 Adam W. Kiefer
Adam W. Kiefer David Pincus
David Pincus Michael J. Richardson
Michael J. Richardson Gregory D. Myer
Gregory D. Myer- 1Division of Sports Medicine, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH, United States
- 2Department of Pediatrics, College of Medicine, University of Cincinnati, Cincinnati, OH, United States
- 3Center for Cognition, Action and Perception, University of Cincinnati, Cincinnati, OH, United States
- 4Department of Psychology, Chapman University, Orange, CA, United States
- 5Department of Psychology, Macquarie University, Sydney, NSW, Australia
- 6The Micheli Center for Sports Injury Prevention, Waltham, MA, United States
Lack of adequate physical activity in children is an epidemic that can result in obesity and other poor health outcomes across the lifespan. Physical activity interventions focused on motor skill competence continue to be developed, but some interventions, such as neuromuscular training (NMT), may be limited in how early they can be implemented due to dependence on the child’s level of cognitive and perceptual-motor development. Early implementation of motor-rich activities that support motor skill development in children is critical for the development of healthy levels of physical activity that carry through into adulthood. Virtual reality (VR) training may be beneficial in this regard. VR training, when grounded in an information-based theory of perceptual-motor behavior that modifies the visual information in the virtual world, can promote early development of motor skills in youth akin to more natural, real-world development as opposed to strictly formalized training. This approach can be tailored to the individual child and training scenarios can increase in complexity as the child develops. Ultimately, training in VR may help serve as a precursor to “real-world” NMT, and once the child reaches the appropriate training age can also augment more complex NMT regimens performed outside of the virtual environment.
The high prevalence of overweight and obese children continues to be a major public health problem (1). Myriad factors underlie this etiology, with physical inactivity identified as a primary cause (2), and one potential mechanism is that many children are not developing the motor skill repertoire and movement confidence at a rate necessary to initiate and maintain a healthy level of physical activity (3, 4). Specifically, both body mass index and physical activity have shown to be predictive of individuals’ Functional Movement Screen scores (5). Further, childhood motor skill proficiency has demonstrated to be predictive of adolescent physical activity (6, 7). While there is limited evidence that there exists a direct link between motor skill proficiency and motor skill confidence, it is likely that motor skill competency is accompanied by motor skill confidence, with the latter a possible mediator in the relation between motor skill competency and obesity. Neuromuscular training (NMT) is an established conceptual program designed to fill this void and improve physical activity in children. NMT is designed to enhance health-related and skill-related components of physical fitness that facilitate safe, effective, and developmentally appropriate fitness training for school-age children (8–10). Specifically, NMT is a focused set of motor control and strength building activities that promote the development of a child’s neurocognitive and perceptual-motor capabilities and, ultimately, ameliorates fundamental motor skill deficits to promote movement confidence. Movement confidence and competence are necessary to promote increases in physical activity and build interest in behaviors (11) that, combined, meet the 60 min or more of moderate to vigorous physical activity, which make up current public health recommendations.
Importantly, NMT-based skill development and retention requires that the child’s level of cognitive and perceptual-motor development is at a level appropriate for individualized programming—typically around 6 or 7 years of age (10). Appropriate programming for children is also conditional on the child’s training age—an age that represents the child’s prior experiences of context-specific training and driven, in part, by the child’s natural development. The initiation of training at an earlier age relates to an increased likelihood of avoiding physical inactivity later in life (12, 13). Thus, an obvious solution is to start the training age “clock” earlier using NMT to advance the time course of motor skill proficiency. This is not easy, however, as the introduction of the child to training is dependent on whether the child is physically or mentally prepared for formalized and specialized training at an earlier age. Therefore, perceptual-motor skill development may be a limiting factor for earlier initiation of NMT. Thus, new interventions are needed to circumvent this training barrier.
In Virtuo Training Scenarios
Virtual reality (VR), or in virtuo,1 training is a viable option to manage limitations inherent to implementation of NMT in children in the early phases of perceptual-motor skill development. The advantage of VR-based training over more standard real-world training interventions (15–19) is that VR can leverage known principles that underlie an information-based behavioral account of motor development (20, 21), and this does not necessitate more advanced phases of perceptual-motor skill developmental that are prerequisites of NMT and other formalized activities. An information-based account presupposes that proficient motor performance arises via unique, learned relations between the information available to the child via their environment and the biomechanical properties of the motor system as children assemble their bodies in specific ways to complete a given task (22–24). Consider that from the time a child is born, the cognitive-perceptual-motor systems are honed to capitalize on action possibilities in the environment. Over time, children learn to exploit information about their bodies (e.g., visual, proprioceptive, and other sensory information about limb and body size and position; muscle strength and biomechanics) as well as information about the world around them (e.g., the natural physics of the world and of objects with which they interact) as they move through and act on their environment. The success and failure of these endeavors provide children feedback as they learn the extent of their action capabilities and ultimately lead to the development of goal-directed behaviors. Through the course of normal development, the child executes tasks of greater complexity as he/she learns to combine individual movements into strings of movement patterns to achieve task goals and, eventually, strings of task goals. Thus, every behavior is a set of perception–action feedback loops that shape the child’s time course of natural development and serves as the dynamic substratum for how children interact with the world around them.
Conversely, a child with motor-skill deficits and/or low movement confidence may struggle to take full advantage of these types of perception–action relations and, as a result, may perform movements more slowly, or default to more basic, early stage movement patterns compared to their typically developing peers (e.g., consider a stage two throw). Such performance deficits may be exacerbated as these children observe their peers performing more and more complex tasks with greater success, while the children with lower motor skill proficiency toil in movement patterns that are suboptimal for adequate performance gains. This can further diminish movement confidence and can lead to a cascade of movement deficits that underlie reduced physical activity, and that will lead the child down the path toward obesity later in life. VR training can integrate the necessary information-based interventions into simulated play in such a way that the child can learn to exploit these perception–action relations at their own pace to optimize motor skill learning. The potential to jump-start the movement-deficient child with fully immersive scenarios can build confidence in movement strategies in a safe and “fun” environment.
Fully Immersive Virtual Environments (FIVEs)
Virtual reality-based training that targets perception–action relations mandates certain requirements for effective implementation, with presence the most important for successful implementation. Presence is achieved when the VR experience compels a feeling of being present in an environment other than the real, physical environment in which the individual is actually performing (25). Presence is increased through the development of specific immersion criteria within a given scenario. Here, we define a FIVE as one made up of five immersion criteria (see Table 1): (1) physical, (2) spatial, (3) strategic, (4) social, and (5) narrative. Similar to Weiss et al. we define general immersion as the extent to which the scenario refocuses the child’s sensations and perception from the real world to the virtual one (26), with all five criteria integral to the achievement of that goal.

Table 1. Examples of essential criteria for a fully immersive virtual environment training scenario.
Physical immersion is accomplished through an ambulatory, three-dimensional (3D) environment that allows the child to navigate the virtual world by walking or running through the virtual (and real) space (27)—with real scale movement especially important for the physically inactive child. Spatial immersion is characterized by a virtual world that is perceptually convincing to the child: that is, objects are of similar scale and move as they would in the physical world (i.e., natural physics) and the child perceives her movement to match that of the real world based on believable optical information, or optic flow—the pattern of motion available from the ground and background surfaces that specifies information about movement speed and direction (28, 29). Strategic immersion requires a combination of immediate, physical responses with more cerebral, cognitive decisions adopted to complete scenario related tasks. This can be enhanced through adaptive artificial intelligence (AI) and well-designed scenarios will require both types of stratagem for successful performance. The fourth component is social immersion and relates to the child’s interaction with other non-player characters (NPCs) that are present in the virtual world. Additional children or an instructor may drive this type of character—commonly referred to as avatars—and these humans may or may not share the same real-world physical space as the child. More likely, these characters are driven by AI models of behavior, and thus termed virtual humans. Importantly, if it is difficult for the child to tell the difference between a human-driven avatar and a virtual human, the social immersion is high. Finally, narrative immersion involves the child’s investment in the scenario or how much he/she cares about the additional NPCs and overall task goals. This is the story for the scenario and serves to motivate the child to perform energetically and in a way that can translate to the real world. Clinical-based VR interventions can be successful in the absence of some of these criteria (26). However, together, these components provide a foundation for the development of FIVE scenarios that can ground the child in a learning-rich in virtuo environment and require physical interaction to promote the transfer of learned skills to real world activities (see Table 2).
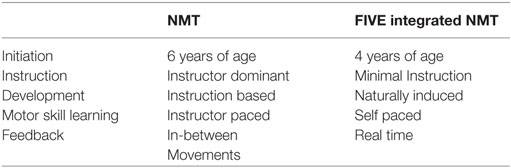
Table 2. A comparison of classic neuromuscular training (NMT) and fully immersive virtual environment (FIVE) integrated NMT.
A scenario that meets these five criteria can become extremely complex from both a hardware integration and virtual environment design standpoint. The former necessitates a head-mounted display (HMD) with a wide (≥100°) field of view for visualizing the 3D virtual environment. The HMD also needs to be wireless (i.e., untethered) with appropriate child-sized head straps, mounts, and padding for visual stability during active movements. A wireless degree of freedom positional tracking system should be used in conjunction with the HMD to provide a 1:1 mapping between the child’s position in the real and virtual environments. Failure to do so will result in a disruption of the child’s sense of realness in the virtual environment, and this can lead to feelings of physical disorientation and nausea (30). Accordingly, such a system requires a large physical space for the child to move—a 5 m × 5 m space is a minimum recommendation—to promote full-form movements and a physically active experience. Additional hardware technologies that provide tactile information (e.g., haptic devices) can provide additional feedback to the child as he or she interacts with the virtual world.
The remaining immersion criteria (strategic, social, and narrative) are more complex from a design standpoint. The development of 3D models that make up the environment can be tedious and expensive; however, well-designed environments, ground textures, and non-player character meshes can greatly enhance the strategic, social, and narrative immersion for the child. Similarly, NPC context specific movements require smooth animations, with true virtual humans requiring precursory motion capture animations of real, age-specific participants, and avatars requiring high fidelity motion capture with minimal lag times for real-time movement display. These animated movements also need to be accompanied by behaviors that are believable within the broader training context.
Complex AI can drive larger scale behavioral networks of artificial agents that move through the world and interact with it, each other, and the child in a believable way. These behavioral networks enhance the strategic immersion of the scenario by facilitating highly specific NPC responses to the user. Non-player character voice recognition also enhances the social immersion and provides the child a more natural means for communication with such characters. These types of non-player characters make up a key component of the virtual environment and establish a believable narrative that engages the child. Together, these five components (physical, spatial, strategic, social, and narrative) contribute to the overall immersion that the child experiences and facilitate the achievement of motor skill development goals.
Initiate an Earlier Training Clock with Fives
In consideration of an information-based behavioral account, the initiation of training at an early age requires an intervention that can target the developing child at the level of information (i.e., feedback) to catalyze motor skill proficiency. VR is uniquely equipped for this and, specifically, can be used to artificially modify visual feedback the child receives as he/she moves through the virtual and real-world space. Thus, the VR scenario covertly modulates the child’s producible motor patterns in a similar way to how a child learns perceptual-motor relations while moving in the real world (i.e., implicit rather than explicit training). This training strategy is not without precedence. The manipulation of visual information through artificial visual displays is consistently effective in changing adult behavior (22, 31–40). For example, artificially manipulating the information that specifies the rotational kinematics of a hand-held object (i.e., decoupling the inertial gain) to optically specify a faster movement of the object on a virtual display while the wielder’s actual movements are hidden from view results in the wielder perceiving a lighter object, and vice versa (39, 40). Analogously, altering the rate of optic flow elicits changes in the walking speed of healthy adults by dissociating the biomechanics of their gait from their perception of walking speed (22). The pattern of optic flow can thus be shifted to the left or right and participants exhibit compensatory postural and steering adjustments that can cause them to walk to the left or right of an intended target (35, 36). This is consistent with the highly successful external focus of attention approach that is well supported in the motor learning literature (41–43).
Such visually induced changes to perception of heaviness and walking speed provide the initial theoretical foundation for the general in virtuo training, we propose to optimize training scenarios for children. Through the utilization of FIVE scenarios, a training regimen can be developed that considers the motor skill deficiencies of the individual child and affects change to their motor patterns gradually over the time course of the prescribed training. The process would likely begin with an assessment of the child’s overall movement capabilities and propensity for physical inactivity. Once completed, several FIVE scenarios could be developed to improve on the child’s existing deficits. These scenarios might involve fundamental movements (e.g., squatting, running, cutting, jumping, or landing) performed in a realistic environment within the context of structured play such as a virtual game of hopscotch, avoiding NPCs in a game of tag, or even chasing the random, 3D movement of a fluttering butterfly. During such tasks, the visual information that pertains to the child’s movement (e.g., optic flow, the movements of virtual limbs, the eye height of the child) in the virtual environment is altered in such a way that the child naturally and subconsciously slows their movements while simultaneously honing their perceptual-motor relations. These types of scenarios would allow the child to refine movement patterns at their own pace, during play, and with only minimal interaction with an instructor. This also allows for scenario complexity to increase during training while building the child’s confidence and increasing her motivation instead of overwhelming the child with difficult movements. Consider that a child learns much of her movement skills in a rich, complex world of information, objects, and people throughout normal development. FIVE scenarios can be designed in a similar way, with added situational complexity used to increase cognitive demands without burdening the child with extremely difficult tasks that require movements beyond the child’s capabilities. As training in these scenarios progresses, the visual information can gradually change until it matches the optic flow and the speed of limb movements in the real world. The progression of this may require several FIVE scenarios across many training sessions, as a precursor to formalized NMT. In this light, a child with a reduced training age might be able to “catch up” to his or her peers through FIVE-enhanced motor skill development, as the goal for FIVE scenarios is to support active reintegration of the child into real-world scenarios with their peers.
Integrating Fives with NMT
Neuromuscular training and FIVE scenarios do not have to be mutually exclusive. As training progresses in FIVE scenarios, NMT-specific exercises can be introduced to the child, initially at a very rudimentary level, to build a foundation of task-specific training. At this point, feedback can be given to the child in virtuo to begin preliminary training of technique. For example, the visual information could be adapted in real time so that the next time the child lands from a jump the visual information about his/her height subtly changes to encourage a deeper knee bend during landing. As the child develops proficiency in certain skills, a weaning off period can begin. Here, the child could be gradually introduced to real-world NMT, and the FIVE scenarios will slowly transition from a primary training tool to a NMT supplement. This begins what has been previously termed a transfer phase (26)—the transference of learned skills from in virtuo to the real world. Throughout this process, a specialized educator or instructor becomes more and more directly involved during actual training, as technique begins to become a focus and training starts to resemble classic NMT approaches (10, 44).
As the child matures and NMT becomes a more prominent part of their overall training regimen, FIVE scenarios can evolve into active play to assess transfer. At this stage, the educator or instructor can become an NPC in the environment as well and provide instructions, in real time, to the child. Alternatively, a pre-recorded instructor can be utilized to provide specific reminders of motor skill technique prior to the beginning of a scenario. Other human or virtual-human training partners can also be introduced to initiate peer-to-peer, or dyadic, scenarios. These types of in virtuo interpersonal training scenarios provide several advantages over dyadic training in the real world. There is the potential for the child to have increased motivation to be physically active when interacting with additional characters. There is also the opportunity to utilize additional developmental learning strategies such as mimicry, or pattern matching, in which the child can emulate another character in the virtual world. It can also promote the development of pro-social behavior that may be transferable to real-world interactions between children and their peers. This training, combined with the increased confidence that is gained with fundamental motor skill development, may provide further motivation to promote a consistently active lifestyle for the child into the future. As technologies are developed that are more portable and cost-effective, in virtuo interventions will become more widely available and should become prominent tools for the fight against physical inactivity and, ultimately, obesity.
Advantages and Considerations for In Virtuo Training
As described, there are many motor-learning advantages to training in VR instead of, or in supplement to, real-world training. In addition to those benefits, VR also may provide a lower-cost solution compared to instructor-led programs. Such programs could leverage VR technology to allow for the training of more children for a given session, with AI-based feedback driving within-trial or within-exercise changes that challenge the child appropriately. Performance data would be available in real-time for the instructor, and the instructor could provide additional feedback as needed. A similar strategy could be used in a telehealth setting for monitoring in-home training while the children are in between on-site training sessions. Importantly, VR training can provide a more fun and engaging environment, compared to real-world NMT. Based on adaptive feedback and, in following, the rules for FIVE scenario implementation, the training can be gamified to promote motivation, engagement, and enjoyment beyond that of traditional physical activity (45). While we have suggested similar interventions for real-world NMT (46), technology-integrated gamification would allow for an additional level of immersion and a fine-grained tuning of parameters that would allow for a more complete integration of fundamental training concepts with aspects of play.
There are, of course, also limiting factors that must be taken into consideration prior to implementing VR in young populations. First, there is currently no scientific basis for the safety and efficacy of VR in young children. Not unexpectedly, this has led to a lack of consensus among experts as to an appropriate age for existing VR HMD use: current hardware manufacturers differ on their safety language, with Oculus Rift (Oculus VR, LLC) setting an age limit of 13+ years, Sony Playstation VR (Sony Interactive Entertainment, LLC) setting an age limit of 12 years, and while the HTC Vive does not set an age limit, there is language in the user guide that states that the HTC Vive (HTC Corp.) was not designed to be used by children. However, several studies have demonstrated the utility of HMD-based VR systems for use in children as young as 5 years of age (47–51), and while safety was not a central focus of these studies, there were minimal to no side effects from HMD use in the young populations. Moreover, while there is currently no data on risks or contraindications from time spent in VR, as with TV/mobile screens, it is likely important to limit VR screen use to targeted training sessions of reasonably limited duration. For example, the training sessions advocated for in the current paper are designed to last for no more than 1.5 h (52), with VR training sessions as described here lasting no more than 30–45 min. While dosage limits and effects will need to be studied to fully understand training benefits and transfer, traditionally, NMT is only performed 3 days/week and, thus, screen time in VR would be far less than what the child would receive during normal daily activities (i.e., 2.5 h/day) (53). Another consideration is the design and implementation of headsets that fit a variety of head sizes. Just as a FIVE scenario requires a headset of specific design standards, adjustable straps and fittings are essential for comfort and safety in younger populations. In addition, HMD weight becomes more of a limiting factor for smaller users. Importantly, these are solvable engineering issues and will likely become more prevalent on future hardware as more and more younger users adopt VR technologies.
Summary
Fully immersive virtual environment scenarios have the potential as important tools in the prevention and treatment of physical inactivity; however, much more work is needed to utilize them efficiently and effectively. Many outstanding issues still need to be addressed to understand the efficacy of FIVE scenarios for use with children under the age of 7 and how to appropriately design and implement visual environments to be most effective for training. The information-based framework for understanding perceptual-motor behavior (20, 21, 23, 29, 54) provides a strong foundation for training motor skills in children. It is also, perhaps, the most critical component to in virtuo training as it takes advantage of the relation between motor control and perceptual information. However, many open questions remain and addressing them requires a strong methodological approach grounded in theory to tease apart these relations. This will help researchers and educators better understand what types of visual information are most important for affecting change in the movement of children; an approach that is equally true for training in the real world. Ultimately, FIVE scenarios as a precursor to, and integrated with, NMT can be additive in the promotion of a healthy, active lifestyle in children and for the treatment of physical inactivity via increased confidence and enjoyment of physical activity during critical phases of motor skill development.
Author Contributions
AK led the development of the manuscript and was primarily responsible for idea development and all writing. GM contributed to the exercise-deficit disorder and neuromuscular training components of the manuscript. DP assisted with idea generation and the interpersonal and cognitive development ideas and writing. MR assisted with the technology development sections and the information-based approach as integrated into the current manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer JN and handling editor declared their shared affiliation.
Footnote
References
1. Skinner A, Skelton JA. Prevalence and trends in obesity and severe obesity among children in the United States, 1999-2012. JAMA Pediatr (2014) 168(6):561–6. doi:10.1001/jamapediatrics.2014.21
2. Barlow SEExpert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics (2007) 120(Suppl):S164–92. doi:10.1542/peds.2007-2329C
3. Myer GD, Faigenbaum AD, Stracciolini A, Hewett TE, Micheli LJ, Best TM. Exercise deficit disorder in youth: a paradigm shift toward disease prevention and comprehensive care. Curr Sport Med Rep (2013) 12(4):248–55. doi:10.1249/JSR.0b013e31829a74cd
4. Faigenbaum AD, Stracciolini A, Myer G. Exercise deficit disorder in youth: a hidden truth. Acta Paediatr (2011) 100(11):1423–5. doi:10.1111/j.1651-2227.2011.02461.x
5. Duncan MJ, Stanley M. Functional movement is negatively associated with weight status and positively associated with physical activity in British primary school children. J Obes (2012) 2012:1–5. doi:10.1155/2012/697563
6. Barnett LM, Van Beurden E, Morgan PJ, Brooks LO, Beard JR. Does childhood motor skill proficiency predict adolescent fitness? Med Sci Sport Exerc (2008) 40(12):2137–44. doi:10.1249/MSS.0b013e31818160d3
7. Barnett LM, van Beurden E, Morgan PJ, Brooks LO, Beard JR. Childhood motor skill proficiency as a predictor of adolescent physical activity. J Adolesc Heal (2009) 44(3):252–9. doi:10.1016/j.jadohealth.2008.07.004
8. Faigenbaum AD, Farrell A, Fabiano M, Radler T, Naclerio F, Ratamess NA, et al. Effects of integrative neuromuscular training on fitness performance in children. Pediatr Exerc Sci (2011) 23(4):573–84. doi:10.1123/pes.23.4.573
9. Myer G, Faigenbaum AD, Ford K, Best TM, Bergeron MF, Hewett T. When to initiate integrative neuromuscular training to reduce sports-related injuries and enhance health in youth? Curr Sports Med Rep (2011) 10(3):155–66. doi:10.1249/JSR.0b013e31821b1442
10. Myer G, Kushner AM, Faigenbaum AD, Kiefer A, Kashikar-Zuck S, Clark JF. Training the developing brain, part I: cognitive developmental considerations for training youth. Curr Sports Med Rep (2013) 12(5):304–10. doi:10.1097/01.CSMR.0000434106.12813.69
11. Myer GD, Faigenbaum AD, Chu DA, Falkel J, Ford KR, Best TM, et al. Integrative training for children and adolescents: techniques and practices for reducing sports-related injuries and enhancing athletic performance. Phys Sportmed (2011) 39(1):74–84. doi:10.3810/psm.2011.02.1864
12. Faigenbaum A, Lloyd R. The role of the pediatric exercise specialist in treating exercise deficit disorder in youth. Strength Cond (2013) 35(3):34–41. doi:10.1519/SSC.0b013e318285618c
13. Seefeldt V. Developmental motor patterns: implications for elementary school physical education. In: Nadeau C, Holliwell W, Newell K, editors. Psychology of Motor Behavior and Sport. Champaign, IL: Human Kinetics (1980). p. 314–23.
14. Tisseau J. In vivo, in vitro, in silico, in virtuo the virtuoscope. 1st Workshop on SMA in Biology at Meso or Macroscopic Scales. Paris, France (2008). p. 1–17.
15. Faigenbaum AD, Lloyd RS, Myer GD. Youth resistance training: past practices, new perspectives, and future directions. Pediatr Exerc Sci (2013) 25(4):591–604. doi:10.1123/pes.25.4.591
16. Benjamin HJ, Glow KM, Mees PD. Choosing a strength training program for kids. Phys Sport (2003) 31(9):27–8. doi:10.3810/psm.2003.09.485
17. Donnelly JE, Blair SN, Jakicic JM, Manore MM, Rankin JW, Smith BK, et al. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc (2009) 41(2):459–71. doi:10.1249/MSS.0b013e3181949333
18. KN P, Wadden TA, Bartlett SJ, Zemel B, Verde TJ, Franckowiak SC. Exercise as an adjunct to weight loss and maintenance in moderately obese subjects. Am J Clin Nutr (1999) 49(4):1115–23.
19. Lee S, Bacha F, Hannon T, Kuk JL, Boesch C, Arslanian S. Effects of aerobic versus resistance exercise without caloric restriction on abdominal fat, intrahepatic lipid, and insulin sensitivity in obese adolescent boys: a randomized, controlled trial. Diabetes (2012) 61(11):2787–95. doi:10.2337/db12-0214
20. Warren WH. The dynamics of perception and action. Psychol Rev (2006) 113(2):358–89. doi:10.1037/0033-295X.113.2.358
21. Goldfield EC. Emergent Forms: Origins and Early Development of Human Action and Perception. New York, NY: Oxford University Press (1995).
22. Warren WH. Action modes and laws of control for the visual guidance of action. Adv Psychol (1988) 50:339–79. doi:10.1016/S0166-4115(08)62564-9
23. Gibson J. Visually controlled locomotion and visual orientation in animals. Br J Psychol (1958) 49:182–94. doi:10.1111/j.2044-8295.1958.tb00656.x
24. Thelen E, Smith L. A Dynamic Systems Approach to the Development of Cognition and Action. The MIT Press (1996). Available from: http://books.google.com/books?hl=en&lr=&id=kBslxoe0TekC&oi=fnd&pg=PR9&dq=A+Dynamic+Systems+Approach+to+the+Development+of+Cognition+and+Action&ots=ncseccPUto&sig=oS2aW5qHSL46yV0onbLdBkyKuhI
25. Sheridan T. Musings on telepresence and virtual presence. Presence Teleoperators Virtual Environ (1992) 1(1):120–6. doi:10.1162/pres.1992.1.1.120
26. Weiss PL, Kizony R, Feintuch U, Katz N. Virtual reality in neurorehabilitation. In: Selzer ME, Cohen L, Gage FH, Clarke S, Duncan PW, editors. Textbook of Neural Repair and Neurorehabilitation. Vol. 2. Cambridge: Cambridge University Press (2006). p. 182–97.
27. Kiefer AW, Rhea CK, Warren WH. VR-based assessment and rehabilitation of functional mobility. In: Steinicke F, Visell Y, Campos J, Lécuyer A, editors. Human Walking in Virtual Environments. New York, NY: Springer New York (2013). p. 333–50.
28. Warren W. Optic flow. 2nd ed. In: Basbaum A, Kaneko A, Shepherd G, Westheimer G, Albright T, Masland R, editors. The Senses: A Comprehensive Reference: Vision II. Oxford: Academic Press (2008). p. 219–30.
29. Gibson JJ. The Ecological Approach to Visual Perception. Hillsdale, NJ: Lawrence Erlbaum Associates (1986).
30. Tarr MJ, Warren WH. Virtual reality in behavioral neuroscience and beyond. Nat Neurosci (2002) 5(Suppl):1089–92. doi:10.1038/nn948
31. Mohler BJ, Thompson WB, Willemsen P, Creem-Regehr SH, Pick HL, Rieser JJ. Calibration of locomotion resulting from visual motion in a treadmill-based virtual environment. ACM Trans (2007) 4:1–17. doi:10.1145/1227134.1227138
32. Pailhous J, Ferrandez AM, Flückiger M, Baumberger B. Unintentional modulations of human gait by optical flow. Behav Brain Res (1990) 38(3):275–81. doi:10.1016/0166-4328(90)90181-D
33. Prokop T, Schubert M, Berger W. Visual influence on human locomotion. Modulation to changes in optic flow. Exp Brain Res (1997) 114(1):63–70. doi:10.1007/PL00005624
34. Varraine E, Bonnard M, Pailhous J. Interaction between different sensory cues in the control of human gait. Exp Brain Res (2002) 142(3):374–84. doi:10.1007/s00221-001-0934-3
35. Bardy BG, Warren WH, Kay BA. Motion parallax is used to control postural sway during walking. Exp Brain Res (1996) 111(2):271–82. doi:10.1007/BF00227304
36. Warren WH, Kay BA, Yilmaz EH. Visual control of posture during walking: functional specificity. J Exp Psychol Hum Percept Perform (1996) 22(4):818–38. doi:10.1037/0096-1523.22.4.818
37. Warren WH, Kay BA, Zosh WD, Duchon AP, Sahuc S. Optic flow is used to control human walking. Nat Neurosci (2001) 4(2):213–6. doi:10.1038/84054
38. Turano KA, Yu D, Hao L, Hicks JC. Optic-flow and egocentric-direction strategies in walking: central vs peripheral visual field. Vision Res (2005) 45(25–26):3117–32. doi:10.1016/j.visres.2005.06.017
39. Streit M, Shockley K, Morris AW, Riley MA. Rotational kinematics influence multimodal perception of heaviness. Psychon Bull Rev (2007) 14(2):363–7. doi:10.3758/BF03194135
40. Streit M, Shockley K, Riley MA. Rotational inertia and multimodal heaviness perception. Psychon Bull Rev (2007) 14(5):1001–6. doi:10.3758/BF03194135
41. Wulf G, McNevin N, Shea CH. The automaticity of complex motor skill learning as a function of attentional focus. Q J Exp Psychol Sect A (2001) 54(4):1143–54. doi:10.1080/713756012
42. Wulf G, Dufek JS, Lozano L, Pettigrew C. Increased jump height and reduced EMG activity with an external focus. Hum Mov Sci (2010) 29(3):440–8. doi:10.1016/j.humov.2009.11.008
43. Wulf G, Prinz W. Directing attention to movement effects enhances learning: a review. Psychon Bull Rev (2001) 8(4):648–60. doi:10.3758/BF03196201
44. Myer G, Lloyd R. How young is too young to start training. ACSM Heal (2013) 17(5):14–23. doi:10.1249/FIT.0b013e3182a06c59
45. Hamari J, Koivisto J, Sarsa H. Does gamification work? – A literature review of empirical studies on gamification. 2014 47th Hawaii International Conference on System Sciences. Waikoloa, HI, USA: IEEE (2014). p. 3025–34.
46. Kushner AM, Kiefer AW, Lesnick S, Faigenbaum AD, Kashikar-Zuck S, Myer GD. Training the developing brain part II. Curr Sports Med Rep (2015) 14(3):235–43. doi:10.1249/JSR.0000000000000150
47. Gershon J, Zimand E, Pickering M, Rothbaum BO, Hodges L. A pilot and feasibility study of virtual reality as a distraction for children with cancer. J Am Acad Child Adolesc Psychiatry (2004) 43(10):1243–9. doi:10.1097/01.chi.0000135621.23145.05
48. Das DA, Grimmer KA, Sparnon AL, McRae SE, Thomas BH. The efficacy of playing a virtual reality game in modulating pain for children with acute burn injuries: a randomized controlled trial [ISRCTN87413556]. BMC Pediatr (2005) 5(1):1. doi:10.1186/1471-2431-5-1
49. Strickland D, Marcus LM, Mesibov GB, Hogan K. Brief report: two case studies using virtual reality as a learning tool for autistic children. J Autism Dev Disord (1996) 26(6):651–9. doi:10.1007/BF02172354
50. Didehbani N, Allen T, Kandalaft M, Krawczyk D, Chapman S. Virtual reality social cognition training for children with high functioning autism. Comput Human Behav (2016) 62:703–11. doi:10.1016/j.chb.2016.04.033
51. Snider L, Majnemer A, Darsaklis V. Virtual reality as a therapeutic modality for children with cerebral palsy. Dev Neurorehabil (2010) 13(2):120–8. doi:10.3109/17518420903357753
52. Sugimoto D, Myer GD, Foss KD, Hewett TE. Dosage effects of neuromuscular training intervention to reduce anterior cruciate ligament injuries in female athletes: meta- and sub-group analyses. Sport Med (2014) 44(4):551–62. doi:10.1007/s40279-013-0135-9
53. Dumuid D, Olds T, Lewis LK, Martin-Fernández JA, Katzmarzyk PT, Barreira T, et al. Health-related quality of life and lifestyle behavior clusters in school-aged children from 12 countries. J Pediatr (2017) 183:178.e–83.e. doi:10.1016/j.jpeds.2016.12.048
54. Goldfield EC, Wolff PH. Development of Perception and Action (2003). Available from: http://books.google.com/books?hl=en&lr=&id=IJI4-JjDEScC&oi=fnd&pg=PA114&dq=Development+of+Perception+and+Action&ots=xlB3X9trcF&sig=pZ_JUR6IsX4AqMudwiOVsN7VPo4
Keywords: virtual reality, neuromuscular training, perceptual-motor learning, obesity prevention, physical inactivity
Citation: Kiefer AW, Pincus D, Richardson MJ and Myer GD (2017) Virtual Reality As a Training Tool to Treat Physical Inactivity in Children. Front. Public Health 5:349. doi: 10.3389/fpubh.2017.00349
Received: 24 April 2017; Accepted: 05 December 2017;
Published: 20 December 2017
Edited by:
Simon Rosenbaum, University of New South Wales, AustraliaReviewed by:
Joe Firth, University of Manchester, United KingdomJill M. Newby, University of New South Wales, Australia
Copyright: © 2017 Kiefer, Pincus, Richardson and Myer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adam W. Kiefer, adam.kiefer@cchmc.org