 Nilufar Mossaheb1*
Nilufar Mossaheb1* Rainer M. Kaufmann2Monika Schlögelhofer3Thushara Aninilkumparambil4Claudia Himmelbauer5Anna Gold6Sonja Zehetmayer7Holger Hoffmann8
Rainer M. Kaufmann2Monika Schlögelhofer3Thushara Aninilkumparambil4Claudia Himmelbauer5Anna Gold6Sonja Zehetmayer7Holger Hoffmann8 Harald C. Traue8
Harald C. Traue8 Harald Aschauer9
Harald Aschauer9
- 1Clinical Division of Social Psychiatry, Department of Psychiatry and Psychotherapy, Medical University Vienna, Vienna, Austria
- 2Kepler University Clinic, Neuromed Campus, Linz, Austria
- 3Department of Child and Adolescent Psychiatry, Medical University Vienna, Vienna, Austria
- 4Penn Hospital – Black Country Partnership NHS Foundation Trust, Wolverhampton, United Kingdom
- 5Department of Internal Medicine, Hospital Amstetten, Lower Austria, Austria
- 6Hospital Oberpullendorf, Oberpullendorf, Burgenland, Austria
- 7Section of Medical Statistics, Medical University Vienna, Vienna, Austria
- 8Department of Psychosomatic Medicine and Psychotherapy, Section for Medical Psychology, University Ulm, Ulm, Germany
- 9Biopsychosocial Corporation BioPsyC, Vienna, Austria
Background: Social interactive functions such as facial emotion recognition and smell identification have been shown to differ between women and men. However, little is known about how these differences are mirrored in patients with schizophrenia and how these abilities interact with each other and with other clinical variables in patients vs. healthy controls.
Methods: Standardized instruments were used to assess facial emotion recognition [Facially Expressed Emotion Labelling (FEEL)] and smell identification [University of Pennsylvania Smell Identification Test (UPSIT)] in 51 patients with schizophrenia spectrum disorders and 79 healthy controls; furthermore, working memory functions and clinical variables were assessed.
Results: In both the univariate and the multivariate results, illness showed a significant influence on UPSIT and FEEL. The inclusion of age and working memory in the MANOVA resulted in a differential effect with sex and working memory as remaining significant factors. Duration of illness was correlated with both emotion recognition and smell identification in men only, whereas immediate general psychopathology and negative symptoms were associated with emotion recognition only in women.
Conclusion: Being affected by schizophrenia spectrum disorder impacts one’s ability to correctly recognize facial affects and identify odors. Converging evidence suggests a link between the investigated basic and social cognitive abilities in patients with schizophrenia spectrum disorders with a strong contribution of working memory and differential effects of modulators in women vs. men.
Introduction
Humans are social beings who have developed the ability to interpret complex and intertwined social contexts using a large array of cues. In fact, the recognition of non-verbal facial expressions of emotion is essential for social interaction and is an important component of social cognition. Similarly, detection of olfactory signals constitutes an essential part of social behavior in many animals. From an evolutionary perspective olfaction is in fact thought to be the oldest sense (1). Schizophrenia has been shown to be associated with impairments in basic and social cognition, which share some neural circuitry. Deficits in emotion recognition (ER) and smell identification [SI; smell identification deficits (SIDs)] have often been detected in chronic (2), first episode (3), and high-risk patients (4) as well as in unaffected relatives (5, 6) [for SID (7)]. Gender dichotomous differences in these domains have been shown in healthy subjects mostly in women showing higher emotional and olfactory discriminative abilities (8, 9). Similarly, in many, but not all studies, women with schizophrenia have been shown to outperform men with respect to both ER processes and olfactory identification (10, 11). However, some inconsistencies have been reported, which might, among other reasons, be explained by the heterogeneity of instruments used for the assessment of ER and SID in the different studies (2, 12).
Both, SI and ER are brain functions involved in social interaction and are connected to neurocognitive functions (13, 14); both are mediated through overlapping and interconnected brain regions including orbitofrontal and temporal regions. The intertwinement of emotional and olfactory processes has been shown in studies examining the hedonic appraisal of different odors (12), showing impairment in the appraisal of pleasant odors in patients with schizophrenia (15); a deficit that seems more prominent in men (16). In a small study investigating the relationship of ER and SI in 19 patients with schizophrenia and 14 controls, patients showed that poorer performances on facial affect recognition but not on odor detection thresholds or identification tasks (17). Neither sex nor severity of symptoms was modulating factors (17). However, there was a relationship between facial ER and unirhinal right nostril performance that was larger in patients than in control subjects and was apparent specifically for sad faces. To our knowledge, no other study has investigated the relationship between these social cognitive domains and possible gender dimorphism, while taking into account potentially influencing factors such as age and cognitive functions. Both ER and SID have been shown to be impacted by age (9, 18, 19) and to be associated with at least some aspects of neurocognitive functioning (14, 20). Thus, this analysis aimed to shed further light on the relationship between ER and SID with respect to possible gender differences in patients with schizophrenia spectrum disorders compared to healthy controls.
Materials and Methods
Sample
Inpatients and outpatients of the Department of Psychiatry and Psychotherapy of the Medical University of Vienna, Austria, with a DSM-IV-TR diagnosis of schizophrenia, schizophreniform, or schizoaffective disorder aged between 18 and 60 years were recruited. Exclusion criteria were organic mental disorder, mental retardation, pregnancy or lactation at time of assessment, clinically significant, non-corrected impairment of eyesight or of the olfactory system, acute medical condition (e.g., common cold), clinically significant dermatological diseases, atopic syndrome, use of anti-inflammatory, anti-allergic drugs or non-prescribed drugs, and alcohol at the time of assessments.
The sample was compared to healthy controls, recruited through concentric circle recruitment. Being healthy was defined as the absence of current or past psychiatric and organic disorders and of a family history of schizophrenia spectrum disorders. In addition to these, the same exclusion criteria as for patients were applied.
The data presented here are derived from a larger study, which was approved by the local ethics committee. The study was carried out in accordance with their recommendations. Written informed consent was obtained from all subjects before inclusion after thorough explanation of the study procedure in accordance with the Declaration of Helsinki. Furthermore, an unpublished master thesis derived from these data (21).
Assessments
Data regarding sociodemographic and psychiatric history were collected in all participants.
Psychopathology was assessed by a trained rater using the Positive and Negative Syndrome Scale (PANSS) (22), a widely used semistructured interview assessing positive and negative symptoms of schizophrenia and global psychopathology. All raters were trained adequately, and interrater consistencies were assessed within team.
Clinical interview, medical records where available, and the Mini-International Neuropsychiatric Interview (MINI German Version 5.0.0) (23) were used for the assessment of diagnosis, which was done by consensus between two psychiatrists. The MINI is a short, structured interview, applicable by non-specialized rater and used to determine the occurrence of 17 psychiatric disorders.
Facial ER was assessed with the Facially Expressed Emotion Labelling (FEEL) test (24), a computerized assessment using color photographs of different people’s faces from the so-called JACFEE (Japanese and Caucasian Facial Expression of Emotion) series developed by Matsumoto and Ekman in 1988 (25) [cited in Ref. (24)]. The six displayed basic emotions are as follows: anger, sadness, fear, disgust, happiness, and surprise. The FEEL test starts with an emotionally neutral face. The same face then reappears for 300 ms displaying one of the above-mentioned emotions. The task consists of correctly identifying the shown emotion. A total of 42 pictures are presented. The maximum achievable score is 42. The FEEL test shows a high reliability (Cronbach’s coefficient of r = 0.77) compared to other published ER tests (24). Healthy women have been shown to outperform men in subtle expressions of emotions in the FEEL test but not in faces with high emotional expressiveness (26).
Smell identification deficits were assessed using the standardized University of Pennsylvania Smell Identification Test (UPSIT) German version (27, 28). A total of 40 odorants is equally divided onto four scratch and sniff booklets. The odorant is embedded in the microcapsules of 10–50 µg in diameter located on scent strips. The test is forced choice and multiple choice. A broad range of single and multiple odorants that can be divided into different classes are used. The UPSIT has been shown to be highly reliable and internally consistent (29). Normal ranges for the UPSIT are 35–40 for men and 34–40 for women; scores below these ranges are signs of olfactory identification impairments. Healthy women have been shown to outperform men in the UPSIT (29).
Intellectual functioning, specifically an estimate of premorbid intelligence, was assessed with the “Mehrfachwahl-Wortschatz-Intelligenztest” [MWT-B; Multiple-Choice Word Test-B (30), a quick and easy-to-administer multiple-choice word test with 37 items (31)]. The MWT-B was administered to exclude differences that might be explained by significant premorbid IQ variations.
The spatial span subtest of the Wechsler Memory Scale—Revised (WMS) (32) was used to assess visuospatial working memory. Working memory is one of the most commonly described domains of neurocognitive impairment in patients with schizophrenia spectrum disorders (33) and was therefore assessed as one neurocognitive marker in this study.
Statistical Analysis
This analysis was performed in all participants younger than 50 years to avoid potential bias of older age on ER and SID, since older age is known to impact both ER and even more so SID (2, 18). For this purpose, data of seven healthy controls and seven patients aged 50 years or older were excluded from the analysis. Thus, the study population consists of 31 male controls, 48 female controls, 30 male patients, and 21 female patients. However, note that values of 10 controls for the variable UPSIT are missing, as well as values of 7 controls and 2 cases for the variable FEEL.
The primary question was the influence of “group” (i.e., healthy control vs. patient) and sex on UPSIT and FEEL scores. A MANOVA with UPSIT and FEEL scores as dependent variables was calculated considering the main effects “group” and “sex,” as well as the interaction between group and sex. In case of a non-significant interaction, the factor was removed from the final model. In a second model, age and WMS total score were considered additionally. All analyses were repeated for the single target variables UPSIT and FEEL [analyses of variance (ANOVAs)]. ANOVAS were calculated as exploratory analyses for the target variables WMS, MWT, and age with main effects “group” and “sex” as well as their interaction. Pearson correlations were calculated between FEEL, UPSIT, PANSS, and WMS scores as well as duration of illness (DUI). Primary and exploratory analyses were performed using the R program, version 3.3.1®. Further descriptive analyses, correlations, Chi-square tests, and t-tests were performed using IBM SPSS Statistics Version 24®. Effect sizes were calculated using freely available online effect size calculators. All tests were two sided, and level of significance was p < 0.05.
Results
The sample for this analysis consists of 51 patients with a schizophrenia spectrum disorder (41.2% female) and 79 healthy controls (60.8% female). There was a significant difference in age between patients and controls (p = 0.002) but not between women and men (see Tables 1 and 2).
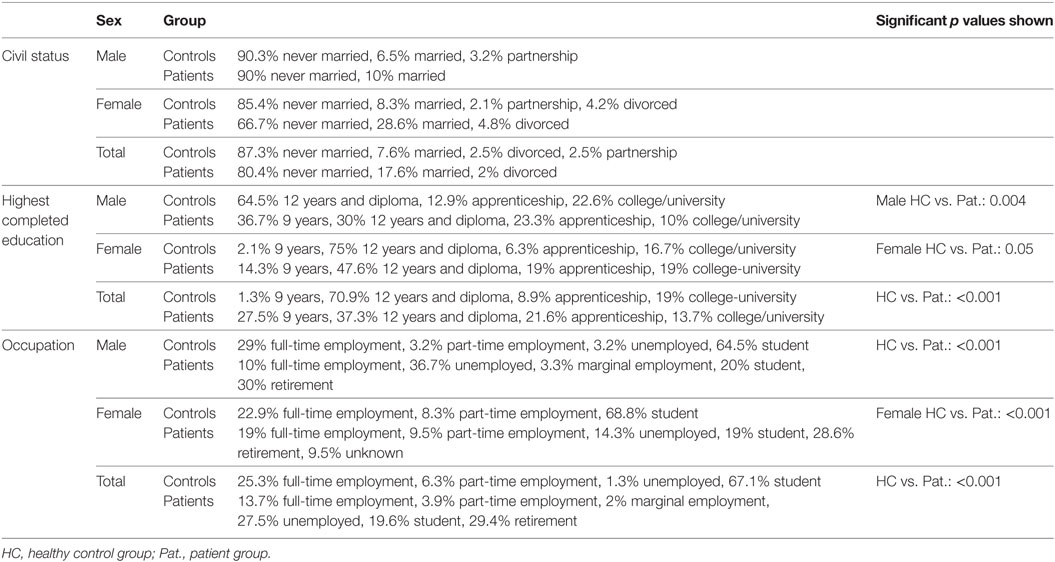
Table 1. Sociodemographic data of patients and controls.
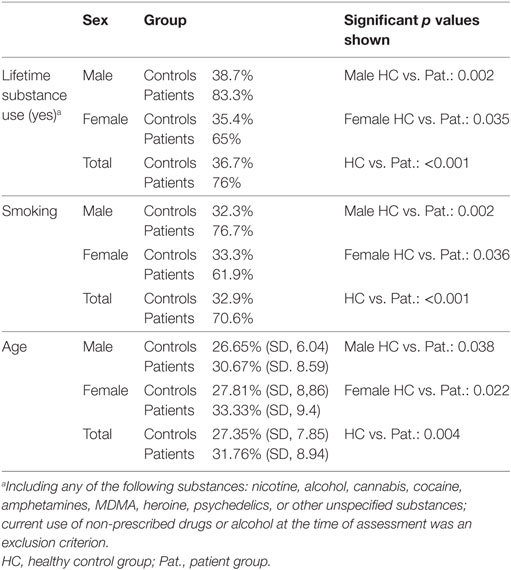
Table 2. Age and substance use in patients and controls.
Group category had a highly significant influence on WMS total scores (p < 0.0001), whereas sex narrowly reached significance level (p = 0.05). Neither sex nor group had a significant influence on MWT-B scores. See Tables 3 and 4 for detailed scores.
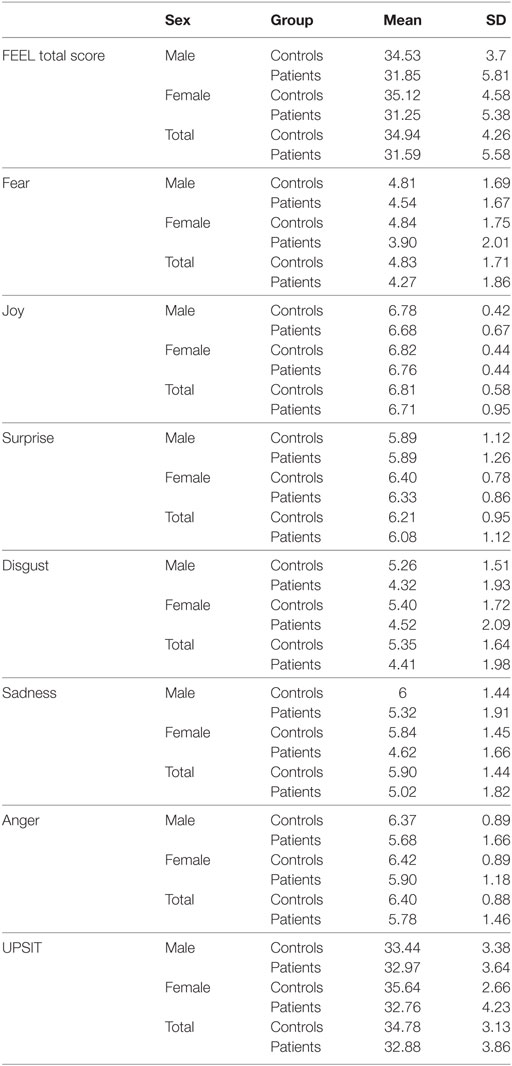
Table 3. Mean values, SDs for FEEL, and subscores and UPSIT.
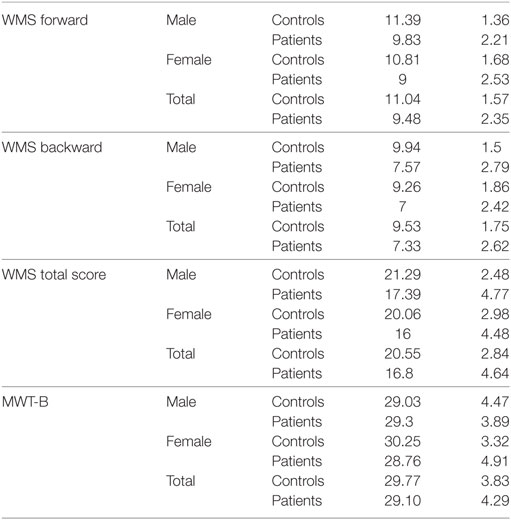
Table 4. Means and SDs for working memory (WMS) and IQ task (MWT-B).
Patients’ Characteristics
Distribution of diagnoses was 43.1% schizophrenia, 23.5% schizophreniform disorder, and 33.3% schizoaffective disorder. There was no significant difference in distribution of diagnoses between female and male patients. Also, there were no significant differences in patients’ characteristics between female and male patients (see Table 5).
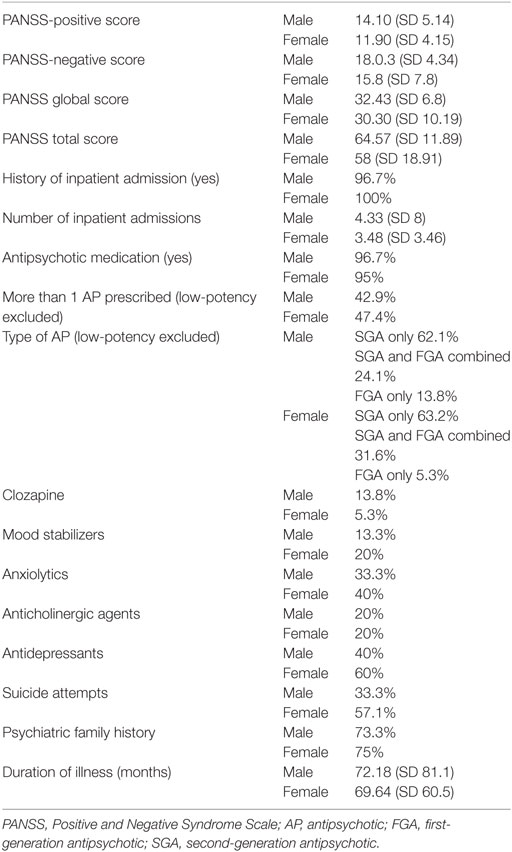
Table 5. Description of patient group.
Primary Analyses
Univariate analyses for UPSIT and FEEL were performed to analyze the influence of sex and group before multivariate analyses.
Smell Identification (UPSIT)
The analysis of variance showed no significant influence of the interaction between sex and age (p = 0.062). The ANOVA with the factors sex and group on UPSIT showed that controls have significantly higher UPSIT scores than patients (p = 0.01) with a moderate effect size (Cohen’s d = 0.529), and sex was only borderline significant (p = 0.07; adjusted R2, 0.08; F-statistic, 6.2 on 2 and 117 df).
In addition, introducing age and WMS scores increased the influence of sex (p = 0.01); on the other hand, the previously significant influence of group category vanished due to its strong relationship with WMS, which had a significant impact on UPSIT scores (p = 0.03; multiple R2, 0.2; adjusted R2, 0.17; F-statistic, 6.5 on 4 and 103 DF). Kendall Tau’s correlation coefficient between WMS total score and group was −0.34, with controls having higher scores than patients. WMS was also correlated with age (Pearson’s correlation coefficient, −0.45). If WMS total score were removed from the ANCOVA, group and age would show a significant influence.
The effect size for the difference between UPSIT scores in males was negligible (Cohen’s d = 0.1). However, in female controls vs. patients, the effect size was large with a Cohen’s d of 0.815. Similarly, differences in UPSIT scores between female controls and male controls had large effect sizes of 0.723, whereas it was negligible with respect to the comparison of sexes in the patient group (Cohen’s d = 0.02).
Emotion Recognition (FEEL)
The interaction between sex and group had no significant influence on FEEL scores and was thus not considered in the analysis of variance. The results showed that sex had no significant influence on FEEL scores (p = 0.89), but group did (p = 0.0004), with healthy controls having significantly higher values on the FEEL test than patients with a moderate effect size (Cohen’s d = 0.675; adjusted R2: 0.09; F-statistic, 6.9 on 2 and 118 df). Additional consideration of age and WMS resulted in a significant influence of WMS (p = 0.01) only.
In addition, the effect size was moderate for the differences in FEEL scores between male controls and patients (Cohen’s d = 0.55) and large for that between female controls and patients (Cohen’s d = 0.775).
Multivariate Analyses of Variance of Sex and Group on UPSIT and FEEL
The interaction of sex and group was not significant neither in the MANOVA nor the MANCOVA, and thus, only main effects were considered. In the MANOVA, only group showed a significant influence on UPSIT and FEEL (p = 0.001), which goes along with the univariate results. However, when age and WMS total scores were included as main factors, sex and WMS became significant (p = 0.03 and p = 0.01, respectively), whereas the influence of group categorization vanished (p = 0.24). The influence of age was not significant (p = 0.3).
Further Analyses
FEEL Subscores
With respect to FEEL subscores, there were between-group differences between patients and healthy controls with moderate effect sizes for anger (p = 0.004, Cohen’s d = 0.51), for sadness (p = 0.004, Cohen’s d = 0.54), and for disgust (p = 0.005, Cohen’s d = 0.52) only, with patients showing lower scores. Male patients showed lower scores than their healthy counterparts (p = 0.05) with a moderate effect size (Cohen’s d = 0.54) in recognizing disgust and bordering significance in recognizing anger (p = 0.059, Cohen’s d = 0.52). The latter was mirrored in female patients with borderline significance for anger (p = 0.052, Cohen’s d = 0.49) and for fear (p = 0.059, Cohen’s d = 0.49). However, female patients also had lower scores than their healthy counterparts in recognizing sadness (p = 0.003) with a large effect size (Cohen’s d = 0.78). There were no significant differences in FEEL subscores between male and female patients. In healthy controls, women had better results in identifying surprise than men (p = 0.026, Cohen’s d = 0.53).
Both patients and controls reached best performances with respect to identifying happy faces and worse for fearful ones. Males and females in both groups mirrored the results on the hierarchy of positive and negative valences; however, male patients had lowest scores for disgust (see Table 3).
Clinical Modulators
Correlation coefficients were calculated between PANSS, estimate of DUI (defined here as the time since appearance of first psychotic symptoms), FEEL, and UPSIT scores to investigate possible modulators.
FEEL and UPSIT correlated significantly with each other (p < 0.001, r = 0.502). Neither UPSIT nor FEEL correlated significantly with PANSS total scores.
Looking at female and male patients separately, the following results were yielded: both within the male and the female patient group FEEL and UPSIT correlated significantly with each other (males: r = 0.487, p = 0.009; females: r = 0.528, p = 0.014), mirroring the results in the entire patient group. However, only in male patients, DUI correlated negatively with both FEEL (r = −0.409, p = 0.031) and UPSIT (r = −0.528, p = 0.003). However, only in female patients, there was a correlation between FEEL scores and psychopathology, i.e., PANSS total (r = −0.526, p = 0.017) and PANSS-negative score (r = −0.696, p = 0.001).
However, both UPSIT and FEEL correlated positively with WMS total scores (WMS-UPSIT p = 0.001, r = 0.328; WMS-FEEL p = 0.000, r = 0.411). Specifically, WMS total score correlated positively with FEEL in the female patient group (p = 0.010, r = 0.608) and with UPSIT in the male patient group (p = 0.003, r = 0.585). Correlations between WMS total score and UPSIT or FEEL were non-significant in all other subgroups.
Discussion
The first finding of this analysis is that being affected by a schizophrenia spectrum disorders impact one’s ability to correctly recognize facial affects and identify odors. Indeed, patients performed worse than healthy controls in both tasks. Deficits in ER and SID in patients with schizophrenia are quite a robust finding (2, 7), and our results serve to corroborate the validity of our sample with respect to these differences.
However, the impact of sex seems more complex both in the existing literature as well as in our sample. With respect to facial affect recognition, the right-hemispheric hypothesis postulates that men might be more affected by deficits in ER due to a greater activation of right-hemispheric regions during such tasks and greater right-hemispheric dysfunctions in schizophrenia (34). The currently available literature is somewhat inconsistent regarding the direction of sex differences of ER in patients with schizophrenia with some studies reporting a female advantage (10, 35), others, e.g., meta-analytical data revealing no effect of sex (2, 36). As for SI, several previous studies performed in healthy samples and in patients with schizophrenia have described subtly better olfactory identification performances in women (8). In our analysis, effects of sex were only borderline significant for UPSIT and not significant for FEEL scores in the univariate analyses, with healthy women having slightly higher scores in both tasks with large effect sizes compared to their diseased counterparts. In addition, healthy women also recognized odors better than their male counterparts, suggesting that the possible female superiority in these tasks might not be only illness related. As a matter of the fact, the multivariate analysis revealed that sex-related effects might become more relevant when additional, potentially influencing factors, such as age and visuospatial working memory, are accounted for. Our results suggest that sex and working memory capacities together might possibly supersede direct effects related to the illness itself. Indeed, both SID and ER scores correlated with visuospatial working memory results. Mind you, however, that working memory itself is strongly affected by illness, with working memory capacities being worse in patients than in controls for both sexes; this impairment being a robust finding in schizophrenia (13). Hence, these findings suggest that sex-related differences in ER and SI tasks in patients with schizophrenia spectrum disorders might need to be interpreted within the context of working memory capacities. ER is acknowledged as a social cognitive ability in the larger sense of the term and SID can be seen as a higher cognitive function, which similarly to ER requires neurocognitive and social cognitive skills. In this context, our results can be cautiously interpreted as evidence for these tasks being indeed complex social cognitions related to neurocognitive functions and being subject to more complex sex-related effects. Also, this analysis reveals that ER and SID are intertwined, i.e., correlated with each other in both sexes, suggesting again that they might underlie similar pathomechanisms in the context of schizophrenia spectrum disorders.
Interestingly, in male patients only, both SID and ER tasks were related to DUI, i.e., the longer the DUI, the stronger the impairment in both tasks, hinting to an effect of chronicity of illness on these abilities that women might be able to compensate somewhat better. However, in female patients, current psychopathology (represented by the PANSS total score) and negative symptoms (PANSS negative score) correlated negatively with facial affect recognition, underlining the notion of the effect of immediate psychopathology on this social cognitive task. Thus, our results might suggest a more complex relationship with sex, which goes beyond a mere dichotomy of superiority or inferiority.
With respect to emotional valence, both groups performed best at recognizing happy faces and identifying fear seemed most difficult to most. Specifically, patients had more difficulties recognizing the negative emotions anger, sadness, and disgust than controls with a differential pattern for men (with disgust and anger being the emotions with the largest difference to healthy controls) and women (with anger, fear, and sadness, respectively).
The more accurate identification of emotionally positive faces and higher number of errors in recognizing negative emotions is a pattern that has been shown in healthy populations and in patients with schizophrenia spectrum disorders (37, 38). The literature supports indeed the notion that negative emotions are more difficult to recognize than positive ones (39, 40). In patients, abnormalities in self-representation and causal attributions that might include misinterpreting negative emotions of others more easily have been postulated to facilitate the development of paranoid ideas alongside a certain degree of distortion of the perception of reality (41). Difficulties correctly identifying facial affects of others might easily lead one to misinterpret facial cues and overestimate or underestimate reactions of social friendliness or adversity, resulting in either suspiciousness or an increased vulnerability to being victimized.
Several limitations that may influence the interpretation of our findings must be addressed. First, the sample size, especially the female sample, is rather small, and some effects might have been concealed. However, most of those differences that were significant had moderate to large effect sizes. Second, patients and controls differed in age; however, the multivariate analysis excluded remaining relevant effects of age. Also, other features of the olfactory system, such as odor threshold sensitivity, unirhinal presentation of odors, which might have allowed for a more differentiated, hemispheric-sensitive appraisal of potential SIDs, and separate analysis of odor valence were not assessed. Menstrual cycle was not assessed; however, most authors perceive a reduction of olfactory functions to mere effects of reproductive hormones as an oversimplification (8). Although we did not specifically correct for type of antipsychotic, there was no correlation between type of antipsychotic (i.e., atypical vs. typical) or monopharmacy vs. polypharmacy and ER or SID test scores. This is somewhat in contrast with meta-analytical data in ER, where greater impairments have been shown with first-generation antipsychotics (2). Of note, there were no significant differences between male and female patients in patients’ characteristics. Also, there were no associations between diagnosis and SID or ER task results for either sex. Testing situation and sex of participant vs. rater was not assessed separately. However, it can be safely assumed that testing situations were fairly similar for all participants, since all active raters were women, and all assessments were conducted in a quiet room without other observers. Nevertheless, it cannot be excluded that a gender-related bias came into play. As a matter of fact, men have been shown to increase their efforts to impress women in competitive situations with a female observer; however, these efforts might rather tax actual cognitive capacities (42). Finally, other groups have suggested that sex of poser vs. that of observer, which we did not assess, might play a role in ER (43). Thus, the results of our analysis must be interpreted in light of these limitations.
In conclusion, both social cognitive abilities assessed here, ER, and SI were shown to being associated with each other in male and in female patients with schizophrenia spectrum disorders with a strong contribution of effects of working memory. Indeed, effects of sex were only evident when taking into account working memory capacities. Differential effects of modulators on these tasks were seen in women vs. men. Converging evidence of this analysis and of previous studies suggests a link between basic neurocognitive and social cognitive functions in patients with schizophrenia spectrum disorders. Further research to evaluate the direction of causality and the specificity of these findings, as well as the magnitude of the effect of modulating factors, should be conducted. Also, a stronger focus on investigating sex vs. gender effects might help clarify some of the reported inconsistencies.
Ethics Statement
This study was carried out in accordance with the recommendations of the Ethics Committee of the Medical University of Vienna, Austria with written informed consent from all subjects. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Ethics Committee of the Medical University of Vienna, Austria.
Author Contributions
NM designed, implemented, and managed the study as Co-PI; was actively involved in participants’ recruitment, interrater training, data management, statistical analysis, and interpretation; and; drafted and elaborated all versions of the manuscript. RK and MS designed and implemented the study, were actively involved in recruitment, data acquisition and analysis, interpretation, and revision of the manuscript. TA, CH, and AG were actively involved in data acquisition, recruitment, assessments, interpretation of data, and revising the manuscript. SZ was involved in the concept and design of the original study, data analysis, statistical calculations, interpretation of data, and critical revisions of the manuscript. HH and HT were involved in the design of the study, provision of assessment instruments, data interpretation and revision of manuscript. HA designed, managed, and supervised the study as Co-PI; contributed substantially to data interpretation; and critically revised all version of the manuscript. All authors contributed to and approved of the final version of the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Parts of the data from the study have been presented as posters at the Conference of the European Psychiatry Association in March 2011 in Vienna, Austria. Lucia Schlehaider and Sabine Inreiter contributed to data acquisition. We are grateful to all participants for their contribution.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sector.
References
1. Hoover KC. Smell with inspiration: the evolutionary significance of olfaction. Am J Phys Anthropol (2010) 143(Suppl 51):63–74. doi:10.1002/ajpa.21441
2. Kohler CG, Walker JB, Martin EA, Healey KM, Moberg PJ. Facial emotion perception in schizophrenia: a meta-analytic review. Schizophr Bull (2010) 36(5):1009–19. doi:10.1093/schbul/sbn192
3. Barkl SJ, Lah S, Harris AW, Williams LM. Facial emotion identification in early-onset and first-episode psychosis: a systematic review with meta-analysis. Schizophr Res (2014) 159(1):62–9. doi:10.1016/j.schres.2014.07.049
4. Turetsky BI, Kamath V, Calkins ME, Brewer WJ, Wood SJ, Pantelis C, et al. Olfaction and schizophrenia clinical risk status: just the facts. Schizophr Res (2012) 139(1–3):260–1; author reply 2–3. doi:10.1016/j.schres.2012.04.016
5. Allott KA, Rice S, Bartholomeusz CF, Klier C, Schlogelhofer M, Schafer MR, et al. Emotion recognition in unaffected first-degree relatives of individuals with first-episode schizophrenia. Schizophr Res (2015) 161(2–3):322–8. doi:10.1016/j.schres.2014.12.010
6. Surguladze SA, Chkonia ED, Kezeli AR, Roinishvili MO, Stahl D, David AS. The McCollough effect and facial emotion discrimination in patients with schizophrenia and their unaffected relatives. Schizophr Bull (2012) 38(3):599–607. doi:10.1093/schbul/sbq141
7. Moberg PJ, Kamath V, Marchetto DM, Calkins ME, Doty RL, Hahn CG, et al. Meta-analysis of olfactory function in schizophrenia, first-degree family members, and youths at-risk for psychosis. Schizophr Bull (2014) 40(1):50–9. doi:10.1093/schbul/sbt049
8. Doty RL, Cameron EL. Sex differences and reproductive hormone influences on human odor perception. Physiol Behav (2009) 97(2):213–28. doi:10.1016/j.physbeh.2009.02.032
9. Fusar-Poli P, Placentino A, Carletti F, Landi P, Allen P, Surguladze S, et al. Functional atlas of emotional faces processing: a voxel-based meta-analysis of 105 functional magnetic resonance imaging studies. J Psychiatry Neurosci (2009) 34(6):418–32.
10. Scholten MR, Aleman A, Montagne B, Kahn RS. Schizophrenia and processing of facial emotions: sex matters. Schizophr Res (2005) 78(1):61–7. doi:10.1016/j.schres.2005.06.019
11. Malaspina D, Keller A, Antonius D, Messinger JW, Goetz DM, Harkavy-Friedman J, et al. Olfaction and cognition in schizophrenia: sex matters. J Neuropsychiatry Clin Neurosci (2012) 24(2):165–75. doi:10.1176/appi.neuropsych.11070154
12. Kamath V, Turetsky BI, Moberg PJ. Identification of pleasant, neutral, and unpleasant odors in schizophrenia. Psychiatry Res (2011) 187(1–2):30–5. doi:10.1016/j.psychres.2010.12.011
13. Ventura J, Wood RC, Jimenez AM, Hellemann GS. Neurocognition and symptoms identify links between facial recognition and emotion processing in schizophrenia: meta-analytic findings. Schizophr Res (2013) 151(1–3):78–84. doi:10.1016/j.schres.2013.10.015
14. Compton MT, McKenzie Mack L, Esterberg ML, Bercu Z, Kryda AD, Quintero L, et al. Associations between olfactory identification and verbal memory in patients with schizophrenia, first-degree relatives, and non-psychiatric controls. Schizophr Res (2006) 86(1–3):154–66. doi:10.1016/j.schres.2006.06.007
15. Crespo-Facorro B, Paradiso S, Andreasen NC, O’Leary DS, Watkins GL, Ponto LL, et al. Neural mechanisms of anhedonia in schizophrenia: a PET study of response to unpleasant and pleasant odors. JAMA (2001) 286(4):427–35. doi:10.1001/jama.286.4.427
16. Moberg PJ, Arnold SE, Doty RL, Kohler C, Kanes S, Seigel S, et al. Impairment of odor hedonics in men with schizophrenia. Am J Psychiatry (2003) 160(10):1784–9. doi:10.1176/appi.ajp.160.10.1784
17. Kohler CG, Barrett FS, Gur RC, Turetsky BI, Moberg PJ. Association between facial emotion recognition and odor identification in schizophrenia. J Neuropsychiatry Clin Neurosci (2007) 19(2):128–31. doi:10.1176/jnp.2007.19.2.128
18. Doty RL, Kamath V. The influences of age on olfaction: a review. Front Psychol (2014) 5:20. doi:10.3389/fpsyg.2014.00020
19. Doty RL, Shaman P, Applebaum SL, Giberson R, Siksorski L, Rosenberg L. Smell identification ability: changes with age. Science (1984) 226(4681):1441–3. doi:10.1126/science.6505700
20. Addington J, Saeedi H, Addington D. Facial affect recognition: a mediator between cognitive and social functioning in psychosis? Schizophr Res (2006) 85(1–3):142–50. doi:10.1016/j.schres.2006.03.028
21. Mossaheb N. Facial emotion recognition and smell identification in patients with schizophrenia, their first-degree relatives and healthy controls – does sex matter? [Master Thesis]. Vienna: Medical University Vienna (2012).
22. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull (1987) 13(2):261–76. doi:10.1093/schbul/13.2.261
23. Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry (1998) 59 Suppl 20:22–33; quiz 4–57.
24. Kessler H, Bayerl P, Deighton RM, Traue HC. Facially expressed emotion labeling (FEEL): PC-gestützer Test zur Emotionserkennung. Verhaltenstherapie und Verhaltensmedizin (2002) 23(3):297–306.
25. Matsumoto D, Ekman P. In: Ekman DP, editor. Japanese and Caucasian Facial Expressions of Emotion (JACFEE) and Neutral Faces (JACNeuF). San Francisco, 401 Parnassus, S.F., CA: Department of Psychiatry, University of California (1988).
26. Hoffmann H, Kessler H, Eppel T, Rukavina S, Traue HC. Expression intensity, gender and facial emotion recognition: women recognize only subtle facial emotions better than men. Acta Psychol (Amst) (2010) 135(3):278–83. doi:10.1016/j.actpsy.2010.07.012
27. Doty RL, Shaman P, Dann M. Development of the University of Pennsylvania Smell Identification Test: a standardized microencapsulated test of olfactory function. Physiol Behav (1984) 32(3):489–502. doi:10.1016/0031-9384(84)90269-5
28. Doty RL, Shaman P, Kimmelman CP, Dann MS. University of Pennsylvania Smell Identification Test: a rapid quantitative olfactory function test for the clinic. Laryngoscope (1984) 94(2 Pt 1):176–8. doi:10.1288/00005537-198402000-00004
29. Doty RL, Applebaum S, Zusho H, Settle RG. Sex differences in odor identification ability: a cross-cultural analysis. Neuropsychologia (1985) 23(5):667–72. doi:10.1016/0028-3932(85)90067-3
31. Lehrl S, Triebig G, Fischer B. Multiple choice vocabulary test MWT as a valid and short test to estimate premorbid intelligence. Acta Neurol Scand (1995) 91(5):335–45. doi:10.1111/j.1600-0404.1995.tb07018.x
32. Wechsler D. WMS-R Wechsler Memory Scale-Revised. San Antonio: The Psychological Corporation (1987).
33. Aleman A, Hijman R, de Haan EH, Kahn RS. Memory impairment in schizophrenia: a meta-analysis. Am J Psychiatry (1999) 156(9):1358–66. doi:10.1176/ajp.156.9.1358
34. Indersmitten T, Gur RC. Emotion processing in chimeric faces: hemispheric asymmetries in expression and recognition of emotions. J Neurosci (2003) 23(9):3820–5.
35. Vaskinn A, Sundet K, Friis S, Simonsen C, Birkenaes AB, Engh JA, et al. The effect of gender on emotion perception in schizophrenia and bipolar disorder. Acta Psychiatr Scand (2007) 116(4):263–70. doi:10.1111/j.1600-0447.2007.00991.x
36. Chan RC, Li H, Cheung EF, Gong QY. Impaired facial emotion perception in schizophrenia: a meta-analysis. Psychiatry Res (2010) 178(2):381–90. doi:10.1016/j.psychres.2009.03.035
37. van’t Wout M, van Dijke A, Aleman A, Kessels RP, Pijpers W, Kahn RS. Fearful faces in schizophrenia: the relationship between patient characteristics and facial affect recognition. J Nerv Ment Dis (2007) 195(9):758–64. doi:10.1097/NMD.0b013e318142cc31
38. Linden SC, Jackson MC, Subramanian L, Wolf C, Green P, Healy D, et al. Emotion-cognition interactions in schizophrenia: implicit and explicit effects of facial expression. Neuropsychologia (2010) 48(4):997–1002. doi:10.1016/j.neuropsychologia.2009.11.023
39. Jansari A, Rodway P, Goncalves S. Identifying facial emotions: valence specific effects and an exploration of the effects of viewer gender. Brain Cogn (2011) 76(3):415–23. doi:10.1016/j.bandc.2011.03.009
40. Johnston PJ, Devir H, Karayanidis F. Facial emotion processing in schizophrenia: no evidence for a deficit specific to negative emotions in a differential deficit design. Psychiatry Res (2006) 143(1):51–61. doi:10.1016/j.psychres.2005.08.006
41. Bentall RP, Corcoran R, Howard R, Blackwood N, Kinderman P. Persecutory delusions: a review and theoretical integration. Clin Psychol Rev (2001) 21(8):1143–92. doi:10.1016/S0272-7358(01)00106-4
42. Nauts S, Metzmacher M, Verwijmeren T, Rommeswinkel V, Karremans JC. The mere anticipation of an interaction with a woman can impair men’s cognitive performance. Arch Sex Behav (2012) 41(4):1051–6. doi:10.1007/s10508-011-9860-z
Keywords: schizophrenia, emotion recognition, smell identification, social cognition, sex
Citation: Mossaheb N, Kaufmann RM, Schlögelhofer M, Aninilkumparambil T, Himmelbauer C, Gold A, Zehetmayer S, Hoffmann H, Traue HC and Aschauer H (2018) The Impact of Sex Differences on Odor Identification and Facial Affect Recognition in Patients with Schizophrenia Spectrum Disorders. Front. Psychiatry 9:9. doi: 10.3389/fpsyt.2018.00009
Received: 11 October 2017; Accepted: 12 January 2018;
Published: 31 January 2018
Edited by:
Philip D. Harvey, Leonard M. Miller School of Medicine, United StatesReviewed by:
Antonio Bruno, University of Messina, ItalyWilliam Horan, University of California, Los Angeles, United States
Copyright: © 2018 Mossaheb, Kaufmann, Schlögelhofer, Aninilkumparambil, Himmelbauer, Gold, Zehetmayer, Hoffmann, Traue and Aschauer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nilufar Mossaheb, nilufar.mossaheb@meduniwien.ac.at