutive expression and localization of the major drug metabolizing enzyme, cytochrome P4502D in human brain. Brain Res Mol Brain Res (2002) 103:49–61. doi:10.1016/S0169-328X(02)00177-8
3. Spina E, de Leon J. Clinical applications of CYP genotyping in psychiatry. J Neural Transm (Vienna) (2015) 122:5–28. doi:10.1007/s00702-014-1300-5
4. Hicks JK, Bishop JR, Sangkuhl K, Müller DJ, Ji Y, Leckband SG, et al. Clinical Pharmacogenetics Implementation Consortium: Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 genotypes and dosing of selective serotonin reuptake inhibitors. Clin Pharmacol Ther (2015) 98:127–34. doi:10.1002/cpt.147
5. Marez D, Legrand M, Sabbagh N, Lo Guidice JM, Spire C, Lafitte JJ, et al. Polymorphism of the cytochrome P450 CYP2D6 gene in a European population: characterization of 48 mutations and 53 alleles, their frequencies and evolution. Pharmacogenetics (1997) 7:193–202. doi:10.1097/00008571-199706000-00004
6. Bertilsson L, Dahl ML, Dalén P, Al-Shurbaji A. Molecular genetics of CYP2D6: clinical relevance with focus on psychotropic drugs. Br J Clin Pharmacol (2002) 53:111–22. doi:10.1046/j.0306-5251.2001.01548.x
7. Scordo MG, Caputi AP, D’Arrigo C, Fava G, Spina E. Allele and genotype frequencies of CYP2C9, CYP2C19 and CYP2D6 in an Italian population. Pharmacol Res (2004) 50:195–200. doi:10.1016/j.phrs.2004.01.004
8. Bernard S, Neville K, Nguyen A, Flockhart D. Interethnic differences in genetic polymorphisms of CYP2D6 in the U.S. population: clinical implications. Oncologist (2006) 11:126–35. doi:10.1634/theoncologist.11-2-126
9. McGrane IR, Loveland JG. Pharmacogenetics of cytochrome p450 enzymes in American Indian and Caucasian Children Admitted to a Psychiatric Hospital. J Child Adolesc Psychopharmacol (2016) 26:395–9. doi:10.1089/cap.2015.0180
10. Aklillu E, Persson I, Bertilsson L, Johansson I, Rodrigues F, Ingelman-Sundberg M. Frequent distribution of ultrarapid metabolizers of debrisoquine in an Ethiopian population carrying duplicated and multiduplicated functional CYP2D6 alleles. J Pharmacol Exp Ther (1996) 278:441–6.
11. Prows CA, Nick TG, Saldaña SN, Pathak S, Liu C, Zhang K, et al. Drug-metabolizing enzyme genotypes and aggressive behavior treatment response in hospitalized pediatric psychiatric patients. J Child Adolesc Psychopharmacol (2009) 19:385–94. doi:10.1089/cap.2008.0103
12. Butwicka A, Krystyna S, Retka W, Wolańczyk T. Neuroleptic malignant syndrome in an adolescent with CYP2D6 deficiency. Eur J Pediatr (2014) 173:1639–42. doi:10.1007/s00431-013-2208-z
13. Gassó P, Rodríguez N, Mas S, Pagerols M, Blázquez A, Plana MT, et al. Effect of CYP2D6, CYP2C9 and ABCB1 genotypes on fluoxetine plasma concentrations and clinical improvement in children and adolescent patients. Pharmacogenomics J (2014) 14:457–62. doi:10.1038/tpj.2014.12
14. Youngster I, Zachor DA, Gabis LV, Bar-Chaim A, Benveniste-Levkovitz P, Britzi M, et al. CYP2D6 genotyping in paediatric patients with autism treated with risperidone: a preliminary cohort study. Dev Med Child Neurol (2014) 10:990–4. doi:10.1111/dmcn.12470
15. Filipski KK, Mechanic LE, Long R, Freedman AN. Pharmacogenomics in oncology care. Front Genet (2014) 5:73. doi:10.3389/fgene.2014.00073
16. Schaeffeler E, Schwab M, Eichelbaum M, Zanger UM. CYP2D6 genotyping strategy based on gene copy number determination by TaqMan real-time PCR. Hum Mutat (2003) 22:476–85. doi:10.1002/humu.10280
17. Steen VM, Andreassen OA, Daly AK, Tefre T, Borresen AL, Idle JR, et al. Detection of the poor metabolizer-associated CYP2D6(D) gene deletion allele by long-PCR technology. Pharmacogenetics (1995) 5:215–23. doi:10.1097/00008571-199508000-00005
18. Fernandez A, Dor E, Menard ML, Askenazy F, Thümmler S. Carbamazepine and psychotropic treatment interaction: two case studies of carbamazepine overdosage. Arch Pediatr (2015) 22:536–9. doi:10.1016/j.arcped.2015.02.010
19. Kasoff LI, Ahn K, Gochman P, Broadnax DD, Rapoport JL. Strong treatment response and high maintenance rates of clozapine in childhood-onset schizophrenia. J Child Adolesc Psychopharmacol (2016) 26:428–35. doi:10.1089/cap.2015.0103
20. Koren G, Cairns J, Chitayat D, Gaedigk A, Leeder SJ. Pharmacogenetics of morphine poisoning in a breastfed neonate of a codeine-prescribed mother. Lancet (2006) 368:704. doi:10.1016/S0140-6736(06)69255-6
21. Coulbault L, Beaussier M, Verstuyft C, Weickmans H, Dubert L, Trégouet D, et al. Environmental and genetic factors associated with morphine response in the postoperative period. Clin Pharmacol Ther (2006) 79:316–24. doi:10.1016/j.clpt.2006.01.007
22. Brandl EJ, Kennedy JL, Müller DJ. Pharmacogenetics of antipsychotics. Can J Psychiatry (2014) 59:76–88. doi:10.1177/070674371405900203
23. Zanger UM, Schwab M. Cytochrome P450 enzymes in drug metabolism: regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol Ther (2013) 138:103–41. doi:10.1016/j.pharmthera.2012.12.007
24. McMillan DM, Tyndale RF. CYP-mediated drug metabolism in the brain impacts drug response. Pharmacol Ther (2017). doi:10.1016/j.pharmthera.2017.10.008
25. Ingelman-Sundberg M, Persson A, Jukic MM. Polymorphic expression of CYP2C19 and CYP2D6 in the developing and adult human brain causing variability in cognition, risk for depression and suicide: the search for the endogenous substrates. Pharmacogenomics (2014) 15:1841–4. doi:10.2217/pgs.14.151
26. Zackrisson AL, Lindblom B, Ahlner J. High frequency of occurrence of CYP2D6 gene duplication/multiduplication indicating ultrarapid metabolism among suicide cases. Clin Pharmacol Ther (2010) 88:354–9. doi:10.1038/clpt.2009.216
27. Chou WH, Yan FX, de Leon J, Barnhill J, Rogers T, Cronin M, et al. Extension of a pilot study: impact from the cytochrome P450 2D6 polymorphism on outcome and costs associated with severe mental illness. J Clin Psychopharmacol (2000) 20:246–51. doi:10.1097/00004714-200004000-00019
28. Ozomaro U, Wahlestedt C, Nemeroff CB. Personalized medicine in psychiatry: problems and promises. BMC Med (2013) 11:132. doi:10.1186/1741-7015-11-132
29. Thümmler S, Dor E, David R, Leali G, Battista M, Askenazy F, et al. Pharmacoresistant severe mental health disorders in children and adolescents: high prevalence of functional abnormalities of cytochrome P450 2D6. Preliminary data and ongoing study protocol. Fundam Clin Pharmacol (2017) 31:45–6.
Keywords: pharmacogenetics, personalized medicine, antipsychotics, antidepressants, child and adolescent psychiatry, CYP2D6
Citation: Thümmler S, Dor E, David R, Leali G, Battista M, David A, Askenazy F and Verstuyft C (2018) Pharmacoresistant Severe Mental Health Disorders in Children and Adolescents: Functional Abnormalities of Cytochrome P450 2D6. Front. Psychiatry 9:2. doi: 10.3389/fpsyt.2018.00002
Received: 19 September 2017; Accepted: 08 January 2018;
Published: 24 January 2018
Edited by:
Maria Rosaria Anna Muscatello, University of Messina, ItalyReviewed by:
Florence P. Varodayan, The Scripps Research Institute, United StatesDean Elbe, BC Mental Health and Addiction Services, Canada
Copyright: © 2018 Thümmler, Dor, David, Leali, Battista, David, Askenazy and Verstuyft. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susanne Thümmler, thummler.s@pediatrie-chulenval-nice.fr